
Abstract
Nurturing psychological safety has become a vital antidote to the psychological depletion driving clinicians from healthcare. How to support the clinician's voice, the question at the heart of this study, has never been more important. Here, we explore a hidden aspect of speaking up conversations, how “receivers” experience the dialog. If, when, and how clinicians take in clinically relevant concerns from others is crucial to patient safety. Yet we know little about how different forms of speaking up impact the receiver of the message. We found that receivers of the same message may respond quite differently depending on their professional identity, context, attributions they made, and how the message was phrased. Our findings suggest several actionable practices: (1) Shift the focus of speaking up to training the receiver; (2) frame speaking up as a shared accomplishment; (3) co-create contexts of shared accountability between the speaker and the receiver.
Keywords
Introduction
The coronavirus disease 2019 (COVID-19) pandemic revealed and accentuated the demands on frontline healthcare workers. Nurturing psychological safety in healthcare systems has become a vital antidote to the psychological depletion driving clinicians from their professions (De Kock et al., 2021; Norful et al., 2021; Rock et al., 2020). Taking care of patients in pop-up spaces, with new equipment, often in newly formed teams with new colleagues, highlighted the importance of collaboration and voice in adapting clinical care on the fly. The surprising complexity and difficulty of deciding when and if to speak up in health care contexts are well-documented (Morrow et al., 2016; Okuyama et al., 2014).
This lack of speaking up has been shown to be directly attributed to patient harm (Douglas et al., 2021; Sutcliffe et al., 2004). In 2016, medical error was the third leading cause of death (Makary & Daniel, 2016), resulting in 206,201 avoidable deaths per annum within the United States hospital system alone (The Leap Frog Group, 2016). Owing to the current rate of medical error, simply being a patient, regardless of the health condition, places one at high risk of a near miss, injury causing harm, permanent disability, or even death (World Health Organisation, 2019). With the aim to help mitigate this risk, organizations implement cultural change initiatives to help employees feel safe and supported to voice concerns. The theoretical background for understanding speaking up programs in healthcare has its origins in the “exit, voice, and loyalty framework” (e.g., Farrell, 1983; Hirschman, 1970). This trichotomy saw employees having the option to be loyal (and silent), exit (without voicing concerns), or raise concerns in an organizational critique. This framework highlighted the difference between seeing speaking up with critiques primarily as negative actions instead of seeing it as the start of a positive dialog that loyalty can promote and improve current practice. While Farrell (1983) and others associate loyalty with silence and not voice, we follow Hirschman in framing critical voice, including speaking up, as an expression of loyalty that promotes learning within an organization.
Healthcare speaking-up programs are informed by concepts of silence. When professionals choose silence, and critical opinions or feelings remain unexpressed, then colleagues who work together (and their organizations) often lose the benefit of information that could improve how they work, learn, and innovate (Argyris, 1993; Edmondson, 2012, 2018; Morrison & Milliken, 2000). Empirical research in the last 20 years has highlighted the many drivers of silence (Detert & Edmondson, 2005; Detert & Edmondson, 2011; Detert & Treviño, 2010). Detert et al.’s work on silence has demonstrated that people hold “implicit voice theories,” internal causal models about the likely consequences of speaking up (Detert & Edmondson, 2011). In contrast, creating a context in which voicing ideas is frequent (versus episodic) spurs innovation (Nawaz et al., 2014), and accelerates learning (Gittell, 2016). Leader inclusiveness behaviors nurture a context in which crucial safety or process improvement information is more likely to be shared (Nembhard & Edmondson, 2006).
It is in this conceptual context that frames how healthcare organizations attempt to minimize unhelpful or risky silence and maximize proactive dialog that shares meaningful, even critical insights. Healthcare organizations make the leap from concept to practice by teaching individuals how to speak up via prescriptive mnemonics, regardless of who the receiver is, or the context of the conversation, for example, CUS: I’m Concerned, I’m Uncomfortable, this is a Safety issue (Hanson et al., 2020), and the two-challenge rule: It is your responsibility to assert your voice at least two times to ensure it was heard (Agency for Healthcare Research and Quality, 2022), and often advocacy/inquiry is used to help frame the message in conjunction with the two challenges (Pian-Smith et al., 2009). The main objective of the mnemonics is to support the speaker, by providing a framework to promptly escalate their concern. The speaking-up messaging aims to be respectful and accommodating to the receiver. However, there is currently a lack of receiver-focused studies specifically evaluating what an accommodative message is and in what context. The mnemonics are taught to be used in all circumstances, no matter who the receiver is, for example, discipline or seniority level, or the context (who is present, clinical situation, level of urgency). If successful speaking up is viewed as competently using a mnemonic, then it follows that speaking up is understood as a skill. This skill can be simply fostered by continually teaching employees how to speak up, whilst implementing cultural support structures to enable this voice. Yet despite this work, speaking-up interventions have overwhelmingly remained resistant to training due to complexities within healthcare, such as hierarchical power imbalances (Jones et al., 2021; Pian-Smith et al., 2009). As a result, speaking up remains difficult and medical errors ensue (Makary & Daniel, 2016). The problem maybe that these programs do not pay equal attention to the training of receivers of the speaking up messages: Speaking up is viewed as the work to be undertaken, rather than a conversation between two equally accountable interactants (speaker/receiver). If, when, and how clinicians react and take in clinically relevant concerns from others is crucial to patient safety.
The lack of receiver training within speaking-up programs is perplexing. Receivers are thoroughly documented as one of the key barriers to voice through speakers fearing retribution (Fisher & Kiernan, 2019), being ignored (Garon, 2012), feelings of futility due to lack of receiver action (Jones et al., 2021), the risk of impairing professional relationships (Schwappach & Gehring, 2014b), fear of the receiver judging the speaker's clinical competence (Feltrin et al., 2019), and fear of hostile receiver responses (Morrow et al., 2016). In this paper, we explore this neglected aspect of speaking up conversations, and how “receivers” experience the dialog. This study aims to understand the role of the receiver in healthcare speaking-up conversations, especially receivers’ perceptions of a speaking up situation. Understanding these perceptions can inform training interventions to enhance how speaking up “lands” on receivers and shape their subsequent responses.
Background
Uncovering mechanisms that strengthen employee retention and cultivate organizational cultures and allow employees to recover a sense of meaning and identity at work, is part of the role of organizational scholars in this peri-pandemic period. In the view of this, we applied Communication Accommodation Theory (CAT: Giles, 2016) which has previously been fruitfully applied to understanding intergroup relationship dynamics that underpin health communication interactions (Watson & Soliz, 2018). We use CAT as a novel approach to investigating the speaking-up context specifically to understand the communication needs of the receiver. CAT is an interpersonal and intergroup theory of communication that is informed by Social Identity Theory (SIT) (Tajfel, 1974) and Attribution Theory (Kelley, 1973). CAT offers a useful model within speaking-up interactions, by explaining how individuals attune to their conversational partner (or not) and what impact this has on voice and message reception. A theoretical example of the impact of voice (receiver's voice) within a speaking-up interaction may be, the extent to which a receiver believes the speaker has displayed behaviors appropriate to their own communication needs and level of competence. This evaluation will influence the receiver's overall thoughts and opinions of the interaction. These evaluations may not always be accurate, as SIT propositions, interactions are influenced by each interactant's cultural norms, beliefs, values, and salient social identities, for example, clinical discipline or level of seniority, (Gallois et al., 2015).
Individuals use specific communication strategies to manage the social distance between their two social groups. For example, if a junior nurse is speaking up to a medical officer and the nurse perceives the medical officer receiver is trying to meet their conversational needs (cognitive, affectual, and/or linguistic), enhance their understanding and/or reduce the social distance (reduce their differences, such as power differentials), the nurse speaker would likely evaluate this as accommodative behavior (accommodative stance of the medical officer [doctor]) (Gasiorek, 2013). If the nurse perceives the medical officer has made no attempt to reduce the social distance or deems the medical officer has been intentionally unhelpful, or patronizing, the behavior will more likely be evaluated as nonaccommodative (nonaccommodative stance), thereby increasing the social distance between the two discipline groups.
Drawing on Attribution Theory, CAT proposes that people within an interaction also make attributions (judgments) of others’ motives and intentions based on internal causes (intention to act that way), or an external one (the situation) (Gallois et al., 2015). Attributions can be made about individuals, or entire groups, for example, a clinical discipline. When inaccurate character-based (dispositional) attributions are made toward an individual, it is known as the “fundamental attribution error.” According to CAT, attributions made about one's speech partner will influence the behavioral strategies an individual will deploy. Positive attributions can help enable communication by holding an interactant in high regard and believing their behavior is well intended. For example, the application of the CAT strategy “appropriate emotional expression,” can help regulate the receiver's own emotions and emotional expressions (warmth, happiness, appreciation) allowing the making of more positive attributions to maintain the social relationship with the speaker (Giles, 2016). The demonstration of “inappropriate interpersonal control” behaviors, can be influenced by the making of negative attributions, for example, the belief an interactant's intent is to cause embarrassment or harm. These attributions can result in the maintenance or extension of existing power imbalances.
When negative attributions shift from an individual to an entire group, thereby viewing the group as a homogenous entity, stereotyping can ensue. This stereotyping can lead to discriminatory behavior, negatively impacting communication. An example would be when a nurse speaks up and feels that their concern is ignored by the doctor. The nurse attributes that perceived negative receiver behavior to all doctors, and creates a stereotype that doctors are not interested in the opinion of nurses. This group attribution is known as the “ultimate attribution error” (Hogg et al., 1995; Pettigrew, 1979, p. 464). Thus, miscommunication may occur because of the interpretation of the behavior and the attributions made about the group or group member, rather than the behavior itself (Gudykunst, 2004). Connecting this phenomenon to CAT, we can show that by misattributing the doctor's intent, the nurse evaluates the doctor's behavior as nonaccommodative, which in turn maintains or even increases the social distance between the groups (e.g., between the clinical disciplines), influencing the nurse's communication behavior in both the immediate and future interactions. Collectively drawing on Social Identity and Attribution theories, CAT posits that social identity (group membership), sociohistorical background (past experiences with a particular group, and group cultural norms) and the attributions each makes of the other, influences how people behave within an interaction. The application of this theory may help explain why speaking up remains difficult and why the receiver is an often-cited barrier.
Barlow et al. (2023) used a vignette approach to investigate receiver behavior. Participants completed two vignettes, each one within a different conversational context: one where there was a breach in Personal Protective Equipment (PPE) where the patient was present, the other, a breach in Hand Hygiene (HH), where the multidisciplinary team was present. Speaker stance was randomized and counter-balanced across the two vignettes, meaning that each participant was receiver of one accommodative and one nonaccommodative speaking-up message. Findings showed that the discipline and seniority of the speaker, their accommodative stance (accommodative or nonaccommodative), and the receiver's discipline, significantly influenced the receiver behavior and subsequent evaluations of the interactions (Barlow et al., 2023). Further, nurse/midwife and allied health receivers rated the message as more acceptable when the speaker used an accommodative stance compared to when the speaker was nonaccommodative. However, medical officers did not rate one speaker stance as being more acceptable than the other, suggesting they found both stances reasonably acceptable. To date, however, the field lacks a clear understanding of what factors make a message more or less acceptable. Such an analysis is crucial to enhancing speaking-up interactions, and essential for improving patient safety. Therefore, we extend the research of Barlow et al. (2023) and undertake a qualitative analysis of the factors that influenced appraisals of message acceptability, using short answer responses provided by participants. As CAT proposes that speaker stance (accommodative vs nonaccommodative messaging), professional identity (e.g., clinical discipline) and conversational context (clinical situation and/or the presence of others) can influence behavior (all elements present within the vignettes), we, therefore, posed two research questions: How does speaker stance and conversational context influence how a speaking up message is received and evaluated? How does receiver group membership according to clinical discipline (nurse/midwife, allied health, medical officer) influence message reception?
Methods
Participants
Two hundred and eight health professionals from a large single site, Australian metropolitan health service consented to participate in the study. The participants were nurses/midwives, inclusive of registered nurses, midwives, and enrolled nurses (n = 142), allied health professionals, consisting of pharmacists, physiotherapists, radiologists, and social workers (n = 44), and medical officers (doctors) (n = 22). See Table 1 for participant characteristics.
Participant Characteristics (n = 208).
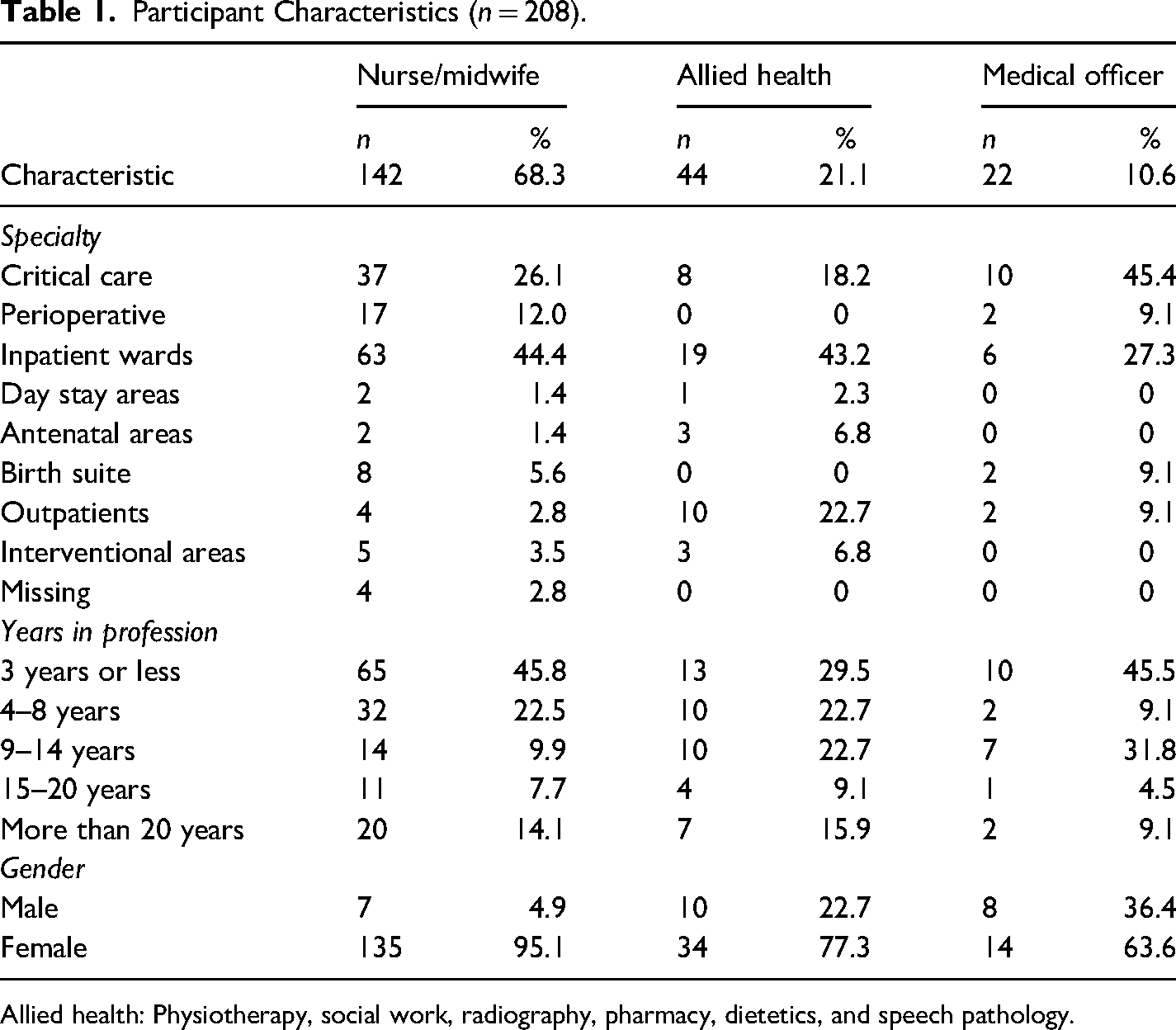
Allied health: Physiotherapy, social work, radiography, pharmacy, dietetics, and speech pathology.
Materials
The vignettes posed two hypothetical clinical situations where participants were receivers of speaking messages within the described scenarios (see Barlow et al., 2023). A vignette approach is a form of mental simulation, similar to the critical event or behavioral event interviewing, that allows the respondent to describe how they would or have responded to similar situations (Flanagan, 1954; McClelland, 1998). Study participants responded within their normal clinical role and seniority level, see Appendix A for vignette examples. In each vignette, the conversational contexts (PPE, HH; presence of the patient or team) and speaker characteristics (discipline and seniority) were defined. The contexts were varied as voice climate (clinical situation) (Morrison, 2014), and the presence of other people (Schwappach & Gehring, 2014a), have shown to be influential contributors within the speaking up context. After reading each vignette and rating the acceptability of the message, the receiver (study participant) was asked to write a short answer to “please explain why you think this behaviour [outlined in the vignette] was acceptable or not.”
The accommodative communication behavior in the vignette applied the conversational strategy called “advocacy/inquiry” (Argyris, 2002; Minehart et al., 2012; Rudolph et al., 2006), which aims to accommodate to the receiver's communication needs by the speaker sharing their thinking, stating their concern, and asking for the receiver's perspective on the situation. This conversational framework has been previously studied within healthcare speaking-up context (Pian-Smith et al., 2009). Additionally, the use of advocacy/inquiry was underpinned by the principle called The Basic Assumption (Clark & Fey, 2020, p. 141; Rudolph, 2022) That is, I should hold the opinion that the person I am communicating with is intelligent, capable, wants to do their best and wants to improve. In this way, respect is given, rather than earned and aims to help individuals make positive attributions about the person they are interacting with. In contrast, the nonaccommodative speaking-up message in the vignettes used language that camouflaged the speakers’ assertion in a question and was not curious to the receiver's perspective. It was phrased as a statement, was potentially patronizing and/or hinted at a problem, rather than directly stating it.
Procedure
Each participant responded to a paper-based survey about the two vignettes. A sample of convenience was used. The research participants were attendees to the organization's speaking up program, as this forum posed a rare opportunity where multiple disciplines with protected (nonclinical) time were gathered. Participation in the study was voluntary and was not a requirement for program attendance or successful completion. After four months of data collection, attendance of allied health and medical officers was lower than anticipated, and thus a purposive sample was recruited. Attendance was low in these cohorts as the program was reliant on a self-enrolment process and the newly implemented program had not yet fully achieved traction within certain disciplines. With the support of the relevant clinical directors, medical officers, and allied health were invited to complete the survey during nonclinical time, for example, at staff meetings, and education forums. The lead author attended the forums to explain the study and invite participation. To prevent coercion, the lead author left the surveys at the forums for voluntary completion. The short answer responses were entered verbatim into a Microsoft Excel spreadsheet and uploaded into NVivo (QSR International, 2018) for analysis. Data collection occurred between May and December 2019. The study had ethics approval HREC/18/MHS/78.
Data Coding
A subjectivist inductive approach was adopted for this qualitative study. This approach views knowledge as subjective, where one person's understanding of a phenomenon may differ from that of another, and acknowledges that an individual's social perceptions are context dependent (Varpio et al., 2020). Thus, the responses to the short answer question in each clinical context (PPE and HH) were analyzed following the six essential steps for inductive thematic analysis (Braun & Clarke, 2006, p. 87). Braun and Clarke explain that the inductive approach identifies patterns of meaning and generates themes of knowledge that emerge from the data. After identifying the emerged themes, CAT was then applied to help explain the findings. Qualitative analysis followed and complied with the consolidated criteria for reporting qualitative research requirements.
The qualitative data underwent four rounds of coding and refining of main and subsidiary themes by the first author (MB). Initially, four themes and nineteen subsidiary themes were identified. All themes (main and subsidiary) were entered into a codebook and 30% of the data were independently double coded by a second member of the research team (BW), resulting in the refinement of the number of subsidiary themes. The data were reanalyzed according to the new structure and codebook. The two coders MB (nurse) and BW (psychologist) met regularly to ensure agreement of the data, with a continual review of the subsidiary themes. Where agreed, subsidiary themes that were similar were merged, and those with minimal supporting text to generate a clear interpretation, were removed. At the end of the analysis, four themes and nine subsidiary themes emerged. After coding, NVivo transcriptions were exported back into a Microsoft Excel spreadsheet, cleaned, and calculated for frequency of occurrence by both speaker stance (accommodative, nonaccommodative) and vignette to understand if clinical situation (PPE, HH), conversational context (who was present: Patient or team) and/or stance, influenced receiver evaluation. Frequency of codes helped to understand patterns within and between professional groups.
Results
Of the total participants who completed the vignette surveys (n = 208), 77.4% of participants provided a response to the short answer question, with 315 open-ended responses across the two vignettes: 160 for PPE scenario (patient present) and 155 for HH scenario (multidisciplinary team present). Table 2 presents the four main and the nine subsidiary themes with exemplar statements. Theme one, “The presence of others,” incorporated references to the conversational context, who was present during the interaction. Themes two and three, “The manner in which the message was delivered” and “What was said mattered” described aspects of the speaker's communication behaviors. The manner in which the message was delivered referred to the receiver's perception of the tone of voice of the speaker based on how the message was phrased, and/or if the receiver described the message as being delivered in a respectful and/or professional way. Two subsidiary themes emerged: “Appropriate speaker manner” and “Inappropriate speaker manner.” There were clear differences in how receivers evaluated the speaker's manner depending on speaker stance, and these descriptions were consistent across the vignettes, confirming the importance of accommodative stance. “What was said mattered” encapsulated the receiver's descriptions of the speaker's choice of words or phrases used and the actual content of the message (the concern). Receivers described what was said as a key contributor to the acceptability of the message. The main theme had three subsidiary themes: Appropriate and Inappropriate phrasing and Perceived validity of the concern.
Themes and exemplar statements for why the speaking up message was acceptable or not.
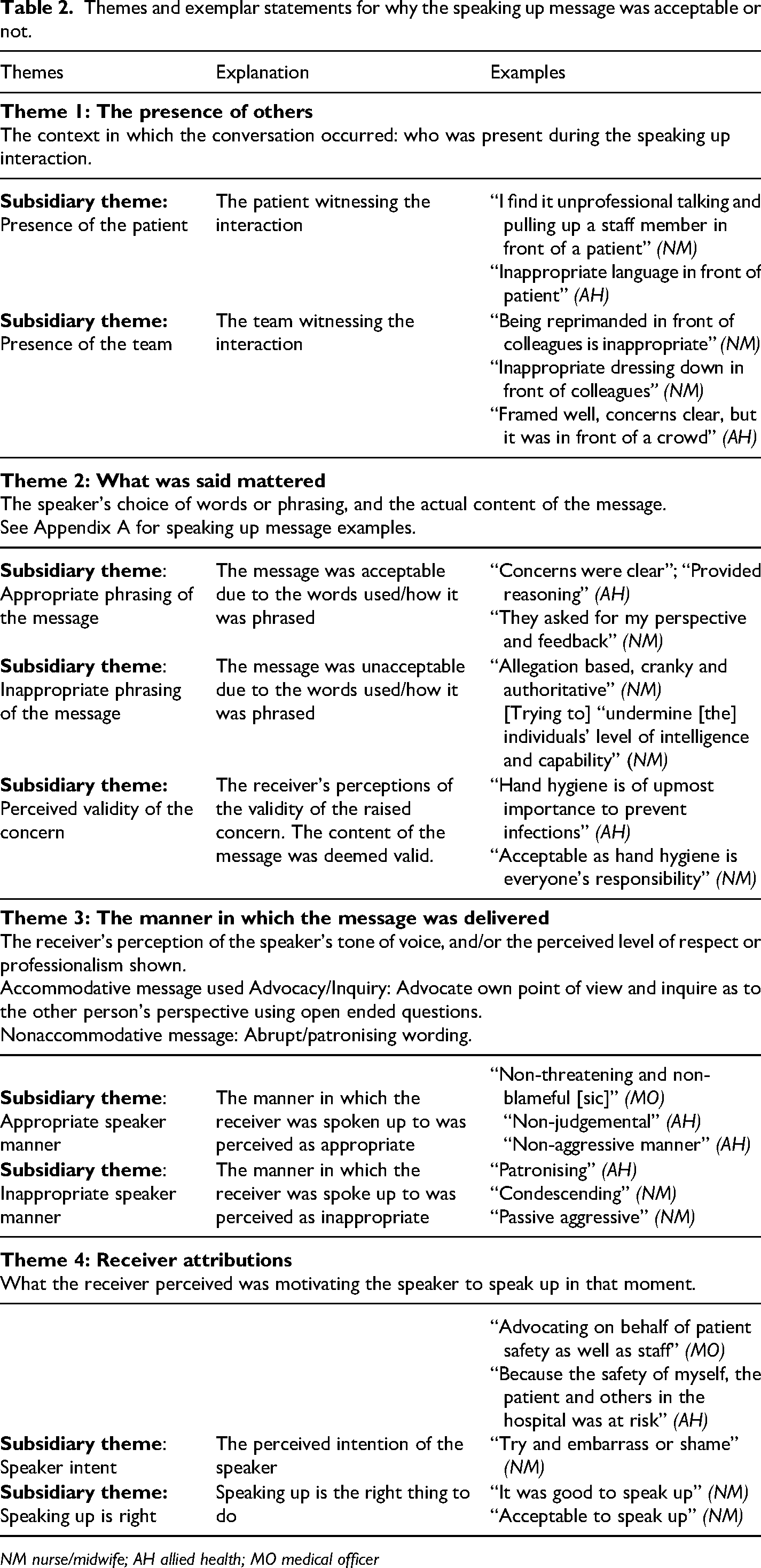
NM nurse/midwife; AH allied health; MO medical officer
Theme four, “Receiver Attributions,” focused on the receiver's perceptions of the speaker's motivation to speak up. That is, how the acceptability of the message was influenced by what the receiver perceived was motivating the speaker to speak up at that moment. There were two subsidiary themes: Speaker intent and Speaking up is right.
Out of the 315 responses, only one comment was made about the influence of the clinical situation (breach in PPE or HH), therefore no future analysis was undertaken on this variable. What was of influence was the interplay between who was present, speaker stance, and attributing positive intent to the speaker's motivation for speaking up.
Figures 1a–c display the patterning of themes and the influence of stance within each receiver group.
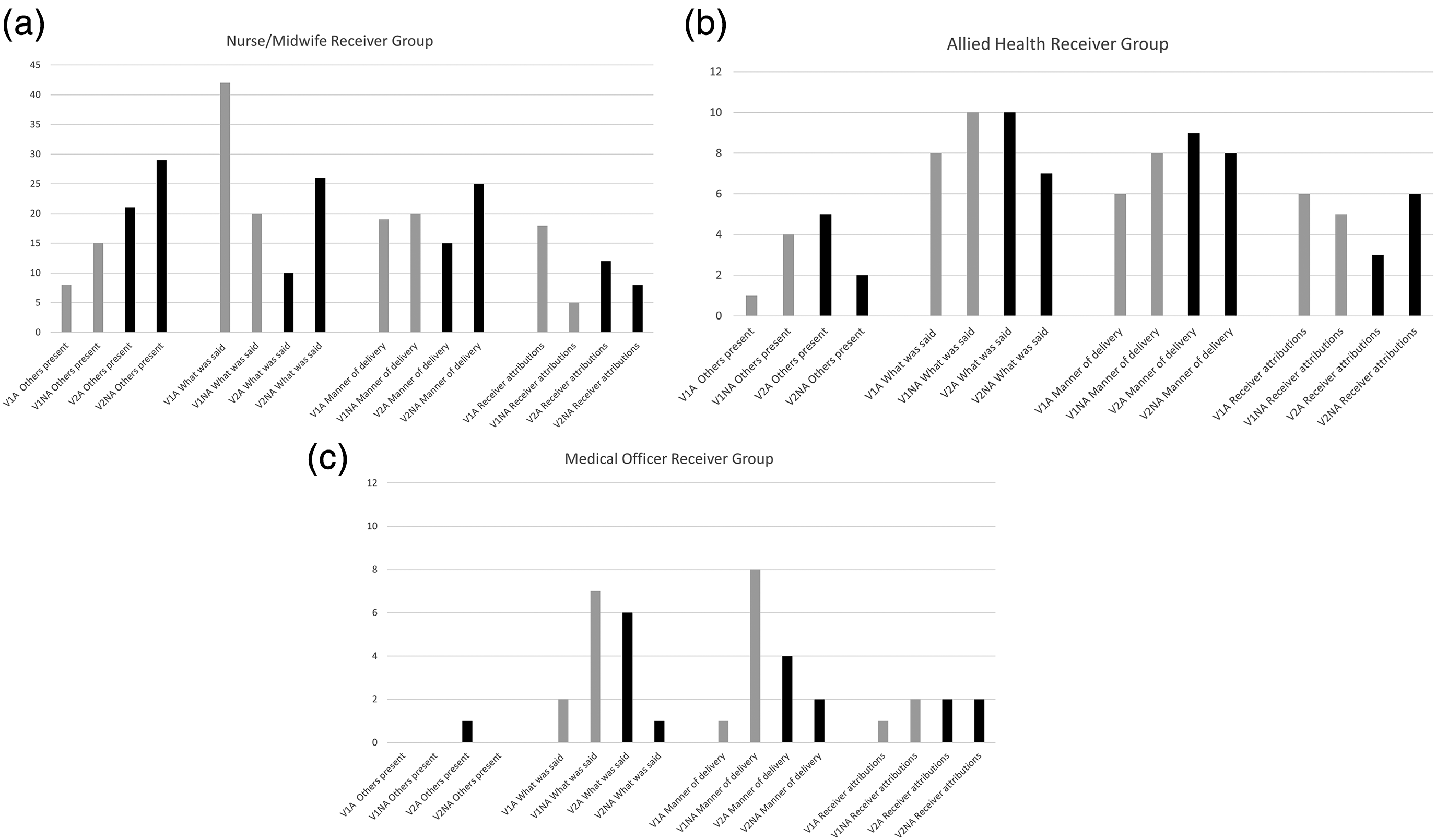
(a) Nurse/midwife receiver frequency of themes according to vignette and speaker stance. (V1 = vignette one, presence of the patient; V2 = vignette two, presence of the multidisciplinary team; A = accommodative stance; NA = nonaccommodative stance). (b) Allied health receiver frequency of themes according to vignette and speaker stance. (V1 = vignette one, presence of the patient; V2 = vignette two, presence of the multidisciplinary team; A = accommodative stance; NA = nonaccommodative stance). (c) Medical officers receiver frequency of themes according to vignette and speaker stance. (V1 = vignette one, presence of the patient; V2 = vignette two, presence of the multidisciplinary team; A = accommodative stance; NA = nonaccommodative stance).
Theme 1: The Presence of Others
This theme describes receivers’ comments regarding the influence of an audience on the interaction, the patient, or the multidisciplinary team. There was a considerable difference in the impact the presence of others had on the different receiver groups. The presence of others was most frequently reported by the nurse/midwife receiver group. Although this receiver group did not find receiving the message in front of the patient acceptable “because she/he shouted at me in front of the patient. It would make both of us uncomfortable,” it was deemed even more unacceptable when in front of the multidisciplinary team. Especially when speaker stance was nonaccommodative, for example, “inappropriate dressing down in front of colleagues,” and “the person could have asked me if she/he can talk to me outside the room” (NM), see Figure 1.
Only a small number of allied health receivers across both vignettes reported the presence of others as an influential factor to message acceptability “They should have taken me aside to talk to me—unacceptable behaviour” and “Framed well, concerns clear, respectfully asked but in front of a crowd.” Only one medical officer reported the influence of an audience, in that the message was acceptable, as it did not occur in front of the patient (occurred in front of the team).
Theme 2: What was Said Mattered
Three subsidiary themes emerged: Appropriate and inappropriate phrasing and perceived validity of the concern.
Appropriate Phrasing of the Message
Across both vignettes, clinicians from all receiver groups positively evaluated the accommodative message as more acceptable, due to how the message was phrased. This was achieved as the speaker “stated the facts” (NM) of the situation, the speaker “explained their reasoning” (NM), thereby helping to provide clarity of the concern. Nurses/midwives reported phrasing of the accommodative message positively influencing the acceptability of the message, more when delivered in front of the patient than in front of the team. As one allied health member reported, the accommodative messaging sought the receiver's perspective “gave me the opportunity to share my point of view” (AH), thereby enhancing their evaluation. As opposed to nurses/midwives, allied health and medical officers reported accommodative phrasing as positively influencing message acceptability more so in front of the team than the patient.
Across all receivers, only one receiver in each nonaccommodative vignette (nurse/midwife on both occasions) believed the message to be appropriate and acceptable; “the wording was acceptable” (NM).
Inappropriate Phrasing of the Message
The phrasing in the nonaccommodative stance was overwhelmingly evaluated as inappropriate by all receiver groups. Receivers described the message as being based on allegations, being judgmental, and it was difficult to understand what the speaker was concerned about, for example, “did not make her point clear” (AH) and “was acceptable [to speak up] but could have been phrased better” (AH). Nurses/midwives reported the unacceptability of nonaccommodative phrasing more with the presence of the team, whereas allied and medical officers reported this more frequently when in front of the patient.
A small number of nursing/midwifery and allied health receivers thought the accommodative messages in both vignettes were inappropriate. One participant stated they felt they were being lectured to, and another thought the content of the message “could have been delivered in a more professional way” (NM).
Perceived Validity of the Concern
Receiver's perceptions of the validity of the concern, influenced their evaluated acceptability of the message. All receiver groups reported validity of the message more when speaking up occurred in front of the patient than the team. Nurses/midwives most frequently reported in the accommodative stance, for example, “PPE and protocol is put in place for a reason” (NM), allied health evenly across both accommodative and nonaccommodative messages, and medical officers in the nonaccommodative messages, for example, “accurate content” (MO).
Theme 3: The Manner in which the Message Delivered
Two subsidiary themes emerged: “Appropriate speaker manner” and “Inappropriate speaker manner.” There were clear differences in how receivers evaluated the speaker's manner depending on speaker stance and professional identity.
Appropriate Speaker Manner
Across both vignettes and when the stance was accommodative, the manner of the speaker was overwhelmingly evaluated as appropriate and described as “respectful,” “non-judgmental”, and “non-threatening” by members in all discipline groups. The major descriptor by receivers was the accommodative message was “polite.”
For nurses/midwives, appropriate speaker manner influencing the acceptability of the message was described more in the presence of the patient than the team “acceptable because the manner in which it was delivered was fine and appropriate” (NM). Whereas allied health and medical officers described the acceptability of appropriate speaker manner more when the team was present as opposed to the patient, for example, “the nurse just let me know the situation in a non-threatening and non-blameful manner” (MO).
A small number of nurses/midwife and allied health receivers (six) described the manner in the nonaccommodative message as appropriate and only in the presence of the team, for example, “The doctor is being polite and professional.”
Inappropriate Speaker Manner
Conversely, the description of inappropriate manner occurred predominately when the speaker stance was nonaccommodative across both vignettes, with receivers using descriptors such as “rude”, “aggressive”, and “patronising.” Nurses/midwives and allied health, across both message types, consistently described the unacceptability of the nonaccommodative speaker's manner due to, “unacceptable tone,” and the speaker being “condescending” and “unprofessional.” Figure 1c highlights that medical officers reported the speaker's nonaccommodative behavior influenced their evaluation of message considerably more when in front of the patient compared to the team, for example, “unacceptable in how the information was delivered i.e., tone of voice.”
Theme 4: Receiver Attributions
The theme of “receiver attributions” described how the acceptability of the message was influenced by what the receiver perceived was motivating the speaker to speak up in that moment. There were two subsidiary themes: Speaker Intent and Speaking Up is Right.
Speaker Intent
When receivers described the making of attributions about the speaker's intent, the most frequently attributed motive for speaking up was the speaker's concern for patient and/or staff safety. Nurse/midwife receivers described positive attributions concerning patient/staff safety most frequently with the accommodative message in front of the patient, the “doctor only looking out for patient's best interest” but did on occasions attribute positive intent when receiving a nonaccommodative message, for example, “Acceptable in the way of advocating good hand hygiene.” Whereas allied health receivers made more positive attributions when the stance was nonaccommodative, “acceptable due to safety,” and “the person is concerned about my wellbeing and the person does not know what I am doing.”
The perceived motivation for the speaking up message was seemingly not an important factor for medical officers, with only three references to positive speaker intent regardless of how the message was delivered and who was present, for example, “It sounds a bit accusatory, but it's for patient care.”
Outside of concerns for safety, there were eight occurrences across nurse/midwife and allied health receivers where positive attributions were made regarding the speaker's intent: The speaker was aiming to be either helpful or unhelpful. When helpful, “they were asking to improve their own practice.” When unhelpful, speaker intent was to “try and embarrass or shame” the receiver.
Speaking Up is Right
A smaller subtheme emerged that across all contexts (speaker stance and who was present) and irrespective of whether the message was evaluated appropriate or not, receivers acknowledged that the act of speaking up was the right thing to do “it's ok to speak up for safety—being accountable” (NM). When comparing by stance across both vignettes, this acknowledgment predominately occurred when the stance was accommodative, “it was good to speak up.”
Discussion
A thematic qualitative analysis approach was used to investigate how the speaker stance, context, and the receiver's professional identity (discipline) influenced the level of acceptability of a speaking-up message. The findings clearly show that receivers of a speaking-up message were influenced by the perceived level of psychological accommodation of the speaker (stance), the speaker's perceived intent and motivation for speaking up (attributions), and the presence of other people. These factors impacted their overall evaluation of the message. Clearly, there is more to how a receiver evaluates a message than what is said. Even though in our quantitative study receiver discipline influenced the rated level of acceptability of the message, qualitatively all disciplines consistently described the accommodative stance being more respectful, polite, and professional compared to the nonaccommodative stance which aligns with theoretical expectations (Gallois et al., 2015). From the results, we can gleam that how the message was phrased and the manner in which it was delivered was important. These findings are consistent with the receiver study by Long et al. (2020) who identified message content and manner as key influential factors for message reception. In our study, receivers positively evaluated the use of advocacy/inquiry to phrase their concern (accommodative stance). Receivers described the accommodative concern as being clearly articulated, and easily interpreted, which is essential for error prevention, and/or prompt corrective treatment (The Joint Commission, 2016). Receivers described the open-ended question (inquiry), actively sought their point of view, and gave them the opportunity to share their perspective. It appears that the active invitation to share thinking in a respectful manner is important and has been shown to help individuals feel less constrained, and better able to engage safely in the conversation, enhancing speaking-up behavior (Brykman & Maerz, 2022; Edmondson, 2003; Kolbe et al., 2022; Nembhard & Edmondson, 2006; Yang et al., 2021). These findings are supported by a study within pharmacy (Chevalier et al., 2017), which found that accommodative messages elicited a sense of openness and reduced the level of uncertainty within an interaction.
Interestingly, across the accommodative vignettes, despite rating the message itself as acceptable (Barlow et al., 2023), a percentage of nurse/midwife and allied health receivers qualitatively described that overall, the interaction was not acceptable, due to the confounding contextual factors, for example, the presence of an audience. This juxtaposition demonstrates the complexity of these conversations within healthcare and why the conversational context plays an integral role in CAT. This may also explain why standardized speaking up mnemonics aren’t consistently enabling voice (Jones et al., 2021; Pian-Smith et al., 2009), again, as message reception is influenced by more than just what is said.
An important element of CAT is the attributions an individual makes about their speech partner, influencing behavior choices (Gasiorek & Giles, 2015). An individual's cognitive processes, such as making positive attributions, influences behavioral strategies deployed and can set the tone of the interaction (Schein & Schein, 2021). Within our study, concern for patient and/or staff safety was the main attributed motive for speaking up. Receivers were making internal, or dispositional attributions about the speaker, rather than external/situational attributions. Attributing positive intentional behaviors of the speaker helped to position the receiver to evaluate the message as acceptable, even when the message delivery was not. This helped the receiver's avoid making a fundamental attribution error (Berry & Frederickson, 2015). These positive attributions made about the speaker are aligned with the principle of the Basic Assumption, which holds people to high standards, while treating them with high regard (Rudolph et al., 2006). Nurses/midwives found holding the Basic Assumption easier to do when the stance was accommodative, and allied health, when the stance was nonaccommodative. Interestingly, medical officers in this study, contrary to the propositions of CAT, did not make any attributions regarding speaker behavior. Further research is required to see if medical officers need training in making positive attributions/holding the Basic Assumption, or this is something they do not see as a requirement to engage in a speaking-up conversation.
Being spoken up to in front of others, particularly the multidisciplinary team when the stance was nonaccommodative, seemed to be highly confronting for nursing/midwifery receivers. Traditionally viewed as lower status, being spoken to in this manner in front of colleagues potentially reinforces their positioning and undermines the group's self-esteem (Scheepers, 2009). Conversely, across our vignette studies, medical officer receivers in both the qualitative and quantitative analysis were not influenced at all by the presence of other people (Barlow et al., 2023). This may be due to their traditional hierarchical positioning (Rogers et al., 2020) and their higher symbolic capital within health organizations, for example, greater recognition, professional prestige, and viewed as a higher social class (Bourdieu, 2018; Pavithra et al., 2022).
Implications for Practice
Our results demonstrate the complexities within healthcare speaking up and why gaining the receiver's perspective is vital for enhancing speaking up and error mitigation. Our previous work found that nurses/midwives and allied health found accommodative messages significantly more acceptable than nonaccommodative (Barlow et al., 2023). This study builds on this work and demonstrates that even when the message itself is deemed acceptable, receivers can be dissatisfied with the overall interaction due to contextual factors such as the presence of other people. This indicates that standardized mnemonics may support the speaker but are not meeting the needs of the receiver and may negatively impact shared clinical decision making. Supported by Brykman and Maerz (2022), voice (speaking up) within undergraduate business students was impacted by both individual characteristics (disposition) and context (situation). It may be that receivers are not ignoring the speaker as commonly reported (Pattni et al., 2019), rather their voice is inhibited due to the context. Additionally, Burris et al. (2022) found that how a message was delivered, such as an employee using both a combination of prohibitive and proactive voice, impeded comprehension of the message. Where previously receivers (managers) silence or inaction has been attributed to their ego being threatened, they found it was due to the type of voice an employee used. This combination of message delivery and context influencing receiver voice, may help, in part, explain reported poor receiver behavior. This evaluation of the interaction according to CAT, would directly influence the immediate response to the voiced concern and future behavior in similar interactions. To specifically help speaking up programs to sustainably shift from being skill focused, to speaking up being a shared accomplishment, the receiver's communication needs must be understood and considered. We, therefore, propose some alternate considerations to help make this fundamental shift. See Figure 2 for the summary.
Instead of just teaching the “skill” of speaking up or responding in a strictly defined manner, we instead view speaking up as a means to start the conversation, setting up an opportunity for open negotiation. Based on the results, speakers will need to negotiate both where the conversation occurs (context) as well as the concern itself. If the speaker previews their desire to raise a concern before initiating the mnemonic, this provides receivers with an opportunity to negotiate the message being delivered in the presence of others, or in a less public forum, to help enhance message reception and quality of response due to the raised level of acceptability of the interaction. Of course, should harm be imminent, a shared negotiation may not be feasible at the moment. Further study into receiver behavior in high stakes situations rather than more “grey” situations, needs to be undertaken. Receivers need to be accountable for poor communication behavior, but to be fair, most receivers have not been specifically trained on how to listen, process, and formulate a response and particularly, how to manage such dynamics as situational context and the impact of social identity. Programs need to train the receiver on the individual micro-skills that allow this framing, that is, management of self and awareness of personal influencing factors. Our findings show that the making of positive attributions can enhance the acceptability of the message, even when poorly delivered. Therefore, such a move should be included in speaking up programs, teaching receivers (and speakers) how to reframe uncharitable attributions into generous ones, using techniques such as the basic assumption, and engage through negotiation, in co-creating the conversational context (where the conversation occurs). By doing so, training can help receivers develop their “psychological immune system” (Eva et al., 2012, p. 23) to accommodatively stand up for what they believe, thereby reducing, defensive behaviors, such as remaining silent.
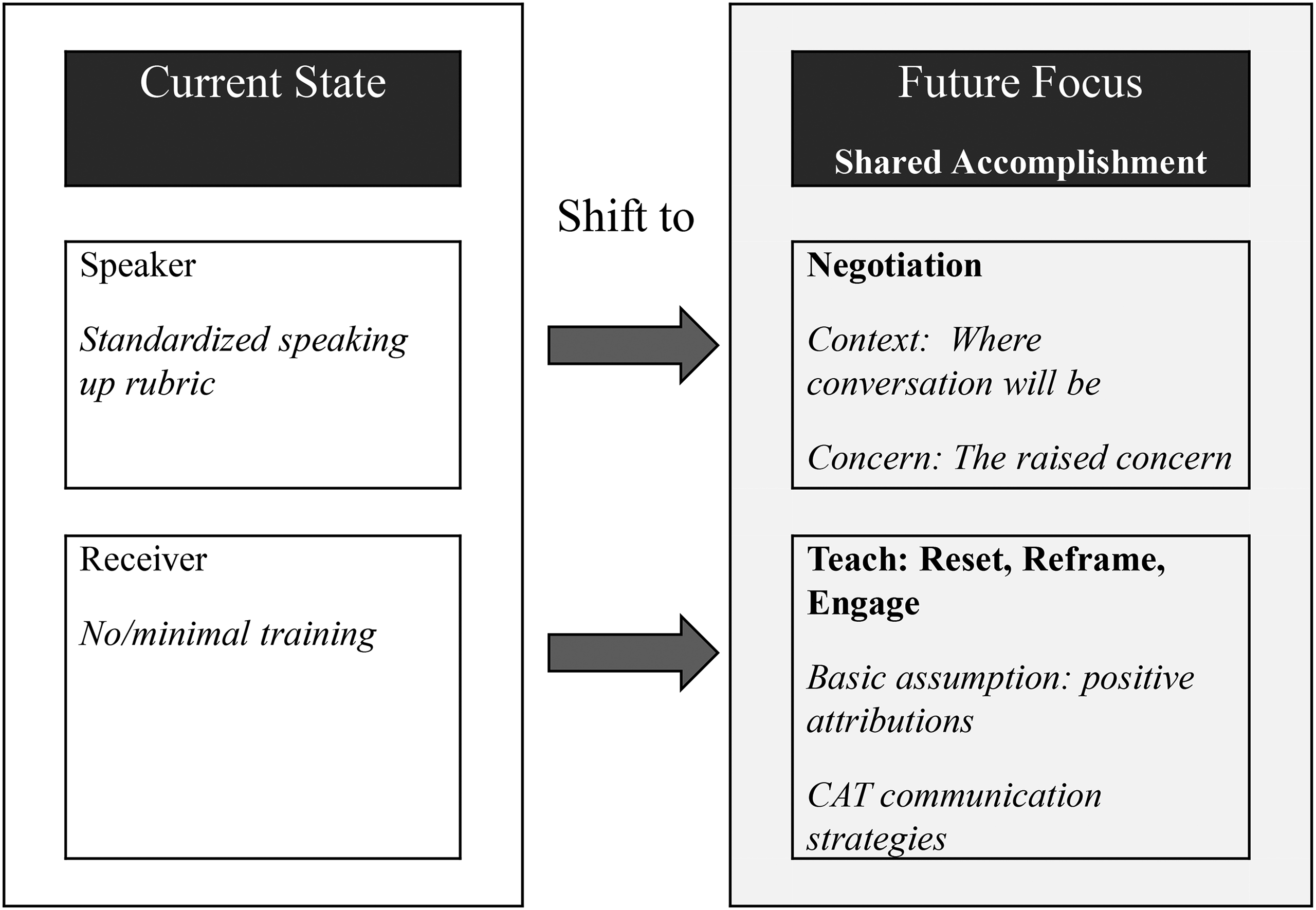
Future considerations for achieving shared accomplishment in speaking up conversations.
By framing speaking up as an open negotiation of both context and concern and equipping both the speaker and the receiver with accommodative communication strategies, speaking up shifts from a speaker-centric, skills-based conversation to a shared accomplishment. CAT can be used to inform, teach, and apply accommodative speaker and receiver communication strategies to achieve this. Further receiver-focused research is required to help best inform these future directions.
Limitations
Speaking up within the vignettes occurred within a defined context, however, transferability of findings is supported by the fact that the clinical scenarios were based on documented and frequently occurring situations within a large and diverse health organization. Paper-based vignettes were used to maximize recruitment of participants, aiming for minimal disruption to the forums in which data collection occurred. Future studies should aim to use video-based vignettes allowing for visualization of speaker behavior and gestures and a more comprehensive evaluation of paralinguistic elements. Additionally, we acknowledge that the vignettes were hypothetical situations and that what an individual espouses may be different from what they do in action. For this reason, we are undertaking additional studies that directly observe receiver behavior in action.
Gender of the speaker was not stated within the vignettes and not was a focus for analysis. It must be noted that some participants in their responses did however make assumptions about the speaker's gender based on their stated discipline within the vignettes. These assumptions on gender may have influenced their responses and should be explored in future receiver-focused research.
It is acknowledged that the authors are psychologists and nurses which may influence interpretation of the data. This was addressed through independent coding, consistent cross checking, and an acknowledgment of the authors professional history and experiences with speaking up (Barlow, 2021).
Conclusion
This study was novel because it is the first to apply CAT in a healthcare speaking-up context. The results suggest that there are a number of factors that influence the way in which receivers of health care speaking up messages evaluate the messages. Situational context, the attributions made, and how the speaking up message was evaluated, was influenced by the participant's salient social identity. Depending on discipline, receivers of the same message may respond quite differently. The application of CAT has demonstrated the impact the context, the attributions made, and the levels of perceived accommodation have on the receiver. In this context, the study highlights the importance of viewing the speaking up encounter as a collective accomplishment that relies on collaboration, not just the individual. This has practical implications for organizations designing and implementing speaking-up programs. Shifting the focus to be inclusive of the receiver as well as the sender of the speaking-up message is a critical first step to implementing and sustaining successful speaking-up programs.
Supplemental Material
Footnotes
Acknowledgments
Thank you to the clinicians who have been spoken up to and had the courage to listen.
Author Contribution
MB handled the conceptualization, data curation, formal analysis, investigation, methodology, project administration, and writing original draft. BW handled the conceptualization, data curation, formal analysis, methodology, supervision, and writing—review and editing. EJ handled the conceptualization, formal analysis, methodology, supervision, and writing—review and editing. KM handled the conceptualization, methodology, supervision, and writing—review and editing. FM handled the supervision and writing—review and editing. JR handled the writing, editing, and critical review.
Data Availability Statement
All data generated or analyzed during this study are included in this published article. Data is available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
The study obtained ethical approval from Mater Health Services Research Human Research and Ethics Committee HREC/18/MHS/78. All participants were over 18 years of age, were provided with a participant consent and information sheet, and informed consent was obtained from all participants. The research was conducted in accordance with NHMRC, Australian Code for the Responsible Conduct of Research (2007), and the declaration of Helsinki. Surveys were distributed to consented participant who identified themselves on the questionnaire using a unique identification number that they created. During data analysis, no individual could be individually identified.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Correction (August 2024):
Article updated with the addition of online supplemental material.
Appendix A: Vignette Examples.
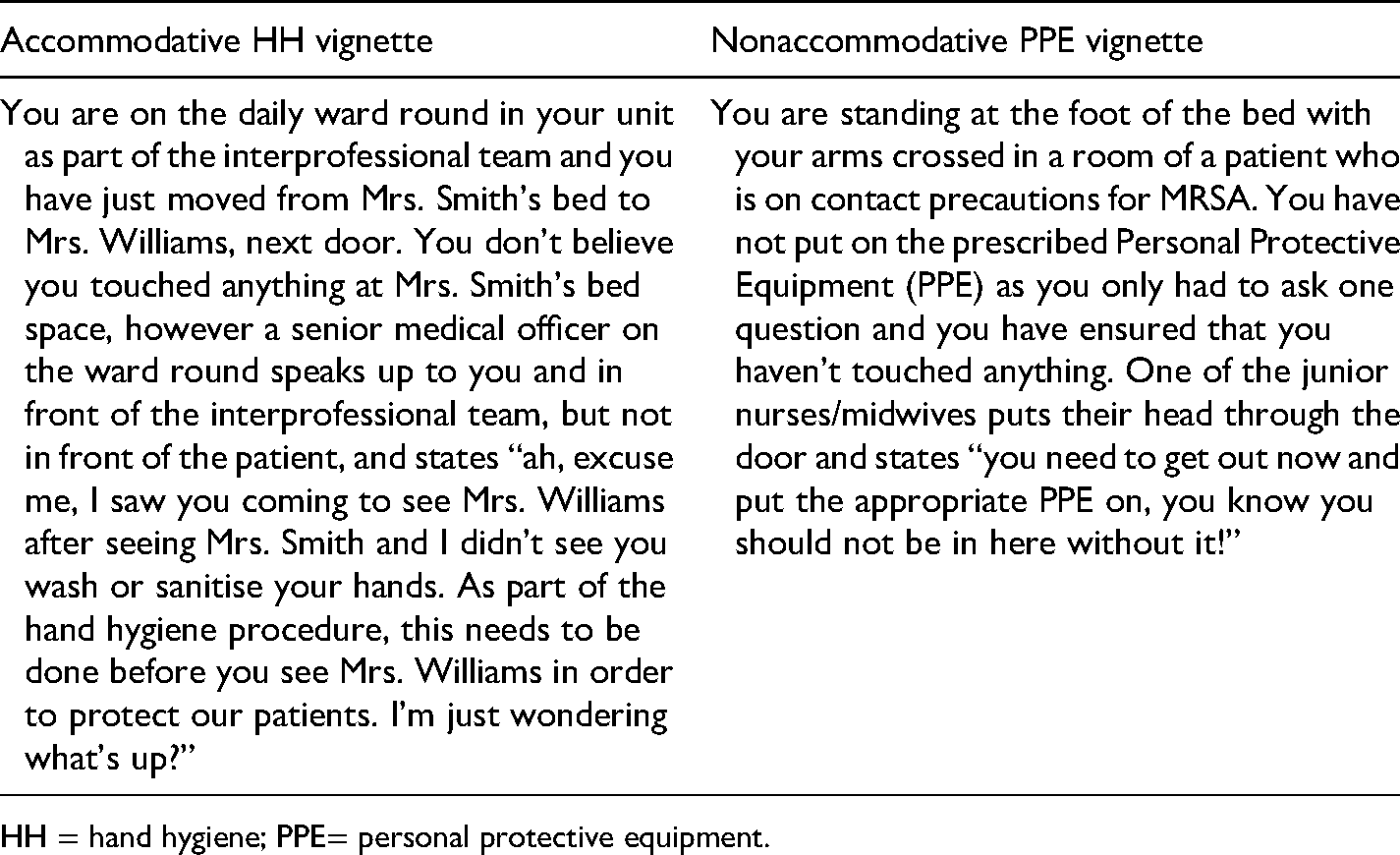
| Accommodative HH vignette | Nonaccommodative PPE vignette |
|---|---|
| You are on the daily ward round in your unit as part of the interprofessional team and you have just moved from Mrs. Smith's bed to Mrs. Williams, next door. You don’t believe you touched anything at Mrs. Smith's bed space, however a senior medical officer on the ward round speaks up to you and in front of the interprofessional team, but not in front of the patient, and states “ah, excuse me, I saw you coming to see Mrs. Williams after seeing Mrs. Smith and I didn’t see you wash or sanitise your hands. As part of the hand hygiene procedure, this needs to be done before you see Mrs. Williams in order to protect our patients. I’m just wondering what's up?” | You are standing at the foot of the bed with your arms crossed in a room of a patient who is on contact precautions for MRSA. You have not put on the prescribed Personal Protective Equipment (PPE) as you only had to ask one question and you have ensured that you haven’t touched anything. One of the junior nurses/midwives puts their head through the door and states “you need to get out now and put the appropriate PPE on, you know you should not be in here without it!” |
HH = hand hygiene; PPE= personal protective equipment.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.