
Abstract
Sedating animals is sometimes necessary in experimental research. This paper presents and discusses the influence of four of the most common anesthetic agents on cardiovascular parameters in rats. We also studied the influence of body temperature. Ten-week-old Sprague-Dawley rats were anesthetized with either isoflurane, pentobarbital, ketamine/xylazine or tiletamine/zolazepam (n = 12 in each group). A pressure-sensing catheter was placed in the right carotid artery for the continuous measurement of arterial pressure, and echocardiography was performed. Indices of cardiac function were significantly higher in the tiletamine/zolazepam rats compared with the other groups. Heart rate was highest but stroke volume lowest with pentobarbital. Left ventricular diastolic dimension was lower in the pentobarbital and tiletamine/zolazepam rats compared with the isoflurane or ketamine/xylazine rats. Intraventricular diastolic pressure was similar in all groups whereas intraventricular systolic pressure, as well as both systolic and diastolic aortic pressures, was significantly higher in the tiletamine/zolazepam rats compared with the other groups. No hemodynamic indices differed significantly among the isoflurane, pentobarbital and ketamine/xylazine rats. Lowering body temperature significantly reduced heart rate and cardiac output but had no apparent effect on hemodynamic parameters. In conclusion, although cardiac functional parameters differed between the different anesthetic agents in ways that could be of relevance to the researcher, they may all have a role in experimental cardiology. Importantly, tiletamine/zolazepam anesthesia resulted in significantly higher indices of cardiac function and elevated blood pressures compared with the other anesthetic agents, a finding that should be kept in mind when interpreting data obtained in rats sedated on this regimen.
Keywords
Non-invasive cardiac imaging of small animal models is an integral part of cardiovascular research. 1 With emerging transgenic rat models, increasing interest is likely to be devoted to these models. 2 Modern imaging techniques allow detailed assessments of global and regional cardiac function, quantifications of myocardial perfusion and studies of cardiac metabolism.3–6 However, many of these techniques require relatively long acquisition times, during which the animal needs to be immobilized. Sedating the animal is therefore necessary3,6 and this presents several challenges to the researcher. First, anesthetized animals are unable to maintain their physiological body temperature. Body temperature is a major determinant of several indices of cardiovascular function as well as an outcome of specific interventions.7,8 The researcher must therefore attempt to control this parameter. Second, the anesthetic agents themselves influence the cardiovascular system. Most anesthetic agents have been shown to affect cardiac contractile function as well as metabolic and cell survival pathways.9–12 Pentobarbital (PEN), ketamine/xylazine (KTX) and isoflurane (ISF) have been widely used for a long time in small animal laboratories. PEN is preferred in some situations, e.g. studies of infarct size, because it is believed not to interact with the preconditioning phenomena. 13 Ketamine is a dissociative anesthetic associated with adrenergic effects including positive inotropy and chronotropy whereas xylazine is considered to be a clonidine analog that produces muscle relaxation and that possesses opposite effects on the cardiovascular system. The effect of combined ketamine and xylazine is therefore variable, depending on the dose, subject and species. 14 The volatile anesthetic ISF is widely used in small animals due to its favorable kinetic profile. Although ISF is often reported to be associated with less severe depression of cardiovascular indices compared with other anesthetic agents9,10,14 some researchers argue that PEN or a combination of KTX is associated with less severe cardiocirculatory depression. 15 We chose to also include tiletamine/zolazepam (TEL), a fourth regimen, because a recent study suggested that TEL is associated with less cardiac depression and therefore may be favorable in at least some settings. 16 Tiletamine is a dissociative anesthetic that is chemically and pharmacologically related to ketamine and causes cataleptoid anesthesia whereas zolazepam is a benzodiazepine with sufficient tranquilizing properties to cause muscle relaxation. 16
Establishment of each anesthetic’s characteristics will aid researchers in choosing the appropriate agent for a given study and when trying to compare studies in which different anesthetic regimens were used. The primary aim of the present study was to determine the influences of four of the most commonly used anesthetic agents, namely PEN, KTX, ISF and TEL on echocardiographic and hemodynamic parameters in male Sprague-Dawley rats.
In addition to the choice of drugs, the concentration of a given anesthetic agent may influence cardiac function. 15 We decided, as one of our secondary aims, to study chosen indices of cardiac function at different concentrations of ISF. Lastly, although, as mentioned above, body temperature is known to affect cardiomyocyte metabolism and survival, information on body temperature is often omitted in research papers. 17 The effect of core body temperature on cardiac function was assessed in this study.
Animals
All animal work was performed in accordance with the National Institutes of Health (NIH) guidelines for use of experimental animals and the study protocol was approved by the Animal Ethics Committee at Gothenburg University. The animals were housed in a temperature-controlled (25℃) facility with a 12 h light/dark cycle and given free access to food and water. A total of 54 male Sprague-Dawley rats weighing approximately 330 g were used in this study. Six rats were used, in a cross-over design, to establish the minimal dose of each of the intravenous anesthetic agents that yielded adequate anesthesia. Forty-eight rats underwent echocardiography and invasive hemodynamic assessment, and were subsequently euthanized by an anesthetic overdose without regaining consciousness.
Materials and methods
The rats were randomized to anesthesia with ISF, KTX, PEN or TEL. For each intravenous anesthetic agent, the minimal concentration that consistently resulted in adequate anesthesia, i.e. complete immobilization and loss of the toe-pinching reflex, was first determined (n = 6 for each anesthetic agent). Twelve rats were then randomized to each group. The rats were weighted and anesthetized with ISF inhalation (1.5%, 1 L/min) or intraperitoneal injection of PEN (30 mg/kg) KTX (30 mg/kg / 5 mg/kg), or TEL (40 mg/kg / 40 mg/kg). Echocardiographic and hemodynamic assessments were performed as described below. The respiratory rate was noted in each animal 15 min post-anesthesia. During the experiments all the animals were breathing a mixture of air and oxygen (30%). The experimental set-up is shown in Figure 1.
Experimental set-up. Heart rate was calculated from the arterial pressure curve. LAX: parasternal long axis cine loop; EKV: ECG-gated kilohertz visualization; PW: pulsed-wave Doppler recording of the pulmonary artery blood flow.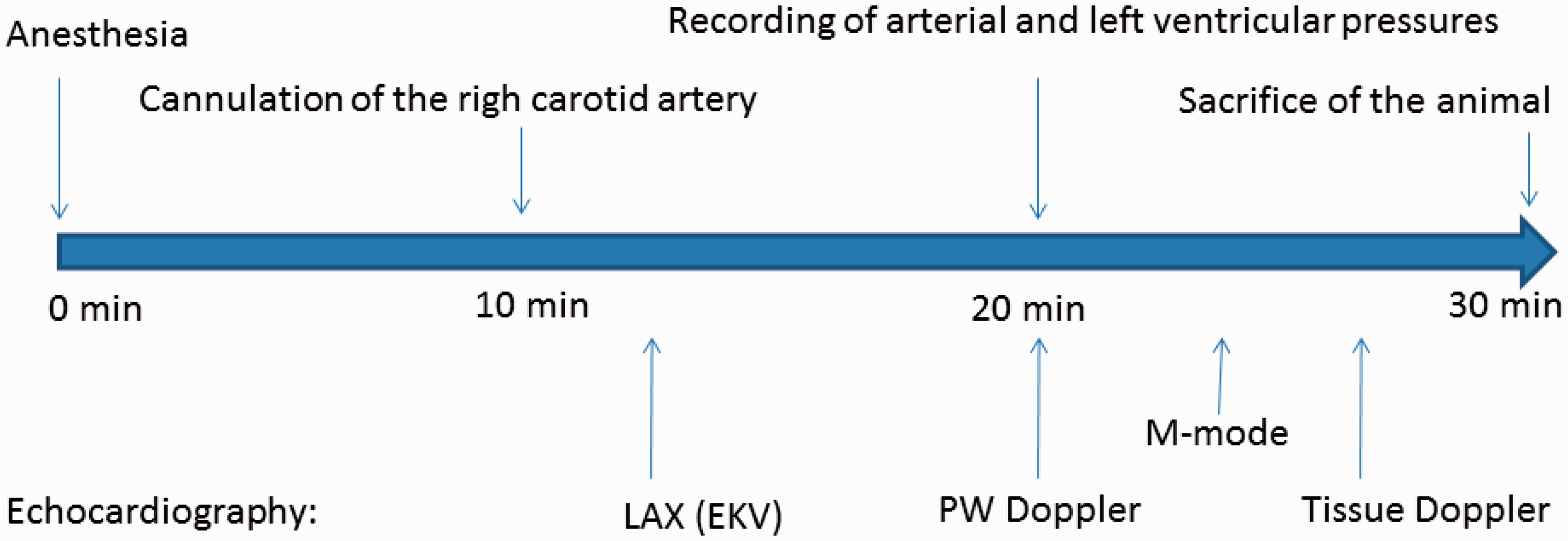
To evaluate the influences of the degree of ISF anesthesia, six of the rats that were randomized to ISF remained anesthetized with a mixture of ISF and air (1 L/min continuous flow) and echocardiography and hemodynamic assessments were repeated at different ISF concentrations (1.5%, 2%, 2.5%, and 3%). Selected hemodynamic and echocardiographic indices were acquired at the different ISF concentrations. The same six rats were used in the assessment of the effect of hypothermia on cardiac function. At 1.5% ISF anesthesia body temperature was allowed to drop to 34.5℃ by lowering the set-point of the heating pad. Recordings were made at 37.5, 37, 36.5, 36, 35.5, 35, and 34.5℃. The rats were stabilized at the given concentration or temperature for 5 min before any recordings were made.
Hemodynamic assessment
The right carotid artery was dissected free and catheterized (St Jude Medicals, Radi analyzer St. Paul, Minnesota; Global Siemens Healthcare, Erlangen, Germany). The catheter was then passed retrogradely into the left ventricle under real-time 2-dimensional (2D) echocardiographic guidance. Proper positioning of the pressure sensor was verified by echocardiography (Figure 2a); Supplementary video 1, see http://lan.rsmjournals.com/lookup/suppl/doi:10.1177/0023677213502015/-/DC1.). Several recordings were stored before the catheter was withdrawn 3 mm into the arterial circulation where arterial pressure recordings were acquired.
Selected recordings. (a) Properly positioned pressure sensor (arrow) without direct tissue contact with the left ventricular wall. (b and c) Pressure recordings obtained within the left ventricle (b) and after withdrawal 3 mm into the aorta (c). (d) Representative continuous Doppler recording of the pulmonary trunk blood flow. (e) Representative M-mode recording in the parasternal short axis 6 mm below the mitral annulus.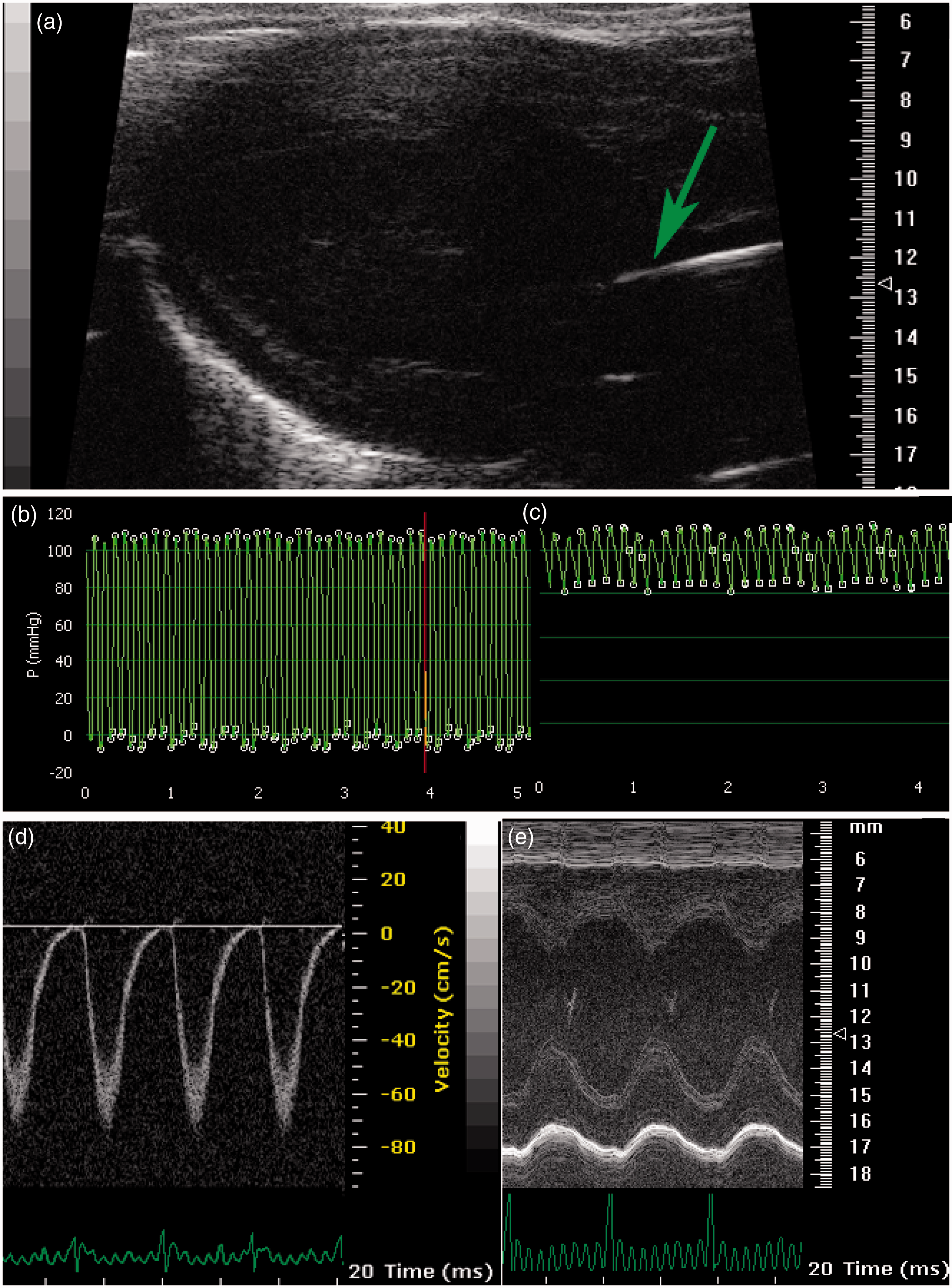
Echocardiography
Echocardiography was performed using a VisualSonics 770 VEVO imaging station (VisualSonics, Inc, Ontario, Canada), which includes an integrated rail system for consistent positioning of the ultrasound probe. The hair from the chest was removed with an electrical clipper and a hair removal gel prior to the examination. The animals were placed on a heating pad and connected to an electrocardiogram (ECG) while rectal temperature was monitored to maintain body temperature 38 ± 0.1℃. A 35 MHz linear transducer (VisualSonics, RMV 707, Inc, Ontario, Canada) was used for imaging. An optimal parasternal long axis (LAX) cine loop (i.e. visualization of both the mitral and aortic valves, and maximum distance between the aortic valve and the cardiac apex) of >1000 frames/s was acquired using the ECG-gated kilohertz visualization technique. Cross-sectional area of the proximal pulmonary artery was measured in B-mode image immediately distal to the pulmonary valve, and continuous Doppler recordings were obtained at the same point in the pulmonary artery with a flow angle near perpendicular to the ultrasonic beam (Figure 2b). The probe was then rotated 90° and positioned 6 mm below the mitral annulus, i.e. at the level of the papillary muscles. Three parasternal short-axis (SAX) M-mode sequences were stored and tissue velocities were acquired by the Doppler technique for the posterior myocardial wall (Figure 2d). Both endocardial and epicardial tissue velocities were recorded.
Fractional shortening (FS) was calculated in the M-mode image as FS = (EDD–ESD)/EDD, where EDD and ESD are end-diastolic and end-systolic diameters, respectively.
Ejection fraction (EF) was calculated as EF = (EDV–ESV)/EDV, where EDV and ESV are end-systolic and end-diastolic volumes, respectively.
The prolate–ellipsoid formula estimates left ventricular (LV) volumes from a single 2D parasternal long axis cine loop as: 18
Stroke volume (SV) was calculated as EDV–ESV, where EDV and ESV are end-diastolic and end-systolic volumes derived by each of the formulas described above, or it was estimated from the pulmonary artery flow pattern. 18
Cardiac output (CO) was estimated as SV (acquired from the pulmonary artery flow pattern) multiplied by heart rate (acquired from the arterial pressure curve).
Mid-myocardial segmental transmural end-systolic radial strain (RS) was calculated in the 6 mm SAX cine loop as ESWT/EDWT, where ESWT and EDWT are end-systolic and end-diastolic average wall thickness, respectively. ESWT and EDWT were automatically derived by the software after circumferential delineation of endo- and epicardial tissue borders.
Statistics
STATA 12 statistics software (StataCorp, College Station, TX, USA) was used for standard statistical analysis of the data. Data are presented as mean ± SD in text and tables and as mean + SEM in figures. Indices of cardiac function were analyzed by analysis of variance (ANOVA) and modified Student’s t-test. Bonferroni corrections were used to adjust modified t-test derived probability values. P < 0.05 was considered statistically significant. All comparisons were specified in advance.
Results
Body weight, heart rate and respiratory rate.
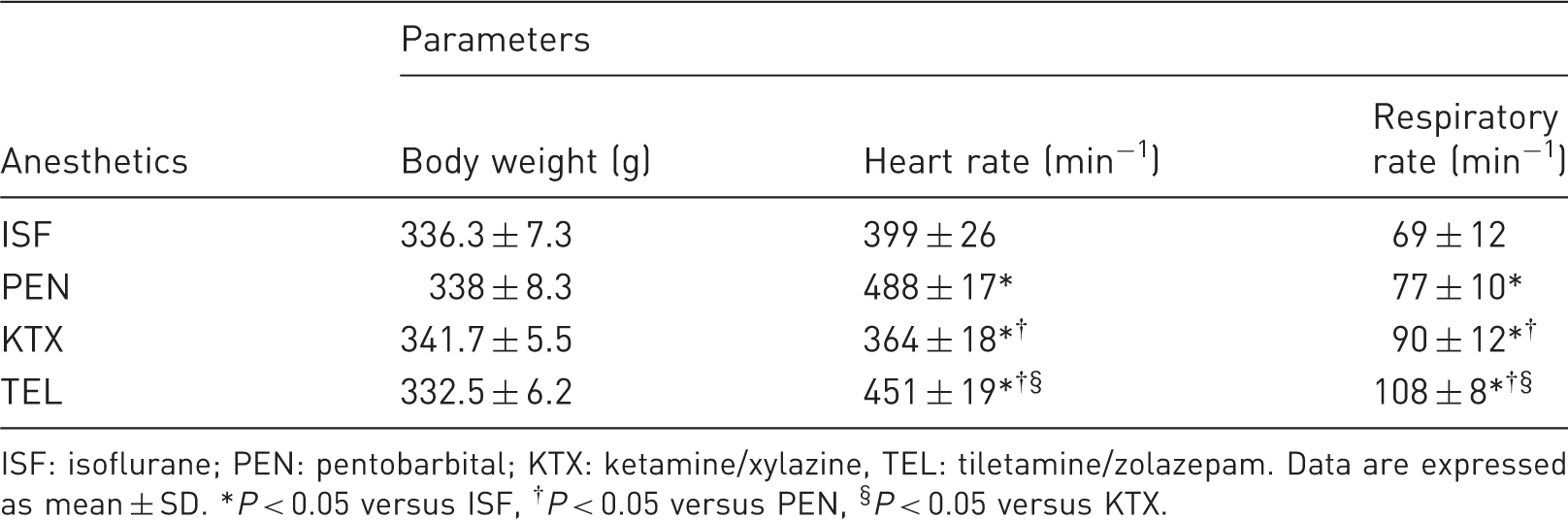
ISF: isoflurane; PEN: pentobarbital; KTX: ketamine/xylazine, TEL: tiletamine/zolazepam. Data are expressed as mean ± SD. *P < 0.05 versus ISF, †P < 0.05 versus PEN, §P < 0.05 versus KTX.
Echocardiography
Echocardiographic parameters measured in rats anesthetized on isoflurane (ISF), pentobarbital (PEN), ketamine/xylazine (KTX) or tiletamine/zolazepam (TEL).
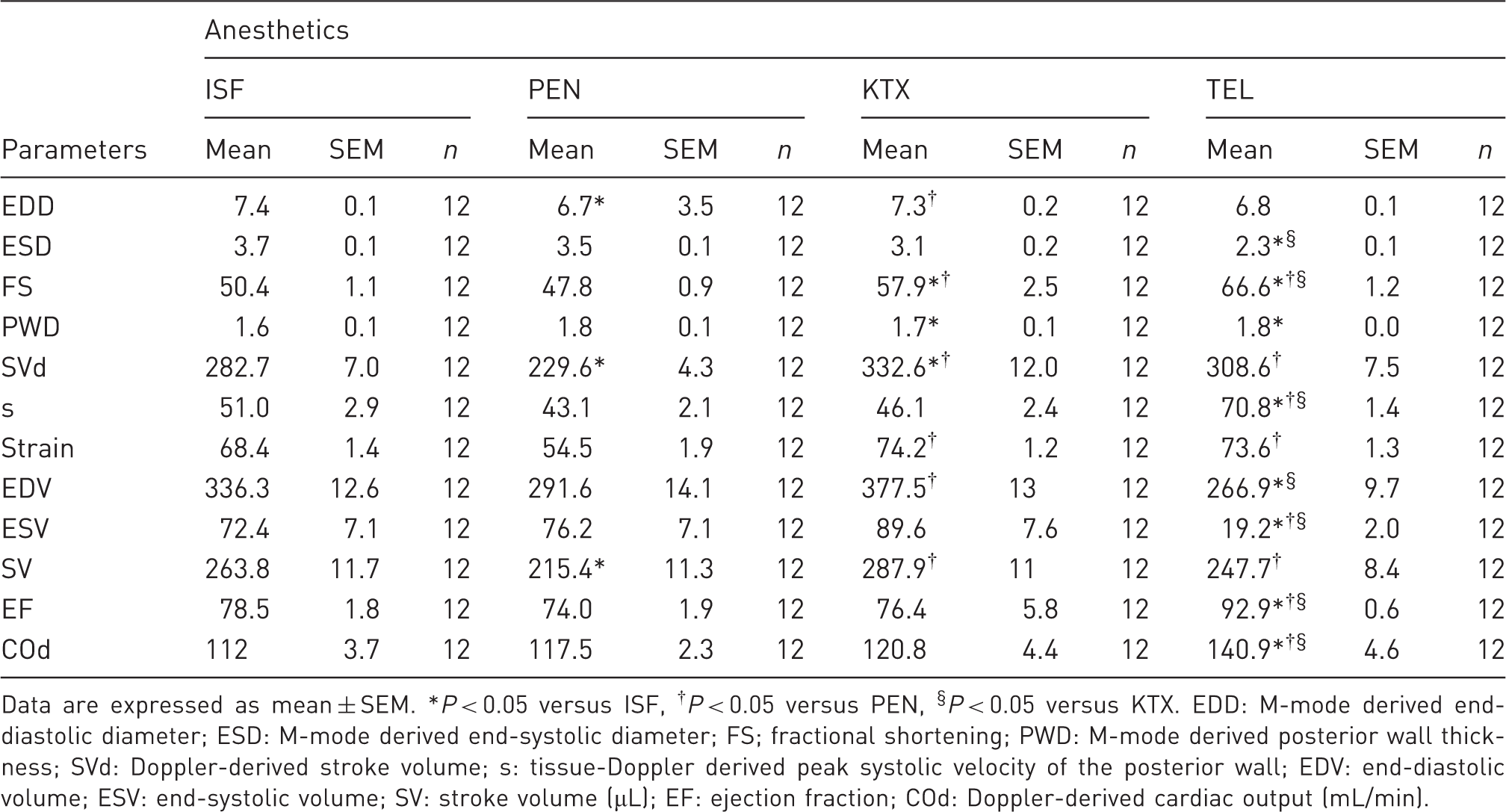
Data are expressed as mean ± SEM. *P < 0.05 versus ISF, †P < 0.05 versus PEN, §P < 0.05 versus KTX. EDD: M-mode derived end-diastolic diameter; ESD: M-mode derived end-systolic diameter; FS; fractional shortening; PWD: M-mode derived posterior wall thickness; SVd: Doppler-derived stroke volume; s: tissue-Doppler derived peak systolic velocity of the posterior wall; EDV: end-diastolic volume; ESV: end-systolic volume; SV: stroke volume (µL); EF: ejection fraction; COd: Doppler-derived cardiac output (mL/min).
Briefly, LV diastolic dimension was lower in the PEN and TEL rats compared with the ISF and KTX rats. FS and EF were significantly higher in the TEL rats compared with the other groups regardless of which estimatory formulas were used (P < 0.05). EF was higher in the KTX rats compared with the ISF and PEN rats. CO was highest in the TEL rats. SV was lower in the PEN rats compared with the ISF, KTX, and TEL rats. Systolic velocity of the posterior mid-myocardial wall was significantly greater in the TEL rats compared with the other groups.
There was a significant dose-dependent relationship between ISF concentration and the degree of cardiac depression (Figures 3a–c). Repeated measures ANOVA also revealed a significantly decreased heart rate and CO at lower body temperatures but did not reveal any significant influence of acute hypothermia on any other echocardiographic indices (Figures 3d and e).
Influence of isoflurane concentration and hypothermia on echocardiographic indexes. Both isoflurane concentration and hypothermia influenced echocardiographic estimates of cardiac output and heart rate. Data are expressed as mean ± SEM. *P < 0.05 for trend. See text for details.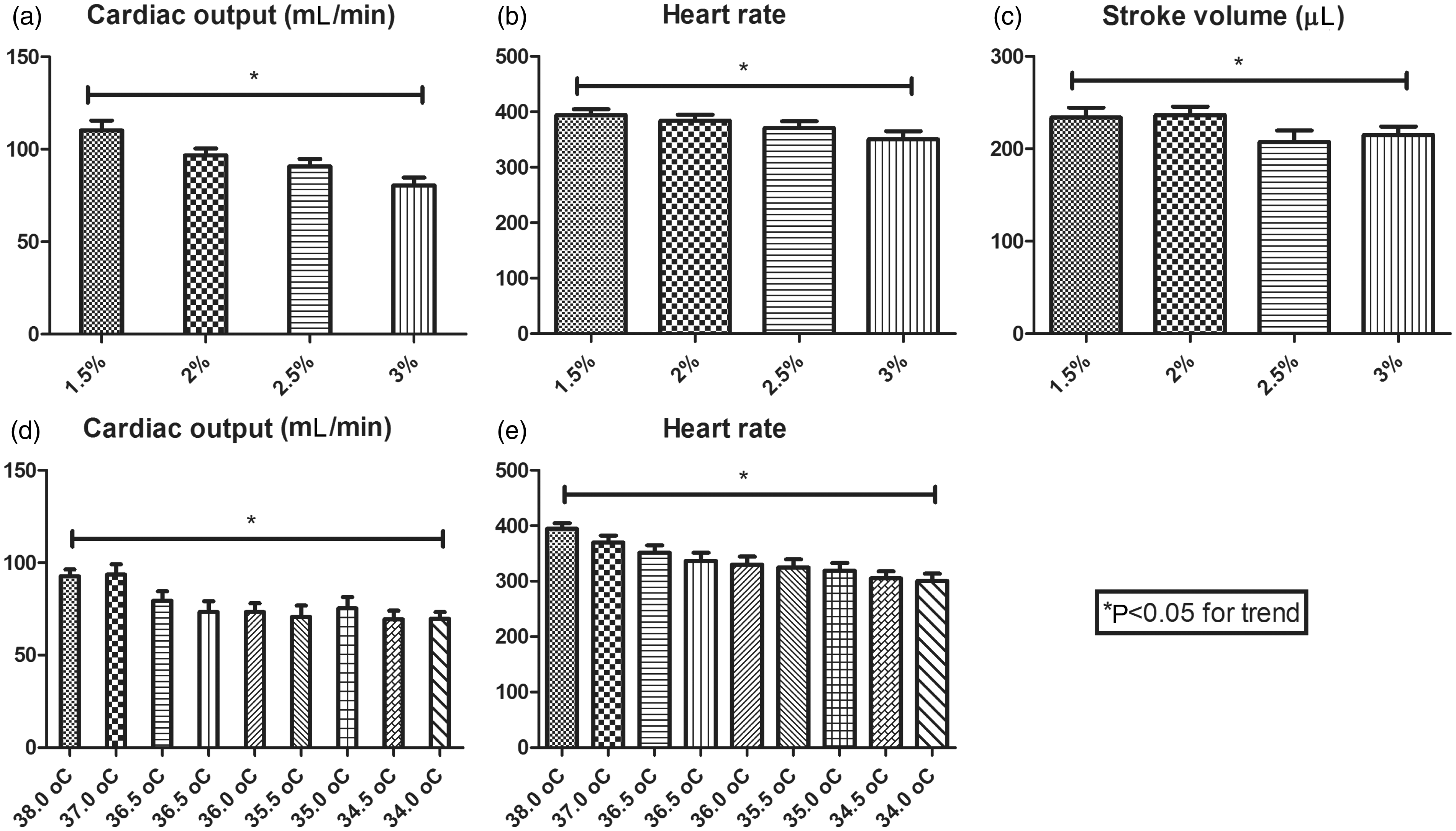
Invasive hemodynamic data
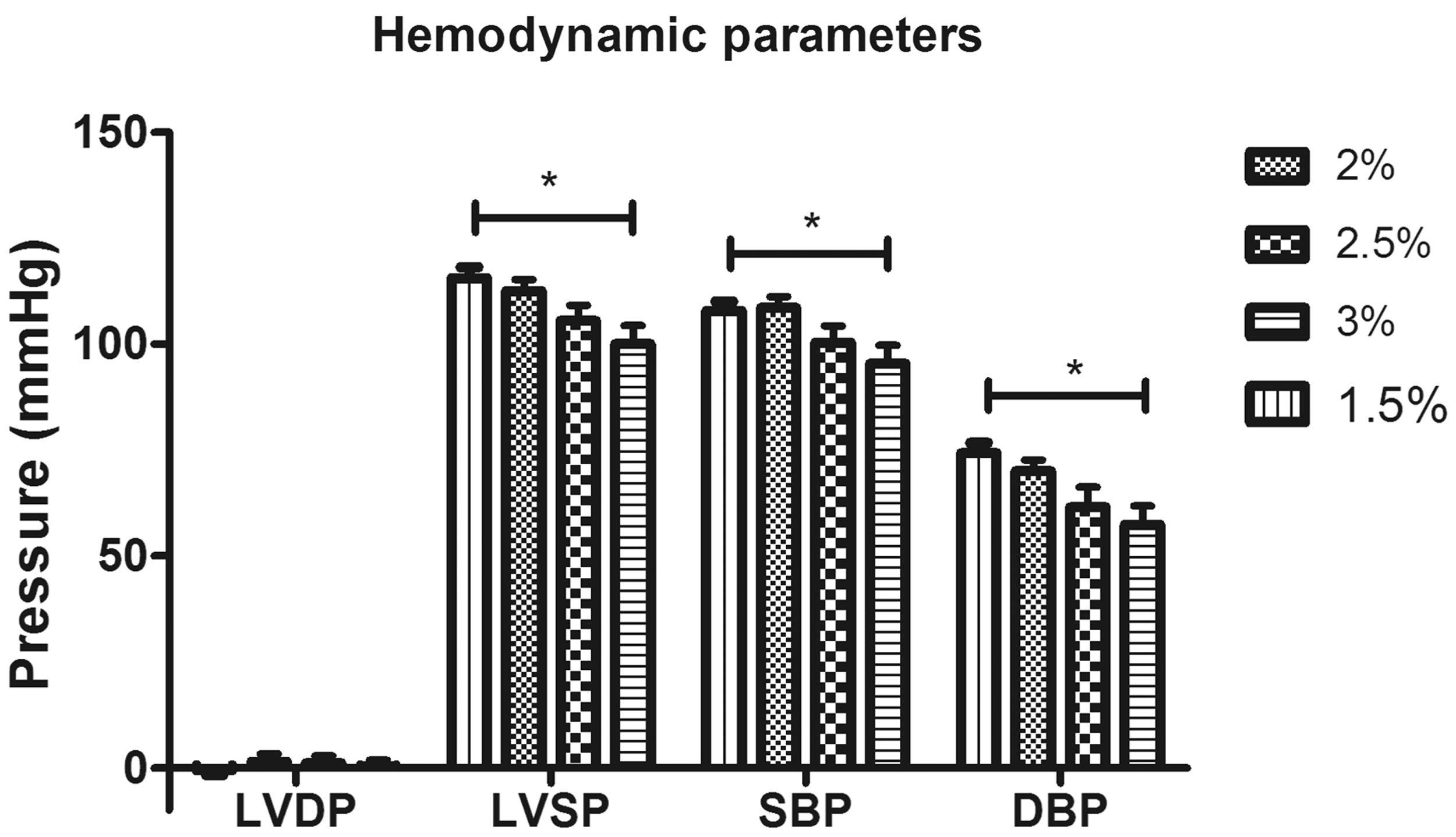
Intraventricular diastolic pressures were similar in all groups. Intraventricular systolic pressures as well as both systolic and diastolic aortic pressures were significantly higher in the TEL rats compared with the other groups. No hemodynamic indices differed significantly among the ISF, PEN and KTX rats (Figure 4). There was a dose-dependent decrease in LV systolic pressure and systolic as well as diastolic blood pressures with increasing concentration of ISF (Figure 5). Hypothermia had no apparent effect on hemodynamic parameters in this study.
Hemodynamic parameters. LVDP: left ventricular diastolic pressure; LVSP: left ventricular systolic pressure; SBP: systolic blood pressure; DBP: diastolic blood pressure. Data are expressed as mean ± SEM. *P < 0.05. See text for details. Influence of increasing isoflurane concentrations on hemodynamic parameters. LVDP: left ventricular diastolic pressure; LVSP: left ventricular systolic pressure; SBP: systolic blood pressure; DBP: diastolic blood pressure. Data are expressed as mean ± SEM. *P < 0.05 for trend, i.e. there was a dose-dependent decrease in LVSP, SBP and DBP. See text for details.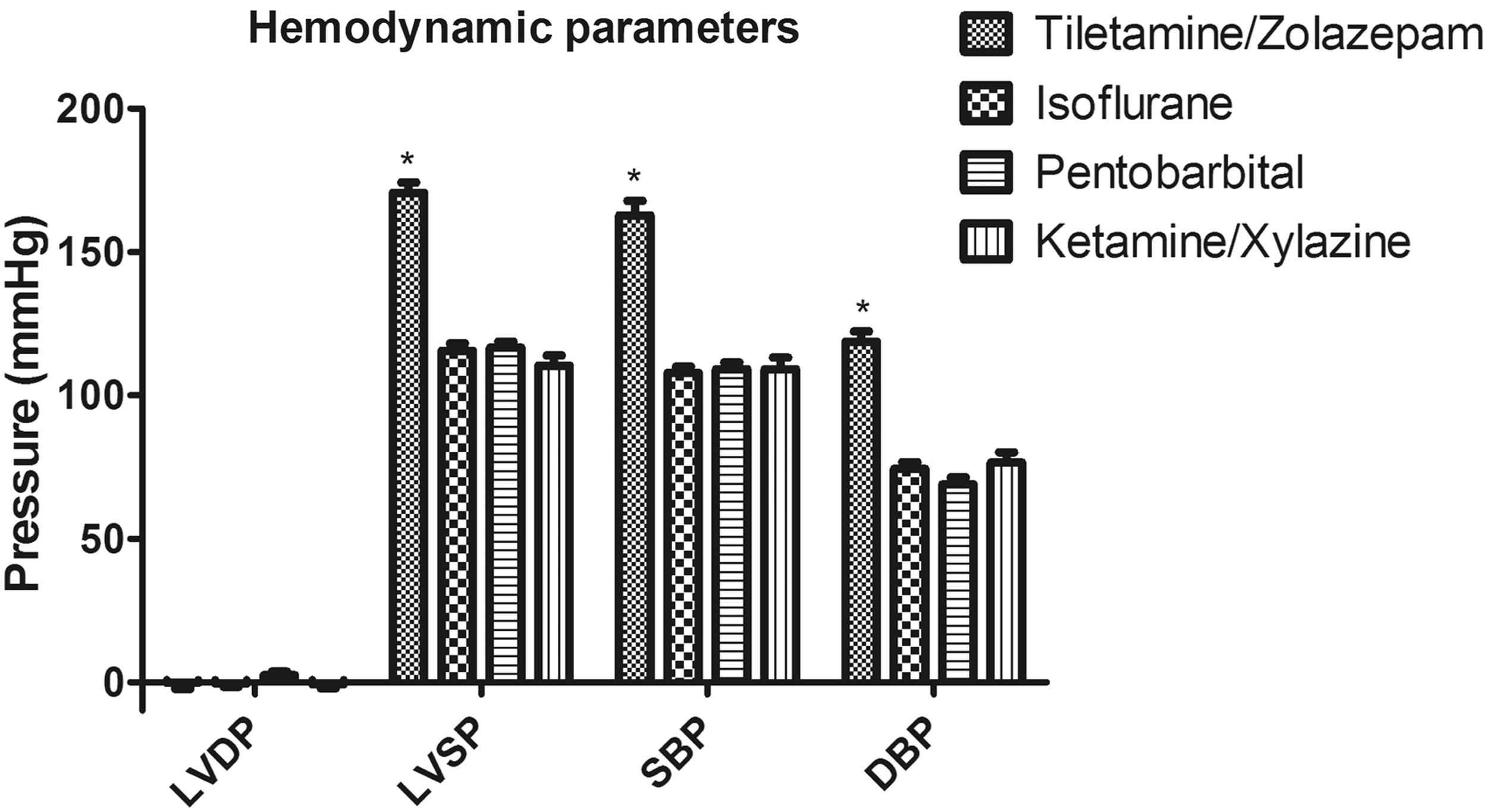
Discussion
In this study we presented echocardiographic and hemodynamic data obtained in rats anesthetized with four of the most common anesthetic agents used in murine models of cardiovascular disease.
Pentobarbital
Our data suggest that low dose (30 mg/kg) PEN is associated with the highest heart rate but with lower indices of cardiac function compared with the other tested anesthetics. Indeed, estimated CO was lowest in PEN rats despite a high heart rate. While it is true that increased heart rate beyond a given limit is often associated with decreasing CO, at the heart rates obtained in this study one would expect an increase in CO with an increasing heart rate (even if SV was to decrease a little secondary to shortened diastole – less time for the ventricle to fill). That is, at the heart rates observed in this study, CO levels in healthy rats should increase with increasing heart rates. 19 Stein et al. have previously reported that PEN preserved cardiac function in rats compared with KTX and ISF. 15 However, although we attempted to use their chosen dose of 25 mg/kg PEN, in our hands adequate anesthesia was not achieved until 30 mg/kg. Stein et al. did observe a dose-dependent decrease in cardiac function but not heart rate at these doses of PEN anesthesia, and this may partly explain the discrepancy between our findings and theirs. However, consistent with our findings, these authors did observe lower cardiac dimensions, at both systole and diastole, in PEN rats compared with ISF and KTX rats. Also consistent with our findings, they noted lower SV in PEN rats compared with ISF rats 15 . It should be noted that Stein et al. studied Fischer 344 rats whereas we studied Sprague-Dawley rats. Between-strain differences may underlie some of the discrepancies between our data and theirs.
Ketamine/xylazine
Rats that were anesthetized on KTX displayed the lowest heart rates. This finding is consistent with previous reports.14,15 Although lower heart rates observed with KTX is sometimes explained by reflex bradycardia (secondary to increased blood pressure/afterload), elevated blood pressure was not observed on hemodynamic recordings. Instead, the relative bradycardia observed with this regimen could be attributed to xylazine’s direct effects on the central nervous system. 16 Also consistent with previous reports were the findings that KTX did not greatly differ from ISF in regard to echocardiographic indices of cardiac function. 14
Isoflurane
In the present study we found that an ISF concentration of 1.5% with a flow rate of 1 L/min consistently yielded adequate anesthesia. Heart rates in ISF rats were intermediate between those obtained in rats anesthetized with PEN and KTX. Hemodynamic indices were similar among ISF, PEN and KTX rats. It is known that ISF causes, among other things, vasodilation. However, this is true also for xylazine and zolazepam and has been suggested for PEN. Although blood pressure was lower than with TEL, blood pressure was not lower with ISF than with PEN or KTX.16,19
Increasing concentrations of isoflurane
Increasing concentrations of ISF were associated with deterioration of cardiac function and decreasing blood pressure. We observed a stronger influence of ISF concentration on cardiac function than that observed in a recent report that studied male Wistar rats. 19 Another argument in favor of carefully controlling the delivered ISF concentration is the observation that increasing ISF concentrations also dose-dependently increase coronary blood flow, a characteristic that may be of relevance in some heart disease models. 20
Tiletamine/zolazepam anesthesia
In this study TEL anesthesia was associated with supranormal blood pressure and high indices of cardiac function. Respiratory rate was highest in TEL rats. Indeed, Saha et al. have previously reported that TEL anesthesia was associated with higher respiratory rate, blood pressure and indices of cardiac function than was PEN or KTX. 16 In our hands TEL anesthesia leads to a hypertonic/hyperdynamic circulatory profile. This should be taken into consideration before choosing TEL as the anesthetic for a given study.
Hypothermia
Lowering body temperature from 38 to 34.5℃ did not significantly affect blood pressure. A significant correlation was found between body temperature and CO. This was mainly due to decreasing heart rate with decreasing temperatures. Similar changes in heart rate have been reported by others. 21
In the present study TEL resulted in significantly higher indices of cardiac function and elevated blood pressures compared with the other anesthetic agents. Although PEN, ISF and KTX differed in ways that could be of relevance to the researcher, e.g. heart rate, they may all have a role in experimental cardiology. The choice of anesthetic agent could instead be based on other agent-specific characteristics, e.g. influence on the preconditioning phenomena, interaction with specific pharmacological agents, or effect of the anesthetic itself on gene and protein expression patterns.22,23
Limitations
Neither blood pH nor degree of hemoglobin saturation was measured in these animals.
This study addressed different anesthetic agents and their influence on parameters of cardiovascular function under baseline conditions. The influence of anesthetic agent on cardiovascular indices may depend on the specific disease model studied. Indeed Plante et al. observed differences between ISF and KTX in rats with aortic regurgitation that were not detectable under baseline conditions. 14 Future studies should address this question.
Conclusion
TEL anesthesia is associated with a hyperdynamic/hypertonic circulatory profile. PEN anesthesia resulted in the highest heart rate, ISF an intermediate rate, and KTX the lowest. It is the authors’ interpretation that neither the data presented in this manuscript nor previously published data convincingly argue in favor of any of the latter three anesthetic regimens.