
Abstract
Thin layer-based technology in cervical cancer screening now allows both Papanicolaou staining and HPV testing on the same sample. Here, we show that in situ hybridization with catalyzed reporter deposition is a powerful HPV detection method when applied on thin-layer cervical smears, allowing distinction between two staining patterns suggestive of two different physical states of HPV DNA, where diffuse signals are suggestive of episomes and punctate signals are suggestive of viral DNA integration
Keywords
H
ISH was applied on 221 of 2400 liquid-based thin-layer cervical smears addressed at our institute for screening. Pap-stained smears were examined by two independent readers and classified according to the Bethesda system. HPV testing was applied on all abnormal smears and on normal smears and smears with minor cellular changes either on request of the clinician or for diagnosis assessment. Human cervical cancer cell lines containing a known number of HPV 16 (SiHa and CaSki 1–2 and 400–600 DNA copies, respectively) or HPV 18 (HeLa 10–50 copies) copies served as intra- and interassay controls in our ISH technique. They were a kind gift from Dr. Wazilik (IGBMC; Strasbourg, France). Cultured cell lines were either paraffin-embedded after 24-hr buffered formalin fixation or prepared using the thin-layer protocol. Cells were suspended for 48 hr in 10 ml of the same preservation fluid used for collecting cervical samples and further processed as described for cervical smears. Thin layer slides of cervical smears were prepared using the CytoRich system (Microm; Francheville, France) according to the recommendations of the manufacturer. Remaining cell suspension was used for the Hybrid Capture II test (HC II) (Digene; Gaithersburg, MD). Thin-layer slides were postfixed in 10% buffered formalin for 15 min before ISH processing.
Protein digestion was carried out with proteinase K (Enzo Diagnostics; Farmingdale, NY) for 15 min at 37C (250 μg/ml for paraffin sections; 80 μg/ml for thin-layer slides). ISH was performed using commercial DNA probes (Enzo Diagnostics) diluted 1:10 with hybridization buffer for DNA probes (DAKO; Trappes, France). The available probes for HPV screening consisted of a mixture of HPV probes 6, 11, 16, 18, 31, 33, 51 (probe mix). For HPV typing, three probe cocktails were used: HPV 6/11 (low risk), HPV 16/18 (high risk), and HPV 31/33/51 (high risk). All slides were first processed with the probe mix. In cases of positivity and if enough cervical material remained, HPV typing was carried out. The probe was applied to the slides, overlaid with a coverglass, denatured for 12 min at 96C on a hot plate, and hybridized overnight at 37C in a moist chamber. After hybridization, the coverglass was removed and slides were rinsed with Signasure wash buffer (Enzo Diagnostics), followed by a stringency wash with In Situ Hybridization Wash-reagent (Enzo Diagnostics), for 10 min at 37C. The CSA system (DAKO) was used to enhance ISH staining, according to the recommendations of the manufacturer. All revelation and amplification steps were carried out at 25C on a calibrated hotplate. VIP (Vector Lab; Burlingame, CA) was used as substrate-chromogen reagent. Sections were counterstained with methyl green, rinsed, air-dried, and coverslipped with Eukitt.
Negative controls consisted of omission of the specific viral probe, use of probes showing no specificity for HPV or known human DNA sequences, and incubation of the specimens with VIP without any other previous treatment to evaluate the endogenous peroxidase activity. Under these conditions, no hybridization signals were observed.
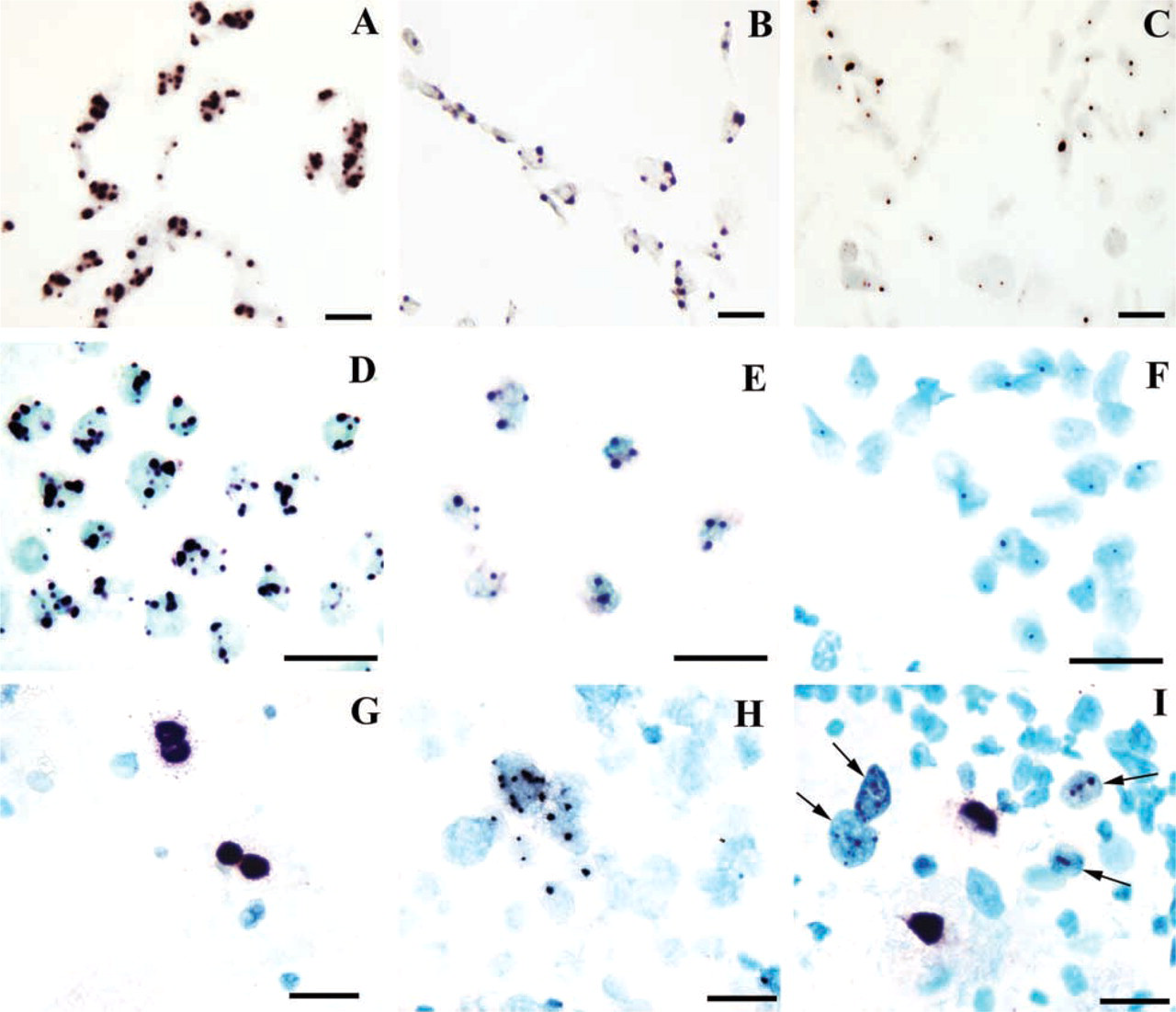
HPV 16/18 detection by ISH with catalyzed reporter deposition. Only cell nuclei are visible; cell cytoplasm has been destroyed by proteolytic treatment. (
Cervical smears with enough residual cells after ISH were processed with the HC II test according to the recommendations of the manufacturer. Seventy-three smears could be tested, including 18 smears with minor cellular changes, 33 ASCUS, 16 LSIL, five HSIL, and one carcinoma. The three cell lines were used as controls. In this test, the smears were analyzed for the presence of low-risk HPV types 6, 11, 42, 43, 44 and high-risk types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68.
For paraffin-embedded cell lines (Figures 1A–1C) and thin-layer preparations of the cell lines (Figure 1D–1F), we observed the same results. Punctate signals were present in cell nuclei with both mix probe and 16/18 probe, but not with 6/11 and 31/33/51 probes. The size of the signals increased with known copy number of HPV DNA: in SiHa cells one or two small dots, in HeLa cells usually two or three large dots, and in CaSki cells many confluent dots. This pattern of staining is comparable to that obtained with cells applied on slides by centrifugation (Lizard et al. 2001). Thus, treatment with the thin-layer technique preserves the ability to detect HPV DNA in situ. This finding allowed us to apply ISH with tyramide amplification on thin-layer cervical smears.
In our study group, 95% of the women screened had a normal smear or a smear with minor cellular changes, 2.75% showed an ASCUS, 1.7% LSIL, 0.6% HSIL and one smear was diagnosed as carcinoma (these percentages are in accordance with those of large cohorts). Comparison between HPV DNA testing and cytological findings showed that the rate of HPV detection increased with the severity of cytology, from 14% in minor cellular changes, 55% in ASCUS, 95% in LSIL, and up to 100% in HSIL and carcinoma. High-risk HPV types were mainly present, alone or associated with low-risk HPV types, whatever the cytological findings. Similar results have been observed in other published studies based on the HC II test, PCR, or indirect in situ PCR (Riethmuller et al. 1999; Manavi et al. 2001).
A good correlation between ISH and HC results was observed with the cervical smears. By using the HC test as the reference method, the sensitivity of our ISH protocol was 87.5% and the specificity 96%. For the discordant cases, it should be noted that the amount of cells used for HC was two- to eightfold higher than that used for ISH. The higher number of probes used in HC may also explain the discrepancy observed between the ISH and the HC results.
One advantage of in situ detection of HPV compared to liquid-based methods is to allow a count of positive nuclei to correlate with cytological data. Here we show that thin-layer smears are suitable for ISH, with no need for destaining before ISH as was necessary for classical Pap smears as previously reported (Autillo-Touati et al. 1998). The other advantage is to distinguish between diffuse and punctate signals. It has been shown, by comparing in situ techniques with PCR, that there is a correlation between the ISH staining pattern and the physical state of HPV (Vernon et al. 1997). HPV present as episomes leads to diffuse staining, while integration of viral DNA into host cell DNA gives punctate signals. In our study, both diffuse and punctate signals, suggestive of the episomal and integrated form of the virus, respectively, were observed (Figures 1G–1I). In LSIL we had mostly diffuse signals. In invasive carcinoma, only punctate signals (two or three dots per nucleus) were observed, in a pattern very similar to that of cervical cancer cell lines. Half of the HSIL and two cases of ASCUS also showed the same integrated pattern, in association with an episomal pattern in other nuclei. Integration of HPV DNA into the host cell genome is considered an important genetic change in cervical lesion progression towards cancer (Zur Hausen 1999). Simultaneous detection of the virus and its physical state may provide helpful information for the follow-up of the patients, particularly in ASCUS patients because 10% of them may underlie a high-grade lesion (Shlay et al. 2000). Our findings must now be compared with results of both histological diagnosis and ISH of the corresponding biopsy. In conclusion, ISH with catalyzed signal amplification is a simple and reliable technique for detecting HPV on the same sample as Pap stained cervical smear.
Footnotes
Acknowledgments
We thank Ms J. Meder and Mr J. Descamps for providing excellent technical assistance.