
Abstract
There are no reported studies evaluating the effect of midazolam on recovery quality, recovery time or minimum alveolar concentration (MAC) at which extubation occurs (MACextubation). Our hypotheses were that midazolam administered prior to recovery would decrease MACextubation, prolong recovery time but provide a smoother recovery. Sixteen Yorkshire pigs were anesthetized with isoflurane for approximately 5 h. The end-tidal isoflurane concentration was then stabilized at 1.4% for 20 min. Pigs were randomly assigned to receive midazolam or saline. The vaporizer was decreased by 10% every 10 min until extubation. Pigs were declared awake by a blinded observer and were assigned a recovery score by the same observer. Mean MACextubation was not significantly different for pigs receiving saline prior to recovery compared with those pigs receiving midazolam. The overall mean MACextubation for both groups was 0.6 ± 0.4 vol%. Time to extubation was not significantly longer with midazolam (124 ± 36 min) compared with the saline group (96 ± 61 min; P = 0.09). Recovery score was not significantly different between groups (midazolam, 0.86 ± 1.1; saline 0.5 ± 0.5; P = 0.26). In conclusion, midazolam did not affect MACextubation. There was no advantage of administering midazolam in the recovery period when performing step-down titration of isoflurane anesthesia.
Pigs often require general anesthesia both for medical care and during research projects. Volatile inhalant anesthetics, such as isoflurane, are commonly used to provide anesthesia. These anesthetics prevent movement and cause unconsciousness. Lack of movement is used to determine the minimum alveolar concentration (MAC) and lack of consciousness is used to determine the MACawake. MAC is the end-tidal concentration required to prevent purposeful movement in response to a noxious stimulus in 50% of patients. 1 MACawake, in humans, is the concentration at which an appropriate response to a command occurs in 50% of patients, 1 and generally represents the concentration at which memory is lost or unconsciousness occurs.2,3 In animals, a value for MACawake is difficult to determine due to the impossibility of obtaining an appropriate response to a verbal command. Because of this, MACextubation, which is the concentration at which tracheal extubation occurs, 4 may be a useful value for anesthetists and may be a reasonable substitute for MACawake in veterinary patients.
While inhalant anesthetics provide immobility and unconsciousness, these drugs also come with significant cardiovascular effects.5,6 Isoflurane causes a dose-dependent decrease in cardiac output, arterial blood pressure, and stroke volume.5,6 In humans, the MACawake for isoflurane is approximately one-third of the MAC.3,7 This allows the inhalant concentration to be titrated to a lower dose while still preventing awareness. Because the adverse cardiovascular effects are dose-dependent, the decreased inhalant concentration should provide better cardiovascular stability.5,6 In humans, MACextubation to MAC ratio is greater than MACawake to MAC ratio, 8 so it is likely that most animals are still unconscious at MACextubation.
The addition of muscle relaxants and analgesics can allow for a decreased inhalant concentration by providing balanced anesthesia (muscle relaxation, analgesia and unconsciousness). Benzodiazepines, such as midazolam, provide muscle relaxation 9 and sedation, at a dose of 0.1–0.2 mg/kg.10–12 The effects of midazolam on the cardiovascular system are minimal. 9 Studies of the cardiovascular effects of midazolam in swine have shown that this drug causes a mild decrease in heart rate but cardiac output and mean arterial blood pressure remain unchanged. 11
Because midazolam has minimal cardiovascular effects and provides muscle relaxation, this drug may be useful as an adjunct to inhalant anesthesia. MAC-sparing effects of midazolam have been reported in various species.13,14 Benzodiazepines, like midazolam, may induce sedation and muscle relaxation by acting on either central or spinal gamma aminobutyric acid type A (GABAA) receptors. 13 Due to these effects, benzodiazepines may reduce MAC and aid in providing balanced anesthesia. Midazolam has been shown to decrease the MAC necessary to abolish all movement (MACNM) in isoflurane-anesthetized dogs. 13 Addition of midazolam may decrease the isoflurane concentration at which consciousness occurs. 14 However, no studies evaluating the effects of midazolam on MAC, MACextubation, or MACawake have been performed in pigs. If midazolam decreases MACawake and MACextubation, the anesthetist may be able to use an even lower concentration of inhalant to prevent consciousness and rejection of the endotracheal tube by administering midazolam to a patient or research subject and to provide a more satisfactory recovery quality. The effect of midazolam on recovery time and quality administered just prior to recovery is unknown in pigs.
The purpose of the study reported here is to determine the MACextubation in pigs. In addition, the effects of the administration of midazolam on MACextubation, recovery time, and recovery quality were evaluated. The hypotheses were that administration of midazolam prior to recovery would lower the MACextubation and provide a more satisfactory recovery but prolong the time to extubation.
Materials and methods
Animals
Sixteen healthy, castrated male Yorkshire pigs (Valley Brook Farm, Madison, GA, USA) were used in the study. They were approximately eight weeks old and weighed between 23 and 31 kg. There was an acclimatization period of seven days prior to the start of the study period. The animals were housed at the Veterinary Bioresources Facility at the University of Georgia, Athens, GA, USA. They were housed in groups of three in pens measuring 4 m × 8.4 m. A 12:12 h light/dark schedule was used. The room temperature was 22.2 ± 2.2℃.
Study design
The study was approved by the Institutional Animal Care and Use Committee. Pigs were premedicated with xylazine (Anased; Lloyd Laboratories, Shenandoah, IA, USA) 1.1 mg/kg, and tiletamine/zolazepam (Telazol; Zoetis, Florham Park, NJ, USA) 2.0–3.0 mg/kg intramuscularly in the epaxial muscles. The pigs then received 1.62–9.26 mg/kg of ketamine intramuscularly (Ketaset; Fort Dodge Animal Health, Madison, NJ, USA) to allow for catheter placement. A 22 gauge, one-inch catheter was placed in the marginal ear vein. Ketamine 0.00–17.05 mg/kg was administered intravenously to effect until orotracheal intubation was achieved. After intubation, buprenorphine (Buprenex; Reckitt Benckiser Healthcare Ltd, Hull, UK) 0.01 mg/kg was administered intramuscularly. The endotracheal tube was then connected to a rebreathing circuit and maintained with isoflurane (Isoflo; Abbott Animal Health, Abbott Park, IL, USA) in 100% oxygen delivered at 1 L/min. Agent-specific, temperature-compensated, calibrated vaporizers were used for the delivery of isoflurane. Intermittent positive pressure ventilation (Multiflow 2002; Hallowell EMC, Pittsfield, MA, USA) was used to maintain a target end-tidal carbon dioxide concentration between 35 and 45 mmHg. End-tidal agent concentrations were sampled via a side stream sampling L-shaped connector attached to both the endotracheal tube and the Y-piece of the anesthesia circuit. End-tidal gas concentrations were continuously measured with a calibrated infrared gas analyzer (POET IQ 602; Criticare Systems, Inc, Waukesha, WI, USA). The gas analyzer was calibrated according to the manufacturer’s recommendations, once a day during the study period. Lactated Ringer’s solution (Hospira, Lake Forest, IL, USA) was administered intravenously at a rate of 10 mL/kg/h. Body temperature (Surgivet Advisor; Smiths Medical, Norwell, MA, USA) was measured continuously by a probe placed in the thoracic portion of the esophagus; and body temperature was maintained between 36.9℃ and 38.3℃ with a forced-air warming unit (Bair Hugger Model 505; Arizant, Eden Prairie, MN, USA). Blood pressure was monitored via an indirect oscillometric device (Critikon Dinamap 8300; GE Medical Systems Information Technologies, Tampa, FL, USA) due to difficulty in achieving arterial access for direct blood pressure monitoring. The blood pressure occluding cuff was placed on the antebrachium of each pig. The width of the blood pressure-occluding cuff was 40% of the circumference of the forelimb of each pig. When MAP decreased to <60 mmHg, a single fluid bolus (5 mL of lactated Ringer’s solution per kilogram) was administered. If hypotension did not resolve, dobutamine (DOBUTamine; Hospira) at 5 mcg/kg/min was administered intravenously.
Determination of MACextubation
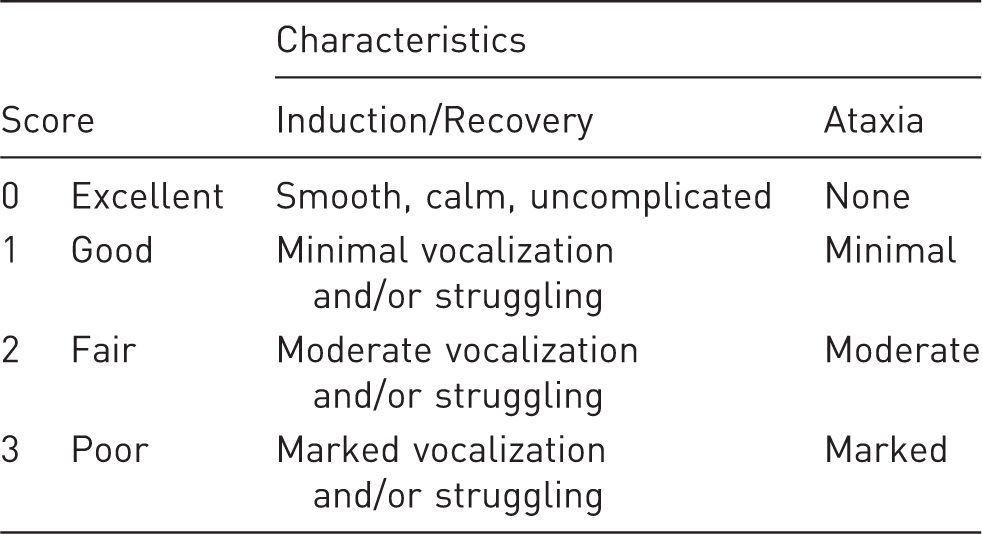
As part of another study, pigs were anesthetized for the creation and treatment of an aortic aneurysm via femoral artery catheterization and ventral midline celiotomy, respectively. Twenty minutes prior to completion of this procedure, the vaporizer was adjusted to achieve an end-tidal isoflurane concentration of 1.4%. Pigs were randomly assigned by lottery to receive midazolam (Midazolam; West-Ward Pharmaceutical, Eatontown, NJ, USA) 0.2 mg/kg intravenously, or an equivalent volume of saline (1 mL/25 kg intravenously). The target end-tidal concentration was maintained at 1.4% for 20 min, then the test drug was administered to each pig. The isoflurane vaporizer dial setting was decreased by 10%, and each pig was allowed to stabilize at that vaporizer setting for 10 min. During each vaporizer step-down, the end-tidal isoflurane concentration remained stable for at least 10 min. Blood pressure, heart rate, respiratory rate, and end-tidal carbon dioxide concentration were recorded, and then the vaporizer setting was decreased by another 10%. This continued until the pig rejected the endotracheal tube, as evidenced by chewing, swallowing and head movement, and was declared awake by one observer blinded to the drug administered. The MACextubation was then calculated as mean of the end-tidal concentration before a positive response was obtained and the end-tidal concentration when a positive response was obtained. The recovery was then assigned a quantitative score using a modified version of a previously published scoring system (Appendix). 15 Upon recovery from anesthesia, buprenorphine 0.01 mg/kg was administered intramuscularly.
Postoperative care
The animals were carefully monitored during anesthesia recovery. They were monitored hourly for 6 h following recovery from anesthesia. The incision and overall health of the animal was evaluated three times daily for seven days following anesthesia and surgery. At the same time the animals were evaluated for pain and buprenorphine 0.01 mg/kg was administered intramuscularly if the pig displayed any signs of pain.
Statistics
Normality was determined using the D'Agostino–Pearson test. Normally-distributed data were compared using an unpaired 2-way t-test, and non-normally distributed data were compared using a Mann–Whitney U-test. Number of pigs in each group with a recovery score of 0 was compared using a chi-square test. Significance was set at α < 0.05.
Results
There were no significant differences between groups with regard to weight (midazolam, 27.2 ± 3.3 kg; saline, 27.2 ± 3.7 kg, P = 0.93) or duration of anesthesia (midazolam, 314.8 ± 41 min; saline 303.3 ± 33 min, P = 0.29). No significant differences were found between groups with regard to dose of intramuscular ketamine (midazolam, 4.2 ± 2.16 mg/kg; saline, 3.24 ± 2.59 mg/kg, P = 0.27), dose of intravenous ketamine (midazolam, 6.59 ± 4.95 mg/kg; saline, 3.6 ± 2.51 mg/kg, P = 0.15), or total dose of ketamine administered (midazolam, 10.79 ± 4.78 mg/kg; saline, 6.84 ± 4.59 mg/kg, P = 0.08). Time to extubation was not significantly longer with midazolam (124 ± 36 min) compared with results from the saline group (96 ± 61 min; P = 0.09). Recovery score was not significantly different between groups (midazolam, 0.86 ± 1.1; saline, 0.5 ± 0.5; P = 0.26).
Mean MACextubation was not significantly different for isoflurane-anesthetized pigs receiving saline prior to recovery compared with those pigs receiving midazolam. The MACextubation for the saline group was 0.65 ± 0.19% and the mean MACextubation for the midazolam group was 0.55 ± 0.18% (P = 0.29). The overall mean MACextubation for both groups was 0.6 ± 0.4%.
Discussion
The results of this study indicate that MACextubation in isoflurane-anesthetized pigs is 0.6%. Previous studies of isoflurane in pigs have shown that MAC for this inhalant is 1.9–2.04%.16–19 Using these previously established MAC values, our study demonstrates that the MACextbuation to MAC ratio in pigs is 0.29–0.34 for isoflurane. This ratio is similar to MACawake to MAC ratios in humans, where ratios of 0.2–0.35 have been reported;1,20 however this is lower than MACextubation to MAC ratios of 0.8–1.4.4,8 All these ratios differ from dogs, which have a MACextubation to MAC ratio for isoflurane of 0.8. 21 Based on these findings, MACawake to MAC and MACextubation to MAC ratios vary among species. The difference in MACextubation to MAC ratios may be attributed to differences in airway sensitivity to endotracheal tubes.
In this study, midazolam, at the reported dose, failed to significantly decrease MACextubation values versus MACextubation for those treated with saline. This indicates that midazolam does not decrease the isoflurane concentration required to prevent extubation. In dogs, administration of midazolam has been shown to have MAC-sparing effects and decrease the isoflurane concentration required to prevent movement. 13 In addition, diazepam, a benzodiazepine, and fentanyl administered simultaneously to isoflurane-anesthetized dogs have been shown to have a greater MAC-sparing effect than fentanyl alone. 22 There have been no studies evaluating the effects of the benzodiazepines (e.g. midazolam) on MAC in pigs.
Evidence regarding the duration of midazolam sedation in pigs is limited. Given that a slow alveolar washout was used to determine MACextubation, it is possible that the potential MAC-sparing effects of midazolam had waned at the time of awakening. The duration of effect of midazolam is approximately 50 min in humans 23 and up to one hour in rats. 24 However, the duration of sedation in alpacas was longer at about 90 min. 25 Despite the potentially short duration of action, studies have shown that midazolam, when used as a premedication agent, reduces MAC by 23% in dogs undergoing ovariohysterectomy. 26 Midazolam, when given as the sole agent for premedication in children undergoing surgery of approximately 90 min, decreases the MACawake compared with saline premedication. 14 Given the results of these studies, midazolam would be expected to have effects at the time of awakening in these pigs.
Midazolam at the dose reported here not only had no effect on MACextubation in pigs, but also did not affect the time to extubation. Inconsistent data regarding the sedative effects of midazolam in pigs have been reported. A study in healthy laboratory piglets found that midazolam at a dose of 0.2 mg/kg intramuscularly provided good sedation. 10 By contrast, 0.25 mg/kg of midazolam provided some sedation in adult swine but this sedation was inconsistent. 9 It is possible that the pigs did not show evidence of longer recovery due to the inconsistent sedation provided by midazolam. In this study, all the pigs received buprenorphine, tiletamine, zolazepam, and xylazine as premedication. A study in pigs has shown that all of these agents cause a reduction in MAC. 27 A MAC-sparing effect of midazolam may have been difficult to detect in the presence of these premedication agents; however both groups received the same drugs as premedication so the effect of this combination of drugs should be minimal. The only variability among individuals in this study was in the dose of ketamine; however the t½ of ketamine is shorter than the duration of anesthesia in this study 28 and there were no differences between the groups with respect to their ketamine dose. To the authors’ knowledge the pharmacokinetics of xylazine in pigs has not been determined; however a study in pigs has determined that sedation with tiletamine–zolazepam, ketamine, and xylazine has a duration of 61 min. 29
The results of this study indicate that midazolam, at the reported dose, had no effect on recovery quality. The quality of recovery is important in order to prevent injury secondary to agitation during awakening. In our study on pigs, it is possible that there was inadequate sedation provided by the midazolam or that the duration of midazolam was too short to extend in the recovery period. However, none of the pigs in this study had adverse events during the recovery period and the recovery score for all pigs was low (<2). It is possible that the presence of other drugs, tiletamine–zolazepam, ketamine, or buprenorphine, caused a quiet, calm recovery state in pigs of both groups. A study evaluating the effects of varying doses of ketamine (up to 20 mg/kg) in combination with xylazine and midazolam resulted in complete recovery, standing with no ataxia, in 92 min, which is much shorter than the duration of anesthesia in the above reported study. 30 Additionally, pigs given xylazine–ketamine–tiletamine/zolazepam for anesthesia had a duration of anesthesia of 61 min which was also significantly shorter than the duration of anesthesia in the current study. 29 Buprenorphine at a dose of 0.01 mg/kg provides analgesia for up to 6 h in pigs. 31 It is possible that this drug played a role in providing smooth recoveries in these pigs, however elimination of analgesic medications in the anesthesia protocol was deemed unethical. To the authors’ knowledge, there are no studies evaluating the effect of buprenorphine on recovery time or quality in pigs, so the effects of this drug on the recovery quality are unclear. Additionally, this was a small sample size which may have made it difficult to detect small differences in the recovery score between groups.
A potential limitation to this study is that it is difficult to assess awareness and consciousness in animals. Other studies evaluating MACawake in animals have been performed.21,32 Due to differences in airway sensitivity among species and lack of response by pigs to verbal commands, MACextubation was evaluated. For this study, a slow alveolar washout was used. This allowed adequate time for the brain and alveolar concentrations to equilibrate, and minimized any potential error in determining MACawake 20 or MACextubation that could result from a fast alveolar washout. Despite our inability to truly assess consciousness in animals, it is useful to know the anesthetic concentration at which a specific species rejects the endotracheal tube. Another limitation of this study is that we were unable to determine MAC for isoflurane in this group of pigs. The pigs used in this study were part of another study and were undergoing surgery for aortic aneurysm formation, which prevented MAC determination during the procedure. However, evaluation of MAC and its relationship to MAC multiples in desflurane-anesthetized dogs have found that the determination of individual MAC for animals used in studies of MAC multiples is unnecessary. 33
Footnotes
Acknowledgements
The authors would like to thank Merilee Thoresen, Tristan Lewis, and Lori Dressel for technical assistance.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.