
Abstract
Cryoultramicrotomy was originally established to provide ultrathin cryosections as substrates for on-section immunolabeling in immunoelectron microscopy. Recently, we recognized that ultrathin cryosections of skin (0.2 μm thick) could serve as substrates for immunofluorescence (IF) with excellent resolution. To assess the advantages and the limitations of IF on ultrathin cryosections, we compared the labeling of IF on 0.2-μm ultrathin cryosections of skin with those of routine IF on 6-μm cryostat sections, confocal laser scanning microscopy (LSM), and immunogold electron microscopy using several markers of keratinocyte cell surface and basement membrane zone molecules. IF on ultrathin cryosections clearly demonstrated a lack of bullous pemphigoid antigens beneath the melanocytes, desmosomal antigens as discontinuous dot-like labeling, and nondesmosomal plasma membrane antigen as a ladder-like pattern. IF on ultrathin cryosections provided convincing images with higher resolution than confocal LSM, which corresponded well to those of immunogold electron microscopy. IF on ultrathin cryosections had superior resolution compared to routine IF or confocal LSM and should serve as a powerful tool in future studies for the analysis of skin antigens.
Keywords
C
Materials and Methods
Antibodies
For the BMZ markers, the following antibodies were used: two bullous pemphigoid (BP) sera that bound only to the 230-kD BP antigen (BPAG1) or the 180-kD BP antigen (BPAG2) by immunoblot as described previously (Ishiko et al. 1993); GoH3 monoclonal antibody against α6 integrin (Sonnenberg et al. 1991); LH7.2 monoclonal antibody against N-terminus (NC-1 domain) of Type VII collagen (Leigh et al. 1988); and polyclonal antibodies against Type IV collagen (LB-1491; LSL/Cosmo Bio, Tokyo, Japan). For the keratinocyte cell surface marker, the following antibodies were used; pemphigus vulgaris (PV) and pemphigus foliaceus (PF) sera that bound only to the 130-kD Dsg 3 or 160-kD Dsg 1, respectively, by immunoblot (Shimizu et al. 1995); anti-desmoplakin monoclonal antibody (Parrish et al. 1987); and anti-desmoyokin polyclonal antibodies (Hashimoto et al. 1993), whose unique ultrastructural binding site was demonstrated previously (Masunaga et al. 1995).
Ultrathin Cryosections (0.1-0.2 μm Thick)
Ultrathin cryosections of normal human skin were obtained basically according to a method described by Tokuyasu (Tokuyasu 1980), with some modification. Fresh normal human skin obtained at surgery was cut into small pieces (<1 mm3), prefixed with acetone at 4C for 30 min, and immersed in 2.3 M sucrose in phosphate buffer. The samples were mounted on pins, rapidly frozen by plunging into liquid propane (-190C), and stored in liquid nitrogen until use. Semithin sections were cut from the surface of the samples at -80C to -100C using an Ultracut-S ultramicrotome equipped with a FCS cryosystem (Reichert-Jung; Vienna, Austria) until both the epidermis and the dermis appeared on a single section. Then ultrathin sections (0.2 μm thick) were cut, transferred to an albumin-coated glass slide using a platinum loop with a droplet of 2.3 M sucrose/PBS, and processed as substrate for IF. For immunogold EM, ultrathin sections (0.1 μm thick) were also cut from the same block, transferred to Formvar-coated nickel grids, and processed for immunolabeling.
Routine Cryostat Sections (6 μm Thick)
Normal human skin was immersed in OCT compound and rapidly frozen by isopentane cooled with liquid nitrogen. Then 6-μm sections were cut using a routine cryostat microtome at -25C.
Immunofluorescence
Immunofluorescence was performed on both routine 6-μm cryostat sections and 0.2-μm ultrathin cryosections of normal human skin, as follows. The sections were incubated with primary antibodies at 37C for 1 hr, washed with PBS, and incubated with FITC-conjugated secondary antibodies (DAKOPATTS; Copenhagen, Denmark) at 37C for 1 hr. The immunolabeled sections were mounted with glycerol/PBS containing p-phenylenediamine as an antifading agent (Krenik et al. 1989). IF on ultrathin cryosections was observed under an epifluoroscope with a high-power objective lens (1:100, NA = 1.3) with oil immersion.
Confocal Laser Scanning Microscopy
Skin cryosections (6 μm thick) were attached to the glass slides. The specimens were incubated with primary antibodies, followed by FITC-conjugated secondary antibodies as described above. The sections were mounted with glycerol/PBS containing p-phenylenediamine and observed under confocal LSM (MRC-600; Nippon Bio-Rad Laboratory, Tokyo, Japan) as described (White et al. 1987), using a high power objective lens (1:100, NA = 1.3) with oil immersion (total magnification 1:1000). A krypton-argon ion laser operating at a wavelength of 488 nm was used as the excitation source. The confocal pinhole was stopped down to the minimal size to obtain the thinnest optical slice. Images were acquired as optical sections and processed with COMOS software which was part of the equipment of the MRC-600. All the color images, including routine IF and confocal LSM, were transferred to Photoshop software (Adobe Systems; San Jose, CA) and printed on Fujifilm Pictro paper.
Immunoelectron Microscopy
Immunogold-EM was performed using either the postem-bedding method (Shimizu et al. 1989) or cryoultramicrotomy (Ishiko et al. 1996) as described previously. The ultrathin sections of normal human skin embedded in Lowicryl K11M (Chemische Werke Lowi; Waldkraiburg, Germany), or ultrathin cryosections obtained from frozen normal human skin were incubated with the primary antibodies listed above, then with 5-nm gold-conjugated secondary antibodies (Amersham International; Poole, UK).
Results
IF on Ultrathin Cryosections Provided Superior Resolution of BMZ Antigens Compared to Confocal LSM and Routine IF on 6-μm Sections
All the BMZ antigens of BPAG1, BPAG2, α6 integrin, Type VII collagen, and Type IV collagen were observed linearly at the dermoepidermal junction with IF on 0.2-μm cryoultrathin sections (Figures 1a, 1d, and 1g), confocal LSM (Figures 1b, 1e, and 1h), and routine IF on 6-μm sections (Figures 1c, 1f, and 1i). However, IF on ultrathin cryosections provided superior resolution, i.e., the immunolabeling was observed as sharp, thin, linear signaling, and fine microvilli of basilar surface of basal keratinocyte were clearly demonstrated on the 0.2-μm ultrathin cryosections (Figures 1a, 1d, and 1g). Furthermore, the lack of the BPAG1 and the BPAG2 (Figure 1d) beneath the melanocytes was observed as occasional discontinuous labeling, while Type VII collagen and Type IV collagen showed a continuous pattern (data not shown). The labeling of α6 integrin, another marker for hemidesmosomes, was indistinguishable from that of BP antigen by IF on ultrathin cryosections (Figure 1g).
Confocal LSM had better resolution compared to routine IF and revealed labeling patterns similar to those of cryoultrathin sections (Figures 1b, 1e, and 1h). However, fluorescence was occasionally detected as a blurred line at the dermoepidermal junction, and the results were less convincing than those of IF on ultrathin cryosections, which provided sharper and thinner signaling, thus enabling the tracing of fine microvilli.
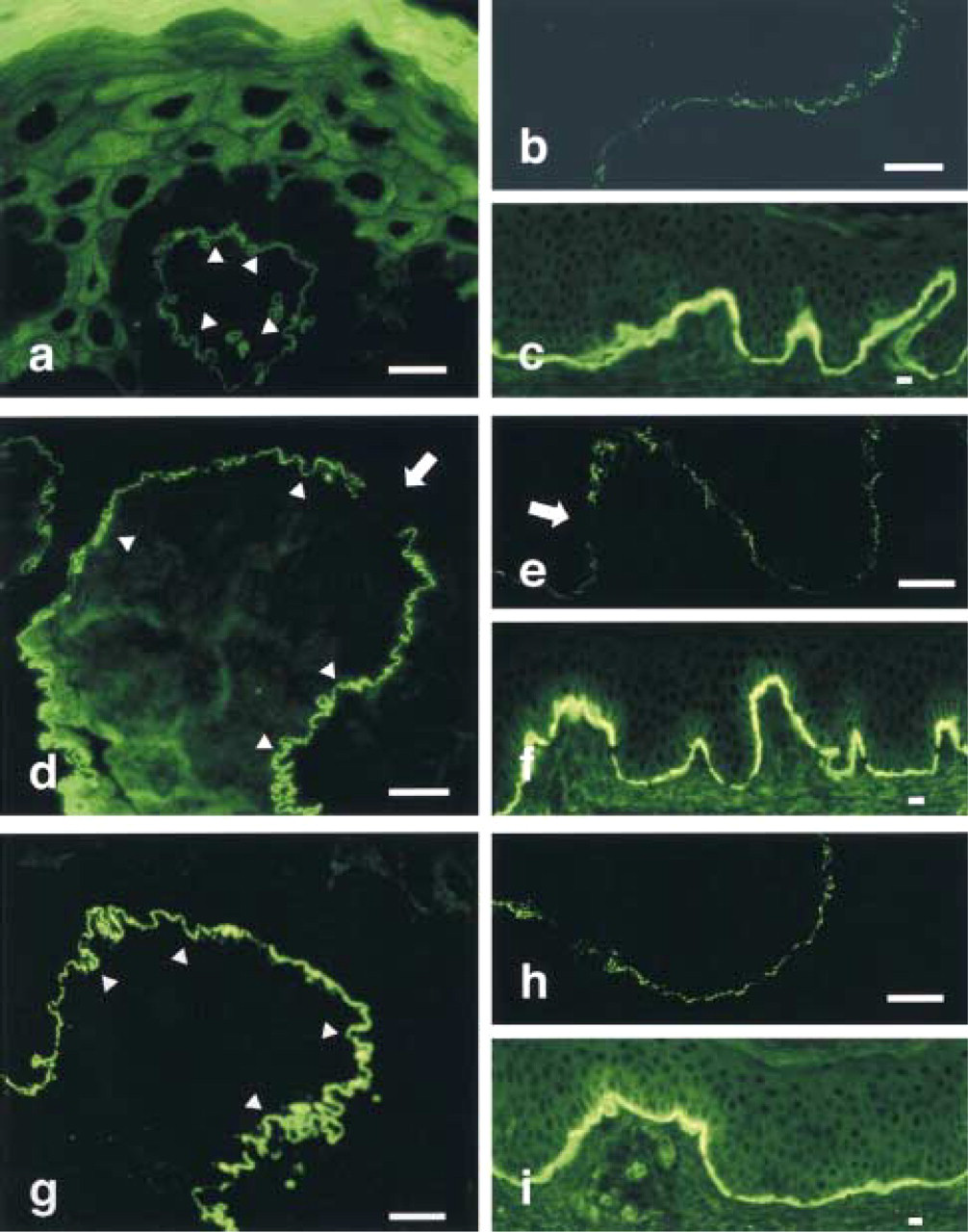
Labeling of epidermal basement membrane zone antigens of BPAG1
Immunogold EM showed distinct distributions of BPAG1, BPAG2, and α6 integrin as described previously, i.e., BPAG1 was localized in the intracellular portion of hemidesmosomes, BPAG2 was localized along the plasma membrane of hemidesmosomes (Ishiko et al. 1993), and α6 integrin was localized on the extracellular surface of hemidesmosomes (data not shown). These differences in ultrastructural localization of antigens could not be detected even by IF on ultrathin cryosections or confocal LSM, indicating the limitation of immunofluorescence.
IF on Ultrathin Cryosections Provided Superior Resolution of Keratinocyte Cell Surface Antigens and Could Distinguish Desmosomal Antigens from Nondesmosomal Antigens
By routine immunofluorescence, all the antibodies to keratinocyte cell surface antigens used in this study, including PF (against Dsg1) (Figure 2c) and PV (against Dsg3) (not shown) sera, anti-desmoplakin antibodies (Figure 2f), and anti-desmoyokin antibodies (Figure 2i), labeled continuously on the keratinocyte cell surface and no significant difference was seen among them. By confocal LSM, all immunolabeling, including desmoyokin, appeared as a discontinuous dot-like pattern with no significant difference among the antibodies (Figures 2b, 2e, and 2h). Using 0.2-μm ultrathin cryosections as substrate, however, the labeling was seen to follow two patterns. The first was a discontinuous dot-like pattern shown by PF serum (Figure 2a), PV serum (not shown), and anti-desmoplakin monoclonal antibody (Figure 2d). PF and PV sera could not be distinguished by this method, but desmoplakin was labeled as larger dots than PF or PV antigens. This dot-like pattern may represent the desmosomal localization of antigens, as demonstrated below by immuno-EM. The second was a ladder-like pattern in the desmoyokin labeling in which the signals were seen along the plasma membrane of keratinocytes (Figure 2g). This pattern was specific to desmoyokin, which localized at the nondesmosomal plasma membrane of keratinocyte as demonstrated by immuno-EM.
In immuno-EM (data not shown), PF antigen and PV antigen were mainly localized at the extracellular portion of desmosome and were indistinguishable from each other, as described previously (Shimizu et al. 1995). Desmoplakin was shown to localize to the intracellular portion of the desmosomes (Shimizu et al. 1992), whereas desmoyokin was distributed along the nondesmosomal plasma membrane of keratinocytes (Masunaga et al. 1995). PF and PV antigens localized in a narrow restricted area, but desmoplakin localized in a broad area in the desmosome complex. These ultrastructural distributions corresponded well to the images of IF on ultrathin cryosections in which desmoplakin was demonstrated as a larger dot-like pattern, PF or PV as a smaller dot-like pattern, and desmoyokin as a ladder-like pattern.
Discussion
In this study, we demonstrated that IF on 0.2-μm ultrathin cryosections of skin can provide better resolution than confocal LSM or routine 6-μm cryostat sections. IF on routine sections has been widely used for antigen immunolocalization at the light microscopic level. Confocal LSM was recently introduced to improve the rejection of out-of-focus noise of IF and to greatly enhance images. On the other hand, improved techniques for immuno-EM have been established for investigating the ultrastructural localization of antigens. Typically, immunohistochemistry using light microscopy and immuno-EM are performed on different tissue preparations, and there may be a gap in the findings between them. Ultrathin skin cryosections from a single block can serve as substrate for both IF and immunogold EM simultaneously, and correlative microscopy by immunofluorescence and immunogold EM on the same block is feasible. For example, a lack of BP antigens beneath the melanocyte, which was visible by immunoperoxidase EM (Shimizu et al. 1988) but not by routine IF, can be clearly demonstrated by IF on ultrathin cryosections. Although immunogold-EM can demonstrate the precise distribution of BP antigen in the hemidesmosomes at the ultrastructural level, this is not suitable for observing such a general distribution of BP antigen at low magnification. Therefore, simultaneous application of IF and immunogold-EM on ultrathin cryosections from the same block of skin tissue should provide superior information about molecular distribution compared to the conventional methods.
Confocal LSM is known to have superior resolution compared to conventional IF, and the improvements are such that it is possible to optically section thick specimens with little degradation in the image quality of interior sections. One can theoretically derive an expression for the thickness of the confocal sections for the limiting case of an infinitely small confocal aperture as follows (Mjlof and Forsgren 1993):
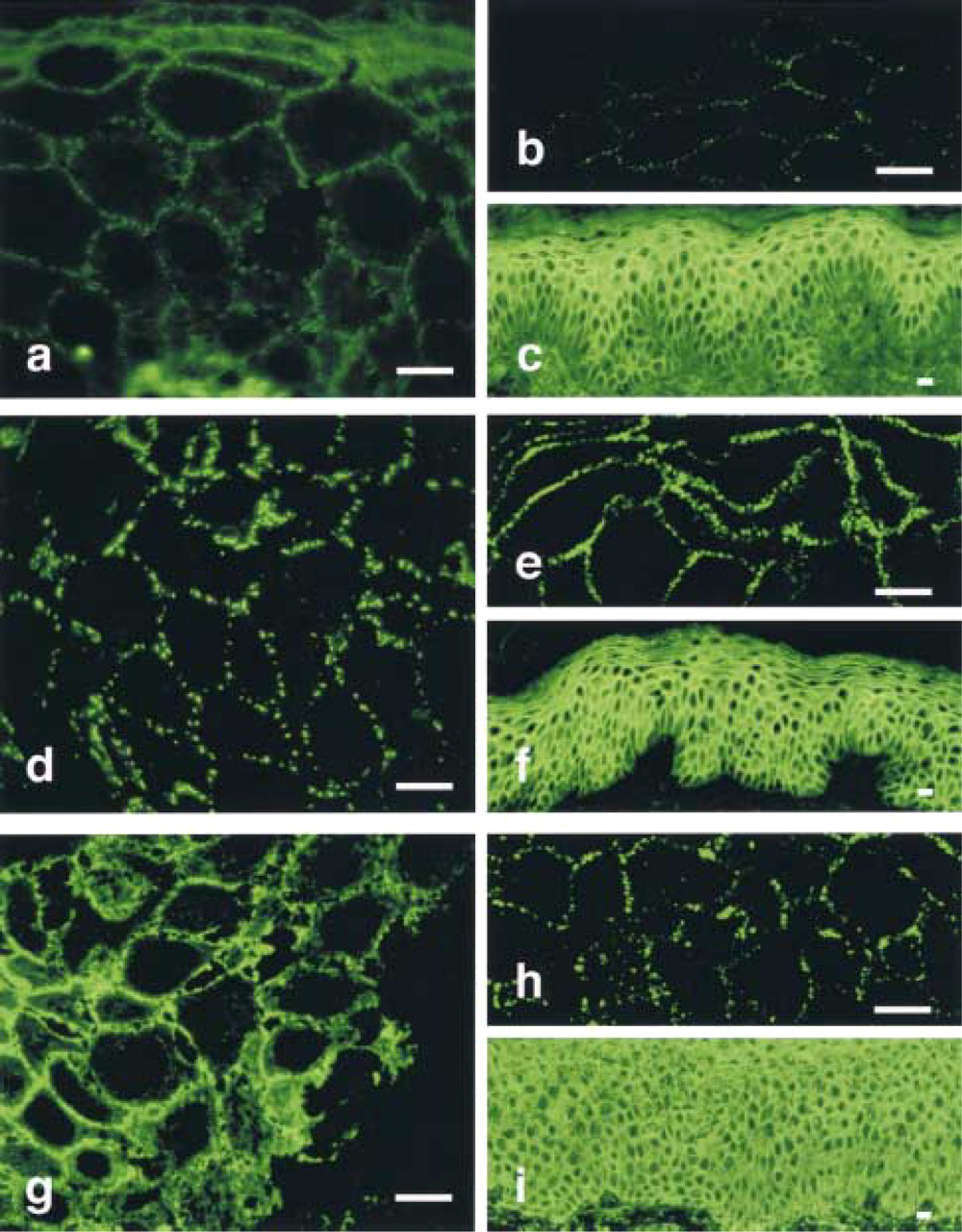
Labeling of epidermal keratinocyte cell surface antigens of pemphigus foliaceus (PF) antigen (Dsg1;

(where λ = wavelength of light = 0.488 μm, n = index of refraction for the immersion medium = 1.5, and NA = numerical aperture = 1.3).
The theoretical axial resolution of confocal LSM is calculated as follows:

The axial resolution of confocal LSM is apparently thicker than 0.2 μm. Therefore, the rejection of out-of-focus noise is theoretically considered to be better in IF on ultrathin cryosections than in confocal LSM. Additional merits of the present method are that apparatus for confocal LSM is not necessary, and that, once cut, the ultrathin cryosections can be stored for at least 6 months at -30C until use. Moreover, on the surface immuno-EM can be conducted on the sections from the same block of tissue after the IF on ultrathin cryosections. The disadvantages of this method include the need for apparatus for cryoultramicrotomy and the fact that skillful sectioning is required.
The dot-like staining at the keratinocyte cell surface observed with PV antigen, PF antigen, and desmoplakin can be interpreted to represent desmosomal localization of these antigens in combination with immuno-EM. On the other hand, the ladder-like pattern seen with desmoyokin can be interpreted to represent the antigen localization of keratinocyte plasma membrane without desmosomal attachment plaques. The present method can therefore be used for differentiation of desmosomal antigen from nondesmosomal antigen without immuno-EM.
In conclusion, IF on ultrathin cryosections, with its resolution superior to that of confocal LSM, provides a better understanding of molecular distribution in combination with immuno-EM labeling, and therefore serves as a powerful new tool for investigating immunolocalization of skin antigens.
Footnotes
Acknowledgments
Supported by Grants-in-Aid for Scientific Research (Nos. 05404036 and 07457191) from the Ministry of Education, Science, and Culture of Japan, and by Keio Gijuku Academic Development Funds.
We thank Ms Megumi Sato for excellent technical help. We are grateful to Dr D.R. Garrod (University of Manchester), Dr I. M. Leigh (London Hospital, UK), Dr T. Hashimoto (Kurume University, Japan), and Dr A. Sonnenberg (University of Amsterdam, The Netherlands) for providing antibodies.