
Abstract
Effective communication is crucial in all service contexts, but especially in clinical healthcare, given its high (sometimes life-or-death) stakes. Fine-tuned messaging and personalization are vital to improving patients’ service experiences, their understanding of and adherence to treatment and therapy, and their physical and mental health. This article aims to guide clinicians specifically, and other service providers more generally, in their communication practices, so that they ultimately improve the quality of service they deliver to patients each day. It presents a comprehensive, integrative review and develops a framework for how clinicians communicate with patients by synthesizing findings from presently disconnected literatures in services, psychology, marketing, communications, and medicine. The framework, which elucidates the communication channels (verbal, nonverbal, and listening) clinicians use to convey meaning to patients, can be adapted to other service contexts, especially professional services. An agenda for future research and implications for improving service provider communications are included.
Keywords
Communication is powerful: It gives meaning to our lives, shapes our interactions with others, and influences who we are and how we see the world. Derived from the Latin noun communicatio, which means “sharing” or “imparting” (Peters 2008), interpersonal communication is a process by which individuals share information, ideas, and knowledge (Trenholm Sarah, 2020). At its most fundamental level, communication involves a sender, a receiver, and the transmission of a message (Schramm, 1997; Trenholm Sarah, 2020). Indeed, the interactive model of communication describes communication as a two-way process wherein the sender and receiver generate meaning by sending messages and receiving feedback within physical and psychological contexts (Schramm 1997). In this way, communication is an active, dynamic, nonlinear process where shared meaning is created (Dance 1967) through verbal (words), nonverbal (body language), and listening channels (Trenholm Sarah, 2020).
In services, communication via these channels unfolds as the service provider and customer interact. The quality of this interaction is essential to value cocreation (Danaher Tracey et al., 2023; McColl-Kennedy et al., 2012; Sweeney et al., 2015) and successful service delivery (Brady and Cronin 2001; Dance 1967). Indeed, social interaction theory posits that communication shapes customers’ perceptions of their experience (Ben-Sira 1976; Webster and Sundaram 2009; Jain, Sethi and Mukherji 2009). The “way” service providers communicate—what they say, how they say it, and whether they listen—influences customers’ evaluations of the service experience, the individual provider, and the firm (Webster and Sundaram 2009). Yet, despite its importance, research on the role and elements that comprise verbal, nonverbal, and listening communication is fragmented.
Effective communication is particularly crucial in ongoing, high-contact, high-involvement, emotional service settings—such as healthcare, law, finance, and education—where customers often have less knowledge than the service provider and may be anxious about the service process or outcome because of the service’s complexity and importance. In healthcare, the focus of our research, communication between a clinician and patient is critical to building rapport and trust, sharing information, and making joint decisions (Dickinson et al. 2017). It is also the foundation upon which patient participation, activation, and value cocreation rest. Effective interpersonal communication is central to high-quality healthcare, ideally involving both clinician and patient as active participants.
While communication is relevant to all services, healthcare communication is especially challenging. Clinicians often must navigate patients’ anxiety, uncertainty, knowledge disadvantage, and expectations that may be unrealistic (Dickinson et al. 2017). And patients often must contend with the service’s complexity, technical language, information overload, and perceived knowledge and power imbalances while in a state of high anxiety ( Berry, Davis and Wilmet 2015).However, good clinician-patient communication can solve problems, poor communication can cause them—for example, patients may not understand their treatment plan, or they may feel they are not being heard; ineffective communication in healthcare can have severe, sometimes life-threatening consequences.
Research on verbal, nonverbal, and listening communication channels is rich and varied. In the service and marketing domains, prior work has focused on: (1) how interpersonal communication affects customer satisfaction during service recovery (e.g., Vaerenbergy et al., 2012), (2) supervisor communication practices and service employee job outcomes (e.g., Webster and Sundaram 2009; Roongruangsee et al., 2022), (3) team communication patterns, inefficiencies, and challenges (e.g., Hedman and Valo 2015; Griffin and Hauser 1992), and (4) outcomes such as repurchase intentions and word-of-mouth (e.g., Berger 2014). In the psychology and medicine domains, studies have tended to focus on: (1) the effect of medical team communication (e.g., different departments and professionals; Pruitt and Liebelt 2010) or (2) clinician communication style (e.g., authoritative, detached, affiliative) on patient satisfaction (Hall et al., 1981; Street and Wimann 1987). However, the integration of communication channel elements and processes has not been a focus in these literatures.
While there is no doubt that patients actively cocreate service experiences via their own communications and actions (Danaher Tracey et al., 2023; McColl-Kennedy et al., 2012; Sweeney et al., 2015), in this paper, we focus on clinicians as communicators—rather than on the dyadic interplay between clinicians and patients—for several reasons. First, as communication is complex and comprises multiple components, an in-depth review of these elements from both the clinician and patient perspective was not possible in one study. Second, although optimal communication involves active patient participation, patients may be too ill, or lack the self-confidence, skills, or capabilities to effectively communicate with their healthcare providers (Berry et al., 2017; Chichirez Cristina & Purcărea, 2018). Under these circumstances, clinicians must do their best to dechipher patients’ needs and preferences and will be better equipped to do so if they themselves have a deep understanding of verbal, nonverbal, and listening communication. Third, insights on clinician communication are actionable and can be incorporated into training in medical school, residency programs, and in practice. Studying clinician communication is a critical first step in better understanding communication dynamics in healthcare.
The focus of our review is on in-person, face-to-face interactions between a clinician and a patient. The COVID-19 pandemic greatly accelerated the use of telehealth (clinicians consulting with patients remotely), and it offers an important channel for medical assistance. However, telehealth’s usage plunged in the U.S. and other countries following the first surge of COVID-19 cases in 2020 due to regulatory, payment, and patient acceptance barriers (Pearl and Wayling 2022). This dropoff, coupled with patients commonly needing in-person care (e.g., physical examinations and surgeries), indicate the limitations of telehealth. Telehealth is most appropriate for lower-complexity and less emotionally intense interactions (Offodile et al. 2022). While the majority of articles in our integrative review focus on face-to-face communication, our findings are relevant to technology-mediated interactions to the degree that communication is adapted to fit the unique characteristics of a virtual experience.
A comprehensive distillation of effective interpersonal communication in service delivery is needed. The current research undertakes this distillation in the domain of healthcare, focusing on clinician communication. We draw on pertinent work in services, marketing, management, psychology, medicine, and other literatures to examine the elements that comprise verbal, nonverbal, and listening communication channels. We also highlight how, when, and why each channel impacts patients. Our overarching goal is to offer an integrative review that synthesizes existing research (Elsbach and van Knippenberg, 2020) and offers a new framework (Figure 2) for conceptualizing clinician communication. In developing this framework, we: (1) identify how clinicians convey meaning to patients through verbal, nonverbal, and listening communication channels, (2) offer an understanding of how, why, and when clinician communication influences patients, (3) present a research agenda to guide future work, and (4) offer practical suggestions for improving communication in healthcare and other services.
Methodology
Applying Elsbach and van Knippenberg’s (2020) typology of integrative reviews, our work falls within the category of a broad review of topics in need of initial synthesis. As such, our aim was to develop an integrative framework of clinician communication by selecting and synthesizing relevant research across disciplines (Elsbach and van Knippenberg, 2020; Snyder, 2019; Jaakkola, 2020). Thus, we pursued a process that ensured sufficient initial coverage of the literature but allowed for flexibility in identifying relevant articles and perspectives.
We began by searching Scopus. We used the terms verbal communication, nonverbal communication, and listening to identify the most common elements in each of these channels (e.g., jargon, kinesics). We updated and added terms as needed. For example, we were aware that kinesics (body language) was a central component of nonverbal communication; however, proxemics (space, distance) emerged as we searched. Next, we conducted two sets of specific searches. First, we searched in titles, abstracts, and keywords for each channel and element. For verbal communication, we searched for metaphor, jargon, and label/labeling; for nonverbal communication, we searched for kinesics [body language, eye contact], haptics [touch], vocalics [tone of voice], and proxemics [personal space, territoriality]); and we searched for listening. We included communication (communicate, language) as a search term (in titles, abstracts, and keywords) and excluded other terms as needed (e.g., off-label drugs, eco-labels) to ensure that we did not retrieve irrelevant articles. For the first set of searches, we restricted the results to the most relevant disciplines outside of healthcare (services, management, psychology). Second, we conducted each search again, with the addition of terms (in titles, abstracts, and keywords) related to health (health, healthcare, medicine) and to the communicators in our context (physician, clinician, doctor, patient, provider, nurse). We restricted our searches to journal articles published in English but did not restrict by year (Elsbach and van Knippenberg, 2020).
This initial process yielded nearly 10,000 articles. We combined our searches by element (e.g., jargon), removed duplicates, and sorted the results by relevance. The number of retrieved articles varied widely by element; for example, we gathered ∼200 articles on proxemics, but ∼2500 on metaphors. For smaller searches, we screened the full article list. For larger searches, we screened the top 10%–15% of the list. To screen articles, we examined titles, keywords, and abstracts, using topic relevance as our primary criterion for inclusion. After screening, we added articles based on prior knowledge and by snowballing (generating leads) from reference lists. We also confirmed that seminal articles in specific disciplines (e.g., Lakoff and Johnson 1980, on metaphors), as well as review articles, were included.
We then moved on to critical analysis and synthesis. Each article was read and processed by one or more authors, with many articles informing our thinking. Given our goal of developing an integrative framework, along with space constraints, we could not cite every article. Instead, on the basis of our reading and synthesis, we selected representative articles across disciplines to include. This overall process yielded a final set of 168 articles cited in the current paper with approximately 110 focusing specifically on verbal, nonverbal, and listening communication. During this process, we allowed insights to “arise from the review” (Elsbach and van Knippenberg, 2020). To facilitate this approach, we noted each article’s predictor variable (usually the clinician’s verbal, nonverbal, or listening activity), mediating or intervening processes, moderating variables, and outcome variables. From this article-level analysis, we categorized and organized variables into broader constructs and an overall framework.
In the remainder of this article, we synthesize the literature we reviewed and outline how, when, and why the elements within each clinician communication channel—verbal, nonverbal, and listening—influence patients. We then present an integrated framework of clinician communication and offer insights for future research and for improving communication.
How Clinicians Communicate
Although our literature search revealed considerable research on communication, we saw no framework integrating verbal, nonverbal, and listening channels to elucidate how clinicians (and other service providers) communicate. We address this gap by synthesizing disparate literatures. Within each communication channel, we review the specific elements prominently identified in our literature search (Figure 1): verbal (metaphors, labels, and jargon), nonverbal (kinesics, haptics, proxemics, and vocalics), and listening. Clinician communication channels: Verbal, nonverbal, and listening.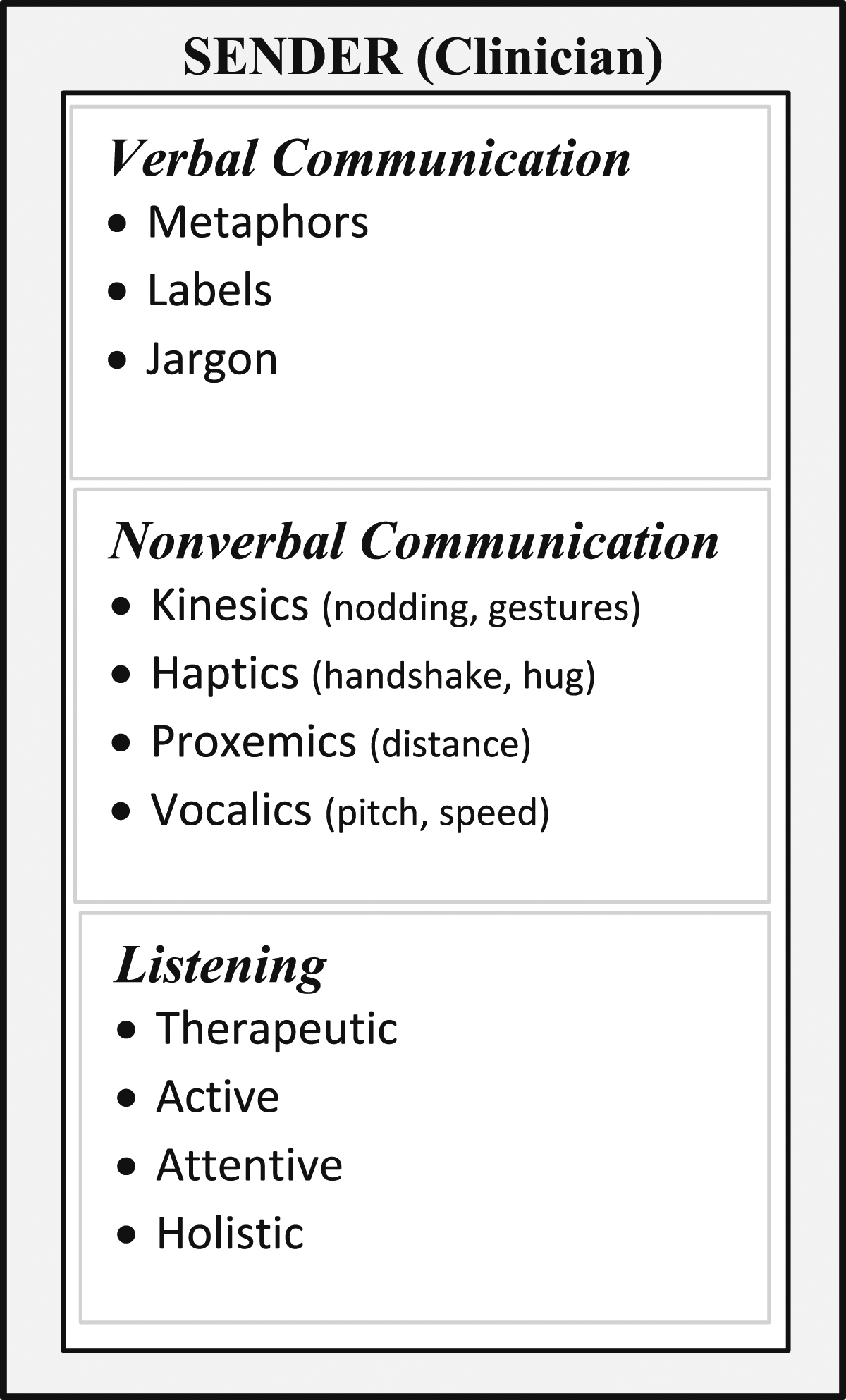
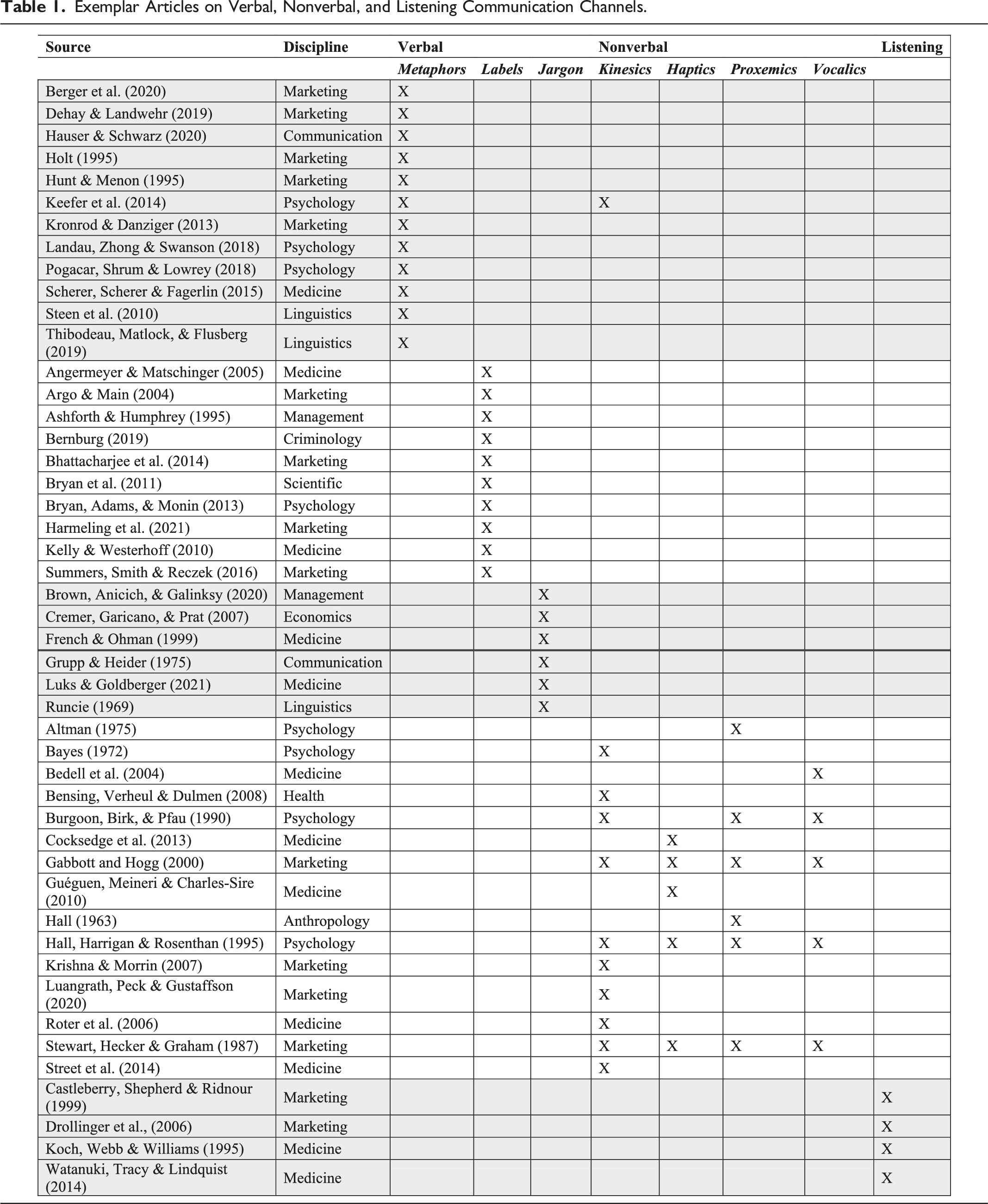
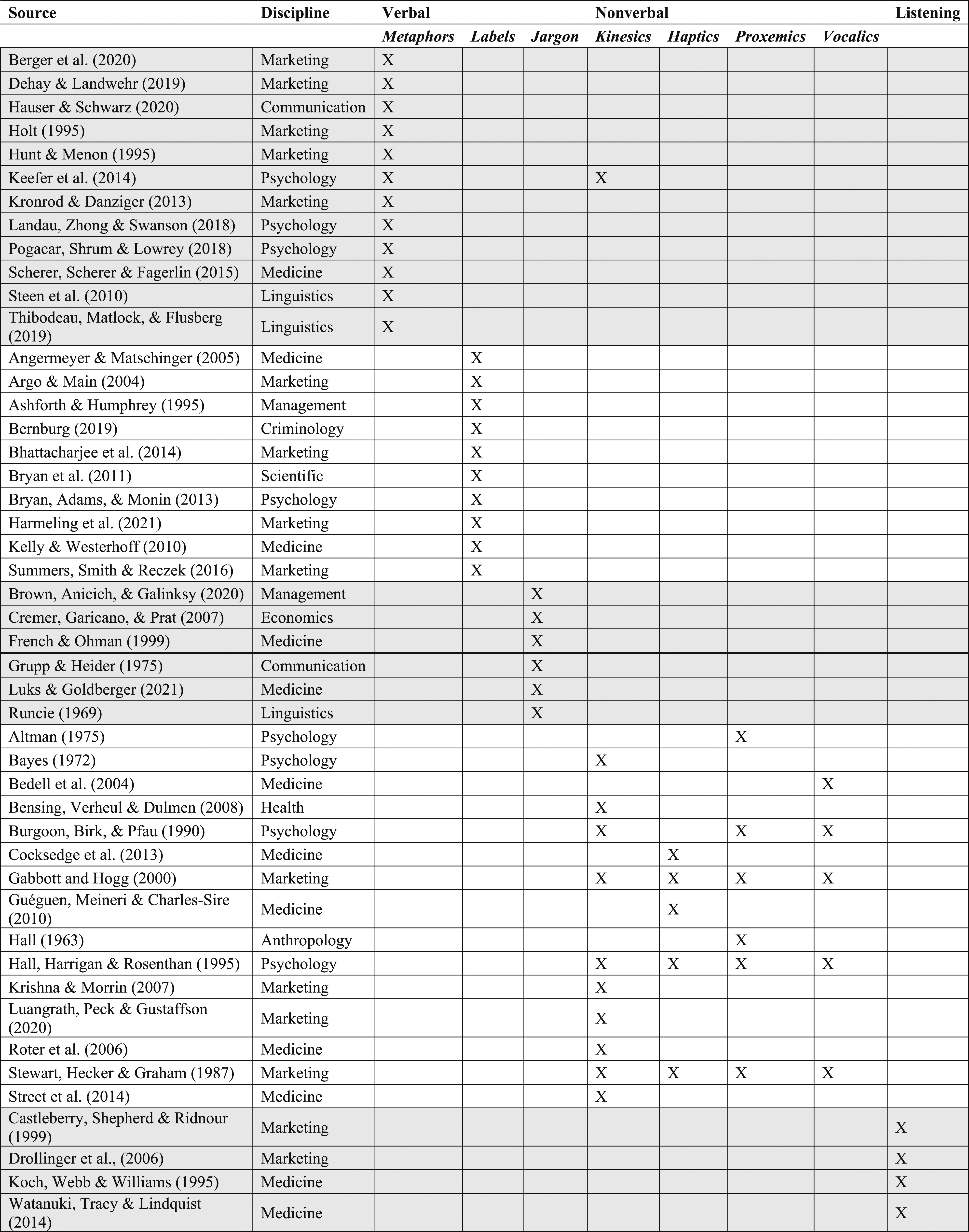
Exemplar Articles on Verbal, Nonverbal, and Listening Communication Channels.
Verbal Communication: The Power of Words
The power of words to convey meaning, and thereby to shape and describe reality, is recognized across disciplines (Bedell et al. 2004; Berry et al. 2020; Dickinson et al. 2017; Pogacar, Shrum, and Lowrey 2018). Words matter because language directly influences receivers’ attitudes and behaviors (Berger et al. 2020). We focus on three verbal elements that emerged from our review and that are highly relevant to healthcare and other services: metaphors, labels, and jargon.
Metaphors
Metaphors are “cognitive tools for understanding…one concept in terms of a superficially dissimilar concept” (Landau, Zhong, and Swanson 2018, p. 55; see also Lakoff and Johnson 1980; Thibodeau, Matlock, and Flusberg 2019). Metaphorical words and phrases convey meaning and shape understanding by helping receivers “map” information about a concrete source concept (e.g., war) onto an abstract target concept (e.g., cancer). They can also be derived from physical experiences (e.g., depression is heavy) or cultural knowledge (e.g., addiction is a journey; Thibodeau, Matlock, and Flusberg 2019).
Metaphors constitute 8%–18% of all discourse (Steen et al. 2010) and are frequently used in business (e.g., Red Bull’s “gives you wings” slogan; Hunt and Menon 1995) and healthcare (e.g., heart disease is a “time bomb in your chest”; Bedell et al. 2004; Casarett et al. 2010). Metaphors influence receivers through various processes: they can activate specific concepts (Boulenger, Shtyrov, and Pulvermüller 2012) and alter attention (Meier and Robinson 2006), memory (Crawford 2014), and perceptions of senders (Casarett et al. 2010). In doing so, metaphors impact receivers’ attitudes (Sopory and Dillard 2002) and choices (Kronrod and Danziger 2013). For example, describing the flu metaphorically (e.g., as a beast), rather than literally (e.g., as a virus), increases vaccination intentions (Scherer, Scherer, and Fagerlin 2015).
The psychological and behavioral outcomes of metaphor use depend on moderating factors. First, a metaphor’s impact depends on receivers’ attitudes and feelings toward, involvement with, and knowledge about its underlying meaning (Landau et al. 2018). Sports enthusiasts, for instance, are more likely to be persuaded by sports metaphors (Ottati, Rhoads, and Graesser 1999). Second, metaphors are more persuasive when senders use them to frame a discussion early on and then repeat them (Sopory and Dillard 2002; Thibodeau, Matlock, and Flusberg 2019). Third, metaphors have more influence when they fit the context in question (Hauser and Schwarz 2020), and when senders use them to frame both problems and solutions (Keefer Lucas et al., 2014).
Metaphors appropriately used by physicians can benefit patients (Scherer et al. 2015). However, mounting evidence points to their overuse, insensitive use, and potential harms (Farrell 2020; Marron et al. 2020). For example, war metaphors commonly used in oncology include “front-line” therapy to “attack” cancer cells that “invade” healthy tissue (Marron et al. 2020). War metaphors can appeal to some patients, but many perceive treatment to be more difficult when their care team uses the language of war (Hendricks et al. 2018). The common use of war metaphors in oncology can be especially inappropriate given that cancer has powerful physical and emotional effects. For example, suggesting cancer is a war implies a patient may die from cancer because they didn’t fight hard enough (Marron et al. 2020).
Physicians typically use metaphors to help patients understand their illness and motivate them to improve their health (Bedell et al. 2004). However, they may also use metaphors habitually, given how embedded some expressions are within medical specialties. Metaphors also may be seen by physicians as time-savers to replace more detailed explanations. For example, in describing asthma, one doctor characterizes the airways as “different-sized drainpipes that can get clogged up and need to be unclogged” (Arroliga et al. 2002, p. E-377). However, poorly worded metaphors can scare patients (e.g., “a time bomb in your chest”; Bedell et al. 2004, p.1365) and obscure understanding (e.g., “diabetes coats red blood cells with sugar until they are little glazed donuts”; Khullar 2014).
Sensitive, well-considered use of metaphors that fit the clinical context—and reflect moderating factors such as individual patients’ experiences, knowledge, and personality—can simplify complex clinical concepts, thereby accelerating understanding (Arroliga et al. 2002). Metaphor use can also improve patients’ ratings of physicians’ communication skills (Casarett et al. 2010). Metaphors can thus be used to accomplish a specific, beneficial purpose that suits the patient and clinical context, such as providing reassurance or enhancing comprehension.
Labels
Labels—a “classifying phrase or name applied to a person or thing” (Oxford English Dictionary 2020)—are ubiquitous in business (e.g., “big spender”) and healthcare (e.g., “difficult patient”). Improving healthcare service through more effective communication includes attention to the relationships among labels, self-identity, social stigma, and behavior.
Labels influence individuals’ behavior in large part through the process of activating their identities. When labels prompt thoughts related to a valued self-identity, they can trigger people to maintain their self-concept by behaving consistently with the label, as when a self-identified “voter” actually votes (Bryan et al. 2011; Bryan, Master, and Walton 2014). Conversely, an undesirable identity label, such as “cheater,” can discourage the related behavior (Bryan, Adams, and Monin 2013). When labels are compatible with prior behavior, individuals adjust their self-perceptions and subsequent behavior accordingly (Summers, Smith, and Reczek 2016). However, if identity-referencing labels are too overt, they can backfire by diminishing individuals’ perceptions of agency (Bhattacharjee, Berger, and Menon 2014).
This psychological process becomes more complicated when labels carry social stigma. Then, labels can influence the formation of ingroups and outgroups and alter interactions between the persons being labeled and those around them (Angermeyer & Matschinger, 2005; Ashforth Blake & Humphrey Ronald, 1995). If the stigma is strong enough that people associated with a label become marginalized, the label can create a self-fulfilling prophecy of persisting in an undesirable behavior (Bernburg 2019). For example, individuals with potentially stigmatizing characteristics (e.g., high body weight) may anticipate stigma for their eating habits, depending on the cues (e.g., slim, muscled people) used in advertising. As a result, beneficial choices (e.g., enrolling in a health workshop) may decline and detrimental choices may increase (Harmeling et al. 2021). This effect may be especially pernicious because of a persistent association between labels and stigma (Link and Phelan 2013) and their related influence on identity and behavior.
The influence of labels extends to personal and social outcomes. For example, labels can affect individual-level variables such as attention, memory, comprehension, and emotion regulation (Argo and Main 2004; Torre and Lieberman 2018), and group-level variables such as helping others (Bryan et al. 2014). Labels also can influence adherence to public health and safety initiatives (Argo and Main 2004) that simultaneously affect individuals and society.
Labels often used by clinicians about patients, such as “substance abuser” or “end-stage,” imply blame, and can increase patients’ psychological distress, diminish trust in clinicians, and undermine willingness to seek medical care (Berry et al. 2021; Hamer et al. 2010). Labeling can even cloud clinicians’ attitudes and treatment recommendations (Goddu et al. 2018; Kelly and Westerhoff 2010). One clinician’s stigmatizing label for a patient, expressed to another clinician, can negatively affect the quality of care from the receiving clinician working with the same patient (Dickinson et al., 2017; Peters, 2008). The term “cancer survivor” is often used in oncology but not for other diseases (e.g., “heart disease survivor”) and has been shown to displease—and even offend—many patients with cancer (e.g., Berry et al. 2019).
While much about illness is uncontrollable, the language of healthcare is controllable. Labels can be imprecise, and imprecision has a cost. Labels often transfer blame to patients, implying fault for getting sick. Although a patient’s lifestyle may have contributed to a certain disease, why use a potentially distressing, identity-diminishing term that can undermine clinician-patient trust (Berry et al. 2021). Language that empowers listeners, that motivates them, is important in service in general—and in healthcare.
Jargon
Jargon refers to “special words or expressions that are used by a particular profession or group of people and are difficult for others to understand” (Oxford English Dictionary 2020). Jargon is learned socially, often by modeling the speech of an ingroup member one seeks to emulate, such as when a medical intern or resident adopts the verbal shorthand of a senior physician (Luks and Goldberger 2021). Illustrative examples of jargon in business and healthcare include: (i) abbreviations, or shortened expressions substituting for the formal word or phrase, such as when marketing specialists talk about their “comms” strategy instead of communications strategy, or doctors say “pre-op” instead of preoperative, (ii) acronyms, which often overlap with abbreviations, are derived from the letters or syllables of formal words or phrases, such as when executives talk about maximizing “CLV” instead of customer lifetime value, or when doctors speak of a patient’s “CBC” instead of complete blood-cell count, and (iii) neologisms, which are newly coined words or old words used in a new way, such as when marketers speak of “brandstorming” (brainstorming new ideas for a brand) and physicians refer to “satting” (oxygen saturation) (Luks and Goldberger 2021).
Jargon is not strictly necessary; it is used instead of language that could be more easily understood (Brown, Anicich, and Galinksy 2020). Nevertheless, it is so prevalent in healthcare that its dictionary definition includes “medical jargon” (Oxford English Dictionary 2020). One reason jargon impedes healthcare communication is that clinicians often do not explain it. In one study, 81% of doctor-patient interactions included at least one piece of unclarified jargon (Castro et al. 2007). Deuster et al. (2008) found that when medical residents discussed cancer screening with patients, they used roughly 20 unique jargon words, explaining only five of them.
Senders may use jargon for many reasons: It can signal expertise and convey specialized knowledge (Grupp and Heider 1975); it can help individuals demonstrate ingroup membership (Chao et al. 1994; Runcie 1969); and certain types of jargon, such as abbreviations and acronyms, can make ingroup communication more efficient (Cremer, Garicano, and Prat 2007). High-status group members, such as attending physicians, may use jargon to test the knowledge of lower-status members, such as medical residents (Luks and Goldberger 2021). Jargon can even serve as “conspicuous communication,” whereby lower-status group members use it to impress higher-status members (Brown et al. 2020).
Although jargon can have legitimate uses, it often impedes patients’ understanding (Grupp and Heider 1975) by making information more difficult to cognitively process, thereby increasing the risk of adverse outcomes (Bullock et al. 2019). Clinicians’ use of jargon is especially problematic for patients with low health literacy (Castro et al. 2007). When jargon conveys a different meaning for experts and nonexperts, it also can cause offense. For example, the commonly used acronym “SOB” in medical records (referring to “shortness of breath”; French and Ohman 1999) may well upset a patient who reads it.
Nonverbal Communication: Communicating Without Words
Nonverbal cues—eye contact, gaze, facial expression, gestures, body position, and posture—are influential in all human communication, and some studies show these cues to be more influential than words (Sundaram and Webster 2000; Burgoon 1991; Preston 2005). Nonverbal communication is crucial in relating to other people, building trust and intimacy, and expressing emotion (Gabbott and Hogg 2000). For example, a doctor who cries along with parents upon sharing their child’s terminal diagnosis conveys deep sorrow, empathy, and understanding of the enormity of the moment; no words have the same power.
Nonverbal elements of an interpersonal exchange can influence perceptions of credibility and trust (Burgoon, Birk, and Pfau 1990), persuasive power (Mehrabian and Williams 1969; Stewart, Hecker, and Graham 1987), courtesy (Ford 1995), and interpersonal warmth (Bayes 1972). In medical settings, nonverbal communication can affect outcomes such as patient satisfaction and anxiety, adherence to treatment, health service utilization, and appointment-keeping (Roter et al. 2006; Bensing, Verheul, and Dulmen 2008). However, nonverbal communication is also ambiguous and easy to misinterpret (Jones 2013), making it crucial for the sender to surmise how the receiver will perceive nonverbal cues. For example, if a physician does not make appropriate eye contact, the patient may perceive a lack of interest or concern (Robinson 2006)—or discomfort in being frank. Interpretation of nonverbal cues is complex and is moderated by the situation, topic of conversation, previous events and behaviors, accompanying words, other nonverbal cues, cultural meaning, and personal attributes such as gender, age, and physical appearance (Bavelas and Chovil 1997).
Compared with verbal exchanges, nonverbal communication is generally perceived to be less controllable or manipulable and therefore more credible and reliable (Gabbott and Hogg 2000). Nonverbal communication reveals genuine intentions, exposing the sender’s underlying thoughts and feelings. As a result, nonverbal communication can carry more weight than words (Gabbott and Hogg 2000), especially in times of stress, when people rely more on intuition (Andersen 1999). In addition, when a sender’s verbal and nonverbal messages conflict, a receiver is likely to rely heavily on nonverbal cues to uncover the true meaning (Hargie 2016).
Despite nonverbal communication’s enormous importance in service settings, pertinent research and practice guidelines remain thin. For instance, the American Society of Clinical Oncology published detailed patient-clinician communication guidelines (see Gilligan, Bohlke, and Baile 2018 for a summary) that offer no guidance on nonverbal communication, despite its salience in a service as emotionally intense as oncology (Berry, Davis, and Wilmet 2015). Nevertheless, what is known about nonverbal communication—kinesics, haptics, proxemics, and vocalics—can clarify the processes by which these elements influence patients’ psychological and behavioral outcomes.
Kinesics
From the root word kinesis, which means “movement,” kinesics is colloquially known as “body language”: facial expression, gestures, posture and gait, and other visible body movements (Hans and Hans 2015; Preston 2005). Kinesics matter, as evident in concepts such as “social servicescape” and “emotional contagion,” whereby the displayed emotions of senders (expressions, postures, and movements) influence receivers’ emotions and behavior (Barsade 2002; Holt 1995; Pugh 2001).
Eye contact, handshakes, nodding, smiling, and body orientation are powerful kinesic signals that convey meaning (Sundaram and Webster 2000; Preston 2005). These signals can occur in isolation but most commonly occur simultaneously. For example, the combination of smiling, leaning forward, and making steady eye contact signals intimacy, friendliness, and courtesy (Sundaram and Webster 2000). In contrast, a stoic facial expression, frowning, avoiding eye contact, and leaning backward imply dominance, emotional distance, and unfriendliness (Burgoon et al. 1990; Mehrabian and Williams 1969).
Kinesic gestures often accompany specific linguistic content (Ekman 1976). Used in speech to convey information more efficiently or to express attitudes or emotions, these gestures have five distinct functional types (Andersen 1999; Ekman 1976): emblems are agreed-upon gestures that substitute for words and phrases (e.g., thumbs-up sign); illustrators accompany or reinforce the verbal message (e.g., hands held apart to show size); regulators control or maintain the pace and flow of conversation (e.g., leaning forward to show attentiveness); affective displays convey emotions through facial and bodily expressions (e.g., smiling, eye contact); and adaptors fulfill psychological needs (e.g., clicking a pen when nervous).
In healthcare, eye contact is one of the most salient kinesic movements. Consistent eye contact between clinician and patient is associated with greater patient understanding, disclosure, and satisfaction (Bensing, Kerssens, and van der Pasch 1995). Appropriate eye contact also bolsters perceptions of a clinician’s honesty (Henry et al. 2011) and trustworthiness (Hillen et al. 2015)—and enhances patients’ attentiveness and involvement (Street et al. 2014). Indeed, physicians who focus on electronic patient records during medical consultations are perceived as less emotionally responsive than those who look at the patient (Duke, Frankel, and Reis 2013).
Haptics
Haptics refer to communication by touch. Touch has the power to comfort people in moments of sorrow when words alone cannot (Andersen 1999). It conveys meaning and can be welcoming, persuasive, or threatening, depending on the context (Andersen 1999; Hans and Hans 2015). In medicine, a request accompanied by touch increases treatment adherence, including taking prescribed medicines (Guéguen, Meineri, and Charles-Sire 2010).
Researchers have identified several types of touch: functional-professional, social-polite, friendship-warmth, love-intimacy, and sexual-arousal (Hans and Hans 2015). Most relevant to medical care are functional-professional touch, related to a goal or routine professional interaction (such as a physical exam), when appropriate touch is expected and unthreatening; and social-polite touch, such as a handshake or a pat on the shoulder, to initiate interactions or show inclusion and respect (Cocksedge et al., 2013). Friendship-warmth touch, such as a hug, also can be appropriate and welcomed, as when a clinician provides care for an extended period of time and becomes close to patients and their family members (Hans and Hans 2015).
In medical settings, functional-professional and social-polite (and sometimes friendship-warmth) touch can facilitate the healing process and convey care and compassion (Singh and Leder 2012). Touch can signal safety, comfort, and trust (Keltner 2010) and has been shown to calm cardiovascular stress by activating the body’s vagus nerve (Keltner 2010) and releasing the positive effects of the hormone oxytocin (Keltner 2010). Patients generally perceive warm touch as conveying acceptance, and clinicians can use it to enhance patient self-esteem (Connor and Howett 2009). In people with Alzheimer’s disease, touch has been shown to improve relaxation, help patients connect emotionally with others, and reduce depression (Keltner 2010).
Proxemics
How people communicate through use of space (Sundaram and Webster 2000) and then adjust their behavior accordingly is known as proxemics. For example, in crowded settings, when personal space is breached unexpectedly, a person might react negatively (Hans and Hans 2015). This is called “territoriality,” a self-other boundary-regulation mechanism during social interactions (Altman 1975) and deters or prevents unwanted infringements on one’s perceived territory, including workspaces and one’s body (Brown 2009).
Personal space is influenced heavily by culture. In the U.S., Hall (1963) identified four interpersonal proximal zones: intimate, personal, social, and public. Intimate space, the area immediately surrounding our bodies (0 to 1.5 feet) is reserved for parents, children, lovers, spouses, and partners. Although breaching this space can bring comfort, especially when words fail (Hans and Hans 2015), it can be counterproductive if patients perceive a lack of control over their own body (Marin, Gasparino, Puggina 2018). It may also be annoying or frightening in some circumstances (Hall 1963; Hans and Hans 2015). The personal zone (1.5 to 4 feet) is the distance at which people interact with family members, good friends, and significant others (Andersen and Sull 1985; Andersen, Gannon, and Kalchik 2013). The majority of communication occurs in the personal zone; at this distance, people can touch another person to facilitate conversation, self-disclosure, and feelings of closeness. The social zone (4 to 12 feet), for friends and coworkers, is typically casual or professional but not intimate or public, still permitting a connection between sender and receiver. The public zone (12 to 25 feet) is for strangers and officials; the least personal zone, it is typically used in formal speech and when the sender wants to feel or seem removed from the receiver (Hans and Hans 2015).
In a study of proxemics in nursing, Moreira et al. (2017) found that the physical distance maintained between a nurse and patient influenced the level and type of communication they had. The researchers noted that the patient’s intimate zone was entered frequently to perform medical procedures and interventions, whereas the personal zone was reserved primarily for conversations and preparation for procedures. At this distance, nurses could detect facial expressions and decode other nonverbal cues, while still being close enough to touch the patient for comfort or reassurance, and to engage in dialogue to build rapport. The social distance was used for observation of patients’ expressions and nonverbal behavior: Nurses were able to identify and attend to patients if they became unwell, uncomfortable, or anxious. At the public distance, interactions tended to be procedural and related to reception, recording of information in medical records, or preparation of medications.
Vocalics
Vocalics are the “paralanguage” that accompanies verbal messages, such as pitch, volume, rate, vocal quality, and verbal fillers (McNeill 2005; Andersen 1999). Vocalics capture how people speak, rather than what they say. These cues can reinforce, complement, or modify verbal and nonverbal meaning—and are useful in emphasizing particular parts of a message (Andersen 1999). Vocalics are especially important when communication has no visual component, as in phone-based telehealth encounters. In these settings, “voice” is the listener’s only cue for decoding emotion and eliciting additional information such as credibility and trustworthiness (Krauss, Freyberg, and Morsella 2002).
Vocalics provide useful context for the verbal content of speech. Pitch helps to convey meaning, regulate conversational flow, and signal the intensity of a message, whereas volume is generally adjusted to the setting and to the distance and relationships among the people (Andersen 1999). Variations in pitch and volume can influence a speaker’s persuasiveness by altering perceptions of their credibility and competence (Van Zant and Berger 2020; Wang et al. 2021). Similarly, speech rate (fast or slow) influences how others perceive the speaker’s emotional state, credibility, and intelligence (Guyer, Fabrigar, and Vaughn-Johnston 2018). Speech rate can also impede others’ ability to receive and understand verbal messages. A fast speaker may be difficult to follow, but fast speech combined with a pleasant tone of voice can aid in gaining adherence and in persuasion (Buller and Burgoon 1986).
Tone of voice can be controlled somewhat with pitch, volume, and emphasis (Robinson 2006), but each voice has a distinct quality or vocal signature. For example, a pleasing voice typically has a signature characterized by vocal variety and lower pitch (Andersen 1999). Vocal expressiveness and sensitivity to tone convey the subtle elements of emotional communication (Rosenthal et al. 2008). Research in medical settings has identified tone of voice as an important nonverbal cue (Hall, Harrigan, and Rosenthal 1995) that is related to patient satisfaction with clinicians’ care (DiMatteo et al. 1980). Warmer, positive tones—associated with better patient-clinician relations (Haskard et al. 2008)—are more caring, friendly, and intimate. When clinicians use warm tones, their patients follow suit; the more negative a clinician’s tone, the less positivity, involvement, and confidence is evident in the patient’s tone (Haskard et al. 2008).
Listening
Listening—essential to effective communication (Drollinger et al., 2006)—is an active, dynamic process that demands intentional effort so that verbal and nonverbal cues are not misunderstood (Watanuki, Tracy, and Lindquist 2014). Listening is distinct from the physiological process of hearing (Wrench 2014). Hearing is an automatic brain response that requires minimal effort; listening is purposeful, active, and directed at understanding meaning (Wrench 2014). Listening requires paying attention not only to what is being told (the story), but also to the nuanced use of language, voice, and body. People also signal their listening behaviorally (Bodie 2012), through nodding or eye contact (Castleberry, Shepherd, and Ridnour 1999), and verbally, by requesting more information or restating what has been said (Castleberry, Shepherd, and Ridnour 1999).
Given listening’s powerful influence in connecting with others (Adler 1997), it is critical to improving service quality and patients’ overall care experiences (Balik and Dopkiss 2010). When people believe they are being listened to, they feel valued and cared for—strengthening relationships and feelings of trust, connection, and intimacy (Koch, Webb, and Williams 1995).
Especially important in healthcare is therapeutic listening, which aims to acknowledge patients’ feelings and experiences—and to encourage them to continue communicating—thereby bolstering the clinician-patient connection (Watanuki, Tracy and Lindquist 2014). Therapeutic listening is particularly effective during difficult, often complex medical conversations, including serious illness diagnosis and treatment planning. Patients who feel understood as a result of therapeutic listening are likely to be more open and responsive to a clinician’s advice and adhere to treatment and care plans (Tayal, Michelson, and Tayal 2018).
Therapeutic listening requires listeners to be “present” and use all of their senses to analyze, infer, and evaluate the stated and underlying meanings of a message (Watanuki, Tracy and Lindquist 2014). Listening in a therapeutic context involves being nonjudgmental; giving the speaker undivided attention; observing body language and other nonverbal cues; attending to both facts and feelings; using thoughtful, open-ended, empathetic questions; allowing silence; restating and paraphrasing to show comprehension; and following up to ensure the person has no more to say (Lietzke 2021; Ohlin 2020). A crucial element is silence, which gives the patient time and space to think (Kacperek 1997) and can emblemize the clinician’s partnership and respect for the circumstances of the moment (Davidhizar and Newman Giger 1994). For example, October et al. (2018) audio-recorded pediatric intensive care conferences with family members, to measure characteristics of physician empathetic statements. Physicians’ “unburied” statements (use of pauses to allow family to respond) were found to be more effective than “buried” statements (medical-speak monologues not allowing time for family response) in revealing a family’s fears, hopes, and values.
In busy healthcare settings, clinicians may need to guide dialogue (Watanuki, Tracy, and Lindquist 2014). Clinicians’ training and experience—and chronic time pressures—encourage them to start formulating a response rather than staying focused on a patient’s attempt to convey a message (Watanuki, Tracy, and Lindquist 2014). Compressed medical care carries real risks of providing ineffective or undesired treatment, possibly missing a patient’s perspective that could alter a treatment plan and making the patient feel unheard and unvalued (Awdish & Berry, 2017; Verghese Anthony, 2016). Clinicians must encourage patient feedback—simply being asked a question can be influential (Bone et al. 2017; Celuch, Robinson, and Walsh 2015). When clinicians seek input and listen to patients, they embrace a spirit of partnership, pooling the physician’s experience with the patient’s self-knowledge, preferences, and values to achieve mutual decision-making and trust (Awdish and Berry 2017).
General Discussion
Our integrative review highlights communication’s multiple channels and layers. Although situated in the domain of clinician communication, the insights from our review are of value to academics and managers studying or applying communication theory in other service contexts.
Figure 2 presents the integrated framework that emerged from our review. This Figure retains the clinician communication channels and elements from Figure 1, as our review primarily focused on these channels. However, Figure 2 extends Figure 1 by summarizing and categorizing why, how, and when clinician communication influences patients thus highlighting additional insights gained from our review. Figure 2 shows that communication can affect patients’ psychological and behavioral outcomes by triggering cognitive, affective, motivational, and perceptual psychological processes. These processes can result in psychological outcomes that are perceptual (e.g., about the self or the situation), attitudinal (e.g., satisfaction), or relational (e.g., trust). Finally, these psychological processes and outcomes can lead to communicative (e.g., information disclosure) or action-oriented (e.g., treatment adherence) behavioral outcomes. Figure 2 also highlights that the effect of clinician communication on these processes and outcomes can be altered by moderating clinician, patient, and contextual factors. For example, the effect of metaphors on receivers’ attitudes (Sopory and Dillard 2002) and choices (Kronrod and Danzinger 2013) can be mediated by concept mapping (Lakoff and Johnson 1980), attention (Meier and Robinson 2006), memory (Crawford 2014), and perceptions (Casarett et al. 2010), and can be moderated by receiver knowledge (Landau et al., 2018). An integrative framework of clinician communication.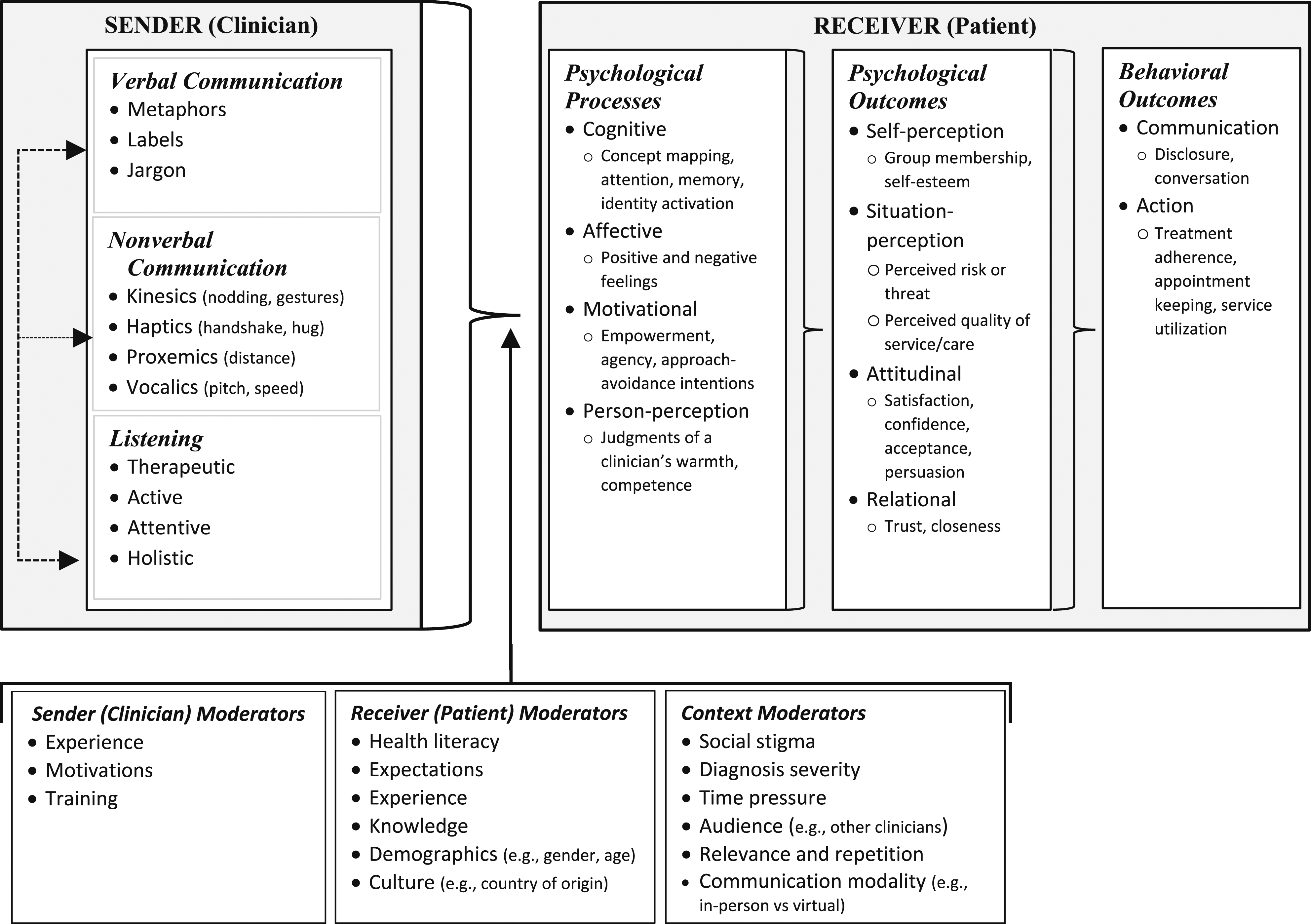
In the following sections, we leverage this integrative framework in two ways. First, we discuss a communications-based agenda for future research. Second, we use the framework to suggest opportunities for improving clinician communication.
Future Research Agenda
Words, Nonverbals, and Listening
Much more can be done to understand words, nonverbal cues, and listening—each modality deserves a focused research agenda. Even more critically, future work could explore interactions among these modalities, to examine what processes and outcomes the synergies trigger. For example, while nonverbal cues may generally exert their effects through nonconscious processes, they may trigger conscious processing when combined with incongruent words, such as when a clinician delivers serious news without making eye contact (Hargie 2016). Similarly, nonverbal cues like facial expression and tone of voice might moderate the effect of verbal cues like jargon and labels (e.g., Burgoon, Birk, and Pfau 1990), such as when a label is used with a sympathetic facial expression or when jargon is accompanied by an explanatory gesture. Observational studies of these communication modalities in medical and service settings would be valuable, as would studies that link specific modalities to outcomes such as patient satisfaction and adherence to prescribed treatments.
Communication Mediators and Outcomes
Research could better explicate mediator variables by exploring which communication channels elicit specific processes and which outcomes are best predicted by each process. For example: (1) nonverbal communication may be more likely to trigger person-perception processes (clinician judgments), rather than cognitive, motivational, or affective processes; and (2) communication outcomes, such as information disclosure, may be more impacted by affective than motivational processes. Research could also explore what words, nonverbals, or aspects of listening, affect specific outcomes. For example, while receivers’ perceptions of a sender’s warmth and competence are known to be influential (e.g., Aaker, Vohs, and Mogilner 2010), more recent work suggests that perceptions of a service provider’s moral character (i.e., their trustworthiness) may exert a stronger influence on outcomes than warmth and competence perceptions (e.g., Goodwin 2015). Given the impact of nonverbal cues on perceived trustworthiness and the importance of trust in communication, future research could consider the mediating role of senders perceived moral character in service-based communications.
Communication Moderators
Our review identified a variety of moderating variables related to the sender, receiver, and context (Figure 2). However, there are opportunities to study these variables further, apply them to different communicators, and identify additional variables. First, existing moderating variables could be explored in the context of our framework. For example, patients with higher health literacy may attend more to clinicians’ verbal communication, whereas those with lower health literacy may attend more to nonverbal communication. Alternately, more-experienced clinicians may use metaphors more effectively than less-experienced clinicians, which may affect medical outcomes. Second, moderators identified in one channel could be explored in other channels. Since culture influences patient responses to communication, it likely impacts clinician communication as well—for example, it may determine a clinician’s choice of metaphor or their use of nonverbals. Further, since repetition has been shown to moderate the impact of metaphors, this variable could be applied to other communicative elements (e.g., labels). Third, novel moderators could be explored. For example, specific aspects of communicative audiences, such as type (e.g., family members vs. doctors in training) or size (e.g., partner vs. entire family) could alter clinicians’ communication and patient outcomes. Alternately, individuals who are more or less comfortable with interpersonal touch (Luangrath and Peck 2015) might respond differently to haptic communication in terms of processes (e.g., motivational) or outcomes (e.g., trust, disclosure).
Communicative Modalities
Most clinician-patient interactions still occur face-to-face, and the majority of the articles we reviewed focused on this modality. However, technology and the COVID-19 pandemic have altered healthcare communication: portals offer patients access to their medical records, and telehealth enables remote, visual interactions. These modalities privilege different aspects of our integrative framework—for example, telehealth emphasizes verbal communication and limits nonverbal communication to what is visible on screen. Future work could explore how message encoding through verbal and nonverbal channels differs between these modalities. For example, are nonverbal cues like kinesics and vocalics as important in telehealth as they are in-person; are words more powerful when utilizing telehealth; do people listen more effectively during telehealth consultations?
Patients as Communication Cocreators
Although we focused on clinicians as senders, patients also use words, nonverbal cues, and listening to send and respond to messages. Indeed, patients contribute to their own care through their cocreation behavior (Danaher Tracey et al., 2023; McColl-Kennedy et al., 2012; Sweeney et al., 2015). Researchers should examine the dyadic and dynamic interplay of communication between a provider and customer. For example, exploring whether patients use metaphors to express or describe their emotions (Cavanaugh, MacInnis, and Weiss 2016) and whether this indicates a lack of cognitive understanding, or a self-perception or identity-based process. Additional research could identify words (e.g., “my diabetes” vs. “this diabetes”), nonverbal cues (e.g., gazing upward), or aspects of listening (e.g., repeating what the clinician has said) that patients use to signal particular psychological processes. For example, eye contact might indicate that a patient is trying to build closeness or trust with the clinician, while repetition might indicate an attempt to understand the clinician’s words. Such research could also explore variables that might moderate patients’ use of specific words, nonverbal cues, or aspects of listening, such as gender, socioeconomic status, race, or role (e.g., patient versus a surrogate such as a parent or caregiver).
Conversational Dynamics
Patients’ truthful disclosure of relevant information to their clinician can influence the accuracy of diagnoses and appropriateness of treatment. The patient must have sufficient trust in the clinician to disclose what often is sensitive information. Our framework shows that trust is an important consequence of clinician communication, highlighting the need for research on conversation, where clinicians and patients take turns as senders and receivers. Marketing research has explored some processes and outcomes of such conversational dynamics. For example, consumers who mimic others’ language use in online forums post more often (Moore and McFerran, 2017), and customers are more satisfied with agents who express warmth early in a conversation via emotional language, and competence later in a conversation via cognitive language (Li, Packard, and Berger 2020). Researchers could identify which aspects of clinician and patient conversation (e.g., mimicry of words or nonverbals) facilitate trust, shift the trajectory of an interaction, or alter patient outcomes. (Dehay and Landwehr 2019).
Improving Clinician Communication
Communicating with patients to strengthen their understanding and trust, engage in well-considered decision-making, and make good behavioral choices, is part art, part science (Pellegrini 2017; Stuart et al. 2019). As our review demonstrates, clinicians must also tread cautiously, ensuring that their communication with patients is appropriate and sensitive. Using a label a patient finds offensive or engaging in touch a patient finds inappropriate could cause patients to change providers, post negative comments on public platforms, or file lawsuits. Each patient’s uniqueness—physically, emotionally, and otherwise—demands individually tailored language. And while much about healthcare is not controllable, how clinicians communicate with patients is. Opportunities for improving clinician communication abound, and these possibilities are pertinent to other service providers.
Be Mindful of Word Choice
Some words are “never words” that can make the recipient defensive, undermine their self-efficacy and self-esteem, and negate their trust in the service provider (Berry et al., 2021). For example, consistent with our framework, the use of labels (e.g., “drug addict”) often has a blaming effect (Dickinson et al. 2017). Clinicians (and other service providers) would help both themselves and their patients (customers) by periodically gathering staff for the purpose of identifying commonly used language that offends, scares, or confuses—and then banish their use (Berry et al. 2021), as some major corporations, such as Apple, have done (Johanson 2017). Service providers can benefit from guidance and training that broadens their understanding of how to adjust their communication style depending on the customer and the situation. Supervisors can use training methods such as role-playing and direct observation and feedback on interactions.
Maximize the Benefit of Nonverbal Cues
Our framework shows the importance of nonverbal communication. Clinicians and other service providers can communicate more effectively by tactfully using nonverbal cues. As mentioned, eye contact is an especially influential type of kinesic nonverbal communication. In conjunction with words and other nonverbals, eye contact—or its absence—can increase or decrease trust in clinicians (Sundaram and Webster 2000). Although physicians sometimes need to stand over patients, such as during a physical exam, sitting at eye level with them during conversation sends a more positive message of unhurried, patient-focused care. Many medical exam rooms were designed before electronic health records (EHRs) and became an integral part of healthcare delivery. An unintended consequence of the EHR is that many doctors spend more time during the visit looking at the computer than at the patient (Berry et al. 2020). Exam rooms can be reconfigured so that a doctor can use the computer while facing the patient and even swivel the monitor to share an image or data with the patient. In services, communication-skill training needs to emphasize the power of nonverbal and listening behaviors and not focus only on verbal communication.
Inform Customized Communications
Healthcare is moving toward precision medicine, tailored to each patient’s genetics and lifestyle. Our framework—especially the moderating variables—suggests that patient communication should mirror this shift. It takes time and effort to get to know a patient, much like earning customers’ patronage and loyalty in other services. The moderating variables identified in our review offer some guidance on sender, context, and patient factors that could be considered when individualizing communication. Patients vary in their illnesses, personal values, emotions, degree of family support, demographics, and other characteristics. A military veteran with PTSD may not react well to war metaphors; one patient may bristle at being called by her first name while another is comforted by it.
Individualizing communications requires good communication practices, and starts with asking questions and listening carefully to the answers—with attention to specific words or nonverbal cues that might be illuminating. For example, oncologist Daniel Martin uses an “ask-tell-ask” approach of inviting patients to describe their understanding of their condition, followed by offering needed clarifications in plain English, and asking patients to restate what was said in their own words. Martin then writes up the salient information in clear language in Open Notes, where patients can read a summary of the visit (Martin 2015). Further, open-ended queries can identify patients’ primary concerns, priorities, personal values, and other individual traits. “What questions do you have for me?” invites candor in a way that “Do you have any questions?” may not (Moriates 2016). Palliative care physician Susan Block learns from seriously ill patients by asking questions such as “What do you understand your prognosis to be?”; “What are your concerns about what lies ahead?”; “What tradeoffs are you willing to make?”; “How do you want to spend your time if your health worsens?”; and “Who do you want to make decisions if you can’t?” (Gawande 2014). These questions can be reoriented to reflect a myriad of professional service settings.
Teach Multimodal Communication Skills
Sharp interpersonal instincts do not substitute for excellent care-communication skills (Gilligan, Bohlke, and Baile 2018). Being articulate does not necessarily transfer into deftly eliciting a seriously ill patient’s goal for treatment (e.g., prolonging survival with the likelihood of harsh treatment side effects versus living a shorter, but higher-quality life). Many service providers must deliver bad news (“The flight is canceled”), but it is typically not life-changing. Informing a patient and family members that the paralysis from an accident is likely to be permanent, or that a disease cannot be cured, is “bad news” at an entirely different level. Many clinicians have never formally cultivated their skills in navigating emotionally charged, complex interactions with patients, which requires the coordinated, purposeful use of words, nonverbals, and listening. Accordingly, major health systems are increasingly investing in communications training for clinical staff. Cleveland Clinic’s R.E.D.E. to Communicate, Henry Ford Health System’s CLEAR Communications, and the University of Pittsburgh’s VitalTalk training programs all seek to better prepare a clinician to grasp the essence of a patient’s story before creating an appropriate care plan. Becoming skillful in conflict resolution is also essential—for example, when patients insist on medically inappropriate interventions or when intrafamily disagreements occur (Berry et al. 2021).
In addition to enhancing training across communication channels (verbal, nonverbal, listening), training could be extended to the multiple modes clinicians now use to communicate. Current training emphasizes verbal, in-person interactions—and while these are still the most common type of interaction, clinicians now communicate through patient portals using text, and through telehealth using video and voice. Different aspects of the integrative framework come into play across these modalities. For example, in a large study of how patients felt when reading their medical records, 11% indicated they felt judged or offended or both. The three main themes were errors and surprises, being labeled (e.g., as “anxious”), and phrasing perceived as disrespectful (e.g., “the patient denies”; Fernandez et al. 2021).
Further, physicians’ common use of jargon and abbreviations in medical records can be problematic. For example, F/U refers to “follow up” in medical jargon but is not something most patients would want to see in their medical record (Parker-Pope 2021). Patient portals require clinicians to focus on words, without the potential for nonverbals or listening to modify or clarify the message. In contrast, the growth of telehealth offers opportunities for clinicians to hone their nonverbal skills for virtual encounters. Given the limitations of remote communication technologies, clinicians and other service providers need to make a concerted effort with their (viewable) gestures, eye contact, and vocalics to build rapport and trust, give comfort, and humanize service delivery in this setting.
Conclusion
Healthcare is a consequential service that all people use, and the quality of communication between provider and patient plays a central role in the overall quality of the service. Clinicians themselves of course face the biggest challenges—and stand to derive the greatest benefits (along with their patients)—in understanding the complexities of their communication practices and then implementing change, as our framework and supporting literature synthesis make clear. But behind these clinicians are professionals—from the service, marketing, psychology, communications, and medical fields—whose research and other endeavors can facilitate the efforts of the people who do the daily work of patient care.
With this article, we hope to stimulate the ideas, marshal the will, and encourage the coordination of researchers across multiple disciplines to contribute to improved healthcare communications. We see optimal communication as one of the next great frontiers in healthcare service delivery. Our focus on clinician communication in this study opens the door for more academic research aimed at better understanding the patient’s active role in healthcare communication given the salience of cocreation in this service. Once both the clinician and patient perspectives are better understood, researchers can focus on studying the dynamic interplay that unfolds when clinicians and patients communicate.
We hope that our framework helps equip relevant stakeholders with the tools they need to attain real, measurable progress in this life-changing domain. We also hope that our framework stimulates new thinking and improvement in communications in the delivery of non-healthcare services. Given healthcare’s complexities, intimacy, and high stakes, much can be learned from studying it that can be adapted and applied to other services.
Supplemental Material
Supplemental Material - Improving How Clinicians Communicate With Patients: An Integrative Review and Framework
Supplemental Material for Improving How Clinicians Communicate With Patients: An Integrative Review and Framework by Tracey S. Danaher, Leonard L. Berry, Chuck Howard, Sarah G. Moore, and Deanna J. Attai in Journal of Service Research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.