
Abstract
Intravenous fentanyl (10 mcg/kg) or saline (control) was randomly administered to 10 healthy sevoflurane-mono-anaesthetized piglets. Trembling was assessed by two blinded observers using a visual analogue scale (VAS) and a simple ordinal scale at baseline and 5 min (T5) after drug administration. If no trembling was observed at that time point, the opposite treatment was administered and piglets were re-evaluated after another 5 min (T10). Four out of five piglets showed trembling after fentanyl (T5), while none given saline showed any trembling. With fentanyl the VAS scores were significantly higher at T5 compared either with baseline or with the control treatment. Control animals received fentanyl after the 5 min evaluation and all piglets showed clear trembling afterwards. The median time after fentanyl administration until first muscle tremors was 51 (20–840) s. In summary, nine out of 10 sevoflurane-anaesthetized piglets showed muscle tremors after intravenous fentanyl. Tremors subsided over time and no specific treatment was necessary.
Trembling can be observed during anaesthesia in pigs. The resulting movements might interfere with planned interventions, and the uncertainty about their origin is disquieting to the anaesthetist. Although the observed trembling is discussed repeatedly and intensively by veterinary anaesthesiologists, no pertinent scientific reports can be found in the literature. To date, the drugs or mechanism(s) that might be involved have only been the subject of speculation.
Fentanyl is one of the preferred opioids in clinical anaesthesia and critical care settings. Therefore, it is also used very frequently in research animals. The goal of the present study was to investigate the effect of a 10 mcg/kg intravenous fentanyl bolus on trembling in sevoflurane-mono-anaesthetized piglets.
Animals
Ten healthy 4–6-week-old female piglets (Strickhof, Lindau, Switzerland) were randomly allocated to the following two treatments; fentanyl (F) or control (C).
Materials and methods
This study was conducted in accordance with the institutional animal welfare regulations and was approved by the district veterinary office of the Canton of Zurich (ZH59/14).
Anaesthesia was induced using sevoflurane (Sevorane®; Abbott AG, Baar, Switzerland) at 6% vaporizer setting in oxygen (6 L/min) delivered by face mask. A 22 G intravenous catheter (Vasovet; Henry Schein, Lyssach, Switzerland) was placed percutaneously into the middle ear vein, and oral endotracheal intubation was performed using a cuffed endotacheal tube with an internal diameter of 4.0 mm. Anaesthesia was maintained with sevoflurane in oxygen and air (25–35% inspired oxygen to maintain haemoglobin saturation >97%; total gas flow 0.9 L/min). Piglets were artificially ventilated using a volume-controlled mode with a positive end-expiratory pressure (PEEP) of 5 cmH2O to maintain physiological arterial partial pressures of carbon dioxide (PaCO2 = 4.7–6.0 kPa). Sevoflurane concentration was adapted to avoid movement and allow artificial ventilation as assessed by an experienced veterinary anaesthetist (SKR). Vital sign monitoring consisted of pulse oximetry, electrocardiogram (ECG), measurement of inspiratory and expired gas concentrations, non-invasive blood pressure and rectal body temperature control.
Two blinded observers (JYM and NS) evaluated the piglets for trembling once they were instrumented (baseline = T0). For this purpose a simple ordinal scale (trembling: no, possible or yes) was used together with a visual analogue scale (VAS: 0 mm no muscle tremors, 100 mm maximal trembling).
After baseline assessment a bolus dose of fentanyl (10 mcg/kg) (Sintenyl; Sintetica SA, Mendrisio, Switzerland) (treatment F) or the same volume of saline (treatment C) was randomly administered intravenously (IV).
Five minutes later the piglets were re-evaluated (see baseline) by the two observers (T5). In addition, time of first muscle tremor observation was noted. In case of no muscle tremors at T5, the opposite treatment was administered, that is fentanyl in treatment C and saline in treatment F, and the piglets were re-evaluated after another 5 min (T10). To avoid possible bias, no scoring was performed at T10 if tremors were already evident at T5.
The piglets were part of a magnetic resonance imaging (MRI) trial and because reliable assessment of trembling would have been extremely difficult after moving to the MRI room, no long-term data were recorded.
Data were analysed using GraphPad Prism 5 software for Mac and SigmaStat (SigmaStat® 3.5; Systat Software Inc, San Jose, CA, USA). A Mann–Whitney U-test was used to compare the two treatment groups for age and body weight. Breeds were compared using a chi-square test. Differences at T5 compared with baseline and between treatments were analysed using a two-way repeated measures analysis of variance (ANOVA) followed by Holm–Sidak for all pairwise multiple comparison for VAS. Average VAS values recorded by the two blinded observers for each piglet and at each time point were used for statistical analysis. Statistical significance was set at P ≤ 0.05. Data are presented as median (range) and mean ± standard deviation as appropriate.
Results
Body weight (Bwt), breed (SL: Swiss Landrace, F1: Swiss Landrace × Swiss Edelschwein), age, end-tidal concentration of sevoflurane (ETsev) and visual analogue scale (VAS: 0 mm = no trembling and 100 mm = maximal trembling) at baseline (T0), 5 min after first injection (T5) (control: saline; fentanyl: 10 mcg/kg IV), and 5 min after opposite treatment injection (T10) in sevoflurane-anaesthetized piglets.
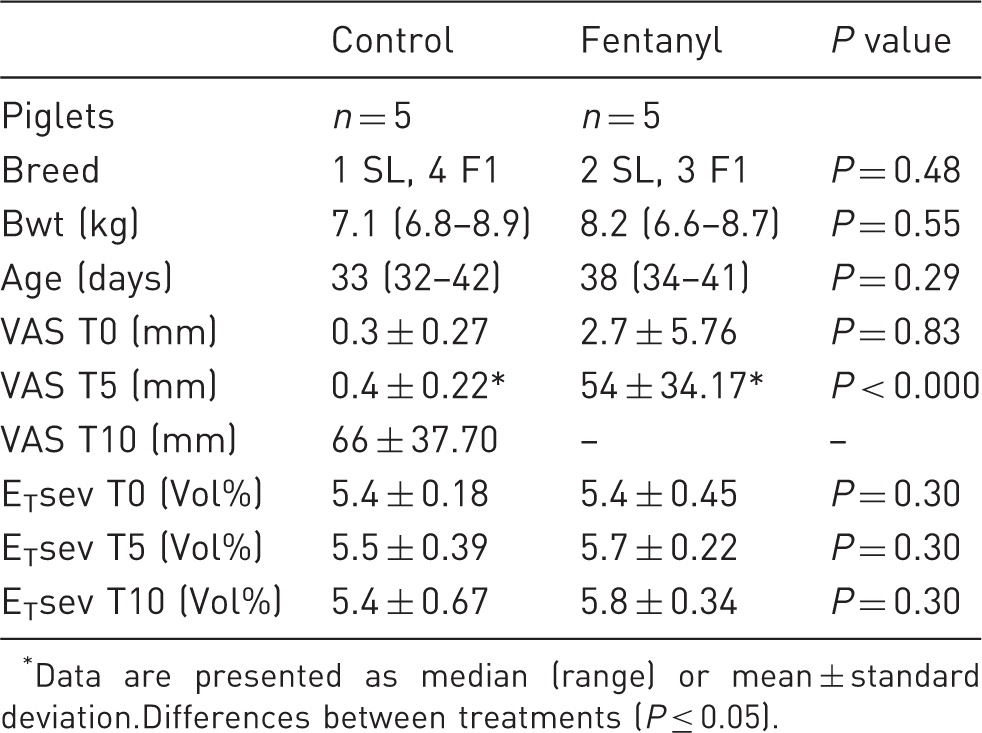
Data are presented as median (range) or mean ± standard deviation.Differences between treatments (P ≤ 0.05).
Based on the ordinal scale, four out of five piglets underwent trembling after administration of the bolus dose with fentanyl (F) (T5), while none of the saline-treated group showed any trembling. The control animals received fentanyl after the 5 min evaluation, and four out of five piglets showed trembling at the T10 evaluation using the ordinal scale. The fifth piglet also showed trembling but only at 14 min after drug administration.
Therefore, in total, only one out of 10 piglets did not show muscle tremors. The median (min–max) time after fentanyl administration until onset of tremor was 51 (20–840) s.
Tremors subsided over time and were no longer obvious at the start of MRI (range 33–43 min after fentanyl injection).
No clinically relevant changes in physiological variables were seen at any time point.
Discussion
The present study was initiated because the authors had repeatedly observed trembling after fentanyl (10 mcg/kg IV) bolus administration to piglets anaesthetized in a previous study. The observation was verified with this prospective randomized blinded crossover trial, in which nine out of 10 piglets showed muscle tremors after a single dose of fentanyl.
Agitation has been described in one- to three-day-old piglets receiving high doses of IV fentanyl (30 mcg/kg followed by 10 mcg/kg/h). 1 In the present study the piglets seemed to remain deeply anaesthetized as assessed by the anaesthetist. Neither was any increase in heart rate or mean blood pressure observed; excitement was therefore considered unlikely to be a cause for the tremors. In human adults and children, chest muscle rigidity (‘wooden chest syndrome’) or myoclonus can occur following opioid administration.2–4 Chest wall rigidity has also been previously reported in newborn piglets. 5 However, to our knowledge, opioid-induced myoclonus has not been reported before in piglets. The trembling observed in the present study could also be termed as ‘myoclonus’, which is defined as sudden, brief, shock-like, involuntary movements caused by muscular contractions or inhibitions. 6
The exact mechanisms leading to opioid-associated myoclonus are not clearly elucidated.3,4 However, their occurrence seems to be dose-dependent. Single moderate to high doses of fentanyl are frequently needed to achieve immediate and short effects, but are also required preceding a constant rate infusion to quickly achieve effective plasma concentrations. The 10 mcg/kg dose used in the present trial was chosen based on pilot results in piglets (unpublished data) and on recommended dosages for human infants. 7
In the present study, no adverse effects on ventilation or oxygenation were noticed. However, the tracheas of the piglets were intubated and the lungs artificially ventilated at the time of fentanyl administration. Unfortunately spirometry data were not recorded. The muscle trembling subsided over time in all piglets, and no specific treatment was necessary. However, muscle trembling might become an increasing problem when higher dosages of opioids are required or during prolonged administration (e.g. constant rate infusion). Muscle relaxants would probably be the rescue medication of choice in case of an urgent necessity to treat the problem.
In conclusion, this prospective controlled randomized study shows that fentanyl bolus administration can induce muscle tremors/myoclonus in piglets during sevoflurane anaesthesia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.