
Abstract
Short-term anaesthesia of the pregnant ewe may be required for caesarean delivery of a preterm foetus within a research protocol. The aim of this study was to evaluate and compare the acid-base and haematological status of the ewe and foetus at the time of surgical delivery by collecting maternal and foetal arterial blood samples. Fifteen date-mated singleton-pregnant merino cross ewes at 122.0 (±0.5) days of gestation were anaesthetised with a combination of midazolam (0.5 mg/kg) and ketamine (10 mg/kg) by intravenous injection. A subarachnoid injection of lidocaine (60 mg) was given to desensitise the caudal abdomen. Supplemental oxygen was not provided, and an endotracheal tube was not placed in the ewe’s trachea. The development of maternal respiratory acidosis (hypercapnia) and hypoxaemia was anticipated. Samples of arterial blood for blood gas analyses were collected simultaneously from the radial artery of the ewe and the umbilical artery of the foetus immediately after delivery. The results from the maternal blood samples were within the normal range for pH, partial pressure of carbon dioxide in arterial blood (PaCO2), base excess, glucose, lactate, haematocrit and haemoglobin concentration. The maternal partial pressure of oxygen in arterial blood (PaO2) revealed hypoxaemia: 45.2 (41.1–53.4) mmHg. Foetal arterial blood gas analysis revealed hypoxaemia (15.0 ± 3.1 mmHg) and hypoglycaemia (0.1 (0.1–1.1) mmol/L). The benefit of providing supplemental oxygen and/or placing an endotracheal tube must be carefully weighed against the benefit of saving time when prompt delivery of the foetus is planned. In this study the pregnant ewe developed severe hypoxaemia, and this abnormality may have contributed to a low foetal PaO2.
Introduction
Short-term general anaesthesia for caesarean delivery of preterm lambs, prior to euthanasia of the ewe, is embedded in the study protocols of research groups investigating the foetal consequences of various maternal exposures.1-5 In these protocols the pregnant ewe is anaesthetised for a brief period before surgical delivery of the foetus and euthanasia. The prompt delivery of the foetus is essential to optimise its physiological status and prevent alterations from the normal state for parameters such as blood pressure, blood gas values and heart rate. To this end it has become standard in some of these protocols to streamline processes: supplemental oxygen may not be delivered and a maternal endotracheal tube may not be placed.
The physiological consequences of general anaesthesia of pregnant sheep without oxygen supplementation or protection of the airway are largely unknown; hence the aim of this study was to evaluate and compare the acid-base and haematological status of the ewe and foetus at the time of surgical delivery by collecting maternal and foetal arterial blood samples for analysis. The development of maternal respiratory acidosis (hypercapnia, partial pressure of carbon dioxide in arterial blood (PaCO2) > 45 mmHg) 6 and hypoxaemia (partial pressure of oxygen in arterial blood (PaO2) < 90 mmHg when breathing room air) 6 was anticipated.
Animals
Fifteen date-mated singleton-pregnant merino cross ewes were used in this study. Prior to transport to the University farm the sheep were inspected by a veterinarian on the farm of origin in the south west of Western Australia to ensure the animals were healthy and in good body condition (body condition score 2.5–3.5 (max 5)). The ewes had been treated for intestinal parasites (abamectin, oxfendazole and levamisole) twice during pregnancy and had been vaccinated against Ovine Johne’s disease (Mycobacterium paratuberculosis) as lambs. After arrival at the University farm the ewes were monitored for body weight, body condition, food and water intake, and general wellbeing twice a week. The ewes had been introduced to the university farm paddocks at least 1 month prior to the study and moved from the paddock to the indoor shed environment 24 hours prior to anaesthesia. The ewes were fed a diet of pasture supplemented with oaten hay and approximately 40 g/head/day pellets (Macco Feeds 707 pellets). The pellets were formulated to meet the requirements for growth in prime lambs and contained 16% protein in dry matter, 12 MJ of metabolisable energy/kg of dry matter, four times the recommended minimum level of cobalt and selenium, and three times the recommended minimum level of zinc (John Milton, personal communication). Neither food nor water was withheld prior to anaesthesia.
Materials and methods
This study was an opportunistic study performed on blood samples collected from animals enrolled in studies approved by the Animal Ethics Committee of the University of Western Australia in accordance with the Australian Code of Practice for the Care and Use of Animals for Scientific Purposes. 7
The pregnant ewes were anaesthetised with a combination of midazolam and ketamine by intravenous injection. An initial dose of midazolam (0.5 mg/kg, Midazolam Apotex solution for injection 5 mg/mL, Apotex Pty Ltd, NSW, Australia) and ketamine (10 mg/kg, Ilium Ketamil Injection 100 mg/mL, Troy Laboratories, NSW, Australia) was administered as an intravenous bolus into a catheter (18 GA, 1.88 IN, Angiocath Becton Dickinson, Brazil) in a cephalic vein. The drugs were combined in the same syringe immediately prior to injection in a 50:50 volume combination. Once the ewe was adequately anaesthetised it was positioned in right lateral recumbency for subarachnoid injection of lidocaine (3 mL, Ilium Lignocaine 20 mg/mL, Troy Laboratories, NSW, Australia), between lumbar vertebrae 6 and 7 or at the lumbosacral junction, with a spinal needle (0.9 × 90 mm Becton Dickinson Spinal Needle, Madrid, Spain). Additional doses of midazolam and ketamine were administered intravenously if signs of inadequate anaesthesia were observed (brisk palpebral reflex, increased muscle tone, increased respiratory effort and/or frequency, gross purposeful movement) by an experienced veterinary anaesthetist. A peripheral arterial pulse was palpated intermittently during the procedure and spontaneous ventilation was observed continuously.
The animal was placed in dorsal recumbency with the neck extended and the head positioned below the edge of the table to facilitate drainage of saliva or regurgitated rumen contents. A ventral midline laparotomy and hysterotomy was performed for delivery of the preterm lamb foetus. A tracheostomy tube was inserted into the foetal trachea and the foetus was delivered and managed according to study protocol. The foetus was mechanically ventilated and monitored intensively for 30 minutes and continuous measurement of arterial blood pressure, oxyhaemoglobin saturation, heart rate, temperature and airway pressure was performed. Samples of arterial blood were collected simultaneously from the radial artery of the ewe and the umbilical artery of the foetus immediately after delivery. These samples were collected into heparinised syringes (RapidLyte Arterial Line Draw Sampler, Siemens Healthcare Diagnostics Pty Ltd, Victoria, Australia) and analysed within 15 minutes (RapidLab 1265; Siemens Healthcare Diagnostics). Blood sample analysis yielded a range of variables: pH; PaCO2 (mmHg); PaO2 (mmHg); base excess (mmol/L); haematocrit (%); glucose (mmol/L), lactate (mmol/L) and haemoglobin (g/L) concentrations. The ewe was euthanased with intravenous pentobarbitone (160 mg/kg, Lethabarb 325 mg/mL, Virbac, NSW, Australia). The foetus was also euthanased with intravenous pentobarbitone at the end of the study protocol 30 minutes after delivery. Death was confirmed by ensuring there was no spontaneous ventilation, no heartbeat and no corneal reflex.
Data were tested for normality with a Shapiro–Wilk test and compared with a t-test for parametric data and a Mann–Whitney test for non-parametric data (GraphPad Prism 7, GraphPad 2016). Normally distributed data are presented as mean (±SD) or mean ± SD (95% confidence interval); otherwise data are median (25–75th percentile). Statistical significance was set at P < 0.05.
Results
Maternal and foetal arterial blood gas analysis results.
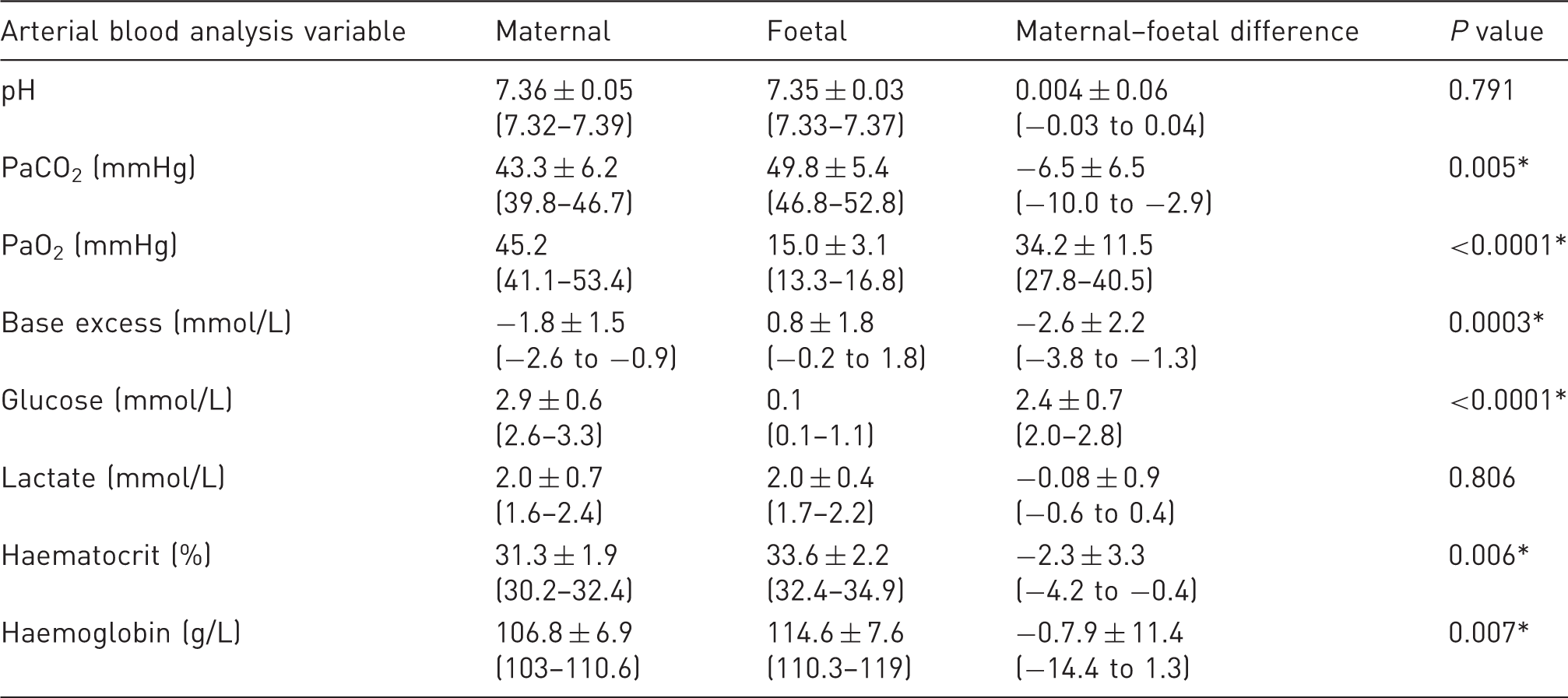
Data are presented as mean ± SD (95% confidence interval) or median (25–75th percentile). *P < 0.05.
There were no complications during the foetal ventilation study and all foetuses survived for the duration of the study (data not published).
Discussion
To ensure prompt surgical delivery of the foetus supplemental oxygen was not administered and an endotracheal tube was not placed during anaesthesia. In general terms this approach is not suitable for anaesthetic management of ruminants, as an endotracheal tube should be placed to secure the airway and protect against aspiration of fluid such as saliva or regurgitated rumen contents 8 but was justified in this streamlined protocol for prompt delivery of the foetus. The major consequence of this protocol was maternal hypoxaemia.
Maternal hypoxaemia in this study may be due to multiple contributing factors including the lack of supplemental oxygen by facemask or endotracheal tube, positioning in dorsal recumbency and pregnancy. Given the requirement for positioning in dorsal recumbency and the pregnancy status of the sheep, the only factor from this list that could have been manipulated to improve maternal PaO2 is the provision of oxygen by facemask or endotracheal tube. The streamlined protocol did not include either of these techniques and future work should investigate the impact of oxygen delivery by these two routes to determine if the benefit outweighs any compromise to efficiency.
Interpretation of the results of this study can be made by either analysis and evaluation of the maternal and foetal results in isolation or by focusing on the calculated differences between the two for each variable. Taking the former approach in the first instance: the results from the maternal blood samples were within the normal range for pH (7.35–7.45),6,9 PaCO2 (35–45 mmHg),6,9 base excess (−5 to 5 mmol/L), 6 glucose (1.2–3.6 mmol/L), 10 lactate (< 5 mmol/L), 6 haematocrit (0.24–0.5) 10 and haemoglobin concentration (80–160 g/L). 10 The maternal PaO2 was low and represents hypoxaemia. 6 Normal values for foetal arterial blood gas results are more difficult to define, but when the results of this study are compared with previous work in anaesthetised pregnant ewes, the foetal blood gas data are superior: the pH is closer to neutral; PaCO2 is lower and only slightly higher than the normal range for an adult sheep; and base excess, glucose concentration, haematocrit and haemoglobin concentrations are comparable.9,11-13 In other studies the foetal PaO2 also indicated hypoxaemia: median (range) of 26 (23.4–30.6) mmHg and 26.9 (23.1–29.8) mmHg in twin pregnancies; 12 and mean (±SD) of 20.1 (±4.2) mmHg 11 and 21 (±1.9) mmHg 9 in singleton pregnancies are reported when the maternal PaO2 was normal for sheep being mechanically ventilated with 100% oxygen through an endotracheal tube. The maternal PaO2 in these studies was reported to be between 173.4 and 404.1 mmHg in twin ewes 12 and 486.3 (±51) mmHg 11 and 278 (±14.2) mmHg 9 for singleton-pregnant ewes but the provision of mechanical ventilation and supplemental oxygen through an endotracheal tube is vital for interpretation of the results in context. Taking this approach, i.e. describing the maternal and foetal results in isolation, to interpretation of the results of this study, the anaesthetic protocol was associated with normoventilation (normocapnia) and hypoxaemia of the ewe, while the foetus was hypoxaemic as well as being hypoglycaemic.
Alternatively, the latter approach of evaluating the difference between the maternal and foetal values for each variable can also be taken. The maternal–foetal differences for PaCO2, PaO2, base excess, glucose concentration, haematocrit and haemoglobin concentration were statistically significant in the current study. However, the clinically significant differences are considered as limited to the values for PaO2 and glucose concentrations. In previous studies the difference between maternal and foetal PaO2 is reported to be between 226.2 mmHg 12 and 461.2 mmHg 11 in ewes breathing 100% oxygen through an endotracheal tube. The ewes in these studies were not hypoxaemic so comparison to the current study may not be valid; however, the PaO2 values of the foetuses in these other studies were also low (as defined in the previous paragraph).9,11,12 The foetal PaO2 in the current study was approximately 5 mmHg lower than these other published data but the importance of this difference is not known.
It is, however, important to acknowledge that foetal PaO2 is usually relatively low in humans 14 and in sheep. 9 This feature of foetal physiology is an adaptation that involves increased oxygen carrying capacity of foetal blood and increased oxygen affinity to haemoglobin that maintains oxygen content of foetal blood throughout the changes that occur during gestation.14,15 In sheep the position of the foetal oxyhaemoglobin dissociation curve is to the left of the maternal equivalent, allowing for greater oxygen carrying capacity in the face of a low PaO2.14,15 How low foetal PaO2 can go before there are physiological consequences is important in the context of this study where the foetal PaO2 was so low. A recent review quotes that a foetal umbilical artery PaO2 of 25 mmHg is representative of normal in humans. 15 In an older (1952) and smaller (n = 7) study of sheep the authors document a maternal–foetal PaO2 difference of 37–44 mmHg, which results in a foetal PaO2 of just 8 mmHg when the maternal value is 44 mmHg. 16 In the current study there were no adverse effects associated with the foetus after delivery, so it is assumed that the low PaO2 represents just a slight deviation from normal and that deviation is attributed to severe maternal hypoxaemia.
The numerical definition of hypoglycaemia for the foetus or newborn is controversial but in human medical practice a blood glucose level < 2.6 mmol/L, even in the absence of clinical signs, is classified as hypoglycaemia. 17 In the context of this study the lambs were hypoglycaemic, but the importance of this value is difficult to interpret. If it is accepted that the results are accurate as the samples were analysed promptly and the analyser was calibrated daily, then interpretation of clinical signs associated with low circulating glucose may assist in determining the significance of the result. Given the foetuses were delivered from anaesthetised ewes and the anaesthetic drugs cross the placenta, 18 the foetuses were also unconscious, and signs of hypoglycaemia such as an altered level of consciousness, tremors, convulsions, apnoea and coma could not be observed. 17 The foetal blood glucose results are unlikely to be significant in short-term studies such as this one where the foetuses were delivered for investigation into the impact of mechanical ventilation on lung injury in a 30-minute treatment period prior to euthanasia. For studies where foetal survival is required ongoing monitoring and management of blood glucose concentration is recommended.
Another important factor for consideration when interpreting the results of this study is the period of time between induction of anaesthesia and delivery of the foetus. In the previous studies the time lapsed was over an hour for single foetuses 11 and approximately half an hour for the first twin and another half an hour for the second twin. 12 The decision to omit the provision of supplementary oxygen and endotracheal intubation and was made in this study as it was expected that the time from induction of anaesthesia to euthanasia of the ewe would be short. If the time frame had been longer it is possible that other abnormalities (aside from maternal and foetal hypoxaemia and foetal hypoglycaemia) may have developed. Although additional doses of intravenous anaesthetic could be administered and were administered to ensure the ewe remained unconscious, supporting ventilation was not possible so prompt delivery of the foetus was essential.
The results of this study must be interpreted in light of the limitations of the study. Firstly, comprehensive physiological monitoring of the ewe was not possible as the priority was to ensure the ewe was unconscious and the site of the surgical incision was desensitised for prompt delivery of the foetus. This approach meant that although the ewe was confirmed to be alive as evidenced by a palpable peripheral pulse and observation of spontaneous ventilation, measurements of the pulse rate, heart rate, respiratory rate and blood pressure were not made. These data would contribute to an evaluation of the safety of the anaesthetic protocol; however, the result of normocapnia demonstrates that at least adequate spontaneous ventilation was preserved. Over such a short timeframe that result is valuable. Given that the ewes were euthanased immediately after caesarean delivery of the lamb, the safety of the anaesthetic protocol applies to a short time frame where recovery from anaesthesia is not planned. Secondly, supplemental oxygen was not provided, and the trachea of the ewe was not intubated. It is likely that oxygen delivered by facemask or endotracheal intubation with or without oxygen supplementation would delay the development of maternal and foetal hypoxaemia. The disadvantage of placing an endotracheal tube is entirely related to the time this procedure takes. In experienced hands this time should be very short, and in light of the results of this study it is possible that the benefit of protecting the airway would outweigh the consequences of a delay to delivery of the foetus if it prevented the development of severe hypoxaemia. Supplementation of oxygen by facemask is a simple approach, which requires an oxygen supply, an appropriate breathing system and a facemask. The impact of delivering oxygen in this way should be evaluated in the future for studies such as the one described here.
Placement of an endotracheal tube in this type of anaesthetic technique would provide a contingency in the event of delayed subarachnoid injection of lidocaine or surgical complications. If an endotracheal tube is in place, then intermittent positive pressure ventilation could easily be administered if hypoventilation or hypoxaemia occurred. The endotracheal tube would optimise the inspired concentration of oxygen (at least to 21% in room air) and prevent partial or complete airway obstruction. Furthermore, an endotracheal tube would also facilitate effective delivery of 100% oxygen. Delivery of oxygen by a facemask may be a less invasive and time-consuming alternative in this context and is likely to improve at least maternal oxygenation given that oxygen by mask improves PaO2 in dogs.19,20
The experimental protocol reported here was appropriate for the prompt delivery of the foetus. Nevertheless, it is difficult to justify a recommendation to avoid providing supplemental oxygen and/or placing an endotracheal tube when anaesthetising sheep. The benefit of providing supplemental oxygen or placing an endotracheal tube must always be carefully weighed against the benefit of saving time and would only be appropriate in short-term procedures where the ewe is not going to recover from anaesthesia. In this study the pregnant ewe developed severe hypoxaemia and this abnormality may have contributed to a low foetal PaO2.
Footnotes
Acknowledgement
The authors thank the research team in the Division of Obstetrics and Gynaecology, University of Western Australia for the opportunity to collect blood samples.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.