
Abstract
Introduction:
Social determinants of health (SDH) influence and modify the risk for mental health disorders. To our knowledge, no study has explored SDH in the context of mental health in Saudi Arabia (SA) using population-based data. This study investigated the association between several SDH and anxiety and mood disorders in SA.
Methods:
We utilized data from the nationally-representative Saudi National Mental Health Survey (SNMHS) conducted in 2014 to 2016. This study examined associations between personal-level, socioeconomic, physical health, and family environment characteristics and anxiety and mood disorders. Participants were classified as having anxiety-only disorders, mood-only disorders, or comorbidity of both disorders. Multinomial logistic regression models were employed to examine the associations between SDH and anxiety and/or mood disorders, comparing them to participants who had not experienced these disorders.
Results:
A total of 4,004 participants were included in this analysis; the lifetime prevalence of disorders was: anxiety only (18%), mood only (3.8%), and comorbidity of both (5.3%). Regression models indicated that females, young adults (26–35 years), individuals with a higher level of education, and those who were separated or widowed had higher odds of experiencing anxiety and/or mood disorders. Furthermore, there was a significant and direct association between having physical chronic conditions and all three categories of anxiety and mood disorders. Experiencing Adverse Childhood Events (ACEs) was also associated with a significant risk of developing anxiety and/or mood disorders, with the highest risk associated with physical or sexual abuse, followed by violence and neglect.
Conclusion:
This study underscores the correlation between several personal-level, socioeconomic, and environmental SDH and anxiety and mood disorders in SA. These findings provide a foundation for future analyses examining the intricate interplay between upstream and downstream SDH in SA. Such research can enhance local scientific knowledge, aid in planning for social services, and inform policy decisions and treatment strategies.
Keywords
Introduction
Mental health disorders (MHDs), including anxiety and mood disorders, are growing challenges to health and well-being. Globally, anxiety and mood disorders are among the leading causes of years lived with disability (GBD 2019 Mental Disorders Collaborators, 2022; Hidaka, 2012). In Saudi Arabia, data from the nationally representative Saudi National Mental Health Survey (SNMHS) indicated that (34.2%) of the population had experienced at least one mental health disorder during their lifetime, while (20%) experienced a mental health disorder in the past 12 months (Altwaijri, Al-Habeeb, Al-Subaie, et al., 2020; Altwaijri, Al-Subaie, et al., 2020). The most prevalent disorders were anxiety (23.3%), mood (9.3%), and disruptive behavior disorders (11.2%), and one in every four participants experienced two or more MHDs during their lifetime (Altwaijri, Al-Subaie, et al., 2020), while treatment seeking was minimal (Alangari et al., 2020).
In recent decades, the relationship between social determinants of health (SDH) and MHDs, including anxiety and mood disorders, has gained increasing attention (Lund et al., 2018). Social determinants are defined as ‘the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life’ (Blas & Kurup, 2010). Social determinants could encompass elements that are not modifiable (e.g., age or race/ethnicity), while others are amenable to change (e.g., home and neighborhood environments). The whole hierarchy of SDH is linked to MHDs’ etiology, prognosis, and association with seeking mental healthcare. Social determinants such as female gender, age, low socioeconomic status, and unemployment are associated with a higher prevalence of anxiety and depressive disorders (Averina et al., 2005; Cheah et al., 2020; Mohammad et al., 2020; Reile & Sisask, 2021; Silva et al., 2016). Similarly, social factors like poor living conditions and adverse childhood experiences (e.g., violence, neglect, abuse) are associated with MHDs later in life (Dahal et al., 2018; Kessler et al., 2010; Paananen et al., 2013). Contextual social factors play an essential role in MHDs; for example, lack of social support and certain cultural/religious beliefs could ameliorate or exacerbate the risk of MHDs in different contexts (Heim et al., 2017; Maulik et al., 2010; Salsman & Carlson, 2005; Vaingankar et al., 2020). Therefore, examining context-specific SDH and how they correlate with MHDs is paramount for risk stratification, allocation of resources, and provision of care for MHDs.
Evidence for the association between social determinants and mental health comes mainly from Western countries (Patel, 2000). Several studies have demonstrated an association between social determinants and mental disorders (Dahal et al., 2018; Lund et al., 2018; Paananen et al., 2013; Silva et al., 2016). Compared to Western countries, Arab countries have different sociocultural systems; thus, different levels, compositions, and dynamics of SDH. These, in turn, may lead to differences in the major etiologies of common MHDs and should be more thoroughly investigated in the local and regional context.
Saudi Arabia’s research on the association between social determinants and health is still nascent. Some recent efforts have examined the impact of social determinants on general and mental health but were limited to the primary care sector or age-specific individuals (Abou Abbas & AlBuhairan, 2017; Almujadidi et al., 2022; Baghdadi et al., 2021). Moreover, these efforts often explored a limited set of social determinants (e.g., age, gender, marital status, education/employment) in the context of mental health. To our knowledge, no studies have explored the association between social determinants and mental health in Saudi Arabia in a nationally-representative sample. The current study explores the association between various SDH and anxiety and mood disorders in Saudi Arabia.
Methods
Sampling and participants
The Saudi National Mental Health Survey (SNMHS) is a part of the World Health Organization’s (WHO) World Mental Health (WMH) survey initiative (Kessler et al., 2009). The SNMHS is a nationally representative community survey of Arabic-speaking Saudi citizens between the ages of 15 and 65 (Mneimneh et al., 2020). The survey covered 11 out of 13 administrative areas in Saudi Arabia; 2 administrative areas were excluded due to security concerns during the data collection period. SNMHS was a face-to-face household survey conducted through trained interviewers (Altwaijri, Al-Habeeb, Bilal, et al., 2020). Based on the 2010 Saudi population census from the General Authority for Statistics, a multistage clustered probability sampling was conducted between 2011 and 2016. The sampling and weight creation were described in detail elsewhere (Mneimneh et al., 2020). One male and one female participant were invited to participate from selected households within primary sampling units within each of the 11 strata. Participants in (part I) were offered the core sections of the (SNMHS) survey, while a sub-sample (part II) was selected to respond to the non-core sections. Part II participants included two types: those who did not endorse any MHDs in the core sections (chosen with a probability of 0.25) and those who endorsed any MHDs from the core section (selected with certainty into part II). Weights were generated for parts I and II in response to the multistage and individual-weight sampling (Altwaijri, Al-Habeeb, Bilal, et al., 2020; Mneimneh et al., 2020). All analyses in this paper accounted for the multistage sample by applying the relevant weights for each analysis separately (i.e., for part 1 or part 2, according to which disorders were included in each part). Interviewers obtained written informed consent prior to each interview. The study was conducted in accordance with the Declaration of Helsinki and all field and consent procedures were approved by the Institutional Review Board committee at the King Faisal Specialist Hospital & Research Centre, Riyadh (RAC#: 2091093).
Instruments
Like other WMH surveys, the SNMHS utilized the WHO’s Composite International Diagnostic Interview (CIDI) in its third version (Altwaijri, Al-Habeeb, Bilal, et al., 2020). CIDI is a fully structured survey commonly used for community surveys, which employs a stem-branch approach to capture the lifetime and 12-month prevalence of selected MHDs. The CIDI 3.0 was translated, adapted, and pretested in the Saudi population (Shahab et al., 2019). In addition, some sections were added to the Saudi CIDI 3.0 to capture context-specific data (e.g., religiosity, polygamy, and attitude toward alcohol use). The Saudi CIDI 3.0 was administered by lay interviewers using computer-assisted personal interviews (CAPI) except for sections deemed sensitive (e.g., substance and alcohol use), that were administered by Audio Computer-Assisted Self Interview (ACASI). In the SNMHS, the Diagnostic and Statistical Manual for Mental Disorders, fourth edition (DSM-IV) (Altwaijri, Al-Habeeb, Bilal, et al., 2020) were used to generate mental health diagnoses from CIDI 3.0 to facilitate comparing results with WMH results elsewhere.
Variables
SDH variables
We included a variety of SDH variables spanning personal-level, socioeconomic (SES), general health, environmental, and childhood-related domains. For the personal (i.e., demographic) domain, we collected data on gender (binary: male/female); age as a categorical variable (15–25, 26–35, 36–50, and 50+ years) to facilitate comparison with other WMH/SNMHS results and to better capture age-related experiences (e.g., entry to the workforce); for the marital status (Married, Never Married, Separated/Divorced and Widowed) we elected to isolate the widowed individuals into a distinct category as the mechanism of un-coupling is different compared to separated/divorced; ever being in a polygamous marriage (Yes, No, and never-married) was reported for the overall sample and stratified by gender. For the SES domain, we included data on education (low 0–6, low average 7–9, high average 10–15, and high +16 years); employment status (Employed, Unemployed, Homemaker, Student, and Others); ever receiving public assistance (yes, no); and income as a ratio of income per capita to the median of the sample, the income per capita is a composite variable that synthesizes the personal income, spouse’s income, and family’s income. The income was classified as (low if the ratio is below 0.5, low-average if between 0.5 and 1, high-average if between 1.1 to 2, and high if the ratio is bigger than 2).
We included information on physical health as this has an intricate, bidirectional association with SDH; specifically, we asked participants about their body mass index (BMI), smoking habits, and if they have any chronic conditions, including cancer, arthritis or rheumatism, chronic back or neck problems, headaches, any other chronic pain, high blood pressure, heart disease, asthma, any other chronic lung disease, like COPD, tuberculosis or emphysema. Then, participants were categorized if they had not experienced any conditions, 1 to 2, or 3+ conditions. For the religious domain, we included a single item asking participants about the frequency of seeking comfort through religious and/or spiritual practices when faced with problems and classified that into (often/sometimes or rarely/never).
For the environmental domain, we included items on the area where the participants were raised (large cities/suburbs/villages or rural areas) and if they moved neighborhoods or towns during childhood. Also, we included household religiosity during childhood, measured on a 4-point Likert scale and categorized as religious (somewhat religious and very religious) and non-religious (not at all religious/not very religious). Lastly, we included items about several Adverse Childhood events (ACE) like physical or sexual abuse, neglect, family economic adversity, physical illness, violence, parental divorce, loss, or mental illness. We operationalized all variables as dichotomous variables as follows: Yes, if participants gave an affirmative answer to ever being subjected to a specific ACE through a series of questions, and No otherwise. To quantify the frequency of ACE, we created a variable of how many ACEs the participant experienced: none, one to two, and three or more ACEs.
Anxiety and mood disorders
We examined mood and anxiety disorders included in the SNMHS survey and classified participants into four groups: having either anxiety or mood disorders only, having a comorbidity between anxiety and mood disorders, or neither anxiety nor mood disorders. The presence of an anxiety disorder included an affirmative diagnosis of any of the following disorders: general anxiety disorder (GAD), obsessive-compulsive disorder (OCD), adult separation anxiety, panic disorder, agoraphobia, social phobia, and Post-Traumatic Stress Disorder (PTSD). Mood disorders included the presence of either major depressive or bipolar disorders. Lastly, the presence of any MHDs other than anxiety or mood disorders was coded as a binary variable and included in the analyses.
Statistical analysis
The lifetime and 12-month prevalence of anxiety and mood disorders were presented for the sample, with weights for parts I and II used as indicated. The distributions of mood and anxiety disorders by the different SDH variables were presented in raw frequencies and weighted percentages for parts I and II; standard errors (SE) were calculated for prevalence values. The descriptive analyses included the whole sample of SNMHS of 4,004 participants. We stratified the lifetime prevalence by gender to examine potential gender-based differences in anxiety and mood disorders distribution.
To explore the association between the different SDH and anxiety and mood disorders, we used crude and adjusted multinomial regression models, with ‘no anxiety nor mood disorders’ as the reference level. Then, after adjusting for age and gender in each model, we assessed the association between each SDH and the presence of anxiety and mood disorders. We elected not to combine various SDH variables in sequential models as our analysis is exploratory rather than causal, and we expected high collinearity between some variables (e.g., education and income). As a sensitivity analysis, to explore if polygamy is associated differently with anxiety/mood disorders based on gender, we included an interaction term between gender and status of polygamy and anxiety/mood disorders. Results were presented using odds ratios and 95% confidence intervals. As some anxiety disorders were only included in the non-core section of SNMHS, part II participants and weights were included in the regression analyses (n = 1981). All analyses were conducted using SAS software 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Sample’s characteristics:
Adolescents and young adults (aged 15–25) constituted (39%) of the participants in SNMHS, and the sample was comparably distributed between males and females (Table 1). Around one-third of the sample had at least a bachelor’s degree (36%); close to half of the participants were classified as having low income (43%), with one-tenth (11%) reporting having received public assistance at least once. Half of the participants were married, and (5%) were in polygamous marriages. Most participants described their household during childhood as very religious (95%), and (80%) reported they sometimes or often seek religious/spiritual comfort when faced with problems. More than half of the participants reported BMI above 25, indicating overweight or obesity (54%), had at least one physical condition (69%), and other MHDs in addition to anxiety and/or mood disorders (17.6%). Regarding childhood environment, the most prevalent ACEs reported by participants was physical abuse (14.3%). Around one in every four participants had experienced one to two ACEs during their childhood, while (2.4%) reported exposure to three or more ACEs (Table 1).
Demographic, socioeconomic, physical health, and childhood environment characteristics by categories of anxiety and mood disorders.
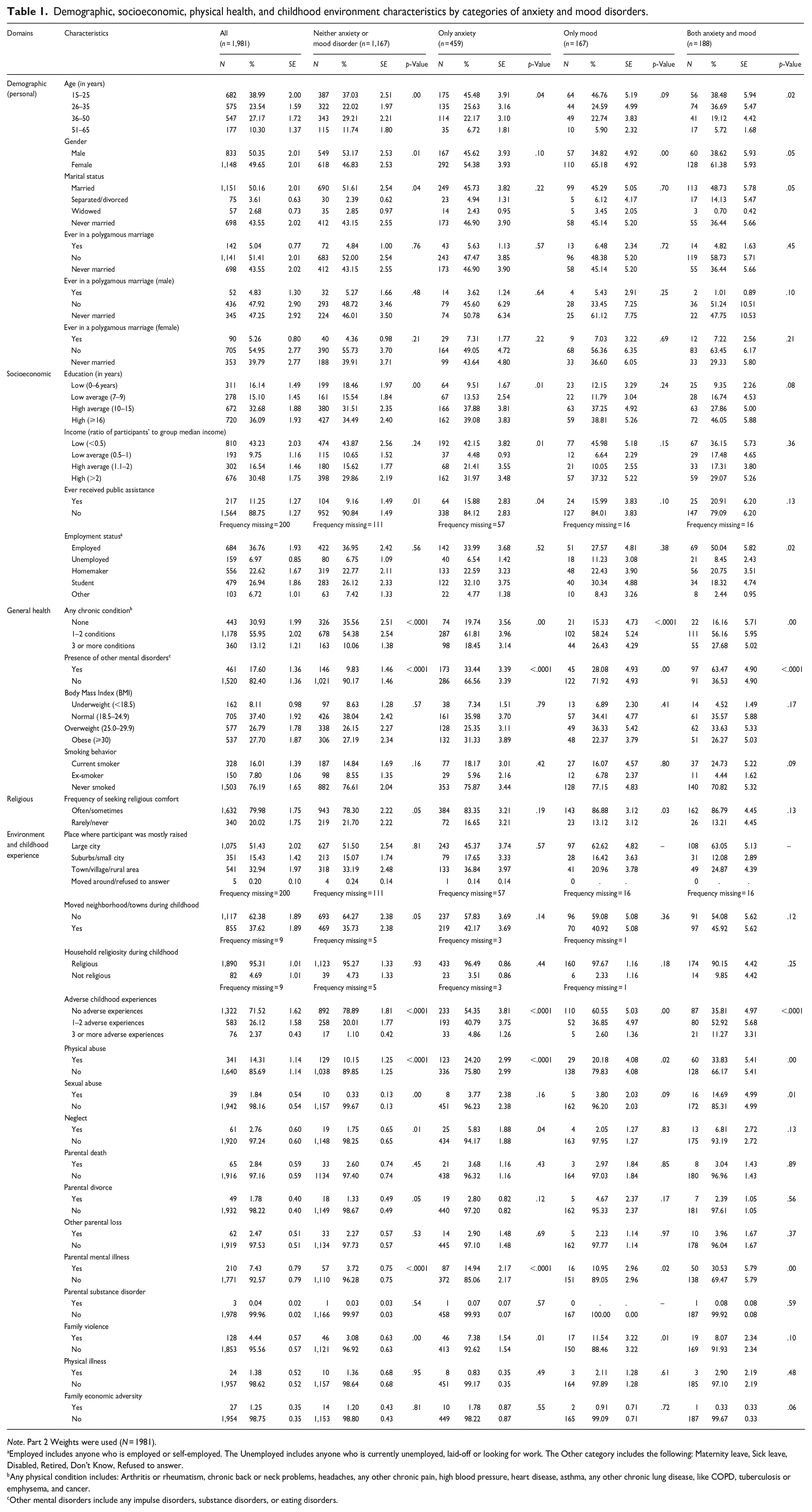
Note. Part 2 Weights were used (N = 1981).
Employed includes anyone who is employed or self-employed. The Unemployed includes anyone who is currently unemployed, laid-off or looking for work. The Other category includes the following: Maternity leave, Sick leave, Disabled, Retired, Don’t Know, Refused to answer.
Any physical condition includes: Arthritis or rheumatism, chronic back or neck problems, headaches, any other chronic pain, high blood pressure, heart disease, asthma, any other chronic lung disease, like COPD, tuberculosis or emphysema, and cancer.
Other mental disorders include any impulse disorders, substance disorders, or eating disorders.
Anxiety/mood disorders by categories of SDH:
Adolescents and young adults reported a substantial prevalence of anxiety and mood disorders (45.5% and 46.8%, respectively) (Table 1). Two in every five individuals with anxiety only or mood only disorders had at least a bachelor’s degree, while that ratio was almost one in every two participants for having comorbidity between anxiety and mood disorders. In addition, employed or students participants accounted for most cases of anxiety and mood disorders (Table 1). More than two-thirds of the participants with anxiety, mood, or comorbidity had at least one physical chronic condition as well. Among participants who did not have any anxiety or mood disorders, one in ten (9.8%) had another mental health disorder (Table 1).
Participants who sometimes or often experienced physical abuse during childhood represented (24%) of participants with anxiety only disorders and (20%) with mood disorders. Among participants who had anxiety and mood comorbidity, one in every seven was subjected to sexual abuse during childhood (Table 1).
Lifetime prevalence of specific anxiety and mood disorders and differences by gender:
Almost one in every five individuals had an anxiety disorder only during their lifetime (18%), with adult separation anxiety was the most prevalent anxiety disorder (12%). On the other hand, the lifetime prevalence of mood only disorders was (3.8%), and the comorbidity between anxiety and mood disorders 5.3% (Supplemental Material 1).
There were differences in the lifetime prevalence of anxiety/mood disorders by gender (Supplemental Material 1). For instance, females had twice as high lifetime prevalence of mood only disorders compared to males, (5% vs. 2.6%) respectively. The prevalence of different types of anxiety disorders was comparable between females and males with the exception of generalized anxiety disorder, social phobia, and agoraphobia, where females had considerably higher prevalence (Supplemental Material 1).
Association between SDH and anxiety/mood disorders:
In Table 2, the crude multinomial models showed that females had significantly higher odds of having anxiety only OR = 1.4 (95% CI [1.1, 1.7]), mood only 2.1 [1.3, 3.5], and comorbidity between anxiety/mood 1.8 (95% CI [1.2, 2.7]) disorders compared to males. Compared to young adults (26–35 years), participants in older age groups seem to have lower odds of experiencing anxiety and/or mood disorders.
Crude and adjusted multinomial logistic regression models examining demographic, socioeconomic, physical health characteristics with anxiety and mood disorders.
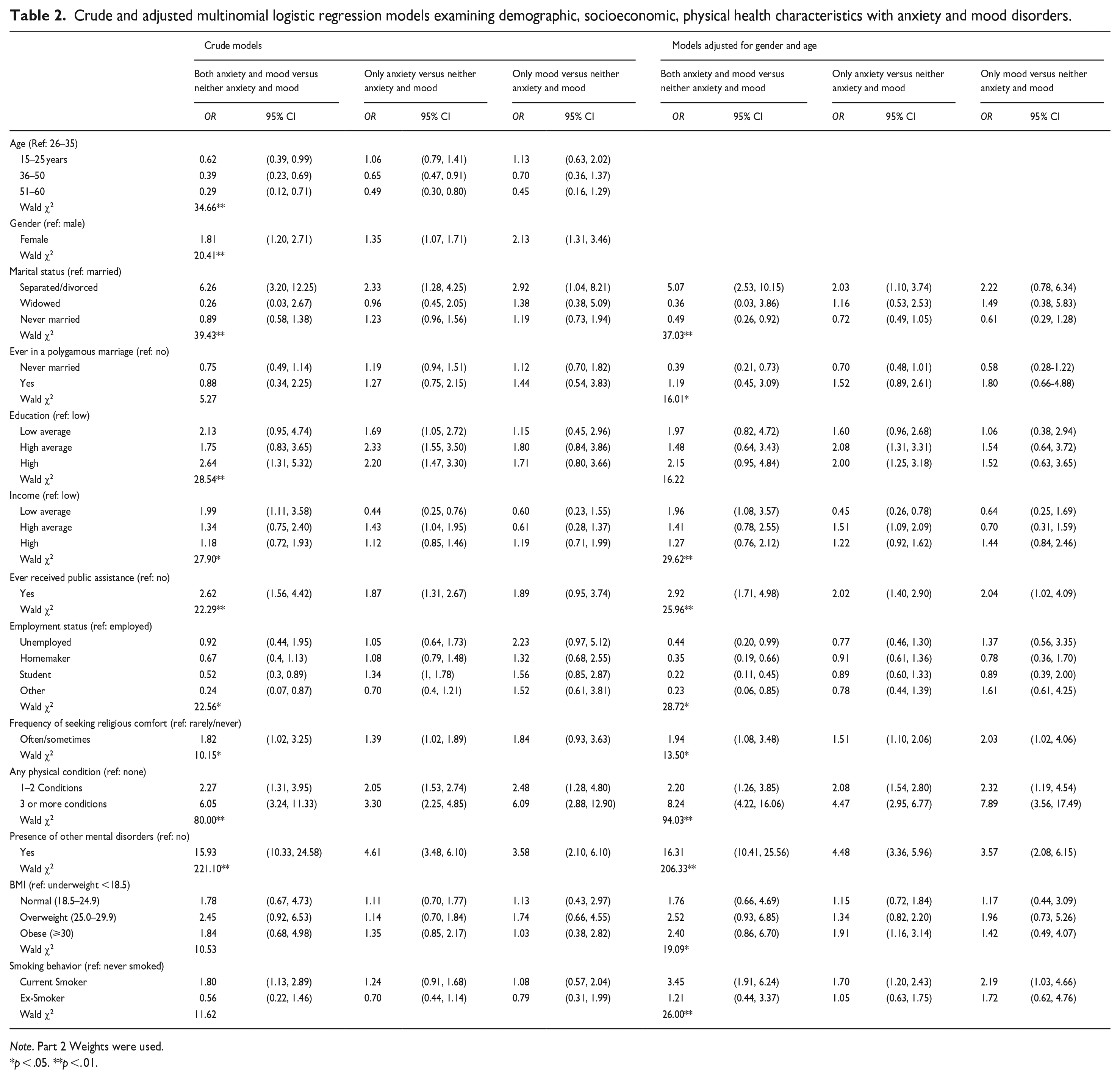
Note. Part 2 Weights were used.
p < .05. **p <. 01.
In the adjusted multinomial models, compared to participants with lower levels of education, participants with higher levels of education displayed increased odds of anxiety, mood, and comorbidity disorders (Table 3). These associations were less consistent when income per capita was considered.
Crude and adjusted multinomial logistic regression models examining environmental and childhood experience characteristics with anxiety and mood disorders.
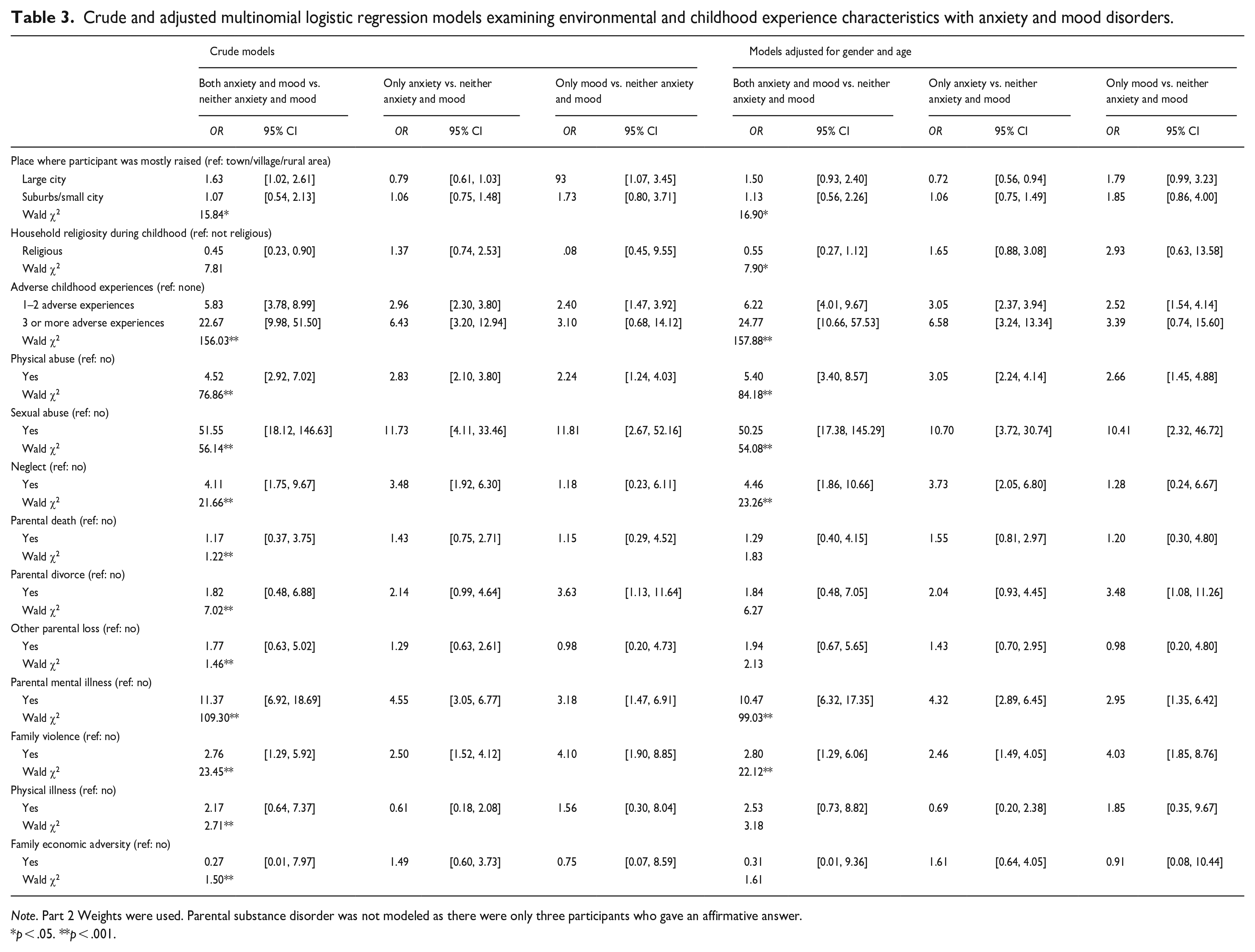
Note. Part 2 Weights were used. Parental substance disorder was not modeled as there were only three participants who gave an affirmative answer.
p < .05. **p < .001.
Participants who were widowed or divorced had significantly higher odds of experiencing anxiety, mood, or anxiety/mood comorbidity compared to married participants. Participants who ever were in polygamous marriages displayed a trend of anxiety and mood only disorders compared to participants who were/are in monogamous marriages (Table 2). When examined in more depth, we found a significant interaction between gender and polygamous marriage status and anxiety or mood disorders – where in polygamous marriages, females had higher odds of experiencing anxiety compared to males (Supplemental Material 2). The frequency of seeking religious/spiritual comfort generally had significant and direct associations with anxiety, mood, and anxiety/mood comorbidity disorders (Table 2).
There were significant dose-response associations between the number of ACEs experienced and all anxiety, mood, and anxiety/mood comorbidity disorders (Table 3). Overall, almost all types of ACEs were associated with increased odds of having anxiety and/or mood disorders. The highest magnitude of association was noted for participants who were subjected to sexual abuse, followed by physical abuse, neglect, and family violence (Table 3).
Discussion
This study presented the first analysis of the relationship between a wide range of social determinants of health (SDH) and anxiety and mood disorders among the Saudi population, utilizing nationally-representative data. Our findings suggested that SDH indicating higher socioeconomic status (e.g., income and education) are associated with increased odds of anxiety disorders. Exposure to adverse childhood experiences (ACEs) was linked with an increased risk of developing anxiety and/or mood disorders. The associations between specific ACEs and the presence of anxiety and/or mood disorders varied in magnitude, and experiencing more ACEs showed increased odds of anxiety and/or mood disorders compared to lower instances of ACEs. Lastly, our results showed that individuals with physical comorbidities have higher odds of experiencing anxiety and/or mood disorders.
This study affirmed previous findings that indicate an increased likelihood of anxiety and/or mood disorders associated with SDH, namely: female gender, being divorced or separated, and younger age (Altwaijri, Al-Subaie, et al., 2020; Lund et al., 2018; Maulik et al., 2010; Tanios et al., 2009). The current analysis revealed that women experienced three times as many mood disorders compared to men, a pattern already observed in literature. This finding may be linked women’s vulnerability to the stress, uncertainty, emotional upheaval, and social changes associated with divorce or separation, which might be more pronounced in the Saudi context where women who are divorced or separated are stigmatized – potentially triggering or exacerbating anxiety or mood disorders (Maulik et al., 2010; Richards et al., 1997). Additionally, our analysis indicated that young adults aged 26 to 35 face higher odds of anxiety and/or mood disorders compared to older age groups. This particular finding is concerning as the Saudi population is among the youngest globally, with a median age of 40 years. Thus, the high prevalence of anxiety and/or mood might continue for years to come. Collectively, these findings highlight the importance of future analyses that explore pathways (that are amenable to interventions) linking these SDH to anxiety and mood disorders among the Saudi population.
Our findings regarding the relationship between indicators of higher socioeconomic status (such as income, education, and employment) and higher odds of anxiety-only disorders were unexpected and contrary to most existing studies in the literature. Previous research indicates that lower levels of education and/or income are associated with a greater risk of anxiety disorders (Bjelland et al., 2008; Kronfol et al., 2018; Lund et al., 2018; Paananen et al., 2013; Tanios et al., 2009). The association between education, employment, and anxiety/mood disorders in our analysis may be partially attributed to the stress experienced in the workforce, such as job-security concerns and a competitive labor market, which could increase the risk of anxiety disorders (Chang-Quan et al., 2010). In our analysis, the income variable was a composite measure (income per capita) that accounts for family, spouse, and individual income and may not necessarily reflect personal income or financial independence. This situation is further influenced by some cultural norms among some communities within Saudi Arabia that might assign financial responsibility to males as heads of households, resulting in less financial autonomy for other household members, or view females’ contribution as unworthy (Alhawsawi & Jawhar, 2023; Syed et al., 2018). Furthermore, other analyses of SNMHS data indicated that women and men had differential associations between relative income and MHDs. These results and potential explanations emphasize that socioeconomic variables are interrelated, and the impact of each component is context-specific within the social settings individuals inhabit (Alegria et al., 2018; Phelan et al., 2010). This conclusion aligns with observations that anxiety disorders demonstrate differential distribution across socioeconomic indicators when stratified by race/ethnicity or country-level income (Nunes et al., 2022; Ruscio et al., 2017).
Our findings provided evidence supporting a significant association between physical comorbidities and anxiety and mood disorders. Specifically, participants with a higher number of physical conditions exhibited greater odds of experiencing anxiety and/or mood disorders. Our results agreed with the existing literature that offers insights into various mechanisms through which physical and mental health mutually influence each other, including pain, worry, functional limitations, and lifestyle modifications (Baghdadi et al., 2021; Gabilondo et al., 2012; Jurisson et al., 2021; Scott et al., 2016; Tsang et al., 2008). These findings hold particular significance within the Saudi context for two main reasons. Firstly, in Saudi Arabia chronic diseases are highly prevalent, indicating a higher potential risk of comorbidity with anxiety and/or mood disorders (Alzahrani et al., 2023; Tyrovolas et al., 2020). Secondly, this association should be taken into consideration when designing healthcare for individuals with physical comorbidities. An interdisciplinary approach that addresses the potential psychosomatic repercussions of physical conditions may prove more effective in delivering comprehensive and effective healthcare (Ford et al., 2004; Jones et al., 2023; Thurston et al., 2023).
Global evidence suggested that exposure to ACEs increases the risk of developing anxiety disorders during both adolescence and adulthood (Kaminer et al., 2022; Sahle et al., 2022; Zarse et al., 2019). Our analysis showed ACEs had a significant, direct association with the presence of anxiety disorders and the comorbidity of anxiety and mood disorders, similar to results from Saudi Arabia and elsewhere (AlHemyari et al., 2022; Alhowaymel & Alenezi, 2022; Almuneef et al., 2017; Kessler et al., 2010; McCutchen et al., 2022; Zarse et al., 2019). However, the association was stronger for certain types of ACEs (e.g., physical or sexual abuse), while others had a weaker association (e.g., family violence) or did not reach statistical significance (e.g., family economic adversity). Moreover, different ACEs, in general, had weaker associations with mood only disorders (compared to anxiety or comorbidity disorder) than other studies (Kessler et al., 2010; McCutchen et al., 2022; Spinhoven et al., 2010). One potential explanation is our choice of model (multinomial logistic) and reference category (those with no anxiety nor mood), which intentionally controlled for anxiety disorders. For example, in other analyses, the comparison could be individuals with mood vs. individuals with no mood disorders but can have anxiety disorders, as such, measures of association could be inflated by including other disorders. Moreover, results of stronger associations between ACEs and anxiety only disorders might reflect that we looked at the collective presence of any of the seven anxiety disorders at once rather than focusing on selected disorders as noted in previous research. Nevertheless, these results invite future research into the specificity of ACEs in the risk of particular anxiety and mood disorders, which the SNMHS intends to explore soon.
Lastly, one of the interesting results was the association between seeking comfort through religious/spiritual practices and anxiety and/or mood disorders. As the prompt for this question was a single item, it is not comprehensive enough to measure religiosity as a construct. Thus, it is hard to infer a relationship between religiosity and anxiety and/or mood disorders among our population; however, the observed association deserves deeper exploration. Specifically, our observation hints that religiosity/spirituality could be leveraged as a complementary approach to mental health care, as evidence has shown its effectiveness in other contexts, especially in anxiety disorders (Goncalves et al., 2015; Razali et al., 1998; Saged et al., 2022).
Recently in Saudi Arabia, there have been new national priorities and policies aiming to enhance mental health and access to mental health care. Some of these efforts include the establishment of electronic mental health services platforms, a national hotline to support domestic violence victims, and initiatives to promote gender equality and women empowerment (Human Resources and Social Development, 2022; National Center for Mental Health, 2022). Therefore, results from the SNMHS serve as a baseline for the extent and burden of MHDs in Saudi Arabia. The current analysis is much needed to assess the specific association of SDH with mental health, especially considering the rapid economic transformation happening in Saudi Arabia. Future efforts can utilize our results, along with others from SNMHS, to help in planning, evaluating, and prioritizing national interventions that pertain to SDH and mental health in Saudi Arabia and the region.
Strengths and limitations
This study presented findings from Saudi Arabia’s largest national survey on mental health, which holds particular significance in revealing the prevalence of undiagnosed mental health disorders within the general, non-institutionalized Saudi population. It is the first population-based analysis to concentrate on a broad range of SDH in Saudi Arabia in the context of mental health. Additionally, the study employed a validated and standardized methodology (CIDI 3.0) to enable comparisons with results from the WMH initiative. The modeling strategy we used (multinomial logistic regression) allowed for simultaneous exploration and comparison of the specific associations between SDH and anxiety only, the mood only, or the comorbidity of both disorders, using a unified reference category. Furthermore, this study investigated culture-specific SDH (such as polygamy) that are seldom examined in the context of mental health and well-being. However, we could not explore the specific mechanisms through which socioeconomic status (SES) and environmental variables interact and influence anxiety and/or mood disorders. Additionally, our analysis centered on anxiety and mood disorders, primarily due to their high prevalence, so the findings regarding SDH may not apply to other mental health disorders (e.g., eating disorders or substance abuse) that may have differential associations with SDH.
Conclusion
This study utilized nationally representative data from the Saudi National Mental Health Survey, a part of the World Mental Health Initiative, to investigate the link between selected social determinants of health and anxiety and mood disorders. We specifically examined personal-level, socioeconomic, and family environment indicators in relation to the presence of anxiety disorders, mood disorders, and the comorbidity of both. Our findings demonstrated that higher socioeconomic status indicators, such as income and education, were associated with experiencing anxiety only disorders. Furthermore, exposure to adverse childhood events was strongly associated with developing anxiety disorders in isolation or combination with mood disorders. Different ACEs increased the odds of anxiety and/or mood disorders differentially.
To advance the field, future research should delve into the context-specific dynamics of socioeconomic indicators within Saudi Arabia. Additionally, a comprehensive examination of religiosity as a construct that influences and/or moderates anxiety and mood disorders might be valuable in the context of providing mental health care. Lastly, exploring the specificity of adverse childhood experiences (ACEs) in relation to mental health burden warrants further investigation.
Supplemental Material
sj-docx-1-isp-10.1177_00207640231197944 – Supplemental material for Social determinants of anxiety and mood disorders in a nationally-representative sample – Results from the Saudi National Mental Health Survey (SNMHS)
Supplemental material, sj-docx-1-isp-10.1177_00207640231197944 for Social determinants of anxiety and mood disorders in a nationally-representative sample – Results from the Saudi National Mental Health Survey (SNMHS) by Lubna A Alnasser, Maria Francesca Moro, Mohammad Talal Naseem, Lisa Bilal, Marya Akkad, Reema Almeghim, Abdulhameed Al-Habeeb, Abdullah S. Al-Subaie and Yasmin A Altwaijri in International Journal of Social Psychiatry
Footnotes
Author contributions
Conceptualization: LAA, MFM, YA, LB; Project administration and investigation: YA, LB, AAS, AAH; Supervision: LAA, MFM, YA, LB; Methodology: LAA, MFM, RA, YA, LB, MTN; Formal analysis: MTN, LAA, MFM; Writing – original draft preparation: LAA, MFM, RA, LB; Writing – review and editing: LAA, MFM, YA, LB, MA; Funding acquisition and resources: YA, LB, AAS, AAH.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The SNMHS is funded by the King Salman Center for Disability Research, Grant Number: KSRG-2022-048. The funder had no role in study design, data collection, data analysis, data interpretation, or writing of the report. All authors reviewed the manuscript and were responsible for the final decision to submit it for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.