
Abstract
Background
Recent data highlight problematic rates of mental health symptoms (MHS) among adolescents and young adults following the COVID-19 pandemic, with implications for early identification and clinical service provision. This study estimated the prevalence of MHS and its sociodemographic correlates among Canadian youths.
Methods
We conducted a cross-sectional analysis of 896 iundividuals aged 18–24 years using data from Statistics Canada’s Survey on COVID-19 and Mental Health. Symptoms of anxiety, psychological distress, depression, and post-traumatic stress disorder (PTSD) were assessed using validated self-report instruments. Analyses included descriptive statistics, Pearson’s chi-square tests, two-way analysis of covariance (ANCOVA), and multivariate linear regression.
Results
Participants’ mean (SD) age was 21.2 (2.0) years; 53% identified as women, and 81% lived in urban areas. Prevalence was highest for psychological distress (57.0%), followed by depression (31.6%), anxiety (23.7%), and PTSD symptoms (12.6%). Women reported higher anxiety and distress than men (p < 0.05). In multivariable analyses, female gender, non-essential worker status, poorer self-rated mental health, weaker community belonging, lower household income, lower life satisfaction, and pre-existing mental health disorder were associated with greater symptom severity (p < 0.05).
Conclusion
The rising prevalence of mental health symptoms reflects gendered, socioeconomic, and psychosocial vulnerabilities, requiring trauma-informed clinical screening and equity-focused public health interventions for Canadian youth.
Plain Language Summary
Before the COVID-19 pandemic, approximately one in five Canadian youth experienced mental health symptoms annually, with limited access to appropriate care; only 20% received the help they needed. Hospitalization rates for mental health conditions were also increasing, signaling a growing public health concern. This cross-sectional study examines the prevalence and sociodemographic correlates of mental health symptoms among Canadian youth aged 18 to 24 during the COVID-19 pandemic. Using national survey data, we found that about 60% of respondents met the screening criteria for at least one mental health disorder, indicating a significant rise compared with pre-pandemic levels. Psychological distress was the most common condition, followed by symptoms of anxiety and depression. The findings revealed that women and youth experiencing socioeconomic or psychosocial disadvantages were disproportionately affected, reflecting intersecting vulnerabilities that compound mental health risks. In contrast, essential workers reported lower psychological distress levels, possibly due to heightened health awareness, stronger coping mechanisms, and a sense of social purpose linked to their occupational roles. These results underscore the urgent need for targeted mental health interventions, particularly for socioeconomically disadvantaged groups and young women. Strengthening accessibility, affordability, and inclusiveness of mental health services could mitigate long-term adverse outcomes. Moreover, identifying the youth demography at most risk may guide the development of community-based preventive and support strategies to enhance youth mental well-being during future public health crises.
Introduction
For over three decades, mental health has remained a pressing concern among Canadian children and youth. National statistics estimate that nearly one in five young people meet the criteria for at least one mental health disorder each year (Statistics Canada, 2021a; Vaillancourt et al., 2021). The COVID-19 pandemic, by disrupting education, employment, and social connections, has intensified these challenges (Bulloch et al., 2021; Capaldi et al., 2022). Emerging reports document sharp increases in depression, anxiety, psychological distress, and post-traumatic stress disorder (PTSD) among young adults during this period (Craig et al., 2022; Gill et al., 2022; Hawke et al., 2020).
Although the literature consistently signals rising rates of psychological symptoms, the majority of Canadian studies have methodological limitations. Several relied on a small sample (Gill et al., 2022), convenience sampling (Craig et al., 2022), was confined to a single university setting (King et al., 2022), or were restricted to particular provinces (Hawke et al., 2020; Salmon et al., 2022). Even when larger samples were included, analyses rarely extended to the sociodemographic correlates of mental health or the ways in which these factors intersect (Gill et al., 2022). This leaves a limited understanding of how gender, income, race, Indigeneity, and other social factors interact to shape youth mental health during crisis periods. A nationwide estimate that integrates these dimensions is therefore essential.
Youths represent a particularly vulnerable group during health crises (McGorry et al., 2025); they face major transitions, completing education, entering the workforce, and establishing independence, while often lacking stable financial and social resources (Ludwig-Walz et al., 2023; Vaillancourt et al., 2021). During the pandemic, these vulnerabilities were exacerbated by school closures, job losses, and disruptions to peer and community networks (Hawke et al., 2020). Our previous study showed a significant effect of the pandemic’s social and economic disruptions on the youth mental health symptoms (Onyeso et al., 2025). The consequences are wide-ranging, including heightened risks of substance use, sleep disturbances, cognitive impairment, family conflict, and suicidal ideation (Bourmistrova et al., 2022; Guerrero & Barnes, 2022; Premraj et al., 2022). Importantly, stigma around mental illness continues to deter youth from seeking help, contributing to unmet need and long-term negative outcomes (Xiong et al., 2020).
Mental health challenges are not evenly distributed. Pre-pandemic research shows that women, youth from low-income households, and racialized or immigrant populations report higher rates of distress (Findlay et al., 2020; Mental Health Commission of Canada, 2021). Yet little is known about how these vulnerabilities compounded during the pandemic, or whether structural inequalities such as gender and place of residence interact to magnify risk (Capaldi et al., 2022; Salmon et al., 2022). International reviews emphasize that young adults should be prioritized in recovery planning and explicitly considered in strategies for future public health emergencies (Newlove-Delgado et al., 2023). To do so, research must move beyond documenting prevalence to examining how sociodemographic factors shape outcomes and create overlapping vulnerabilities.
This study is grounded in the Social Determinants of Health (SDH) framework (World Health Organization, 2022), which emphasizes that health outcomes are shaped not only by individual behaviours but by broader social, economic, and environmental conditions. For youth, determinants such as income security, education, employment, housing, and social belonging are particularly salient. The pandemic highlighted how disruptions in these domains, such as reduced work hours, remote learning challenges, and weakened community ties, exposed young adults to increased mental health risks (Onyeso et al., 2025; Yu et al., 2021). Applying the SDH framework allows us to interpret prevalence not merely as an epidemiological measure, but as the outcome of structural inequities. This lens underscores the need to identify which youth populations are most disadvantaged and to inform policies that reduce barriers to mental health and social supports.
Building on these gaps and guided by the SDH framework, the present study aims to: (1) estimate the prevalence of four mental health symptoms; anxiety, depression, psychological distress, and PTSD among Canadian young adults aged 18 to 24 during the COVID-19 pandemic, (2) examine the influence of sociodemographic characteristics, including gender, education, area of residence, indigeneity, visible minority status, immigration status, household income, community belonging, and self-rated health, and (3) explore whether intersectional effects, particularly between gender and area of residence, further explain variations in mental health symptoms.
By offering a nationwide analysis of mental health symptom prevalence and sociodemographic correlates, this study extends the Canadian evidence base in several ways. First, it overcomes limitations of earlier pandemic research by drawing on Statistics Canada’s Survey on COVID-19 and Mental Health, a large-scale dataset with robust methodology. Second, it provides an intersectional analysis, highlighting how overlapping vulnerabilities shape risk. Finally, it translates findings into actionable insights for policy, particularly the importance of gender-stratified and equity-focused approaches in post-pandemic public health surveillance. Hence, the study contributes to both scholarly debates and practical efforts to support the well-being of Canadian youth.
Methods
Data Source
The study was a secondary data analysis using Statistics Canada’s Survey on COVID-19 and Mental Health (SCMH) datasets (2020 and 2021) (Statistics Canada, 2023). The SCMH was a cross-sectional, national rapid-response survey to assess the impacts of COVID-19 on Canadians’ mental health and well-being (Statistics Canada, 2023). The SCMH employed a simple random two-stage sampling design: the sampling unit for the first stage was the dwelling within each province, and the second stage was the persons within a dwelling (Statistics Canada, 2023). Statistics Canada obtained informed consent from the participants and was responsible for the research procedures and ethics.
The present study pooled the two cycles of SCMH collected in the fall of 2020 (n = 14,689) and spring of 2021 (n = 8,032) (Guerrero & Barnes, 2022). The survey was administered online or by telephone. Aside from marital status, which was not collected in 2020, the questions, variables, mode of administration, and the study population were the same for both cycles. Therefore, the pooled dataset met all five assumptions of comparability: same study population, sampling technique, instrument, outcomes, and context (Schenker & Raghunathan, 2007), and Thomas and Wannell (2009) guidelines for pooling similar Statistics Canada datasets. SCMH involved individuals aged 18 years and older from all provinces and territories in Canada, excluding people living on federal reserves, in institutions and outside the capital cities in the territories. The study involved young adults aged 18 to 24 years. After rigorous data cleaning, including removing univariate and multivariate outliers based on the primary outcomes, the study involved 896 participants.
Patient and Public Involvement
Our study involved a secondary analysis of the Statistics Canada Mental Health (SCMH) survey data for 2020 and 2021. Statistics Canada promotes public involvement in their survey designs by establishing multi-stakeholder steering committees during the development phase of their surveys. For this research, the study proposal was shared internally with academic colleagues for feedback during the development and review stages. Interpretation of findings was informed by scholarly discussion and peer feedback, including presentations at relevant academic conferences. This engagement process allowed us to ensure that our research was in tune with community interests and that the results were communicated in an effective manner.
Outcome Variables
The SCMH used standardized screening tools to assess symptoms associated with anxiety, psychological distress, depression, and post-traumatic stress disorder (PTSD) (Statistics Canada, 2021b). Anxiety was assessed using the Generalized Anxiety Disorder Scale (GAD-7) (Spitzer et al., 2006). The GAD-7 is a seven-item questionnaire that evaluates the presence and severity of generalized anxiety disorder. Items were rated on a four-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). The responses were summed to provide a score ranging from 0 to 21, with higher scores indicating greater anxiety levels. A score of 10 or higher represented the cut-off point for identifying cases of generalized anxiety disorder (Guerrero & Barnes, 2022; Spitzer et al., 2006).
Psychological distress was assessed using the ten-item Kessler Psychological Distress Scale (K10) (Kessler et al., 2003). The scale obtained respondents’ self-rating of their psychological distress symptoms in the previous four weeks based on a five-point Likert scale ranging from 0 (none of the time) to 4 (all of the time). The expected range was 0 to 40, with higher scores indicating greater levels of psychological distress (Cornelius et al., 2013). Nine (9) was adopted as a cut-off mark previously used in the Canadian context (Caron & Liu, 2010; Guerrero & Barnes, 2022).
Depressive symptoms were assessed using the nine-item Patient Health Questionnaire (PHQ-9) (Kroenke et al., 2001; Manea et al., 2012). The PHQ-9 assesses the frequency with which nine depressive symptoms have occurred in the past two weeks on a four-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). Respondents’ overall scores range from 0 to 27, with higher scores indicating more severe depressive symptoms. A score of 10 was the cut-off point for identifying cases of major depressive disorder (Kroenke et al., 2001; Manea et al., 2012). The PTSD was assessed using the 20-item self-report PTSD checklist (PCL-5), a derivative of the Diagnostic and Statistical Manual of Mental Disorders Version 5 (Roberts et al., 2021). The PCL-5 is a five-point Likert scale (0 = not at all, 4 = extremely) describing an individual’s traumatic experiences. The total score can range from 0 to 80. Thirty-three (33) was adopted as the cut-off point following the recommendations in the literature (Bovin et al., 2016).
Covariates
Following an in-depth literature review, 16 covariates were included in the models: age, gender, level of education, area of residence, immigration status, indigenous identity, visible minority identity, COVID-19 locus, sense of belonging to the local community, history of access to mental and emotional health resources, perceived mental health, mental health status compared to before COVID-19, being an essential health worker, household size, total household income (THI), satisfaction with life in general, and region of residence. An essential worker is an individual who works in a service, facility or activity necessary for the preservation of life, health, public safety, or basic societal functions (Guerrero & Barnes, 2022). Satisfaction with life in general was self-reported on a scale from 1 to 10, with higher scores indicating greater satisfaction.
The COVID-19 locus was a derived variable measuring a participant’s level of social connectedness with people diagnosed with COVID-19 infection. COVID-19 locus was a dichotomous variable defined as “proximal” if the participant or any household member was diagnosed with COVID-19 or “distal” if the participant’s close friend or family member outside the household, a coworker or colleague, or someone else interacted with in the community was diagnosed with COVID-19. This variable aligns with the socioecological framework for mental health (Michaels et al., 2022), allowing us to explore how proximal and distal pandemic-related exposures may differentially influence youth mental health outcomes.
Statistical Analysis
Data was analyzed using the Statistical Package for Social Sciences (SPSS) Version 28. Descriptive statistics – frequency (percentage) and mean (standard deviation) were used to summarize the participants’ characteristics. The primary outcome variables were dichotomized to facilitate prevalence and crosstabulation analysis. However, continuous outcome variables were used for multivariate regression analysis to avoid the loss of statistical power and inflation of residual confounding inherent in dichotomizing a continuous variable for multivariate analyses (Royston et al., 2006).
The dataset was diagnosed and fixed for univariate and multivariate outliers using the standardized Z-score and Mahalanobis distance approaches. Each mental health outcome was assessed for normality by computing its skewness, linearity was established through a QQ plot, and multicollinearity in each regression model was assessed and adjusted using the variance inflation factor (VIF <5).
Pearson’s Chi-square was used to test the association between mental health indicators and sociodemographic characteristics. A two-way analysis of covariance (ANCOVA) was used to estimate the main and interaction effects of gender and area of residence on the mental health indicators while adjusting for the covariates. Finally, multivariate linear regression models were used to determine the sociodemographic factors that could predict the mental health indicators.
Results
Sociodemographic Characteristics
Sample Sociodemographic Characteristics
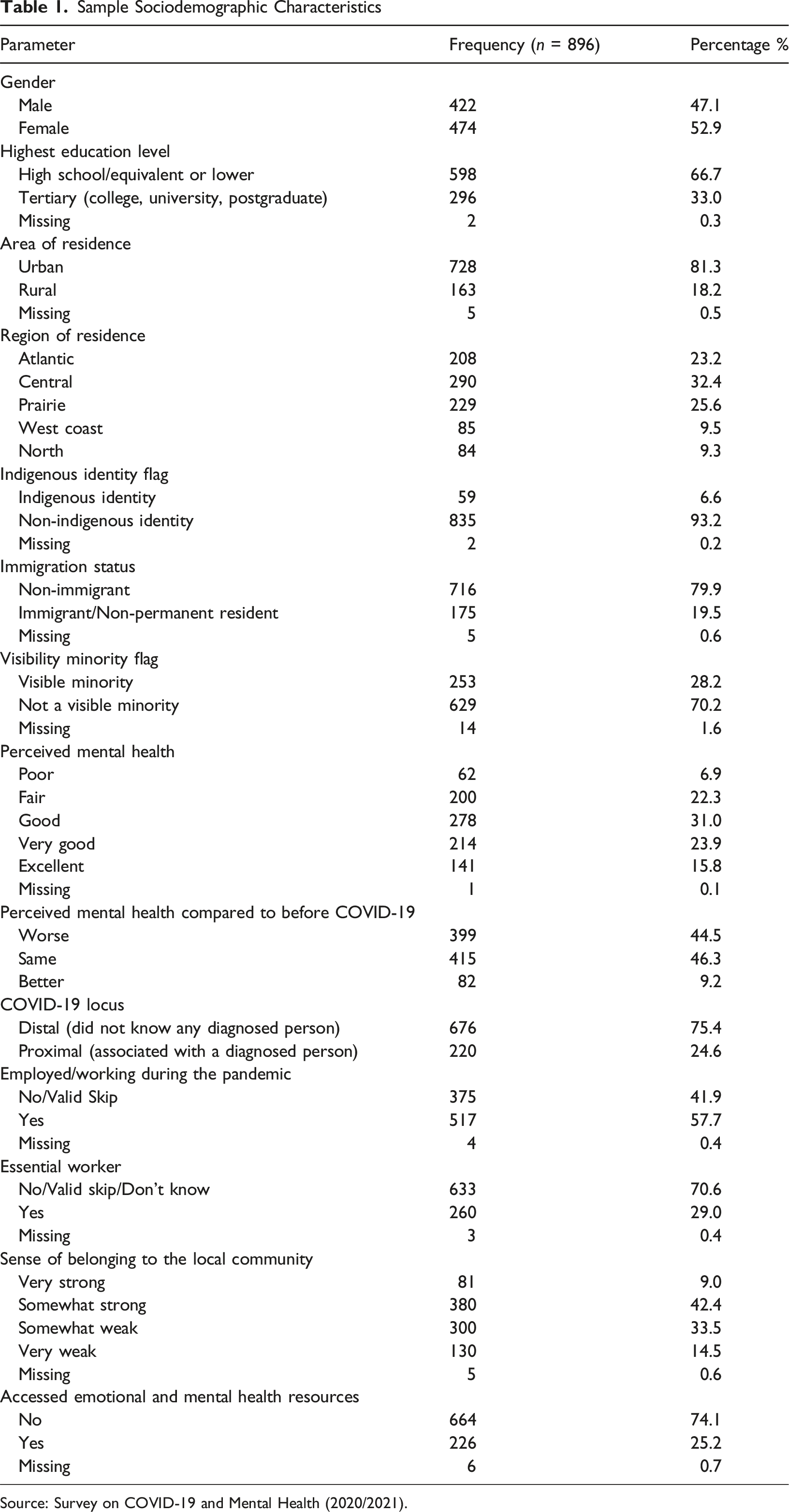
Source: Survey on COVID-19 and Mental Health (2020/2021).
Prevalence of Mental Health Symptoms
Mental Health Profile of the Participants (Based on Standardized Cut-Off)
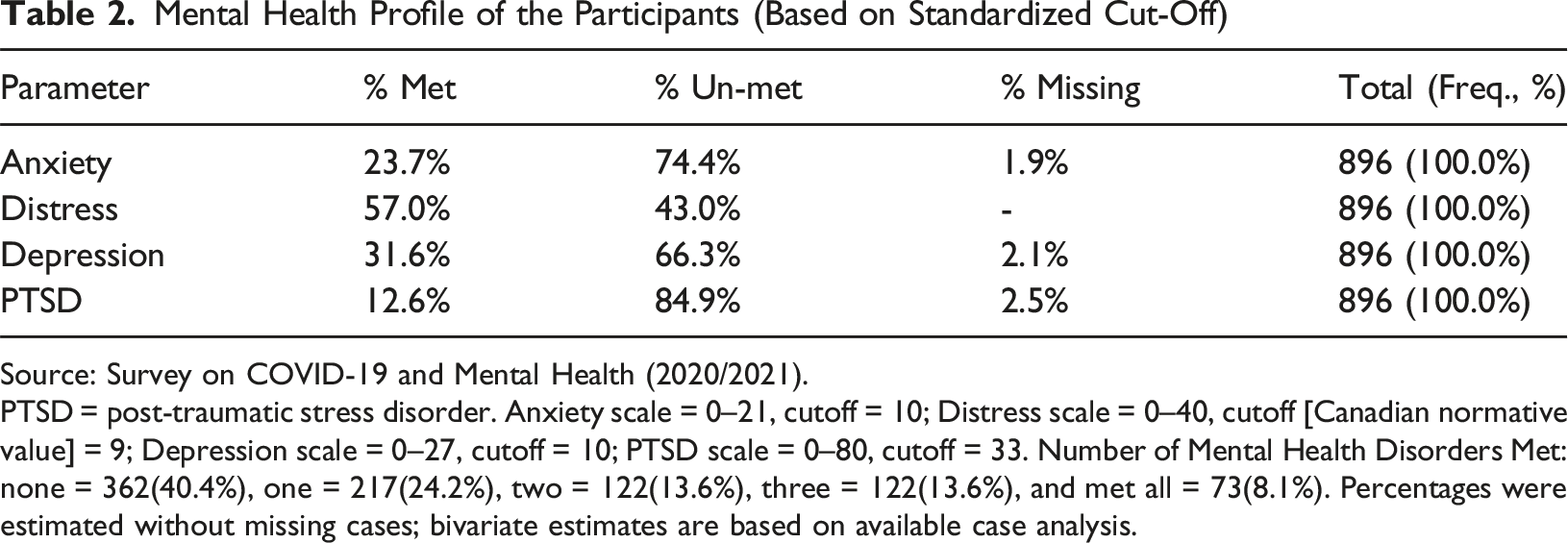
Source: Survey on COVID-19 and Mental Health (2020/2021).
PTSD = post-traumatic stress disorder. Anxiety scale = 0–21, cutoff = 10; Distress scale = 0–40, cutoff [Canadian normative value] = 9; Depression scale = 0–27, cutoff = 10; PTSD scale = 0–80, cutoff = 33. Number of Mental Health Disorders Met: none = 362(40.4%), one = 217(24.2%), two = 122(13.6%), three = 122(13.6%), and met all = 73(8.1%). Percentages were estimated without missing cases; bivariate estimates are based on available case analysis.
Association Between Demographic Variables and Mental Health Symptoms
Bivariate Association Between Sociodemographic Variables and Mental Health Outcomes
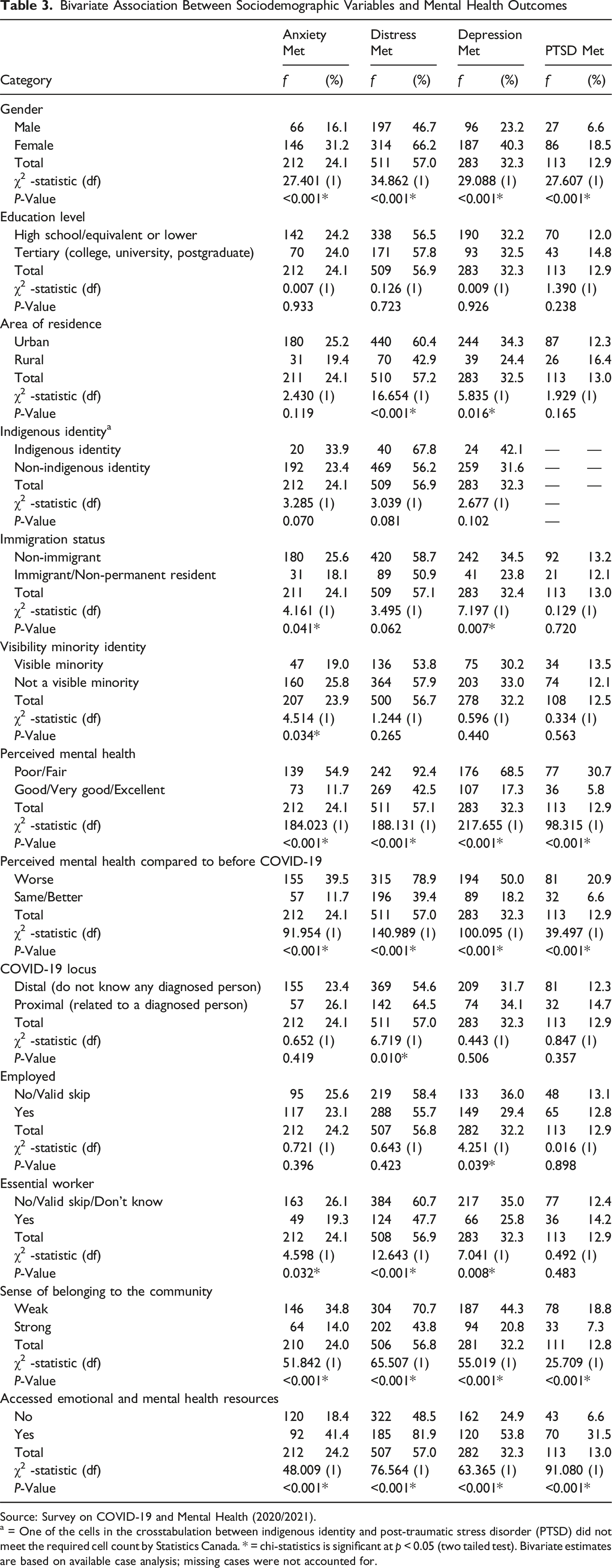
Source: Survey on COVID-19 and Mental Health (2020/2021).
a = One of the cells in the crosstabulation between indigenous identity and post-traumatic stress disorder (PTSD) did not meet the required cell count by Statistics Canada. * = chi-statistics is significant at p < 0.05 (two tailed test). Bivariate estimates are based on available case analysis; missing cases were not accounted for.
Multivariate Analysis
Two-Way ANCOVA for Gender and Area of Residence Effects on Mental Health Outcomes
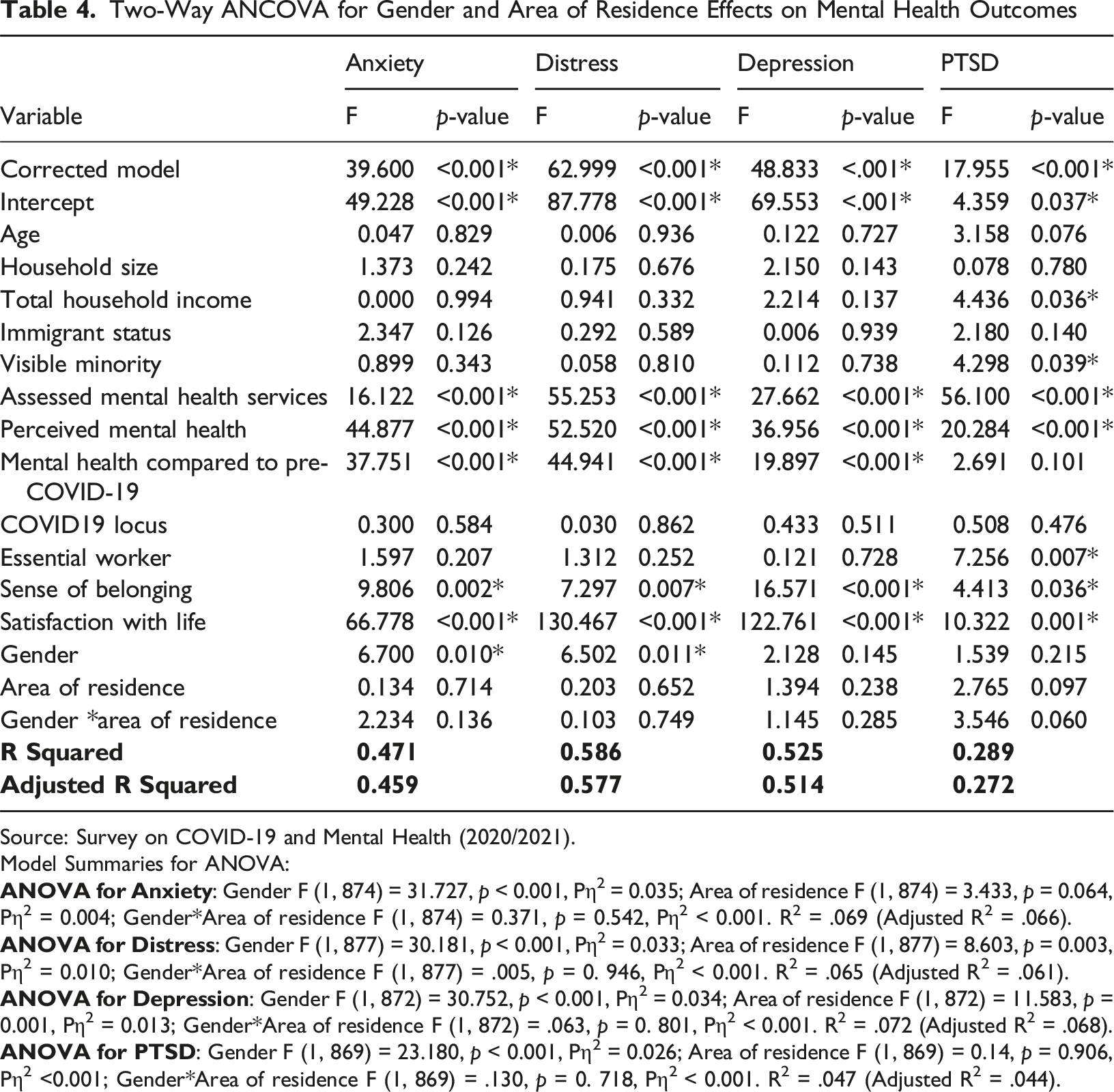
Source: Survey on COVID-19 and Mental Health (2020/2021).
Model Summaries for ANOVA:
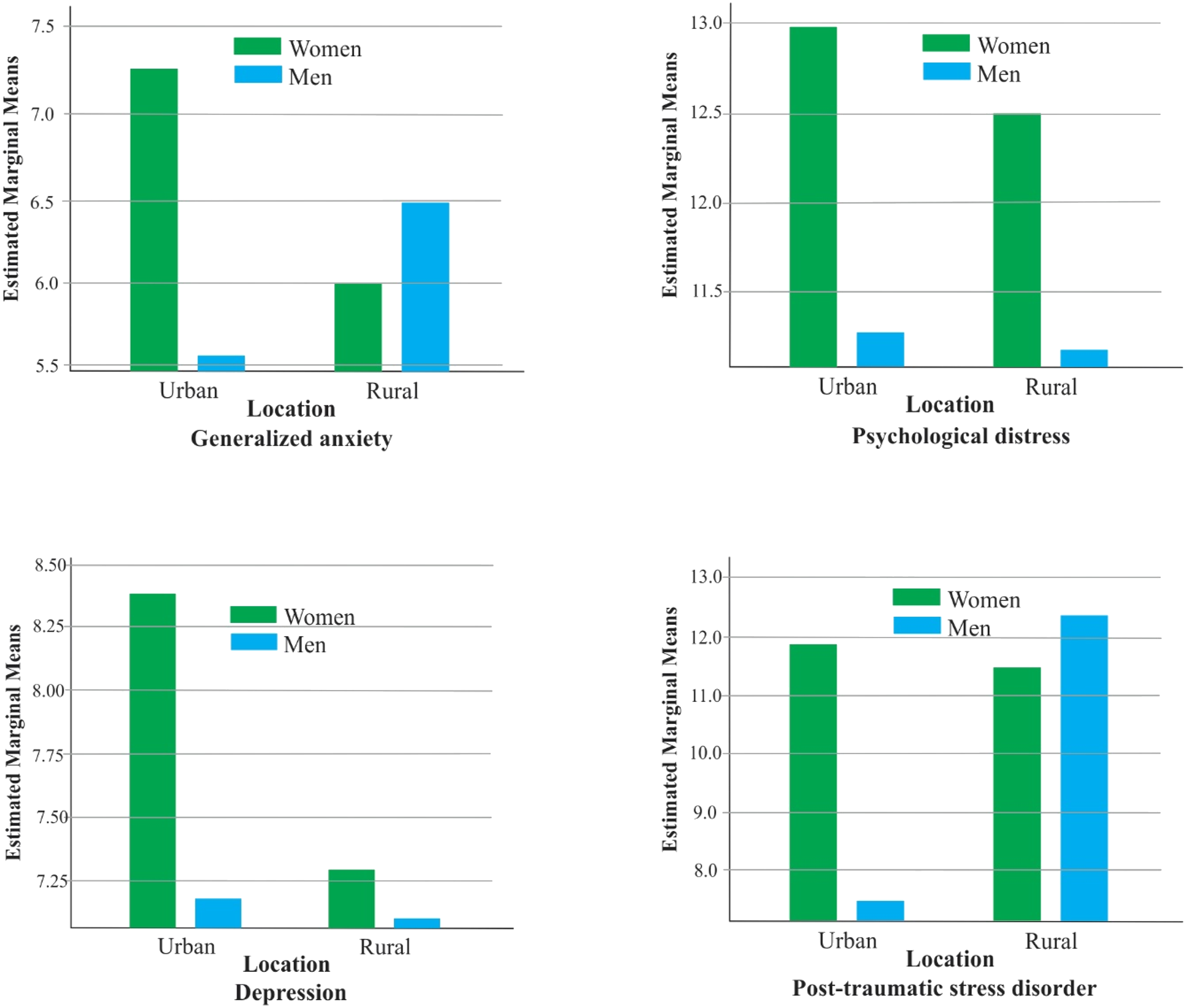
Two-way ANCOVA, estimated marginal means of the interaction effects of gender and area of residence on mental health outcomes.
Multivariate Linear Regression for Sociodemographic Predictors of the Mental Health Outcomes
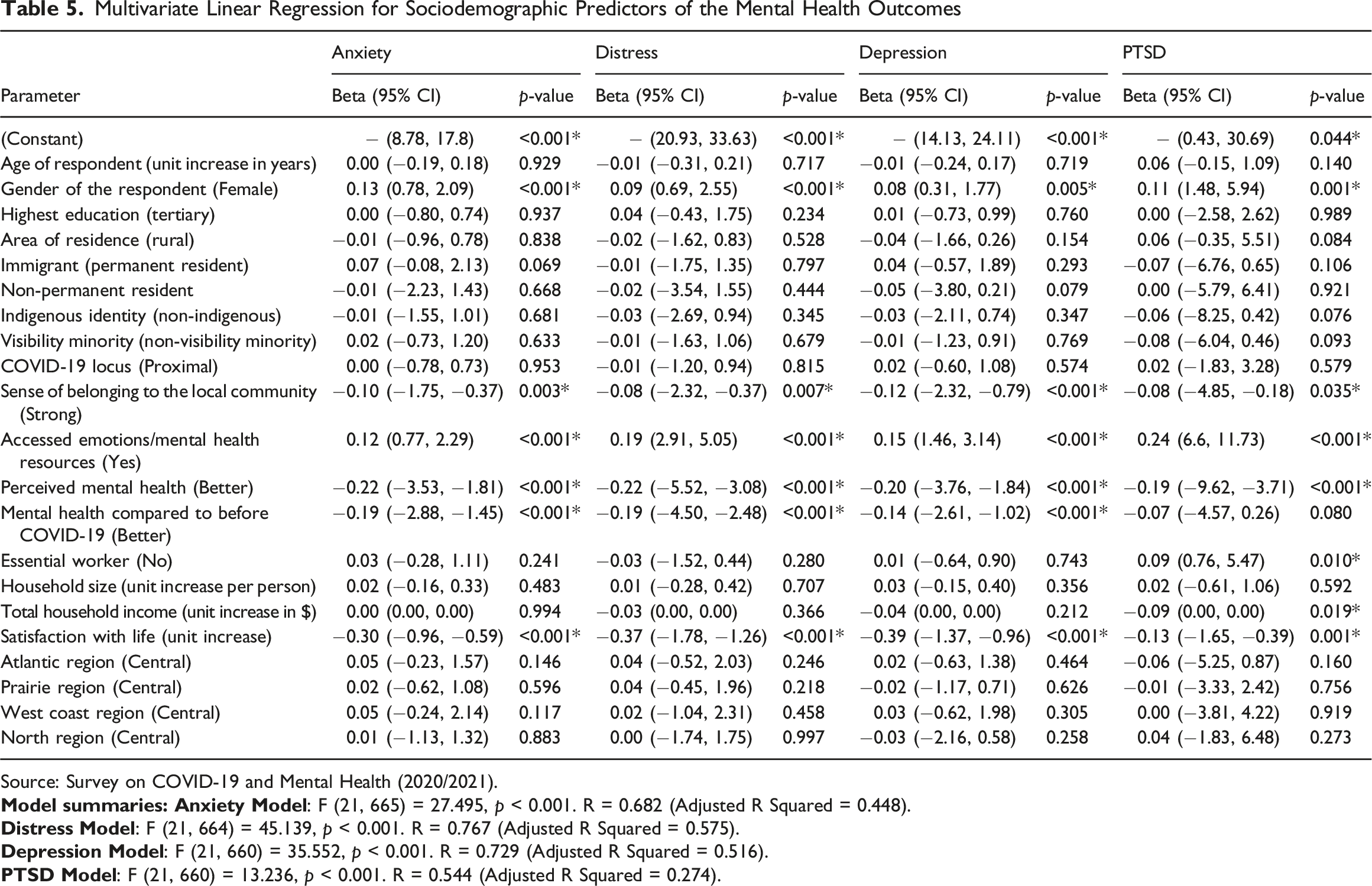
Source: Survey on COVID-19 and Mental Health (2020/2021).
Predictors for psychological distress and depression were the same factors as in anxiety; Table 5 showed the effect estimates. The model (F [21, 665] = 27.495, p < 0.001) accounted for 57.5% of the total variance in psychological distress. Similarly, the model summary for depression explained 51.6% of the total variance (F [21, 660] = 35.552, p < 0.001).
Table 5 showed that all the predictors of anxiety, psychological distress, and depression, including being an essential worker during the pandemic (β = 0.09, p = 0.010) and a unit decrease in household income (β = −0.90, p = 0.019), were significant predictors of PTSD. The model explained 27.4% of the total variance (F [21, 660] = 13.236, p < 0.001).
Discussion
The study examined the prevalence and sociodemographic correlates of mental health symptoms among Canadian youth aged 18 to 24 years, focusing on the effect of gender and area of residence and their intersectionality on mental health outcomes. In the early stage of the pandemic, global research interest focused on mortality among older adults who were more vulnerable to COVID-19 (Findlay et al., 2020; Pérès et al., 2021). Beyond mortality, interests have shifted to the pandemic’s indirect effects, such as the rising prevalence of mental health disorders globally (Bourmistrova et al., 2022). The present study concurred with Gill et al. (2022), who reported that 60.1% of Canadian youths (18 to 24 years) meet the criteria for at least one of psychological distress, depression, anxiety, or PTSD. The result showed that 59.6% of the sample met at least one of these four symptoms. The pre-pandemic prevalence of mental health disorders among Canadian youths was of national concern (Statistics Canada, 2021a; Vaillancourt et al., 2021). Emerging data have shown a worsening trend following the pandemic (Bulloch et al., 2021; McGorry et al., 2025).
The discussion focused on the results of the multivariate-adjusted models. The ANCOVA models showed that females reported significantly higher anxiety and distress symptoms than their male counterparts. Virtually all the Canadian mental health studies of adolescents and youths supported the findings that mental health symptoms were more prevalent among women (Capaldi et al., 2022; Craig et al., 2022; Findlay et al., 2020; Salmon et al., 2022). It was expected that the impact of COVID-19 would be felt more by rural women (Mental Health Commission of Canada, 2021; Moffitt et al., 2022). Moffitt et al. (2022) suggested that rural women will be more vulnerable to the mental health impact of COVID-19 due to increased home violence, job loss, family chores, and childrearing responsibilities. Similarly, the Mental Health Commission of Canada (2021) posited that the unique influence of the social determinants of health in rural and remote communities makes the rural dwellers more vulnerable to the mental health impacts of COVID-19, as well as a lack of access to adequate and timely services and support. However, the estimated marginal means showed that rural residents had milder symptoms, especially for psychological distress and depression. This finding aligns with Capaldi et al. (2022), which showed that many people in rural areas reported better or stable mental health in 2020 and 2021 compared with urban dwellers. Whether facilitated by social supports, family, or a reduced prevalence of COVID-19 itself, there may have been a “rural advantage” for youths during this period. Another study among older adults found that people living in rural areas during COVID-19 experienced better social support, greater family presence, and fewer depressive and anxiety symptoms (Pérès et al., 2021). All the inferential statistics completed in the present study showed that gender was the primary sociodemographic correlate of mental health outcomes during the pandemic. Women had higher levels of anxiety, physiological distress, depression, and PTSD, especially in urban areas. The gendered finding aligned with other COVID-19 literature on Canadian youth reporting significantly higher prevalence of mental health disorders among women (Capaldi et al., 2022; Craig et al., 2022; Findlay et al., 2020; Salmon et al., 2022).
Aside from gender, the multivariate regression models showed other predictors of mental health symptoms, including being an essential worker, total household income, and psychosocial factors, such as a sense of belonging to the local community, mental health status before COVID-19, adverse change in mental health due to the pandemic, and satisfaction with life. Contrary to the assumption that essential workers would experience more mental health symptoms (Warren et al., 2021), essential workers and people from higher-income households reported less PTSD. The finding is congruent with other studies reporting that essential workers suffered less PTSD than the general population (Gill et al., 2022; Warren et al., 2021). Essential workers are in tune with their role expectations (Wang & Tang, 2020). While their workload and risk of infection increased, the perceived importance of their work, devotion to service, altruism, and heroism may have mitigated the adverse psychological effects (Wang & Tang, 2020). In line with other Canadian literature, this study found household income to be a significant predictor of young adults’ mental health (Salmon et al., 2022; Yu et al., 2021). Youths in low-income households may experience disproportionate traumatic health, social, and economic disturbances during the pandemic and have reduced access to mental health resources (Vaillancourt et al., 2021). Low-income households have been associated with an elevated risk for PTSD (Statistics Canada, 2024b), because economic disadvantage increases exposure to trauma, reduces access to protective and recovery resources, and contributes to chronic stress that heightens vulnerability to post-traumatic symptoms (Vaillancourt et al., 2021).
Psychosocial vulnerabilities are a determinant of mental health outcomes (Caron & Liu, 2010; Pérès et al., 2021). The present study has shown some sociodemographic and psychosocial factors relevant to post-pandemic surveillance. A weak community sense of belonging and decreased satisfaction with life (in general) negatively impacted all the mental health symptoms. Canadian young adults’ mental health was adversely affected by COVID-19-related social dynamics that impacted their interpersonal relationships, community cohesion, and ways of living (Gill et al., 2022; Hawke et al., 2020; Vaillancourt et al., 2021). Self-report of pre-existing mental health disorders, being enrolled in a mental health intervention before the pandemic, and perception of worsened mental health due to the pandemic were predictors of poor mental health. These findings agreed with Hawke et al. (2020), who reported a significant deterioration of mental health among Canadian youths in Ontario who had mental health illnesses before the COVID-19 pandemic. Similarly, Canadian studies have demonstrated that stronger community belonging is associated with higher life satisfaction and better mental health among youth, including those aged 15–29 (Foran, 2025) and 18–34 (Capaldi et al., 2022). However, our study specifically focused on youths aged 18–24.
Beyond the variables included in the present analysis, several pandemic-related contextual factors may further explain the elevated mental health symptoms observed among Canadian youth. Restrictions on outdoor physical activity and in-person social interaction, along with the resulting increase in digital engagement and screen time, have been consistently linked to higher levels of anxiety, depressive symptoms, sleep disturbances, and emotional dysregulation among adolescents and young adults (Chen et al., 2022; Santos et al., 2023). Prolonged reliance on online schooling and remote work has also been linked to cognitive overload, reduced academic structure, and heightened stress, especially among youth with limited access to supportive learning environments (Vaillancourt et al., 2021). In addition, a prior study on this cohort showed that social disruptions, including the death of a family member, friend, or colleague, feelings of loneliness, social isolation, emotional distress, and restrictions in personal relationships, negatively affected youth mental health during the pandemic (Onyeso et al., 2025). Although these factors were not directly measured in the present study, they likely served as salient contextual stressors and potential confounders during the pandemic, warranting explicit consideration in both clinical assessment and future research.
The exclusion of youth living on reserves and certain territories governed by distinct data-collection frameworks (The First Nations Information Governance Centre, 2019) may have resulted in conservative prevalence estimates or obscured some structural inequities affecting mental health outcomes. In our adjusted model, Indigenous youth showed higher levels of PTSD, while no statistically significant difference was observed in other mental health symptoms. Similarly, there was no significant association between youth mental health symptoms and immigration or minority status. This contrasts with broader Canadian evidence showing disproportionately higher rates of mental health disorders among Indigenous people, immigrants, and racialized adults, driven by structural inequities, historical and intergenerational trauma, systemic racism, and limited access to culturally safe services (Statistics Canada, 2024a). Our findings for immigrants and visible minority youth may differ from patterns typically observed in adults due to the characteristics of this cohort, namely its youth-specific composition (18–24 years), predominantly urban residence, and the rapid rise in mental health symptoms across the population during the pandemic, which may have reduced the ability to detect disparities at the population level. Nonetheless, inclusive surveillance systems and targeted research that centre the experiences of marginalized youth remain essential.
This study has some clinical and public health implications. The results support other studies that reported rising prevalence of mental health symptoms among Canadian youths (Bulloch et al., 2021; Findlay et al., 2020; Hawke et al., 2020; Li et al., 2023; Vaillancourt et al., 2021). From a clinical perspective, the observed associations point to intersecting risk pathways in which gender, socioeconomic disadvantage, pre-existing mental health conditions, and weakened community social cohesion increase vulnerability through cumulative stress exposure and reduced access to protective resources. At the same time, comparatively milder symptom profiles observed in some groups suggest the presence of resilience-promoting factors, including social support and economic stability, underscoring the importance of trauma-aware, socially informed clinical assessment and formulation that consider both vulnerability and resilience processes. Clinical psychotherapy and psychosocial interventions that strengthen coping capacity, social connectedness, and functional recovery may therefore play a key role in reducing symptom severity and supporting mental health among Canadian young adults.
From a public health perspective, surveillance efforts should prioritize urban-dwelling young women, individuals from lower-income households, and youth with prior mental health diagnoses or psychosocial disadvantage. The findings suggest a disproportionate concentration of mental health burden among young adults in urban settings, highlighting the need for targeted monitoring and intervention strategies. Community-based social interventions that enhance emotional support, foster positive relationships, and strengthen social cohesion should be integrated into public health responses. Consistent with the recommendations of Salmon et al. (2022), pandemic relief resources should be explicitly directed towards families and young adults at higher risk, such as families with young women and low-income households.
Strengths and Limitations
The current study involved a multivariate analysis of a large national sample collected by a reliable federal government agency (Statistics Canada). Beyond the zero-order association between mental health symptoms and sociodemographic factors, the interaction effects were explored, while confounders were controlled within multivariate models.
However, the study has some limitations, such as using self-reported screening tools in lieu of clinical diagnosis of mental health disorders. Standardized self-reported screening tools assume a minimum level of health literacy; therefore, the quality of data obtained from youths may be influenced by variations in their literacy levels. Nonetheless, the instruments used in the study were screening tools whose reliability and validity are well-established, but the outcome should not be misconstrued as a clinical diagnosis. However, screening results are helpful for surveillance of population-based prevalence and justification for further clinical assessment and probable diagnosis of individuals. Although all Canadian provinces and territories were part of the survey, people living in federal reserves, institutions, and outside the capital cities in the territories were excluded from the survey due to a distinct data collection legislative framework and governance. Hence, the report was based on the analyzed samples and may not be generalizable to the entire Canadian population.
Conclusion
There was a high prevalence of anxiety, psychological distress, depression, and PTSD symptoms among Canadian young adults during the COVID-19 pandemic. Mental health problems appeared to be higher among urban dwellers and females, irrespective of their locality. Essential workers reported less PTSD than non-essential workers and unemployed people during the pandemic. Being from a low-income household was a significant predictor of PTSD. Psychological determinants, such as low community sense of belonging and poor satisfaction with life, were associated with higher anxiety, psychological distress, depression, and PTSD scores. People with mental health problems before COVID-19 were significantly more affected than their counterparts. This study alerts the public health authorities to the impending post-pandemic rise in the prevalence of mental health disorders among Canadian young adults and vulnerable sub-populations. Interventions that enhance social connectedness, address socioeconomic stressors, and support adaptive coping may be particularly critical in mitigating long-term mental health consequences for youth exposed to large-scale public health crises. Screening and counseling services that are culturally safe and trauma-informed could be offered in schools and recreation centers, making them more accessible to youth.
Footnotes
Acknowledgement
This research was supported by funds to the Canadian Research Data Centre Network (CRDCN) from the Social Science and Humanities Research Council (SSHRC), the Canadian Institute for Health Research (CIHR), the Canadian Foundation for Innovation (CFI), and Statistics Canada. Although the research and analysis are based on data from Statistics Canada, the opinions expressed do not represent the views of Statistics Canada. The authors acknowledge the Statistics Canada staff at the Research Data Centre (RDC), University of Lethbridge and University of Calgary, who vetted the statistical outputs, and Carly Heck, who completed the editorial revision of the manuscript.
Ethical Considerations
The study was a secondary data analysis of Statistics Canada’s Survey on COVID-19 and Mental Health. Statistics Canada obtained ethics approval and was responsible for the research procedure.
Consent to Participate
Statistics Canada obtained consent from the survey participants.
Author Contributions
O.K.O., A.B., M.K.I., and L.H. contributed to the conception of this study. L.H., M.K.I., and L.H. contributed substantially to the design and data acquisition. O.K.O. performed the statistical analysis. O.K.O. and A.B. were responsible for drafting the article. L.H. completed its critical revision. All authors approved the final manuscript for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funds to the Canadian Research Data Centre Network (CRDCN) and from the Prentice Institute for Global Population and Economy, University of Lethbridge. Open access publication was supported through the Canadian Research Knowledge Network (CRKN) open access agreement with SAGE Publishing.
Declaration of Conflicting Interests
The authors declare that they have no competing interests.