
Abstract
Colorectal cancer is one of the most common human cancers, for which 5-fluorouracil (5FU) is usually part of the treatment. Thymidylate synthase (TS), the target enzyme for 5FU, can be predictive for the outcome of 5FU-based therapy. TS levels in tumor samples can be determined with radiochemical enzyme assays, RT-PCR, and immunohistochemical staining. We validated TS immunohistochemistry with a polyclonal rabbit anti-human TS antibody using the avidin-biotin method. This antibody can be used on paraffin-embedded, formalin-fixed material using an antigen retrieval method with citrate buffer and microwave treatment. The antibody shows a granular cytosolic staining pattern. The reproducibility in cross-sections from colorectal tumors from 50 patients was 90% and the interobserver variability was acceptable with a kappa of 0.45. On Western blotting it detects purified TS at 36 kD, while in 5FU-treated cells the ternary complex between FdUMP, TS, and 5,10-methylene-tetrahydrofolate is clearly visible at 38 kD, with no other interfering bands. In a separate set of tumors, immunostaining was compared with enzyme levels; Western blots correlated with enzyme levels. Because both this polyclonal antibody and the monoclonal antibody TS-106 are being used for large-scale studies, we also determined whether they could be used interchangeably. No differences were observed. This polyclonal antibody is specific and gives reproducible results. A study on a larger scale is ongoing to determine the role of TS as a predictive parameter in patients with colorectal cancer treated either with postoperative adjuvant 5FU/levamisole or with surgery only.
T
Clinical drug resistance at the TS level is of relevance for response to 5FU; increased TS mRNA, insufficient TS inhibition by 5-fluoro-2′-deoxyuridine-5′-monophosphate (FdUMP), increase of TS levels after treatment are all mechanisms of 5FU resistance related to TS (reviewed by Peters and Jansen 1996). Several studies suggest a prognostic significance for TS in relation to 5FU-based therapy in advanced disease. In patients with gastric and colorectal cancer treated with 5FU-based chemotherapy, response to therapy and survival were statistically significantly related to TS mRNA (Leichman et al. 1995; Lenz et al. 1996).
In a previous study we measured TS levels enzymatically in patients with advanced colorectal cancer and found a significant relationship between the response to 5FU therapy and the TS levels (Peters et al. 1994). In rectal cancer and in advanced head and neck cancer patients treated with adjuvant and neoadjuvant 5FU-based chemotherapy, respectively, TS was an independent prognostic marker for disease-free and overall survival when measured by immunohistochemistry (Johnston et al. 1994,1997).
TS levels in patient samples can be measured by various methods. With enzymatic assays (Peters et al. 1987,1991), the number of FdUMP binding sites and the TS catalytic activity (the conversion from dUMP to dTMP) can be quantified with radioactively labeled substrate. A drawback is the requirement of about 100 mg freshly frozen tissue. With RT-PCR, the TS mRNA level can be measured (Lenz et al. 1995). This assay can be performed on small biopsy samples but needs technical expertise to measure the mRNA level reliably. A disadvantage of both assays is that the tumor morphology is lost. Because tumor samples often also contain normal cells, TS values are dependent on the purity of the samples. With immunohistochemistry, tumor and normal cells can be discriminated. Another advantage of immunohistochemistry is that this assay can be performed on a larger scale (e.g., at more centers), which is of interest for study, e.g., of patients treated with adjuvant chemotherapeutic regimens. TS expression using immunohistochemistry with a monoclonal antibody against human TS, TS-106, has been extensively characterized previously (Johnston et al. 1991,1992; Drake et al. 1993; Edler et al. 1997). The use of a TS polyclonal antibody has been reported on cytospins of tumor cell lines from different origin (Van der Wilt et al. 1993), in ELISA methods (Aherne et al. 1992; Van der Wilt et al. 1997) and in paraffin embedded material (Findlay et al. 1997).
In this article we describe the methodology and validation of the use of a polyclonal TS antibody for quantitation of TS levels in paraffin-embedded material from 50 representative patients with colorectal cancer. A secondary aim of the study was a comparison of the polyclonal antibody with the monoclonal TS-106 to establish their interchangeability. We also tested the intensity of the (immuno)staining compared with TS enzyme levels. Samples were obtained from patients who were entered in the Netherlands Adjuvant Colorectal Cancer Project (NACCP) trial in which postoperative 5FU/levamisole is compared to surgical treatment only in patients with colorectal cancer.
Materials and Methods
Tissues
Formalin-fixed, paraffin-embedded material from the primary tumors from 50 randomly selected patients with colorectal cancer were used. These patients were entered in the NACCP trial. In this trial, patients with colon and rectal cancer were randomized between surgical treatment only or surgery followed by 5FU combined with levamisole (Reynolds 1995). Samples were obtained at surgery from the group of patients evaluated in this study; 66% had colon cancer and the remainder rectal cancer. Both Dukes Stage B and C were included in this group, with an equal ratio for the colon tumors, whereas the majority of rectal tumors were Dukes B. In this patient group the male:female ratio was equal and the median age was 64 years. The majority of the tumors were moderately differentiated. From a separate group of untreated patients, we were also able to obtain biopsy specimens that were immediately frozen in liquid nitrogen for use in measurement of TS levels by an enzyme assay.
Immunohistochemical Staining
Tissue sections were cut at 4 μm, and mounted on poly-L-lysine-coated slides, and dried. The sections were deparaffinized and rehydrated by incubation twice for 3 min in 100% xylene, followed by incubation in decreasing ethanol concentrations. Antigen retrieval was necessary (Freemantle et al. 1991; Taylor et al. 1994; Brown and Chirala 1995) for the immunostaining on paraffin-embedded, formalin-fixed material with the TS polyclonal antibody (kindly provided by Dr. G.W. Aherne; Sutton, UK) or with the TS monoclonal antibody TS-106. Therefore, the sections were heated in the microwave twice for 5 min in 10 mM sodium-citrate buffer (pH 6.0) at 750 W. For the second heating step, fresh citrate buffer was used. The sections were then allowed to cool down in the buffer for at least 20 min. The sections were washed with PBS and blocked with normal goat serum (1:50) for 20 min. The primary polyclonal TS antibody was diluted 1:100 in 1% bovine serum albumin (BSA)/PBS and incubated for 1 hr at room temperature. Normal rabbit serum was used as a control for aspecific staining. After PBS wash steps (twice for 5 min), the secondary antibody (DAKO; Glostrup, Denmark), biotin-labeled (1:800) goat anti-rabbit, was applied and incubated for 30 min. The sections were rinsed again with PBS (twice for 5 min) and incubated with horseradish peroxidase-labeled avidin-biotin complex for 30 min, according to the recommendation of the manufacturer; 3-amino-9-ethylcarbazole (AEC) was used as a chromogen. The sections were counterstained with hematoxylin. All slides were examined by two observers in independent examination sessions. The whole sample was evaluated by scoring at least four high-power fields (×10 and ×40 magnification). Statistical evaluation was performed using SPSS software.
To compare the polyclonal TS antibody with the TS monoclonal antibody TS 106 (kindly provided by Dr. P.G. Johnston; then at the National Cancer Institute, Bethesda, MD) which has already been extensively characterized, we used the same protocol as above. The monoclonal antibody was 1:50 diluted in 1% BSA/PBS and incubated for 1 hr followed by incubation with the second goat anti-mouse biotin-labeled antibody (1:50). As a negative control, a mouse IgG1 antibody was used.
Western Immunoblotting and Enzyme Assays
For further characterization of the antibody with Western immunoblotting, monolayer SW1573 cancer cells in exponential growth phase were treated for 24 hr at 50% growth-inhibitory concentrations of either 5FU or the TS inhibitors AG377 and ZD1694. Treated and control cells were harvested, washed, and centrifuged, and the pellets were immediately frozen in liquid nitrogen and processed essentially as described previously (Van Triest et al. 1997). Samples were kept at −80C. The cytosolic cell fraction was isolated by lysis in buffer containing 0.1% Triton X-100, 150 mM NaCl, 10 mM Tris-HCl, pH 7.6, 5 mM EDTA, and centrifuged for 10 min at 15,000 × g at 4C. From each sample an equivalent amount of protein (50 μg) was loaded on a 12% SDS-polyacrylamide gel, followed by blotting onto nitrocellulose PVDF membranes. Thereafter the membranes were blocked overnight with blocking buffer (1% nonfat dry milk, 1% BSA in 10 mM Tris-HCl, pH 8.0, 0.15 M NaCl, 0.05% Tween-20). The primary antibody, rabbit anti-human TS (1:3000 in blocking buffer) was incubated for 1 hr. Then, the blot was incubated with the secondary antibody (1:1000 in blocking buffer), horseradish peroxidase-conjugated goat anti-rabbit antibody. Finally, the blot was stained using AEC as a chromogen. The density of the bands was quantified using a densitometer (G690; Biorad Laboratories, Nazareth, Belgium). TS enzyme levels were determined enzymatically as described previously (Peters et al. 1991; Van Triest et al. 1999).
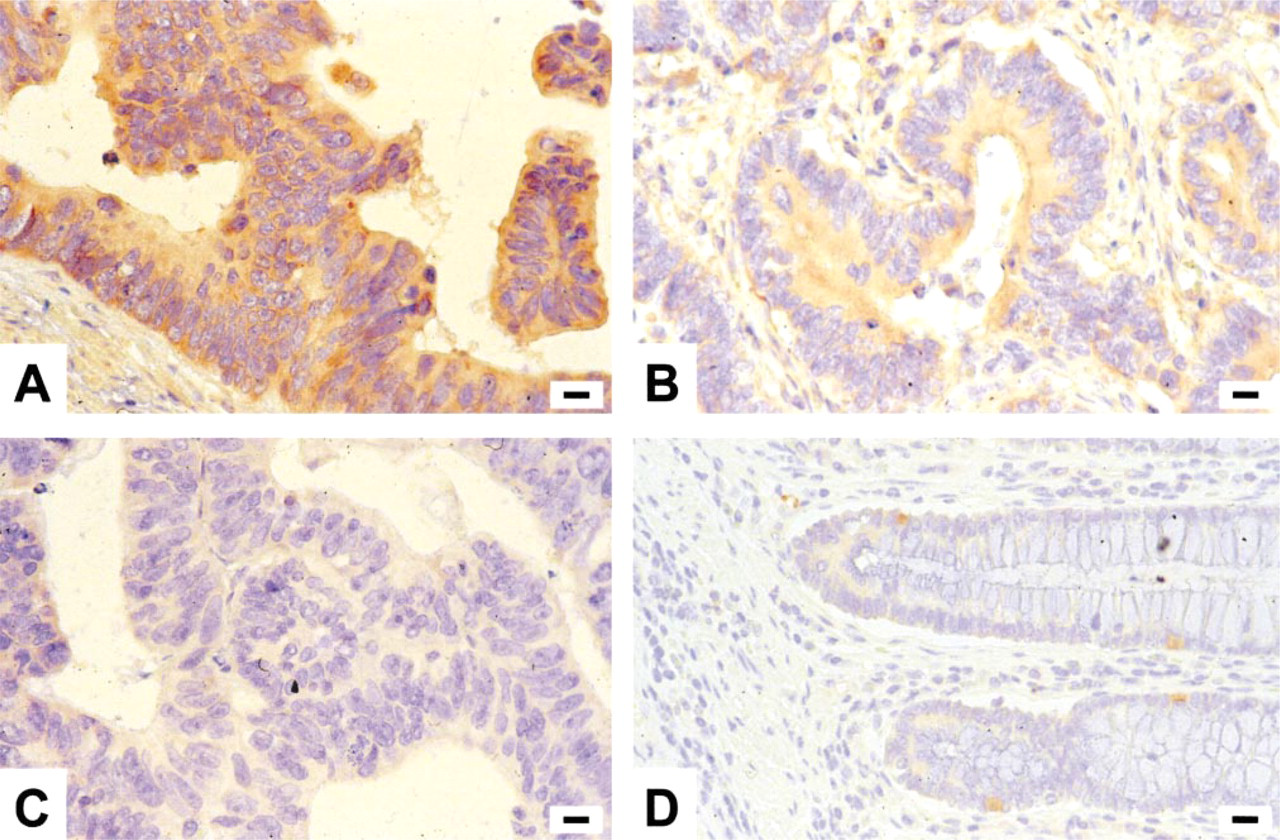
Immunohistochemical staining of thymidylate synthase (TS) in a human colon cancer tumor. The TS polyclonal antibody was used at a concentration of 1:100. (
Results
Immunohistochemistry
Antigen retrieval with citrate buffer, pH 6.0, was essential for positive staining of the formalin-fixed, paraffin-embedded tumor samples. Titration of the primary TS antibody concentration between 1:50 and 1:500 resulted in optimal staining when a concentration of 1:100 was used. Antigen retrieval was necessary; omission of this step resulted in nonevaluable samples. After the retrieval step, all samples could be evaluated. An example of a colon tumor stained with the TS polyclonal antibody is shown in Figure 1. Positive staining with the polyclonal TS antibody gave a granular cytosolic staining pattern in the tumor cells. In most tumor samples the staining was diffuse, although heterogeneity was also observed. The intensity of the staining was scored as low, intermediate, or high (1 + to 3+) and in Figure 1 an example is shown. Figure 1A is high intensity, Figure 1B intermediate, and Figure 1C low intensity. Normal colon epithelial cells showed weak positive staining, but this was much weaker than in tumor cells (Figure 1D). There was more intense staining at the proliferative zone. A colon tumor sample of a patient with high TS expression was always used as a positive control and gave a similar staining pattern in each separate experiment. The results of the immunostaining were as follows: 17 patients had 1 +, 24 had 2+, and nine patients had a high TS level of 3+. Therefore, the majoritiy of the patients had an intermediate TS intensity. The reproducibility of this staining was tested by replicate staining of 50 samples and was 90%. The interobserver variability was tested between two observers (BvT and BML) and was acceptable, with a kappa of 0.45. On 36 of the 50 samples the two observers agreed. When the observers disagreed on the results of the TS staining, the debate was on differences between 1 + or 2+ or differences between 2+ and 3+. The slides were then re-examined by both observers and agreement was obtained. This antibody was also suitable for immunostaining on cytospins of tumor cell lines and on frozen tissue (not shown). The polyclonal and monoclonal TS antibodies showed comparable results. TS staining was identical concerning the intensity of the tumor and normal tissue in 12 different samples from paraffin-embedded tumor sections. No differences in background staining could be observed between the polyclonal and the monoclonal antibody.
Western Immunoblotting and TS Activity Level
To evaluate the specificity of the antibody, TS Western blotting was performed in the human non-small-cell lung cancer cell line SW1573 (Figure 2) and in a panel of 13 human colon cancer cell lines (Van Triest et al. 1999). The band for TS was as expected at 36 kD. No additional bands were observed in this blot and no nonspecific products could be visualized, so the detection of the TS protein level was highly specific. After treatment with 5FU, a ternary complex is formed between TS, FdUMP, and 5,10-methylenetetrahydrofolate, which can be seen as an additional band in the second lane, indicated as T (= ternary complex) and N (= normal TS). The polyclonal and monoclonal antibodies were also compared during Western immunoblotting. For both antibodies, the band for TS could be visualized at the same MW. No other additional bands could be detected. The results indicated that on Western blots both antibodies were also comparable. In 13 colon cancer cell lines, intensity of Western blotting was compared with enzyme levels; a positive linear relationship was observed between both parameters (r=0.62; p<0.05). In a separate group of 32 patients, immunohistochemistry was compared with enzyme levels; here the relationship tended to be significant (r=0.53; p=0.07) (Van Triest et al. in press).
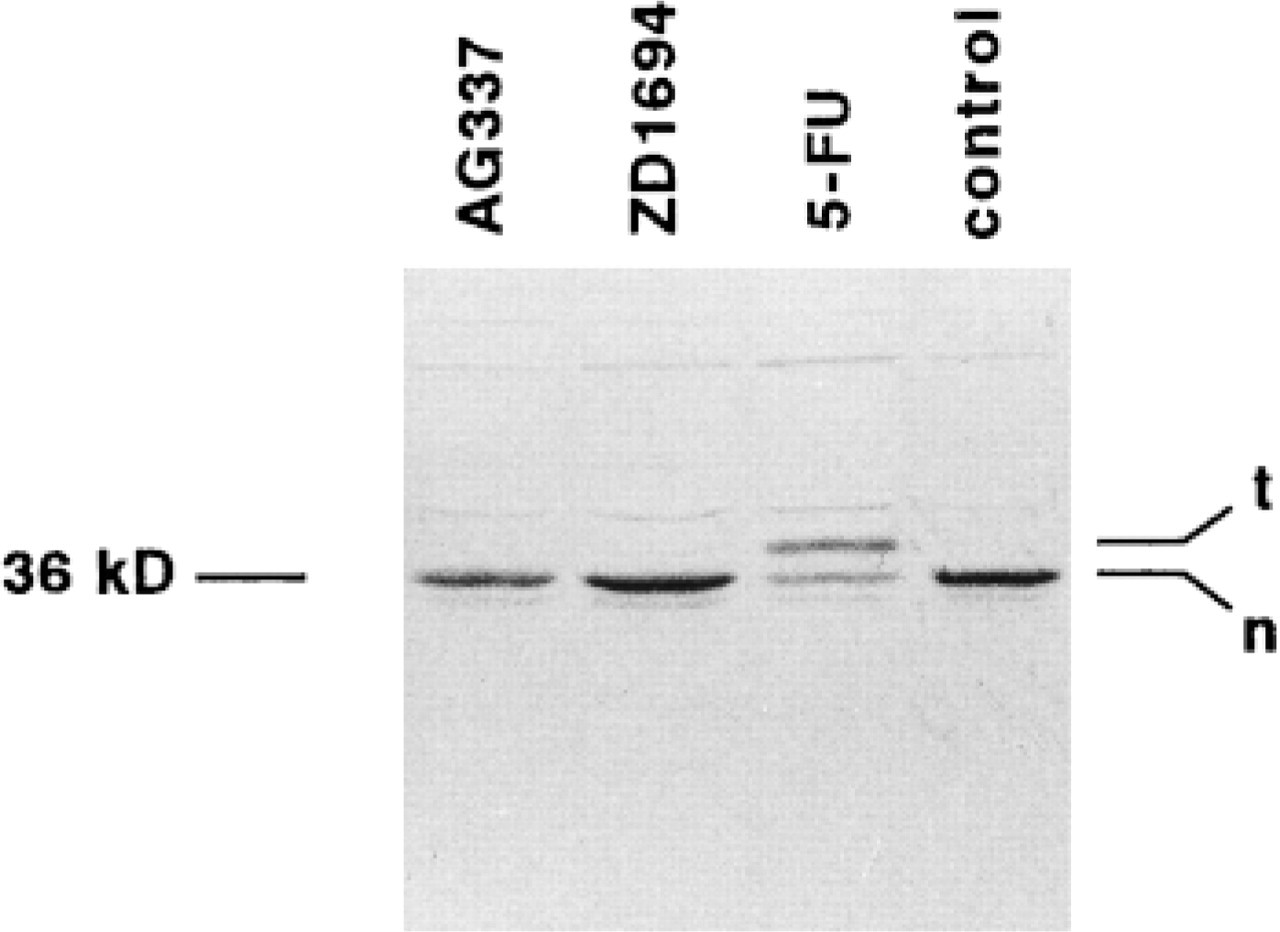
Western blot using the TS polyclonal antibody (1:3000) on SW1573 human non-small-cell lung cancer cells. Each lane represents a sample of cells treated for 24 hr with 50% growth-inhibitory concentrations of AG337, ZD1694, or 5FU. The right lane contains a sample of untreated cells. In each lane a band is observed at 36 kD, which represents the native enzyme. An additional higher molecular weight band is found in the 5FU-treated cells, which is the ternary complex formed by FdUMP-thymidylate synthase and CH2-THF.
Discussion
In this article we describe the results of the validation of a polyclonal antibody for TS staining in paraffin-embedded colon or rectal tumor material. This polyclonal antibody was highly specific and could detect the TS protein using Western immunoblotting and immunohistochemistry. A discrimination between high and low TS levels could easily be measured in 50 samples of patients with colon tumors. In the tumor material, the method for the TS immunostaining was reproducible and showed acceptable intraobserver variability.
For immunostaining with the polyclonal TS antibody, various methods of detection have been used. For detection of TS in tumor cell lines we initially used a direct peroxidase-labeled secondary antibody (Van der Wilt et al. 1993). Findlay et al. (1997) used an immunogold probe with silver enhancement for paraffin-embedded material because alkaline phosphatase-labeled secondary antibodies were not sensitive enough. This technique is indirect, and an immunoglobulin absorbed to colloidal gold is used as the secondary antiserum. The gold particles attached to the specific antibody are revealed by a silver precipitation technique. Although being a very sensitive technique, the antigen recognition strongly depends on the size of the gold probe (Holgate et al. 1983). In our study, we used a biotin-labeled secondary antibody coupled to an avidin-biotin-peroxidase complex. A disadvantage of this ABC method may be the binding of avidin to endogenous biotin. However, the very coarse granular cytosolic staining typical for binding to endogenous biotin was not seen in our samples. For the detection of TS with the monoclonal antibody TS-106, the indirect ABC method was also used for amplification of the signal (Johnston et al. 1991; Edler et al. 1997). Studies on detection of other cytosolic proteins, such as bcl-2, by immunohistochemistry in colorectal tumors also used anti-peroxidase, anti-alkaline phosphatase (Schneider et al. 1997), or the ABC method (Merritt et al. 1995) for specific detection of the primary antibody, without evidence of a very coarse granular cytosolic staining.
A comparison with the TS monoclonal antibody developed by Johnston et al. was undertaken to determine whether these antibodies could be used interchangeably. Both antibodies showed similar results for the intensity of staining of tumor and normal tissue, the background and on TS Western immunoblotting (Johnston et al. 1992; Drake et al. 1993; Edler et al. 1997) and can be used to determine TS expression by immunostaining in paraffin-embedded material such as from ECOG, NSABP, SWOG, and EORTC studies for the monoclonal antibody. The polyclonal antibody is now being used for large-scale screening of TS expression in paraffin-embedded tumor material from patients with colorectal cancer Stages B and C, entered in a randomized study, either with no further treatment or adjuvant treatment with the combination of 5FU plus levamisol. This will enable us to determine whether TS levels are of predictive value for treatment outcome of adjuvant 5FU-based therapy.