
Abstract
The purpose of the study was to optimize postoperative comfort in lambs anaesthetized for the surgical creation of scoliosis while maintaining the ewe–lamb relationship to miminize rejection rates. The first management plan produced six scoliotic lambs but intraoperative hypoventilation and hypovolaemia followed by postoperative dyspnoea, pain, monitoring and nursing difficulties, hypothermia, hypoglycaemia and tympany were encountered. Three of eight lambs (38%) were rejected by their ewes. Perioperative management was amended which, combined with improved surgical technique, produced 16 scoliotic lambs. The lambs recovered more rapidly (mean time to standing after discontinuation of anaesthesia was reduced from 12 h to 70 min) and appeared to be more comfortable. No rejections occurred after the refinements were implemented.
Spinal curvatures develop in children when vertebral growth imbalances result in progressive spinal deviations in the coronal (scoliosis), sagittal (lordosis/kyphosis) and axial (rotation) planes.1,2 Untreated children develop thoracic insufficiency with cardiorespiratory failure and ultimately death. 3 Optimal treatment involves harnessing growth 4 rather than forcibly reducing an existing deformation with instrumentation: the latter restricts pulmonary function and retards growth, preventing younger children reaching their full height. Some recently introduced devices appear to function as growth harnesses 5 but testing their pre-commercialization performance requires a valid animal scoliotic model. 6 Despite the questionability of using quadrupeds to study disorders in bipeds, calves, pigs, and goats have been used to model vertebral column surgery for human beings. Sheep vertebrae are similarly-sized to those of children and, it is believed, provide a more valid biomechanical model for studying human spinal disorders. 7
Objections to the use of lambs and kids, whose rapid postpartum growth assures their suitability as models for human skeletal growth disorders, 8 may be countered by providing optimal perioperative care. Problems have arisen after the traumatic avulsion of ventral cervical spinal cord nerve roots in unweaned lambs. 9 There is a conflicting need to provide effective analgesia and surgical conditions in physiologically immature animals that have a high metabolic rate and body water content, yet low body fat, poorly developed thermoregulatory and cardiovascular reflexes and a different response to drugs. Preserving the postoperative ewe–lamb bond is also important. Anaesthetic techniques used in eight-week-old goats undergoing scoliotic surgery have been reported but details of perioperative care are very limited 10 or absent. 11
Altered attitudes to human neonatal pain management 12 have important implications in the perioperative management of young laboratory ruminants, in which pain behaviours are less ostentatious than those of other species. This biological adaptation which serves to reduce the risk of predation probably leads to postoperative pain being under-diagnosed and under-treated.
The creation of scoliotic lambs was expected to be challenging because of the degree of surgical invasion, the anticipated duration, the fact that some animals would be younger than those previously encountered 9 and previously reported ‘serious’ complication rates of 18%. 13 Earlier experiences also prompted reservations with the adequacy of analgesia described by McArthy et al. in kids (four intramuscular [IM] flunixin doses [1.5 mg/kg] and a single [50 µg/kg] butorphanol injection). 10 Consequently, a more aggressive approach involving newer analgesic techniques, combined with greater emphasis on the postoperative needs of both lambs and ewes was planned. This paper describes features of perioperative management that appeared to improve the welfare of lambs and ewes involved in major experimental orthopaedic surgery.
Animals
Twenty-six Scottish Blackface ewe–lambs were purchased with their ewes from a commercial flock. Five weeks pre-purchase the ewes had been wormed and vaccinated against Clostridium perfringens and C. tetani (Lambivac; Intervet, Milton Keynes, UK). All were in good health based on physical examination. The animals were acclimatized in purpose-designed indoor small ruminant housing within the laboratory for >10 days before the first experiment. Housing was two opposing lines of five hurdled pens (1.5 × 2 m) littered with barley or wheat straw. Each lamb and its dam were confined in a single pen: water and hay were available ad libitum and the ewe was provided with commercial pellets (0.5 kg/day in two aliquots). Artificial lighting was maintained from 08:00 until 23:30 h each day. The study was approved by the University's Ethical Review Committee and was licensed under the Animals (Scientific Procedures) Act 1986.
Materials and methods
The lambs were anaesthetized for the surgical creation of a right-sided scoliotic curve. Problems encountered in the first eight lambs (including two fatalities) necessitated radical technical changes. Consequently, the first eight animals became regarded as pilot cases (and designated P1–8).
Surgery involved a dorsal midline skin incision made between T4 and L2 through which the paraspinal muscles were retracted to expose the left lamina of T4–T6 and L1–L2. A 4 mm braided synthetic Dacron tape (Abbott Spine, Austin, TX, USA) was passed under the T5 lamina, tunnelled submuscularly, passed under the L1 lamina and looped back to form a tether. This was held under tension during the next surgical stage. Dissection bilaterally exposed the caudal six ribs. On the right, 4 cm was resected subperiosteally from each rib avoiding breach of the thoracic pleura. On the left, the ribs were bound together with tape (3 mm nylon, Ethicon; Ethicon UK, Livingston, UK) just distal to their angles. The combination of the rib tether and final tightening and suture of the laminar ligament was intended to produce a curvature with approximately a 25° scoliosis.
Pilot study
Pre-anaesthetic medication was midazolam 0.5 mg/kg (Hypnovel; Roche, Welwyn Garden City, UK) and ketamine 5 mg/kg (Vetalar V 10%; Pfizer, Sandwich, UK) injected into the m. semimembranosus/semitendinosus. Anaesthesia was induced with isoflurane (IsoFlo; Abbott, Maidenhead, UK) using a Hall’s pattern face mask and a Bain breathing system. Total gas flow was 3 L/min. When the palpebral reflex disappeared the trachea was intubated under laryngoscopy with a suitable (5 or 6 mm cuffed) endotracheal tube (Portex Blue Line; SIMS Portex Ltd, Hythe, UK). Anaesthesia was maintained with isoflurane delivered in a 1:2 oxygen (O2):nitrous oxide (N2O) mixture. The lungs were ventilated mechanically (Blease-Manley; BME, Chesham, UK) to maintain normocapnia. Neuromuscular blockade was produced with atracurium (0.5 mg/kg) (Tracrium; GlaxoSmithKline, Uxbridge, UK) to improve operating conditions and suppress ventilation. Ringer's lactate solution (Vetivex 11; Dechra, Shrewsbury, UK) was infused (10 mL/kg/h) and during anaesthesia, heart rate (HR), the electrocardiogram (ECG) arterial pressure (AP), end-tidal concentrations of isoflurane (F
P1–8 had a mean age of 4.6 (range 3–6) weeks and weight of 11 (9–17) kg. Operating conditions were adequate in all cases, but two lambs died. Haemorrhage occurred in P2, a lamb weighing 7 kg, which lost 208 mL (50% circulating volume) over 2 h. Infusing 100 mL colloid (Haemaccel; Intervet, Milton Keynes, UK) failed to prevent cardiac arrest. Postoperative dyspnoea occurred in P3 in which asymmetric right thoracic and spasmodic right abdominal wall movements obscured agonal breathing patterns. Post-mortem examination revealed total lung collapse on the left side where the tether had been over-tightened.
Other complications were: pain on midazolam/ketamine injection; difficulty in postoperative pain assessment; nursing difficulties; prolonged recoveries from postoperative hypothermia, tympany and inappetance. Intraoperative hypoventilation occurred in P1–5. Lambs P4, P5 and P6 were rejected by their ewes and required hand-rearing. Recovery times to first unassisted standing ranged from 12 to 20 h, No lambs from the pilot study were reused.
Main study
Major changes to lamb and ewe management were made after the pilot study. Forty-eight hours pre-surgery, the lambs' operation sites were clipped, sponged with surgical disinfectant (povidone iodine; Vetasept, Animalcare, York, UK) and covered with conforming bandage (Vetrap; 3 M, Bracknell, UK) to familiarize the ewe with the lamb’s postoperative appearance and smell and so reduce rejection risk. Antibiosis was started 24 h pre-surgery with IM oxytetracycline (20 mg/kg IM, Engemycin; Intervet, Milton Keynes, UK). Two hours pre-surgery the ewes were milked to provide an alternative postoperative food option to a proprietary milk replacer. Four hundred millilitres of maternal blood was also collected at this time and stored at room temperature (Teruflex; Terumo, Egham, UK). The lambs were allowed milk until separated from their ewes for pre-anaesthetic medication. This was changed to medetomidine (10 µg/kg, Domitor; Pfizer, Sandwich, UK) injected into the epaxial muscles. The lambs were reunited with their ewes until they became recumbent.
When profound sedation and recumbency were present, anaesthesia was induced with isoflurane or sevoflurane (Sevoflo; Abbott, Maidenhead, UK) delivered in 100% O2. After intubation, anaesthesia was maintained with the same agent used for induction: end-tidal isoflurane (F
Before surgery, meloxicam (0.6 mg/kg) and morphine (0.5 mg/kg) were injected IV. A constant rate infusion of ketamine (10 µg/kg/min) was delivered by a syringe driver (Graseby MS16A; Smiths Medical, Ashford, UK) after a loading dose (1 mg/kg) had been given. Ketamine (0.3 mg/kg) was available in case inadequate anaesthesia or analgesia was identified. Before wound closure, bupivacaine (1.5 mg/kg) was sprayed on to the operation site using a mucosal atomization device (Wolfe Tory Medical, Waukesha, WI, USA).
A 22 gauge cannula was placed in the auricular artery for collecting blood for gas analysis (i-STAT, Abbott Diagnostics, Dartford, UK) and monitoring AP. A human earlobe probe attached to the tongue was used for pulse oximetry (SpO2). The oesophageal and rectal temperatures were monitored with thermistors advanced per os to the heart base and per rectum, respectively. An attempt to maintain normothermia was made by increasing the ambient temperature to 22–24℃. A warming pad, and a heat and moisture exchange filter (Hydro-Therm II HME; Intersurgical Ltd, Wokingham, UK) were also used.
A 22 gauge cannula was placed in either the cephalic or a lateral saphenous vein and Ringer’s lactate solution infused at 10 mL/kg/h. Arterial hypotension (mean AP < 55 mmHg) was treated with ephedrine (0.1 mg/kg IV, ephedrine hydrochloride injection 3%; Martindale Pharmaceuticals, Brentwood, UK) or dextran (4 mL/kg, Dextran 40; Baxter Healthcare, Thetford, UK).
After venous access was established blood was taken and cross-matched with a sample collected earlier from the ewe using a technique described by the Animal Health Trust, UK (http://www.aht.org.uk/cms-display/diag_clinpathis1.html).
Lacrilube (Allergan Pharmaceuticals, Westport, Ireland) was placed hourly into the conjunctival sacs for corneal protection.
Haemorrhage was quantified by weighing bloodied swabs on a precision balance PGW 153 e (Precision Laboratory Balances, Milton Keynes, UK). One millilitre of blood was taken to weigh 1.3 g. This value is greater than that reported for sheep (1.08 g) 16 but was applied to compensate for evaporative plasma water losses that were likely to have occurred before measurement. The blood volume lost (Ve) through surgical suction was estimated by recording the volume in the suction jar (V), measuring in vivo and in vitro haematocrit (Hct) and applying the equation: Ve = (in vitro Hct/in vivo Hct) × V.
Surgery was performed with lambs in the prone position supported by a vacuum pad (Buster vacusupport; Krusse A/S, Marslev, Denmark) shaped to contour the animal’s abdomen in a way that minimized intra-abdominal pressure and so reduced surgical haemorrhage. Cefuroxime (20 mg/kg IV, Zinacef; GlaxoSmithKline, Uxbridge, UK) was given immediately before surgery and continued at 8 h intervals for four days. Metronidazole (20 mg/kg, Metronidazole 0.5%; Baxter Healthcare, Thetford, UK) was also given for five postoperative days.
When surgery ended, ketamine and inhaled anaesthetic administration were discontinued and the trachea was extubated once laryngeal reflexes were forceful. The leads for physiological monitoring were left in situ while the lamb was transferred from the operating table to a sling (Figure 1). The slung lamb and multichannel monitor were then moved into a room next to the operating theatre where O2 was available and where the lamb's ewe waited in a divided stall. The sling was positioned in the stall in a way that allowed partial contact between the two animals. The lamb's section was bare-floored but warmed with infrared (IR) lamps and the sling was draped with bubble wrap under which a proprietary hair drier blew warm air. The ewe's section of the stall was littered with straw and equipped with food and water bowls.
A purpose-built sling for recovering lambs after major surgery. The frame accommodates differently sized subjects. Height is readily adjusted (long slider). The frame’s width ensures the sling is taut enough for sternal support, but does not restrict breathing. Short slider adjustment allows the unconscious lamb’s head to rest in a way that allows single-handed tracheal intubation when necessary. The frame was a 5 cm stainless steel box and could be heat-sterilized. The sling was made of washable linen toweling. All measurements are in centimetres.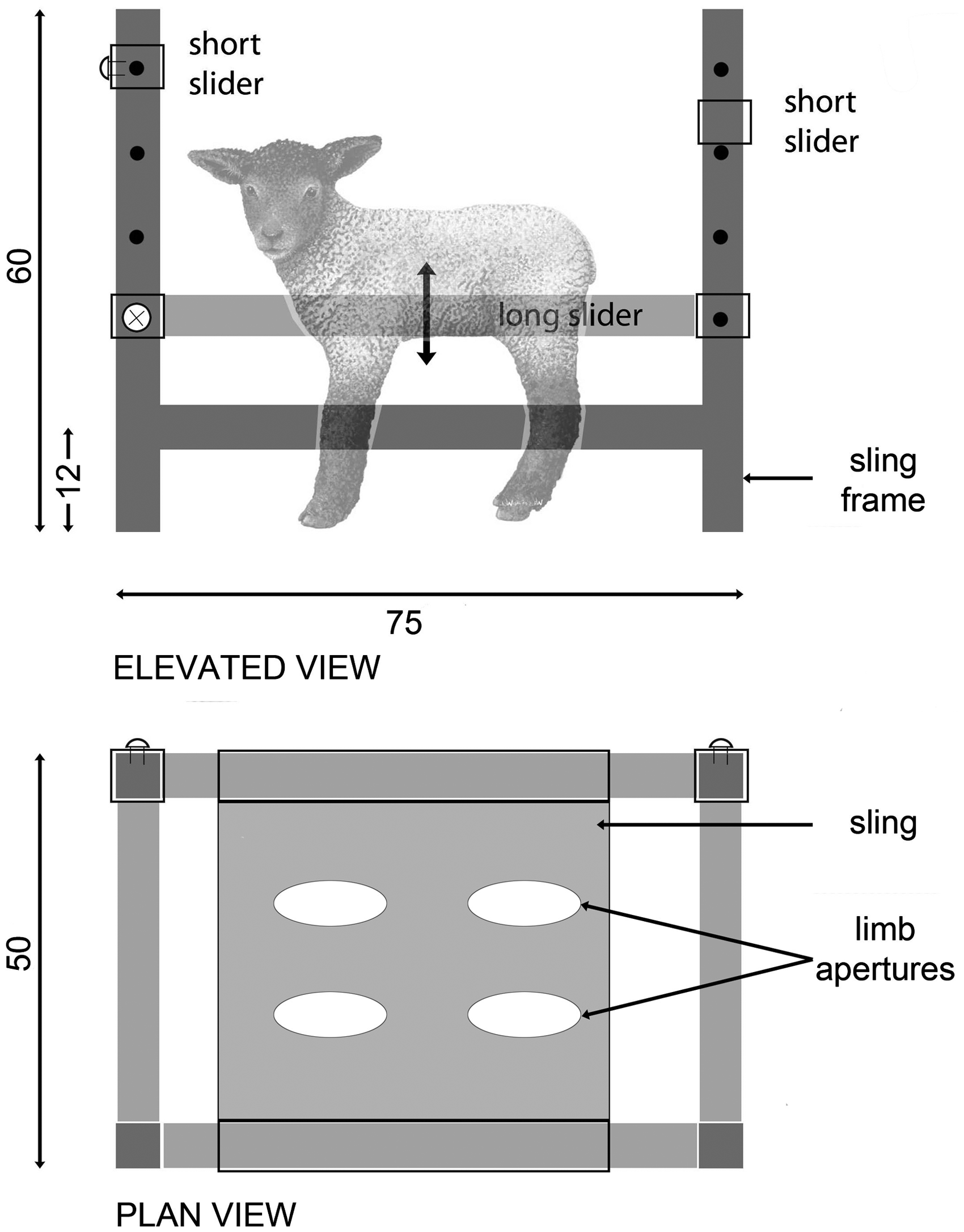
Monitoring physiological variables continued in recovery along with fluid infusion. Oxygen was delivered by mask only when pulse oximetry and other signs convincingly indicated its need. Arterial samples were taken for blood–gas analysis whenever abnormal breathing patterns coincided with SpO2 values <0.9. Bottled ewe's milk or milk replacer was offered at hourly intervals for the first 3 h, when venous blood samples were taken to monitor blood glucose levels (One-Touch Ultra 2; LifeScan Inc, Milpitas, CA, USA).
Signs of postoperative pain (plaintive bleating, bruxism, depression, disinterest in the ewe, trembling, reflex ‘cringing’ on attempts to stand) were treated with morphine (0.5 mg/kg IV) or buprenorphine (20 µg/kg IM) and/or ketamine (0.3 mg/kg/h) depending on the timing of previous doses.
Monitoring and O2 delivery continued until the lamb could stand within the sling when the arterial cannula was removed. Fluid infusion, maintained at 10 mL/kg/h during recovery was discontinued when bottled milk was imbibed readily. At this time, the barrier between the stalls was removed and the ewe was allowed access to the lamb. The animals' behaviours were monitored directly for at least 20 min after this. At least one venous cannula was retained for the first 24 postoperative hours.
Once the lambs were standing unaided and interacting normally with their ewes they were removed from the sling, but most initially did not suck normally and required some bottled ewe’s milk or replacer. An observer was continuously present during the first hour of recovery but withdrew thereafter to monitor the animals on closed circuit television (CCTV).
Meloxicam was injected once daily for 3–7 days and buprenorphine was given according to individual needs. If the latter was ineffective, IM morphine at doses up to 0.5 mg/kg were used instead. The ewe–lamb pairs were allowed into a grassed paddock from the third postoperative day if the weather was fine.
Results
The revised technique produced 18 scoliotic lambs, with a more rapid recovery from anaesthesia 14 (70–90 min to stand), and a briefer interval until successful reunification and with no lamb rejection. Two lambs died however from peri-acute postoperative C. perfringens endotoxaemia. 17 The median age of the animals studied was four weeks (range 3–6 weeks) and their body mass 12 ± 2.3 kg (means ± standard deviation [SD]).
Medetomidine (10 µg/kg) injection produced little reaction and profound sedation within 15 min in all the lambs. Mask induction was well-tolerated and effective; tracheal intubation was normally completed in 2–3 min.
14
The anaesthetic produced adequate surgical conditions in all the lambs with a median (min–max) recorded F
The Penlon ventilator achieved normocapnia in all the lambs without complication or modification. Mean ( ± SD) fr of 17 ± 3 breaths/min and a median (min–max) peak inspiratory pressure (PIP) of 22 (16–30) cmH2O resulted in a median V
Haemodynamic variables were stable in all cases, although all but one were hypotensive. Ephedrine and/or dextran were effective on all occasions. After treatment for hypotension, the mean intraoperative HR was 128 ± 23 beats/min while systolic, mean and diastolic AP were 88 ± 11, 67 ± 12 and 56 ± 12 mmHg, respectively.
Hourly arterial blood analysis revealed a mean ( ± SD) arterial pH of 7.43 ± 0.05, base excess (BE) of 4.7 ± 32 mmol/L and HCO3– of 29.0 ± 3.2 mmol/L. Median (min–max) lactate and glucose were 1.5 (0.72–2.95) and 5.75 (2.3–15.2) mmol/L, respectively.
No in vitro reactions were observed on mixing blood from 18 ewe–lamb pairs, and no adverse effects were observed in the single lamb requiring transfusion (which received 25 mL/kg of maternal blood at 0.5 mL/kg/h rising to 5 mL/kg/h after 30 min).
The mean ( ± SD) rectal temperature recorded at end surgery was 38.69 ± 0.5℃.
As the study progressed, reduced surgery times caused a corresponding reduction in anaesthesia time, with mean values of 125 ± 24 min and 214 ± 45 min (from induction to the discontinuation of isoflurane), respectively. No further problems were encountered with postoperative dyspnoea and postoperative blood–gas values indicated adequate pulmonary function and levels of ventilation.
Signs of postoperative pain were observed in most of the lambs during early recovery and were treated with variable success. The intensity and duration of pain signs diminished as surgery became briefer and less traumatic. Postoperative monitoring, fluid and O2 administration, general nursing and maintaining normothermia were greatly facilitated by the sling (Figure 1). The lambs and ewes were reunited on average 70 min (range: 20–637) after anaesthesia was discontinued.
The animals' behaviours normalized rapidly in the first 20 min after reuniting. No rejections occurred in the second group and no lambs were unable or disinclined to suck naturally. Only one lamb in 18 required additional morphine and no cases of tympany were observed. All the lambs were behaving, suckling and moving normally within 48 h of recovery. This process was accelerated by allowing the ewe–lamb pairs access to pasture.
Modest abdominal gas distension was detected during recovery and relieved by trochar (P2) and stomach tube (P8).
Discussion
Management changes during the study’s course were successful on the basis of lower morbidity, mortality, and ewe rejection rates, with more rapid and more comfortable recoveries. Therefore, the changes were regarded as a refinement of methods described previously. 9 Nevertheless, two lambs unexpectedly died of clostridial enterotoxaemia. 17 It is possible that lamb vaccination, in addition to ewe vaccination, might have provided higher levels of protection after colostral immunity had waned 18 and might have prevented losses in the main study.
Maximizing the ewe’s involvement in her offspring’s perioperative care reduces the cost of human assistance. However, this relies on the early and complete acceptance of the lamb. Any human intervention, such as that required for analgesic administration, will obviously threaten the ewe–lamb bond. In this study, effective analgesia was prioritized on practical, as well as welfare, grounds. Postsurgical lumbar pain could conceivably have reduced the lamb’s ability to stand and ‘bunt’ the udder to promote milk ‘let-down’. The literature does not give guidance to help solve this problem. The report of a caprine scoliosis model (McCarthy et al.) 10 has limited management details of drugs and doses for anaesthesia and postoperative analgesia (vide supra) but provides no information on the comfort achieved and does not describe the dams’ role. Other reports of scoliotic 4–8-week-old kids give no information on analgesics or the role of the dam.11,13
In our study, the anaesthetic provided adequate surgical conditions and uncomplicated recoveries. Medetomidine injected IM caused less reaction than the ketamine–midazolam mixture probably because ketamine causes muscle damage.
19
Ventilation was more easily controlled with the Penlon Nuffield 200. The Blease-Manley device required a ‘controlled leak’ to restrict peak inspiratory pressures to 20 cmH2O when gas flows and ventilator settings were producing normocapnia. The ‘leak’ – an adjustable pressure limiting valve incorporated into the inspiratory limb – needed constant adjustment and waste gas scavenging. Despite this, limiting lung inflation pressure to 20 cmH2O failed to achieve normocapnia in P1 and P2, even when gas flows exceeded the minute volume of ventilation (V
Measures taken after P2’s demise from haemorrhagic shock, i.e. contouring the surgical mattress and refining surgical technique, prevented further losses from hypovolaemia. Only one lamb went on to require a maternal blood transfusion. This animal lost approximately 25 mL/kg blood during surgery which exceeded the 15 mL/kg, that would be expected to compromise circulation in a conscious adult sheep. 21 A literature review conducted after P2’s loss failed to confirm meloxicam’s potential anticoagulant effect, so the drug was not withheld from subsequent cases.
Haemolytic tests are preferred for grouping sheep blood, except factor D 22 (Nguyen & Bunch) whose antigens are detected by agglutination. 23 The lack of commercial blood-typing cards or gels for sheep precluded the straightforward characterization of the ewe and lamb blood in the current study so transfusion reaction risks were reduced by cross-matching the blood of each ewe–lamb pair. No adverse in vitro reactions were seen in the 18 cross-matches, and no adverse reactions occurred in the single lamb receiving transfusion.
The fatal postoperative dyspnoea occurring in P3 has also been reported in caprine scoliotic models with postoperative respiratory failure in 8% 13 and 7% 11 of animals. In the main part of the current study, complications were avoided by more judicious tensioning of the surgical tether. It could still be expected that rib resection and tethering on the convexity and concavity of the curve respectively would significantly inhibit ventilatory function. In essence the lambs had a flail chest wall segment on one side and limited capacity to ‘over-expand’ the lung on the other. Although not measured, the dead space could increase, possibly by as much as 50%. Ventilatory function was also monitored more effectively using hourly arterial blood–gas analysis in preference to continuous pulse oximetry.
While nursing and monitoring reunited lambs required additional staff for ewe restraint, early reunification was prioritized. However, identifying the ideal time for this was complicated by the difficulty of interpreting the ewes’ intent. This in turn was complicated by the presence of people. Such difficulties contributed to three rejections during the pilot study. Lambs began vocalizing in early recovery which elicited vocal responses in the ewes and prompted reunification. However, some lambs vocalized while recumbent, which caused two ewes to vigorously ‘paw’ their offspring in an apparent attempt to prompt standing and movement, but with a force that threatened the surgical site. By contrast, the ewes of P3 and P4 allowed suckling within 2–3 h of recovery from anaesthesia while P5’s dam persistently head-butted its offspring, which had to be removed and nursed manually. It became apparent during the recovery of P6 that continuous human presence contributed to ewe anxiety and probably lamb rejection.
Measures taken to reduce maternal rejection, i.e. familiarizing ewes with their lambs' postoperative state, minimizing postoperative human interference using CCTV and reuniting slung lambs as soon as possible were successful because no rejections occurred in the main study. That rejections were not encountered in another study using ewes of a different breed 9 suggests a problem with the mothering characteristics of the Scottish Blackface. However, some pilot lambs of the current study were, if anything, over-mothered, i.e. they were vigorously ‘pawed’ by their dams.
The potential variation in mothering qualities within and between breeds coupled with variation in the robustness of lambs complicates the choice of any specific breed for experimental surgical studies. However, on the basis of the experiences described, ewe familiarization, early reunification and remote postoperative surveillance are strongly recommended.
The sling, as shown in Figure 1, provided numerous benefits. Unconscious lambs could be moved from the operating table while attached to the breathing system and physiological monitors, saving time and allowing uninterrupted monitoring. By restricting lamb movement, the physiological monitors, fluid and O2 administration were resistant to disruption. The sling allowed more intimate access to the lamb by the ewe while protecting the former from over-attention. By supporting the lamb, the sling probably relieved tension in the paraspinal muscles and so reduced pain, both at rest and during attempts to stand that would otherwise have been necessary. By elevating the animal from the floor, the sling assisted in keeping vascular access points clean and improved the ergonomic efficiency of nursing. The attendants did not have to repeatedly kneel, and the animal and instrumentation could be moved more easily. The sling’s design also contributed to restoring normothermia.
Assessing postoperative pain was difficult and there was variation in perceived comfort levels in animals receiving similar analgesics. Signs of discomfort were usually presaged by generalized shivering early in recovery. Most lambs bleated before rejoining their ewes, when they became silent (indicating that separation may have been causative) but those in discomfort continued to be depressed, reluctant to feed and disinterested in the surroundings. Bleating could be stopped by re-infusing ketamine or injecting morphine or buprenorphine, but whether this was the result of sedation or enhanced analgesia was impossible to determine. Strong, sustained bleating had the dubious benefit of demonstrating that the surgically-created flail segment was of limited functional significance.
Under non-laboratory conditions, vocal behaviours between ewes and lambs are breed-dependent and serve several purposes including location after separation. 24 Lambs also vocalize in response to acute pain caused by castration and tail docking, although this does not always correlate with apparent intensity and its expression varies greatly among individuals. 25 However, there appears to be little information on the relative contribution of separation versus pain to vocalization during castration or docking, which is unfortunate as such information would have been of considerable use in the current study. Until this becomes established, we propose that the absence of postoperative vocalization in separated or reunited lambs is no assurance of an absence of pain.
Other (non-vocal) signs of pain lambs related to husbandry procedures, e.g. castration, have been extensively described in lambs. 26 These, however were of limited use in the current study because the pain was different as it arose from more extensive musculoskeletal injury inflicted over a greater area.
Aggressive analgesia did not appear to cause problems and no signs of overdose or adverse reactions were observed. However, some lambs responded disappointingly to extradural drugs. For example, P7 received 2 mL (0.25 mg) bupivacaine mixed with 0.2 mg/kg morphine before recovery yet looked depressed and adopted a torticollic position. Two additional epidural injections (same drugs and doses) were without apparent effect. However, 6 h later P7 made a full and rapid recovery, behaving normally thereafter. Improved responsiveness of lambs to analgesics in the main, compared with the pilot study, probably resulted from an improved surgical technique and associated reduction in surgery time. Probably the aggressive polymodal pain therapy, with some elements being given pre-emptively, also helped.
The measures we adopted to limit hypothermia were successful in the main study. This was important because the postoperative hypothermia that occurred in all the pilot lambs appeared to retard recovery. Cranial nerve reflex recovery only began once re-warming achieved rectal temperatures >35℃. We observed that withholding oxygen from the inspired breath in lambs with rectal temperatures between 32 and 35℃ resulted in tachycardia, rapid falls in SpO2 and parallel rises in F
Finally, the variability in the ewes’ readiness to suckle and the lambs’ inclination to imbibe complicated the maintenance of stable postoperative blood glucose levels. Our recorded values ranged from 2.3–15.2 with a mean of 5.7 mmol/L. The published blood glucose values for 4–8-week-old lambs range of 3.7–4.8 mmol/L 27 suggests that most of ours were hyperglycaemic. This perhaps was not unexpected. The postsurgical stress response in preterm humans 28 and lambs 29 involves plasma glucose surges that parallel plasma cortisol levels and broadly reflect surgical trauma. 27 These factors prevailed against attempts to maintain normoglycaemia and so the objective re-focused on ensuring that the lambs periodically drank milk, with a rationale that this would promote sucking and ewe–lamb bonding, while providing glucose in the animals that were hypoglycaemic. Consequently, bottled ewes’ milk, or milk replacer (approximately 180 mL) was provided at 3 h intervals to lambs which were not allowed or unable to suckle. Lambs refusing the bottle received 40% glucose (15 mL) IV over 10 min. Concerns with osmotic diuresis were dispelled by infusing crystalloid solution at supra-maintenance levels. The cause of the noted abdominal gas distension in P2 and P8 was unknown as the two animals were managed no differently from those recovering without gastrointestinal disturbances.
Normal ewe and lamb behaviours were almost completely restored when the animals were allowed on to pasture. Under these conditions, lambs that had surgery only three days earlier displayed sucking and play behaviours that were indistinguishable in terms of complexity and vigour from those demonstrated by lambs which had not undergone surgery. Exposure to a grassy environment also appeared to accelerate the restoration of normal ewe–lamb behaviours which in some cases appeared to be subdued by indoor conditions.
In conclusion, experiments involving major surgery on lambs compromise the welfare of both the lambs and their ewes. We have outlined specific measures that will limit complications and increase the likelihood of rapid and comfortable recoveries. Ewe and possibly lamb vaccination against clostridial disease is strongly recommended.
Footnotes
Funding
The study was funded by the Medical Research Council, UK (MRC G0700918).