
Abstract
The authors propose a new truth-telling technique and statistical model called “item count response technique” (ICRT) to assess the prevalence and drivers of sensitive consumer behavior. Monte Carlo simulations and a large-scale application to self-reported cigarette consumption among pregnant women (n = 1,315) demonstrate the effectiveness of the procedure. The ICRT provides more valid and precise prevalence estimates and is more efficient than direct self-reports and previous item count techniques. It accomplishes this by (1) incentivizing participants to provide truthful answers, (2) accounting for procedural nonadherence and differential list functioning, and (3) obviating the need for a control group. The ICRT also facilitates the use of multivariate regression analysis to relate the prevalence of the sensitive behavior to individual-level covariates for theory testing and policy analysis. The empirical application reveals a significant downward bias in prevalence estimates when questions about cigarette consumption were asked directly to pregnant women, or when standard item count techniques were used. The authors find lower smoking prevalence among women with higher levels of education and who are further along in their pregnancy, and a much higher prevalence among unmarried respondents.
Marketing managers, policy makers, and researchers are often interested in assessing the prevalence and drivers of “dark side” and “vice” consumer behaviors, such as illegal movie streaming; software downloading; shoplifting; tax evasion; or consumption of prohibited drugs, pornographic material, alcohol, or tobacco (Andrews et al. 2004; De Jong, Pieters, and Fox 2010; Wang, Lewis, and Singh 2016; Weaver and Prelec 2013). Because of the sensitive and sometimes unlawful nature of such behaviors, consumers may not respond truthfully to direct questions about them even when they are common. The resulting response bias hinders identification of the true prevalence of the behaviors in the target population and impedes effective managerial decision making and policy evaluation.
We propose a new truth-telling technique to assess the prevalence and drivers of such sensitive consumer behavior. Our methodology builds on the item count technique (ICT) to administer sensitive questions in surveys. Rather than asking consumers to respond to a sensitive question in isolation, the ICT asks consumers to count the number of affirmative responses to a set of items that includes the sensitive question. The added privacy protection increases truthful responding. Despite its intuitive appeal and growing usage in other disciplines (Coffman, Coffman, and Marzilli Ericson 2017; Imai 2011; Kuha and Jackson 2014; Nepusz et al. 2014), 1 the ICT has not yet been applied in marketing. Moreover, existing applications of the technique have important shortcomings that prevent it from reaching its full potential. We propose the “item count response technique” (ICRT) to address these issues. Our research fits in a larger stream of marketing research on truth-telling for stated preference data, such as randomized response and similar techniques for surveys (De Jong, Pieters, and Fox 2010; Weaver and Prelec 2013), incentive alignment in conjoint settings (Ding, Grewal, and Liechty 2005), and behavioral research on when consumers are willing to divulge sensitive information (John, Acquisti, and Loewenstein 2011).
The proposed ICRT is applicable to a variety of sensitive consumer behaviors. It comprises a data collection method and a statistical model to make inferences about the prevalence of the sensitive behavior and its correlates. We demonstrate the potential effectiveness of the ICRT using Monte Carlo simulations and apply it in the context of a very sensitive behavior: cigarette consumption during pregnancy (Bradford 2003). Smoking during pregnancy puts not only the prospective mothers but also their unborn children at serious risk of contracting an alarming range of defects and inflictions (Hackshaw, Rodeck, and Boniface 2011), resulting in multimillion-dollar neonatal health care costs (Adams et al. 2002). The design and evaluation of countermarketing and antismoking programs rests on the accuracy of estimates of smoking prevalence and its correlates (Andrews et al. 2004; Wang, Lewis, and Singh 2016). However, the societal stigma about smoking, in particular smoking during pregnancy, may prevent prospective mothers from admitting their smoking habit and thus leading them to underreport their smoking status when answering direct questions in surveys (Dietz et al. 2011; Lumley et al. 2009). Using biomarkers to establish smoking prevalence among pregnant women is prohibitively costly and difficult to implement on a large scale. Thus, Jain (2017, p. 9) stresses in a comprehensive review that “efforts must be made to improve survey questionnaire content and/or methodology to be able to obtain better estimates of smoking prevalence.” Our research follows up on this call.
The next section presents the standard ICT and its assumptions. Then, we describe our new technique and how it improves on existing ones. We present Monte Carlo simulations to assess the performance of the new technique relative to standard techniques and our empirical application to cigarette smoking among pregnant women. We end with a discussion, suggestions for implementation of the procedure, and for recommendations for future research.
The ICT
The standard ICT uses a two-group design to ask sensitive questions. A sample of respondents is randomly assigned to either a control group or a treatment group. Respondents in the control group receive a list of baseline questions. Respondents in the treatment group receive the same list of baseline questions plus one extra question: the target item. The ICT is an indirect self-report technique—that is, respondents in both groups do not have to indicate directly whether they affirm or disconfirm each individual item in their list. Instead, they only have to count and report the total number of items in their list that they affirm. Then, the prevalence estimate of the target item is derived by taking the difference in the average number of affirmative responses between the treatment and control group. In an early application, Kuklinksi, Cobb, and Gilens (1997) asked respondents how many from a list of three (control group) or four (treatment group) events would anger or upset them, with the fourth, target event being, “A black family moving in next door.” For respondents in the U.S. South, the average item counts were, respectively, 1.95 in the control group and 2.37 in the treatment group, implying that such an event would anger or upset 42% of respondents in the treatment group (2.37 − 1.95 = .42). The ICT protects the privacy of respondents in the treatment group because it is impossible to determine what a respondent’s answer to the target item would be. Table 1 summarizes the ICT and its assumptions and compares the standard implementation (first column: type A), which has been most widely used, with recent improvements.
ICT: Characteristics and Assumptions.

Notes: The basic data collection design requires at least two samples, namely, a treatment and a control group. Some applications (e.g., Anderson et al. 2007; Blair and Imai 2012) use multiple treatment groups with different target items. “Identification Strategy” describes how the prevalence (group level) or probability (individual level) of the target item is inferred from the list sum reported by respondents.
Compared with direct questioning (DQ), the ICT increases the willingness of respondents to truthfully disclose sensitive information. This finding is consistent across multiple versions of the ICT and across a variety of attitudes and behaviors, such as racial and gender attitudes (Imai 2011; Kuklinski, Cobb, and Gilens 1997), election attitudes and behavior (Corstange 2009; Imai, Park, and Greene 2015), eating-disordered behaviors (Anderson et al. 2007), recreational drug use (Nepusz et al. 2014), high-risk sexual behavior (Tian et al. 2014), and various forms of delinquency (Wolter and Laier 2014).
The ICT has several strengths compared with other self-report techniques that aim to elicit truthful answers, such as the randomized response technique (RRT) (De Jong, Pieters, and Fox 2010; Fox, Avetisyan, and Van der Palen 2013; Lamb and Stern 1978). In the RRT, the sensitive question is asked directly, but a randomization mechanism adds “noise” to the respondent’s answer. Thus, the researcher does not know whether the answer that a respondent provides is true or forced by the randomization device. For example, respondents might be asked whether they currently smoke or not. They are instructed to provide their true answer when a real or electronic coin comes up heads, and to respond with a forced “yes” when the coin comes up tails. Because the probability of the forced “yes” is known from the randomization device, prevalence of the sensitive behavior at the sample level can be readily inferred.
An important strength of the ICT relative to the RRT is that the instructions to respondents are generally easier to understand, which reduces measurement error from miscomprehension. A second strength is that the ICT does not rely on a randomization device, which increases the trustworthiness of the privacy protection and thereby adherence to the data collection procedure. Moreover, the ICT does not force respondents to select a particular answer that they do not like, which also increases adherence to the procedure. Together, this makes the ICT well-suited to be used in large-scale self-administered surveys for marketing research and policy purposes.
Identification Strategy and Assumptions of the ICT
The standard ICT uses the difference in the mean reported list sums between the treatment and control group to identify the prevalence of the target item (Table 1, type A). That is, the treatment group (T) receives a list of K baseline items plus the target item. The probability of an affirmative response for respondent i on baseline item k (k = 1,…, K) then is

where

where Ui is the binary response to the target item. In the control group (C), respondents receive a list with only the K baseline items. In that group, for k = 1,…, K, the probability of an affirmative response for respondent j and the list sum is


The prevalence of the target item then is calculated as the difference in means between groups:

where NT is the number of respondents in the treatment group, and NC is the number of respondents in the control group. Importantly, three assumptions need to be met to estimate the prevalence of the sensitive behavior consistently and unbiasedly from Equation 5: Group equivalence: Respondents in the treatment and control groups are equivalent in all characteristics, except in the content of the item list they receive. Procedural adherence: Respondents adhere to the instructions and truthfully answer the target item. Then, Homogenous list functioning: The target item in the list does not change the sum of affirmative answers to the K baseline items. That is, the sum of the Zik, k = 1,…, K are the same no matter whether respondent i is in the treatment group or control group.
Assumption 1 is met by random assignment of respondents to treatment and control group and violated without it. Assumption 2 is likely to be violated when there is a ceiling effect (Corstange 2009). A ceiling effect occurs when truthful answers require a respondent to answer all items in the list affirmatively:
While simple to implement and analyze, the standard ICT has three major drawbacks that may hamper its validity and widespread application in theory testing and policy application. First, it can neither test nor account for cases that its assumptions are violated, resulting in unknown, biased estimates. Second, it makes inefficient use of the available sample size, because only the treatment group answers the sensitive item. Third, it provides prevalence estimates of the sensitive behavior at the group level rather than at the individual level, which impedes theory testing and targeted policy making (Table 1: “Analysis Level” column).
Assumption tests
To address the first issue, Imai (2011) and Blair and Imai (2012) propose formal tests of Assumptions 2 and 3 (Table 1: type C). However, as yet there are no principled approaches to cope with situations that the assumptions are violated.
Single sample approach
To address the second issue, Nepusz et al. (2014) propose the “single sample item count technique,” which uses a single sample of respondents only. Then, all respondents receive a list with the target item and baseline items. To identify the prevalence of the target item, baseline items are used that each have a known 50/50 probability in the population of interest (Table 1: Type B). Examples of such baseline items are whether a respondent has a birthday that falls on an even or uneven day, was born in the first or the last six months of the year, is male or female, or lives at an address with even or uneven street number (Nepusz et al. 2014; Petróczi et al. 2011). The proportion of respondents affirming the target item can then be readily estimated, as the average response percentage above the known joint baseline item percentage. There are several limitations of this approach. First, using evidently uninformative baseline items makes the sensitive, target item salient, and adds to the “weirdness” of the overall list (Kuha and Jackson 2014, pp. 12–13). This increases the likelihood of procedural nonadherence and differential list functioning, violating Assumptions 2 and 3. Second, the approach makes it virtually impossible to examine the impact of individual-level drivers of the target behavior, because the distributions of the baseline items are only known at the population level.
Individual-level analysis
To enable inferences about individual-level drivers of the target behavior, Imai and colleagues (Imai 2011; Imai, Park, and Greene 2015) generalize the difference-in-means estimator in Equation 5. Collecting all list scores in the vector Y (that is,

Such a specification implies that Xiγ captures the effect of the covariates in Xi on the list score of respondents in the control group. Yet, because baseline items in the list are often weakly or even uncorrelated, the variance accounted for by the covariates in Xi will tend to be low. Thus, estimates of the probability that respondent i affirms the target item are likely to be imprecise and difficult to estimate. As a case in point, Wolter and Laier (2014) using the provided R program could not get the Imai estimator to converge in their application.
Kuha and Jackson (2014) go one step further by estimating the probability of affirming each of the baseline items, through a set of explanatory variables for each of the Zik. Yet, their model assumes that the relationship between predictors and baseline items is invariant across treatment and control groups (assumption 3), and the prevalence estimates are sensitive to the exact model assumed for the baseline items (idem, p. 335). That is, both the distribution assumed for the Zik, and the specific explanatory variables (and possible interactions) included in the model for the Zik affect the prevalence estimates, which is undesirable.
The ICRT Methodology
The ICRT methodology improves on previous techniques in three important ways (Table 1, type D). First, it uses a single sample only. This makes Assumption 1 redundant and uses survey resources efficiently. Second, it accounts for situations in which Assumptions 2 and 3 are violated. This provides valid estimates of the sensitive behavior even in cases of procedural nonadherence and differential list functioning. Third, it uses information provided by (and known only to) respondents elsewhere in the survey to accurately estimate the probability of affirming each of the baseline items in the list. This enables estimating the probability of the sensitive behavior at the individual level and facilitates multivariate analyses of potential correlates of the target behavior. Let us describe data collection and statistical model of ICRT.
Data Collection
Our identification strategy is to make use of the correlation between baseline items “inside” the list and baseline items “outside” the list elsewhere in the questionnaire. This correlation allows us to estimate the probability that each of the baseline items inside the list is affirmed. From that information, we can identify the probability that the target item in the list is affirmed at the individual level using a single sample of respondents only.
Specifically, we propose to use K baseline items inside the list that come from K different validated multi-item measures of latent variables, such as attitudes or traits (Bearden, Netemeyer, and Haws 2011). For now, assume that these K baseline items are unrelated to the target item in the list (we relax this assumption later). One item from each of the K measures is included as a baseline item inside the list. Assume that measure k consists of Nk items that reflect a latent variable (θik). Because one of its items is already inside the list, Nk − 1 items remain in measure k. These remaining items are administered outside the list, before or after, and are asked directly. These “outside” baseline items may be measured on a binary or polytomous response scale.
To illustrate, consider the data collection in our empirical application. Respondents first answer a few baseline items directly. Baseline items are based on the impulsiveness and self-discipline facets (two items from each) of the Big Five personality trait inventory (Costa and McCrae 2008), and are shown in a matrix table:

Later in the questionnaire, the list section is introduced as follows: Below, you will find three statements. We would like to know HOW MANY of these statements are true (we do not wish to know which statements are true or false, only how many are true). I currently smoke at least 1 cigarette per day. Sometimes I do things on impulse that I later regret. I’m pretty good about pacing myself so as to get things done on time.
Inside this list, item (a) is the target item, item (b) measures impulsiveness, and item (c) measures self-discipline. Thus, baseline items 1 and 2 outside the list and baseline item (b) inside the list all measure impulsiveness (Hyman 2001, p. 127). Because a latent trait (θi, impulsiveness) underlies responses to all three items, these should be strongly correlated. Knowing the answer to baseline items 1 and 2 outside the list then enables predicting the answer to the baseline item (b) inside the list, even though we do not observe the answer to that item in the data. The same reasoning holds for baseline items 3 and 4 outside the list and baseline item (c) inside the list.
To formalize the reasoning, because item k in the list comes from validated measure k, it is natural to assume that

That is, the unobserved baseline item Zik inside the list is a function of the latent variable score θik and of unique variance captured in ∊ik. The high intercorrelations between items from validated measures enable estimating Zik in the list using information from baseline items assessed directly, outside the list. 2
Statistical Model
We use an item response theory (IRT) specification to estimate the response to the target item in the list, given the total item count from the list and the responses to the baseline items outside the list. Thus, the name “item count response technique.” To specify the functions g(.) in Equation 7, assume a total of H polytomous baseline items administered outside the list, where

This model specifies the conditional probability of a respondent i, responding in a category c (c = 1,…, C) for item h, as the probability of responding above c − 1, minus the probability of responding above c. The specification is a graded-response IRT model (Samejima 1969), with latent variable θi, k(h), discrimination parameter ah and threshold parameters γh,1 <…< γh, C. Discrimination parameters are conceptually similar to factor loadings in a factor-analytic framework. The threshold γh, c is the value on the scale of θi, k(h), where the probability of responding above a value c is .5.
Next, we focus on the list-based items. Because the list contains K baseline items from existing multi-item measures, we modify Equation 1 using the two-parameter normal ogive IRT model. Thus, for k = 1,…, K:

with

An attractive feature of the specification in Equations 8 through 10 is that it is sufficient to derive the probability of an observed item count Yi for the list. For instance, with two baseline items and one target item inside the list, and a corresponding item count that ranges between 0 and 3, because of conditional independence we have:




So far, we assumed that the baseline items are unrelated to the target item in the list, as in prior ICT research (Glynn 2013; Imai 2011; Kuha and Jackson 2014; Nepusz et al. 2014; Tian et al. 2014). Our model can relax this assumption. It models the potential association between the baseline traits and the target behavior now indexed by i, via a standard Probit regression:

where
Accounting for Assumptions
Because the ICRT requires a single sample only, Assumptions 1 and 3 concerning group equivalence and homogeneous list functioning are redundant.
To account for nonadherence due to ceiling, we model an intermediate step in the response process in which respondents may decide to “edit” their true answer if their true list score equals K + 1. Denoting the true list score by

Then the probabilities of answering K + 1 and answering K become, respectively,


These altered list score probabilities can be substituted in the likelihood function.
Model Estimation
Estimation of the proposed model is challenging because of its high dimensionality. While some researchers have relied on expectation–maximization algorithms to estimate previous item count models (Blair and Imai 2012, Imai 2011; Tian et al. 2014), the multidimensional integrals required here make an expectation–maximization algorithm cumbersome to implement. Therefore, we rely on Markov chain Monte Carlo (MCMC) methods (Bradlow, Wainer, and Wang 1999; Fox and Glas 2001; Rossi, Allenby, and McCulloch 2005). The likelihood for the ICRT is

To identify the latent variables

after which we can simultaneously draw {Zi1,…, ZiK, Ui} using the probabilities in Equation 20. Note that two particularly easy cases are when Yi = 0, implying that Ui = 0, or when Yi = K + 1, implying that Ui = 1. Estimation details are in Web Appendix 1. We used MATLAB to estimate all models. The Web Appendix provides WinBUGS code (Spiegelhalter et al. 1996) to facilitate wider adoption of the method.
We compare the observed list score distribution to replicated list score distributions from the posterior predictive distribution:

with
In addition, we test the importance of model components (such as the need to include a nonadherence parameter) using the pseudo-Bayes factor (Geisser and Eddy 1979; see also Web Appendix 1). Values of the pseudo-Bayes factor closer to zero indicate better fit.
Monte Carlo Simulation
We conducted two Monte Carlo simulation studies that compare the performance of the proposed ICRT with the standard ICT estimator under a range of conditions. We describe these studies in the following subsections.
Differential List Functioning, Nonadherence, and Correlation with Baseline Traits
Study 1 assesses the violation of which assumptions threatens the validity of the standard ICT most. It also demonstrates that the ICRT can then still recover the true proportions. The experimental design has 20 conditions, namely 4 (assumption: differential list functioning of difficulty, and of discrimination parameters, procedural nonadherence, and correlation between baseline trait and target item) × 5 (true proportion of target item: .10, .30, .50, .70, and .90), each with 20 replication data sets. True sensitive proportions can vary widely. 3 In their review, Wolter and Preisendorfer (2013) document proportions of the sensitive behavior varying from 19% to 100%. Therefore, our simulations consider a wide range of proportions as well.
Each data set has 2,000 respondents in the list group and 2,000 respondents in a control group who receive DQ. The control group is needed for the standard ICT estimator, but not for the ICRT estimator. For each data set, we compute the prevalence estimates of the target behavior for the standard ICT and for the ICRT estimator using 5,000 burn-in draws and 5,000 draws for posterior inference for each replication data set.
The item list has two baseline items and a target item. The two baseline items are generated according to an IRT model, with discrimination and difficulty parameters specified in Table 2. Furthermore, for the ICRT model, there are H = 6 baseline items outside the list, each item measured on a five-point response scale. The first (last) three outside baseline items and the first (second) inside baseline item measure the same latent trait. Web Appendix 2 has details about item parameters. Item parameters are chosen such that the reliabilities of baseline trait are .80, in line with typical reliabilities of validated scales (Bearden, Netemeyer, and Haws 2011).
Simulation Study 1: Performance of ICT and ICRT Under Differential List Functioning, Nonadherence, and Trait-Target Correlation.

Notes: a = item discrimination; b = item difficulty; τ = incidence of procedural nonadherence. For Panel A: a1, list = a1, DQ = 1.1, a2, List = a2, DQ =1.2, and b1, list = .1, b1, DQ = −.9, b2, list = .3, b1, DQ = −.5. For Panel B: a1, list = .5, a1, DQ = 1.1, a2, list = .8, a2, DQ = 1.2, and b1, list = b1, DQ = −1, b2, list = b1, DQ = 1. For Panel C: a1, list = a1, DQ = 1.1, a2, list = a2, DQ =1.2, and b1, list = b1, DQ = .1, b2, list = b1, DQ = .3, and τ =.6. For Panel D: a1, list = a1, DQ = a2, list = a2, DQ =1.4, and b1, list = b1, DQ = −.5, b2, list = b1, DQ = .3, τ =.5, and
Table 2 reports the average ICT and ICRT estimates across the 20 replication data sets for each of the conditions. Panels A and B report the impact of differential list functioning (difficulty and discrimination parameters) on model performance. Panel C reports the impact of procedural nonadherence, and Panel D reports the impact of correlation between the baseline traits and the target item in the list on model performance.
Across conditions, the standard ICT underestimates the true proportion by 44% on average, whereas the ICRT underestimates the true proportion by .1% only (difference t(798) = 8.48, p < .001). Differential item difficulty (Panel A) can produce severe underestimates up to 460% of the true prevalence for the standard ICT (average underestimation 163%) but leaves ICRT estimates essentially unharmed (average overestimation 1.7%, t(198) = 10.88, p < .001). Differential discrimination parameters (Panel B) produce an average overestimation of 7.4% for the standard ICT (7.4%), and less than 1% underestimation for ICRT (difference t(198) = −5.04, p < .001). The large difference in bias for ICT due to differential difficulty versus differential discrimination parameters is because a shift in difficulties directly shifts the argument of the standard normal cdf (Equation 9), whereas the discrimination only shifts the argument of the standard normal cdf indirectly through multiplication by theta. Because theta has a mean of zero, the impact of the discrimination parameter will be smaller. Even procedural nonadherence of 60% (Panel C) leaves ICRT estimates essentially intact (<1% underestimation) but biases standard ICT estimates downward up to 30% (average underestimation 12.6%, difference t(198) = 7.47, p < .001). Finally, correlation between baseline traits and target item (Panel D) also leaves the ICRT estimates intact (<1% underestimation) but biases ICT estimates downward up to 12% (average underestimation 7.2%, difference t(198) = 4.07, p < .001). Further meta-regressions support the large bias in prevalence estimates when using the standard ICT, and the improved accuracy and close to zero bias (<2%) when using the ICRT estimator, for all conditions (Web Appendix 2: Table WA4).
List Size and Reliability of Measures of Baseline Traits
Study 2 tests the effect of list size, reliability of baseline measures, differential list functioning, and procedural nonadherence in more detail for the following two reasons. First, larger list sizes improve the respondent’s privacy protection but also muddle the analyst’s task by exponentially increasing the number of possible response patterns that produce a specific list score. In typical applications of the ICT, the list size varies between three and five items. For a list size of three, only three response patterns produce a list score of two (Equation 13). Yet for a list size of five, already ten possible response patterns produce a list score of two. The large number of patterns impedes empirical identification, despite theoretical identification.
Second, a higher reliability of the multi-item measures of baseline traits increases precision of estimating the sensitive proportion. Because of their higher intercorrelations, the outside baseline items predict the inside baseline items better, which in turn improves estimating the response to the target item. Thus, higher reliability might offset reduced precision owing to larger list sizes.
The experimental design has 90 conditions, namely 3 (list size: three, four, or five items) × 3 (reliability of measures: .70, .80, and .90) × 2 (assumption: differential list functioning, or differential list functioning plus procedural nonadherence) × 5 (true proportion of target item: .10, .30, .50, .70, and .90), each with 20 replication data sets. As in Study 1, we report the means of 20 replication data sets. We use difficulty parameters for inside baseline items that produce about a .5 probability of an affirmative response. We introduce either mild differential list functioning or mild differential list functioning plus procedural nonadherence (details in Web Appendix 2) and establish how the ICT and ICRT estimators perform under these conditions. Table 3 summarizes the results.
Simulation Study 2: Performance of ICT and ICRT for Various List Sizes and Scale Reliabilities.

Notes: DLF = differential list functioning; PNA = procedural nonadherence. Mean prevalence estimates are shown across 20 replication samples for each condition.
Across conditions, the standard ICT severely underestimates prevalence of the target item with on average 70%, whereas the ICRT overestimates this but much less at 10% on average (difference t(3,598) = 41.78, p < .001). Even at a moderate reliability of .70 and with a list size of three, the accuracy of the ICRT estimator is already very good, irrespective of the true proportion (Table 3, Column 1; average overestimation 1%). The standard ICT estimator performs much worse, with an average underestimation of 51%.
With larger list sizes, the standard ICT estimator progressively underestimates prevalence (underestimation at list sizes three, four, and five, respectively, is 44%, 89%, and 76%), while the ICRT estimator overestimates prevalence but much less (overestimation at list sizes three, four, and five, respectively, is <1%, 1%, and 27%). Importantly, and as predicted, when list size and reliability increase, the precision of the ICRT estimate increases as well (average bias < 1% at list size 5 and reliability of .90; see Table 3). Yet, the ICT estimator then still underestimates prevalence on average by 71%. At a list size of three, as in our empirical application, the ICRT estimator essentially has no bias (<1%) whereas the standard ICT estimator grossly underestimates prevalence (51%). Further metaregressions support the large bias in prevalence estimates for the standard ICT estimator and the improved accuracy for the ICRT estimator and show how improved reliability compensates bias from larger list sizes (Web Appendix 2; Table WA5).
Conclusion
The accuracy of the ICRT is very good, with essentially ignorable bias for list sizes of three and four at moderate levels of reliability of baseline trait measures. When the list size increases to five, high reliabilities of the baseline trait measures of .90 are needed to obtain reasonable prevalence estimates for the sensitive item, especially if the true sensitive proportion is low. Such high reliabilities require the use of conceptually and semantically very similar items, which is undesirable for reasons of privacy and trustworthiness. The “General Discussion” section returns to this topic.
The ICT and ICRT estimators perform equally well in case of full procedural adherence (Assumption 2) and homogenous list functioning (Assumption 3). Yet the ICRT but not the standard ICT estimator is shielded against bias when these assumptions are violated. For all examined conditions, the ICRT estimator outperforms the standard ICT estimator. The ICRT is also more efficient by leveraging the information contained in the baseline items outside and inside the list, even with small list sizes and at moderate levels of reliability of the baseline traits. The “General Discussion” section provides guidelines for the design of item count studies.
Empirical Application
The empirical application concerns cigarette consumption (“smoking”) by women during pregnancy. Large-scale research on cigarette consumption has typically relied on self-reports from population surveys, such as the National Health and Nutrition Examination Survey, the Global Adult Tobacco Survey, and the National Maternal and Infant Health Survey (Bradford 2003; Cui et al. 2014). The societal stigma that rests on smoking tobacco makes the validity of such self-reported smoking questionable, in particular for vulnerable segments such as prospective mothers (Hackshaw, Rodeck, and Boniface 2011; Lumley et al. 2009). That prompted our empirical application.
Data
We conducted a two-group controlled survey experiment among currently pregnant women to establish their smoking prevalence. Respondents were randomly assigned to either a list group or a direct question (DQ) group. We compare the ICRT with direct self-reports (DQ) and with the standard ICT estimator, and we explore potential drivers of smoking prevalence. Data collection was online and took place in Spring 2015 in the Netherlands in collaboration with the market research company TNS Nipo, part of the Kantar group (http://www.tnsglobal.com/).
Sampling occurred in three steps. First, the market research company identified 581 currently pregnant women in their access panel of approximately 120,000 people. The sampled panel members received a link by email to participate in the online survey and were compensated for their participation with incentive points convertible into gifts. Second, sampled panel members received a separate email with the request to invite other pregnant women from their own personal networks to participate in the survey. Each sampled panel member received three unique links to the questionnaire to forward to people in their network. Panel members who recruited pregnant women from their network received additional incentive points. This step led to identifying an additional set of pregnant women, yielding 41% of the total sample. Third, an email with three unique links was sent to 23,000 nonpregnant women from the panel in the age group of 18–45 years old. They also received additional incentive points if they recruited pregnant women from their personal networks to participate. Among the participants from these nonpanel members, two gift vouchers of 50 euro each were raffled off. After this step, the final sample size was 1,315 currently pregnant women.
From the final sample, 886 respondents (2/3) were randomly assigned to the list group, and 429 respondents (1/3) were randomly assigned to the DQ group. The DQ group answered all items directly. The ICRT does not require it, but including the DQ group enables us to compare prevalence estimates between indirect and direct question methods. Moreover, we also use the DQ group to validate the ICRT method using a synthetic list.
Measures
List composition
The target sensitive item in our application is cigarette consumption. Many women who are addicted to cigarettes try to cut their cigarette consumption per day during pregnancy (Bradford 2003). Yet even reduced and light smoking holds serious health dangers for mother and child (Hackshaw, Rodeck, and Boniface 2011). Therefore, we use a conservative smoking measure: “I currently smoke at least 1 cigarette per day” (yes/no). Similar measures have been used in population surveys (Cui et al. 2014)
As baseline trait items, we selected six items from the impulsiveness facet of neuroticism and the self-discipline facet of conscientiousness in the Big Five inventory (Costa and McCrae 2008), three from each facet. One item from each facet was selected as baseline item inside the list, and the remaining two items from each facet were administered outside the list. Validation research shows that Big Five measures are not unduly contaminated by social desirability bias (Costa and McCrae 2008; Marshall et al. 2005). The two selected facets tend to be negatively correlated, which is desirable to prevent ceiling effects in list counts (Glynn 2013).
Baseline items outside the list
The four outside baseline items had a five-point Likert response scale with endpoints “Strongly disagree” and “Strongly agree.” Their wording was presented in the earlier example, and item order was the same for all respondents. In our application, the outside baseline items preceded the list question. The DQ group answered the four outside baseline questions (five-point scale anchored by “strongly disagree” and “strongly agree”) as well as the three inside list items directly (binary: true/false).
Covariates
Information was available from the research company’s database on respondent’s age (measured in years), number of children in the household, relationship status (married or not), and level of education (low, medium, high). In addition, we asked how many weeks the respondent was pregnant. Supplementary measures of psychological characteristics were included in the questionnaire to capture the nomological net in which smoking of pregnant women is embedded. First, we measured health locus of control (Moorman and Matulich 1993) using two five-point Likert items. We asked for the currently perceived availability of financial resources as a measure of respondents’ perceived socioeconomic status (Griskevicius et al. 2011), with three five-point Likert items (e.g., “I have enough money to buy the things I want”). Descriptive statistics for the list and DQ groups appear in Table 4.
Empirical Application: Descriptive Statistics.

Notes: Current perceived socioeconomic status is anchored by 1 = “low” and 5 = “high”; health locus of control is anchored by 1 = “low” and 5 = “high”; education is anchored by 0 = “low” and 2 = “high.”
Results
DQ and ICT Estimator
It is informative to compare prevalence estimates under DQ with standard ICT estimates, which can be done using Equation 5. We used regular regression with bootstrapping (10,000 samples) to compute the 95% confidence interval of the ICT estimates (Imai 2011). We report these in Table 5. There are little to no differences in prevalence between the DQ (10.7%) and the standard ICT (10.1%). In a separate survey among 260 pregnant women from the same population and market research company, the average probability (0%–100%) that smoking during pregnancy damages the health of one’s unborn baby and one’s own health was judged to be on average, 84% and 82% in the DQ and ICT estimates, respectively. In view of the known health risks and social stigma about smoking during pregnancy, as well as prior research on smoking prevalence during pregnancy, the lack of difference between the DQ and standard ICT estimate casts doubt on their validity. The Monte Carlo simulations revealed that differential list functioning and procedural nonadherence invalidate prevalence estimates from the standard ICT estimator but not from the ICRT. We examine this issue next.
Estimates of Smoking Prevalence: DQ, ICT, and ICRT.
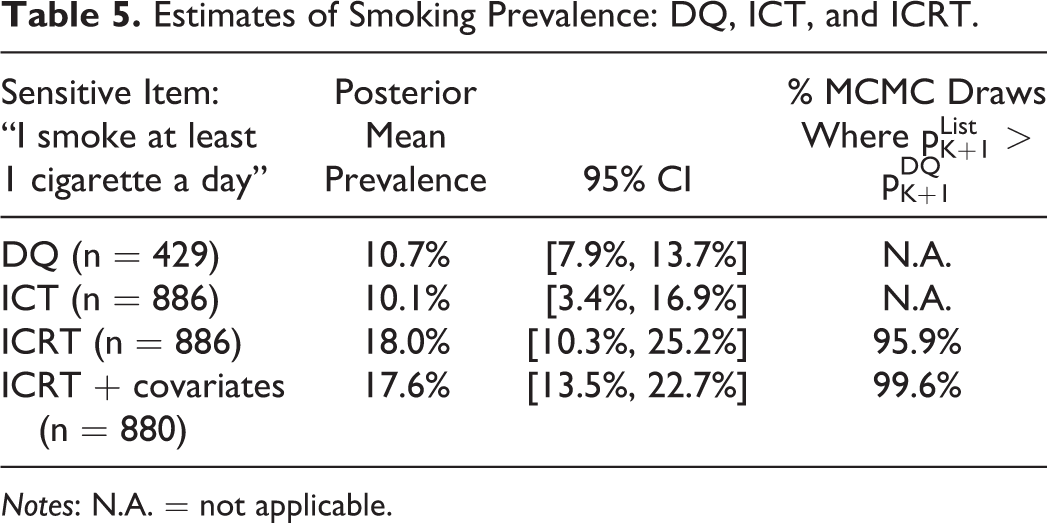
Notes: N.A. = not applicable.
ICRT Estimator
The analysis proceeded in two stages. In the first stage, we specified the sensitive proportion pK + 1 to be independent of respondent characteristics. Here, we use Equations 9 –15 and 17 –19, with an uninformative beta(1,1) prior for the sensitive proportion pK + 1. In the second stage, we added information on respondent characteristics (described in the next subsection). We used 100,000 burn-in draws and the next 100,000 draws for inference.
The model fits the list data very well. Observed list counts are 56, 569, 240, and 21 (total n = 886) for list counts of, respectively, zero, one, two, and three, whereas average replicated frequencies (Equation 21) over the MCMC draws after burn-in are 58, 563, 245, and 20, respectively, for a 98% hit rate. 4 In addition, when we use 750 of the 886 respondents to calibrate the model, and the remaining 136 respondents (16%) as a holdout sample, observed holdout frequencies are 6, 97, 31, and 2 for list counts of, respectively, zero, one, two, and three, whereas average replicated frequencies are 9, 85, 39, 3, respectively, for an 82% hit rate. Furthermore, we validated the ICRT differently, using a synthetic list that we compose in the DQ group. 5 This validation shows that the ICRT can estimate back a known nonsensitive proportion for real data instead of simulation data. We discuss each component of the ICRT model for the treatment group next.
Baseline items outside the list
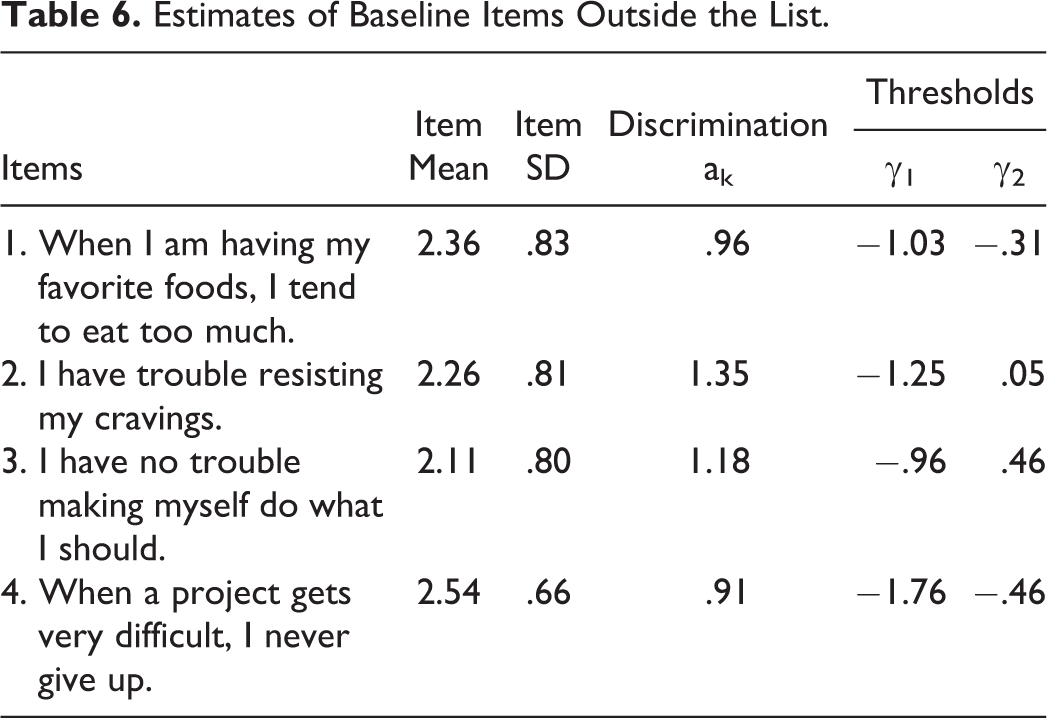
Item parameters of the baseline items outside the list are in Table 6. Although these items were measured on a five-point response scale, we noticed that the endpoints of the rating scale were rarely used. Therefore, we decided to collapse the endpoints of the response scale (merging “strongly disagree” and “disagree,” and “strongly agree” and “agree”) to create three-point response scales without loss of generality. Not doing so results in unstable first- and fourth-threshold estimates. Respondents mostly scored above the midpoint (two on the three-point response scale) for impulsiveness and self-discipline. The item parameter thresholds are well-separated. Most respondents have relatively moderate scores on the personality facets, which was already clear from the low frequencies of using the outer categories. This makes the items well-suited for the lists and ensures that the base rates are not too extreme. The baseline constructs are negatively correlated, with posterior mean correlation of −.292, which helps avoid ceiling effects (Glynn 2013).
Estimates of Baseline Items Outside the List.
Procedural nonadherence
The posterior mean of the nonadherence probability is 19.0%, with 95% CI = [1.0%, 45.1%]. The posterior mean resembles the 22.9% biomarker-based noncompliance estimate reported in Dietz et al. (2011). Controlling for procedural nonadherence slightly improves model fit (LMDwithNA = −3,976.9 vs. LMDwithoutNA = −3,977.0).
Differential list functioning
Our ICRT model does not require a control group. However, in our research design, we do have a control group and can test the assumption of homogeneous list functioning that is required when using the standard ICT difference-in-means estimator. We use the machinery of measurement invariance testing (Holland and Wainer 1993; Steenkamp and Baumgartner 1998). If baseline items inside the list behave differently from baseline items in the DQ group, we have
Item Parameters of Baseline Items Inside the List.

Notes: a = item discrimination; b = item difficulty.
These differences in item parameters have several consequences. As the simulations showed, prevalence estimates of the DQ group become much too low if the difficulty parameters of the baseline items are deflated. The differential list functioning results in a downward bias in the estimated prevalence of smoking during pregnancy in the DQ group.
To help interpret the item parameters, Figure 1 provides the item characteristic curves for the two baseline items inside the list for the list and DQ groups. Item characteristic curves show how the probability of an affirmative response varies as a function of the latent trait score. The latent trait score is on the x-axis and the probability of affirming the sensitive item (Pr[Zi, k = 1]) is on the y-axis. For lower trait values, the probability of an affirmative response is close to zero. Item parameters are on the same scale as the latent trait.

Item characteristic curves of inside baseline items in DQ group and list group.
Prevalence estimates
Table 5 shows that the ICRT prevalence estimate, which protects the respondent’s privacy and accounts for procedural nonadherence and differential list functioning, is indeed substantially higher than the prevalence estimate in the DQ group (18.0 vs. 10.7%, respectively). This percentage difference is in line with the reported percentage difference between DQ and biomarker estimates of smoking during pregnancy (Dietz et al. 2011; Lumley et al. 2009). Finally, the ICRT model with covariates, discussed next, estimates the prevalence to be 17.6%, which is also higher than in the DQ group.
We test the significance of the difference in prevalence estimates between DQ, standard ICT, and ICRT with a tail-area probability. We compute the fraction of the MCMC draws in which the prevalence estimate for the list group
Although the 95% credible interval for the ICRT model without covariates is relatively wide, 95.9% of the
The last row in Table 5 shows how well the predictors help to narrow the credible interval of the sensitive proportion pK + 1. The improvement in precision is about 38% relative to the prevalence estimates of the ICRT without covariates, and as a result, 99.6% of the
Drivers of Smoking Decision
In the second analysis stage, we estimated the ICRT model with Equation 16 instead of Equation 11 to relate the estimated smoking prevalence to covariates. Table 8 summarizes the results. Predictors are impulsiveness, self-discipline, and respondent’s age, number of children in the household, relationship status, number of weeks pregnant, education, current perceived socioeconomic status, and health locus of control. Uninformative normal priors were used for the regression coefficients.
Predicting Smoking Prevalence During Pregnancy.

Notes: 95% CI of boldfaced mean estimates does not include 0.
Except for the respondent’s age and the number of children in the household, all covariates are significantly related to smoking prevalence. In line with previous findings (Terracciano and Costa 2004), pregnant women with more self-discipline are less likely to smoke. Moreover, unmarried women are more likely to smoke. In fact, using the model estimates and holding all other covariates at their mean, smoking prevalence is estimated to be 4.6% among married women but 14.9% among unmarried women, which is more than three times higher. This difference is not due to differences in health locus of control, age, impulsiveness, and so on between unmarried and married pregnant women, because these variables were all statistically controlled for by the model, which makes the large difference even more telling.
The number of weeks that women were pregnant has a negative effect on smoking prevalence. Using the model estimates and holding all other drivers at their mean, smoking prevalence is estimated to be 18.1% after seven weeks of pregnancy but drops to 2.9% after 37 weeks. This reflects the increased urgency to stop smoking when pregnancy progresses and is in line with research documenting an increased effectiveness of smoking cessation interventions toward the end of pregnancy (Lumley et al. 2009). Women with higher levels of education and perceived socioeconomic status are less likely to smoke during pregnancy, which converges with other reports (Zimmer and Zimmer 1998). Furthermore, women with higher health locus of control scores are less likely to smoke during pregnancy.
Finally, we compare the covariate results of our model with the probit results in the DQ group. The latter results are obtained using the directly measured values for the three baseline items in the DQ group, instead of the augmented data {Zi1, Zi2}, Ui, as in the list group. There are several important differences between the regression results when stratifying by data collection method. In particular, marital status, number of weeks pregnant, and current socioeconomic status have no effect in the DQ group. Thus, above and beyond the significant difference in prevalence estimates between the ICRT and DQ, the ICRT method is also able to uncover more covariates that are related to smoking during pregnancy, which is notable in its own right.
General Discussion
We proposed the ICRT as a new truth-telling technique in consumer surveys about sensitive topics. The ICRT asks a single group of respondents to count how many items from a list of items they affirm, rather than whether they affirm each individual item from the list. The list contains several baseline items and the sensitive item of interest. This indirect way of asking questions protects respondents’ privacy and increases the likelihood of truthful responding as compared with direct questions about the sensitive behavior. The ICRT identifies the prevalence of the sensitive item by making use of the statistical association between baseline items inside the list and baseline items asked outside the list elsewhere in the questionnaire.
The ICRT introduces several innovations compared to earlier implementations of the ICT. First, the data collection design of the ICRT requires a single group of respondents only, rather than separate treatment and control groups. Thus, it makes more efficient use of the available survey resources, and it makes the assumption of group equivalence redundant. Second, the statistical model of the ICRT is the first to account for violations of procedural adherence and homogenous list functioning. By doing so, it provides more accurate prevalence estimates of the sensitive behavior than alternatives do. Third, the statistical model of ICRT facilitates multivariate analyses of potential drivers and correlates of the sensitive behavior at the individual level. This improves theory testing as well as policy decision making and evaluation. We provide specific recommendations for implementation of the ICRT subsequently.
The simulation results demonstrate the strengths of the ICRT model and have implications for existing ICT research, including controlled validation studies (Rosenfeld, Imai, and Shapiro 2016). The validity of ICT studies based on the standard ICT estimator that do not account for procedural nonadherence and differential list functioning is uncertain. The gain in validity of the estimates owing to the privacy protection provided by the ICT might be nullified by the loss in validity owing to violation of the ICT assumptions. To date, few ICT studies test for assumption violation (Blair and Imai 2012; Kuha and Jackson 2014).
We applied the ICRT to the domain of smoking behavior with a sample of 886 pregnant women, for which smoking is especially sensitive. We find evidence of substantial and significant underreporting when questions are asked directly, despite the standing practice in large scale research to rely on direct self-reports of smoking behavior during pregnancy (Bradford 2003; Lumley et al. 2009). Rather than merely establishing whether people smoke (or engage in other sensitive behaviors), ICRT also makes it easy to assess the drivers of smoking during pregnancy. This is relevant for theory testing and for the design and evaluation of smoking cessation interventions (e.g., http://www.acog.org). When pregnant women underreport their cigarette consumption, or cravings and feelings of being addicted, obstetricians, gynecologists and other professionals could deploy the wrong tools in cessation programs, with adverse health consequences (Lumley et al. 2009) and vast neonatal health care costs (Adams et al. 2002). Indeed, our findings indicate that several covariates (marital status, socioeconomic status, and number of weeks pregnant) that were insignificant in the direct questioning group were in fact significantly related to smoking during pregnancy when using the ICRT.
Implementation Recommendations
Analysts need to make various decisions when designing an item count study. Drawing on our theoretical analysis, simulation studies, and empirical applications, we formulate the following recommendations: List size. A total list size of two to four items (K = 1, 2, or 3) is optimal. This range balances acceptable complexity of the respondent task with good statistical accuracy. Privacy protection is obviously greater for larger list sizes (five and up). Yet such larger list sizes complicate the respondent’s task and require undesirably high reliabilities (see the bullet point on reliability of scales) of the baseline trait measures of .90 to obtain precise prevalence estimates for the sensitive item, especially for low true-sensitive proportions. Validated scales for baseline items. It is preferable to use K “inside” baseline items from K validated scales and administer remaining items from the scales “outside” the list. This will make the sensitive, target item in the list least salient, provides maximum privacy protection, and ensures trustworthiness of the procedure. Negative correlation of scales. To reduce ceiling effects of the list sums that participants need to report and to reduce procedural nonadherence, we recommend selecting at least two negatively correlated validated baseline scales within the set of K validated scales. Reliability of scales. The reliability of each of the K scales is preferably around .8, which is common for validated scales. Using validated scales with higher reliability (say .95) is undesirable. Such reliabilities usually require the use of conceptually and semantically similar items, which erodes privacy protection and trustworthiness of the list technique. Using validated scales with lower reliability (say .7 or less) reduces precision of the estimated prevalence of the target item. Number of outside baseline items. It is recommendable to include for each validated scale k, at least two or three “outside” items elsewhere in the survey. Using more “outside” baseline items per validated scale k increases the burden to respondents and may not be needed in case reliable, short-form multi-item measures are available or easily developed. Statistical model. Use of the ICRT statistical model for data analysis is preferable. Its better performance outweighs the added modeling effort. Follow-up analyses (details in Web Appendix 2) studied the performance of two simple benchmark models that, as the ICRT, also do not use information from a direct questioning group. The results indicate poor performance of these benchmark models and stress the importance of using the ICRT estimator. Whenever possible, we strongly recommend to collect relevant covariates (general and/or domain-specific covariates) that predict the the sensitive item. Using a probit equation for the sensitive item helps to narrow the credible interval of the sensitive proportion (which can otherwise be quite wide) and yields additional insights into the drivers of the sensitive behavior.
Opportunities and Future Developments
There are several opportunities for future methodological and substantive research. Methodologically, it would be interesting to compare the results of list-based questions with other privacy-protected questions, such as randomized response questions. Then strengths and weaknesses of various privacy protection techniques can be assessed. Initial attempts at such comparisons (Rosenfeld, Imai, and Shapiro 2016) could not yet model the response process to test crucial assumptions. That makes it difficult to assess the validity of such comparisons.
Substantively, it would be interesting to apply the ICRT across cultures to examine how people from different countries respond to the list-based questions, how the method’s accuracy varies across cultures compared with other types of privacy protection methods (e.g., randomized response), and how procedural nonadherence varies across countries. In a similar vein, the ICRT can be applied to obtain valid prevalence estimates of a host of other sensitive consumer behaviors wherein direct questions are likely to produce biased responses.
To return to the original challenge that motivated our research—as Jain (2017, p. 6) stressed, “The practice of computing smoking prevalence rates without adjusting for bias associated with self-reported smoking status is flawed.” The ICRT promises to be a valuable new addition to the toolbox of marketing and survey researchers who aim to know the prevalence of sensitive consumer behaviors, such as smoking status, by using self-reports, and the drivers of these behaviors. This might eventually help avert and curb the prevalence of such dark side and vice consumer behaviors.
Supplemental Material
Supplemental Material, jmr.17.0275_web_appendices - Assessing Sensitive Consumer Behavior Using the Item Count Response Technique
Supplemental Material, jmr.17.0275_web_appendices for Assessing Sensitive Consumer Behavior Using the Item Count Response Technique by Martijn G. de Jong and Rik Pieters in Journal of Marketing Research
Footnotes
Acknowledgments
The authors thank the JMR review team for their valuable suggestions and guidance throughout the review process. They have also benefited from comments by seminar participants at Vienna University.
Associate Editor
Peter Danaher served as associate editor for this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Martijn G. de Jong thanks the Netherlands Organization for Scientific Research for research support.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.