
Abstract
Aims:
Most lifetime mental health disorders begin by age 25 years, and the prevalence among young people has been increasing over recent years. We sought to understand what impact, if any, social determinants have had on this increase through the analysis of an Australian longitudinal dataset (with data from 2007 to 2021).
Methods:
The analysis focused on five social determinants: loneliness and lack of social support, family relationships, participation in education and employment, receipt of government benefits and relative socio-economic status. We analysed cross-sectional changes in self-reported psychological distress between 2007 and 2021 (using the Kessler-10 item; K10 scores) and examined the effects of these five social determinants on psychological distress using weighted linear regression models.
Results:
We identified a significant increase in psychological distress among Australians from 2007 to 2021, with the sharpest rise among those aged 15 to 25 years, who saw more than doubling in the percentage of high and very high K10. This period also saw an increase in the prevalence of social determinants such as loneliness and lack of social support, as well as poor family relationships, particularly in 2021 post COVID-19 pandemic. Regression models suggest loneliness and lack of social support had the most pronounced and increasing impact on psychological distress, followed by poor family relationships.
Discussion:
The observed significant and steady increases in psychological distress and related social determinant factors, particularly loneliness and lack of social support among young people, highlight the urgent need for comprehensive actions. Coordinated research and community-based initiatives are needed to deliver intrapersonal, interpersonal and socially-focused interventions with a holistic approach to support psychosocial wellbeing. Policymakers must adopt a comprehensive shift in political commitment and a whole-of-government approach to address these challenges.
Introduction
Most lifetime experiences of mental ill-health onset by the age of 25 years (Kessler et al., 2005; Solmi et al., 2021). Mental ill-health is the primary source of disease burden for young people between the ages of 15 and 25 years (Gore et al., 2011). The prevalence of mental ill-health in this demographic is on the rise – in Australia the proportion of young people reporting a 12-month mental disorder rose from 26.4% in 2007 to 38.8% in 2022 (Australian Bureau of Statistics, 2022). A worsening generational experience of mental health has been identified in Australian birth cohorts from the 1980s and 1990s (Botha et al., 2023), a trend not limited to Australia, with increases among young people evident globally (Castelpietra et al., 2022; Ford & Freund, 2022). Understanding the drivers of these increases is essential to shape more effective responses from a policy, service and care perspective.
Social determinants of health provide a framework for considering non-medical factors that influence health outcomes, including mental health. The need to address social determinants was recognised internationally in the WHO Commission on Social Determinants of Health, 2005 to 2008, as well as in the 2011 Rio Political Declaration on Social Determinants of Health (Commission on Social Determinants of Health, 2008; Working Group for Monitoring Action on the Social Determinants of Health, 2018). Social determinants include factors at the societal level as well as the individual level – for example, demographic, economic, neighbourhood, environmental events and social and cultural factors. They may be dynamic or fixed characteristics. Interactions between social determinants can result in greater impacts or influences on mental health (Kirkbride et al., 2024; Lund et al., 2018). Life course perspectives underline the significance of tackling social determinants of mental health and wellbeing during adolescence, acknowledging that experiences during one phase of life can impact subsequent life stages. Adolescence is a key period for the development of skills that assist in addressing social determinants in adulthood, as well as a period where vulnerability to mental ill-health as a consequence of the influence of social determinants is quite high (Fusar-Poli et al., 2021). A better understanding of the role and impact of social determinants can inform the development and delivery of early intervention programs and services that provide holistic support for young people’s mental health and wellbeing.
To understand the opportunities available for early intervention we have examined the impact of social determinants on people’s mental health in Australia. To do this we utilised data from the largest Australian longitudinal cohort study, the Household, Income and Labour Dynamics in Australia (HILDA) Survey. With data collected annually since 2001, we aimed to explore associations between social determinants and psychological distress, whether these have changed over time and the direction this might provide for early intervention.
Methods
Study design, data source and procedures
This study was a secondary data analysis of the HILDA Survey panel data, with variables selected to evaluate the mental health impact of different social determinants on people over time. The HILDA Survey, collected since 2001, is a household-based longitudinal panel study that collects data on economic and personal wellbeing, labour market dynamics and family life .
The original Wave 1 of data collection applied a multi-stage clustered stratified design, with data collected from 19,914 participants. Follow-up data was collected from the original households as well as children subsequently born to, or adopted by, the participating households. The cohort expanded in 2011, with additional top-up samples (~2,000 participants) added each year. Psychological distress, measured by the 10-item Kessler Psychological Distress Scale (K10; R. C Kessler et al., 2002), was collected every two years from 2007. At the time of writing, eight waves of data that included the K10 were available and used in the analysis, that is data between 2007 and 2021. Individuals aged 15 years and under were excluded due to limited available data collected.
Measures
Detailed information about the data collection methods, sampling techniques and survey items has been comprehensively described in the HILDA User Manual (Summerfield et al., 2021). Measures used in this analysis are described below.
Outcome variable – K10
Psychological distress (self-reported through a self-completion questionnaire) was measured using the K10 biennially. K10 is a 10-item scale measuring non-specific psychological distress, scored using a five-level response scale with total scores ranging from 10 to 50. Continuous K10 scores can be converted into four K10 psychological distress subgroups: low, moderate, high and very high (Andrews & Slade, 2001).
Exposure variables – Social determinants
To identify variables of interest, all data items from the HILDA survey were systematically mapped to factors related to the Australian Government’s wellbeing framework (Australian Government, 2023) and broader social determinants of health identified throughout the literature (Elias et al., 2019). These included variables that covered psychosocial stressors (e.g. homelessness, financial stressors, educational stressors, family issues) and social disadvantage (e.g. educational, income, stigma, discrimination, loneliness, isolation).
Five binary indices of social determinants were ultimately created: loneliness and lack of social support, poor family relationships, Not in Employment, Education or Training (NEET), receiving government benefits and living in low socioeconomic status (SES) areas. Loneliness and lack of social support were created based on the 10-item social support index (Scutella et al., 2009), with participants ranked in the lowest quartile (25%) being classified as exposed. Family relationship was based on self-reported satisfaction with parents or step-parents, ranging from completely dissatisfied (0) to completely satisfied (10). Scoring 5 or less was considered as having poor family relationship. NEET status was obtained by combining self-reported employment, education or training. Receiving government benefits was based on self-reported status of received income in the form of a benefit, pension or allowance. The 2021 Index of Relative Socio-Economic Advantage and Disadvantage (IRSAD) deciles (ABS, 2011) were used as the indicator of residential area SES. Deciles were recommended as a consistency measure over time due to variations in how IRSAD scores were estimated between different years (Australian Bureau of Statistics, 2021). People living in areas of the three lowest deciles of IRSAD were considered as living in low SES areas. All five variables were extracted as binary risk factors and were coded as ‘Yes’ when the risk factor was present. Details of the social determinant factors can be found in Supplemental Table S1.
Statistical analysis
Analyses were conducted using R version 4.2.2 (2022-10-31). The cohort was subdivided into four age groups: 15 to 25, 26 to 35, 36 to 65 and above 65 years. To address the study aims, we were primarily interested in the youngest age group (people aged 15–25 years), with other age groups utilised as comparators. To obtain an estimate most relevant to the Australian community at each time point, we conducted cross-sectional analyses using the self-completion questionnaire (SCQ) responding person weight (cross-section population weight rescaled to sum to the number of responding persons in the relevant wave) in all analyses.
Basic descriptive statistics
Simple descriptive statistics including age and sex were used to broadly explore the characteristics of the cohort and individual age groups for each year that the K10 was collected. Changes in social determinants and K10 scores over the years were explored for the entire cohort as well as for each age group using time series plots.
Regression models
Both univariate and multivariate weighted linear regression models were used to evaluate associations between the social determinant variable(s) and K10 scores, treating data collected at each time point as cross-sectional data. The univariate models estimated the relationships between each of the social determinant variables and the outcome (K10), while the multivariate model incorporated all social determinant variables concurrently. We ran the regression model for each year and each of the age groups as well as the whole cohort for comparison. Missing data were addressed using multiple imputation and pooled using Rubin’s rules (Rubin, 2004). Weighted linear regression models were built on 20 imputed datasets by chained random forest (using R function missRanger; Mayer, 2021).
Results
Cohort demographics
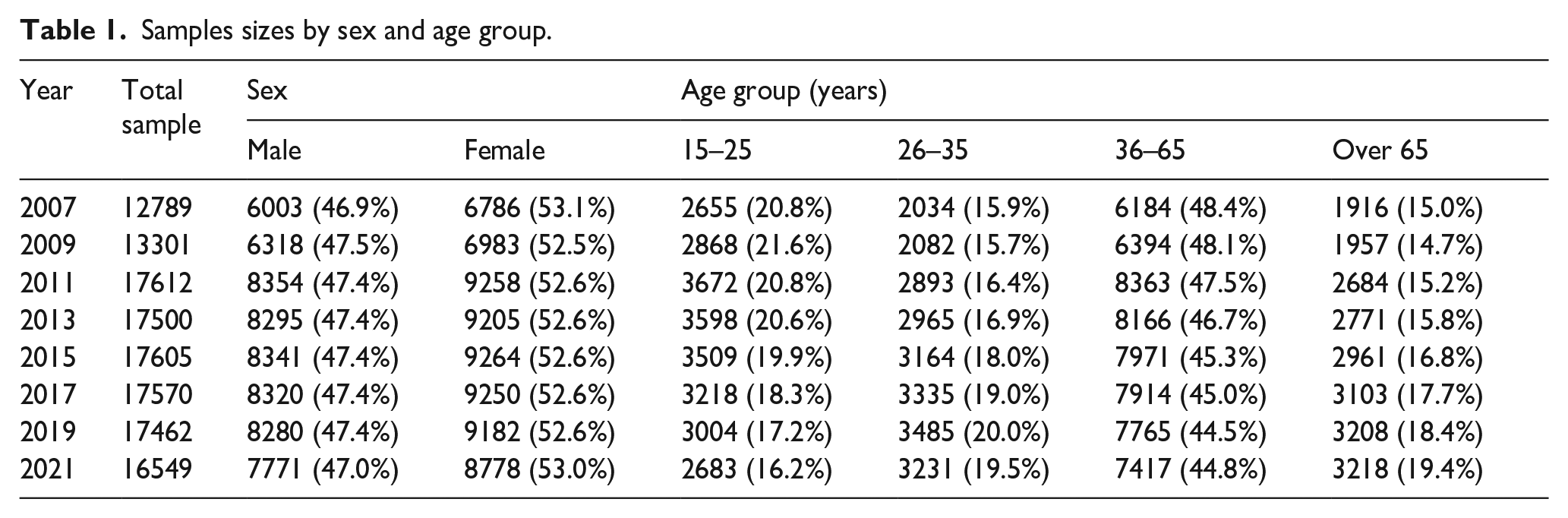
Sample sizes by sex and age group are shown in Table 1. When the HILDA survey first included the K10 in 2007, 12,789 people participated in the survey. The total number of participants increased substantially from 2011 (~17,000) due to the cohort expansion and decreased slightly to 16,549 in 2021. Consistently, ~53% of people reported their sex as female at each time-point. A slightly lower proportion of young people aged 15 to 25 years completed the survey in 2021 (16.2%) compared with other years (~20%).
Samples sizes by sex and age group.
K10 changes over time
Figure 1 shows the K10 distribution (categorical and continuous) for each cohort from 2007 to 2021. Over this period of time, there was a clear gradual increase in the percentage of people with high and very high K10 scores (16% in 2007 increasing to 26% in 2021, Figure 1a), as well as an upward shift in continuous K10 scores – median (IQR) = 14 (11–18) in 2007 to 16 (12–22) in 2021 (Figure 1b), especially in the year 2021.
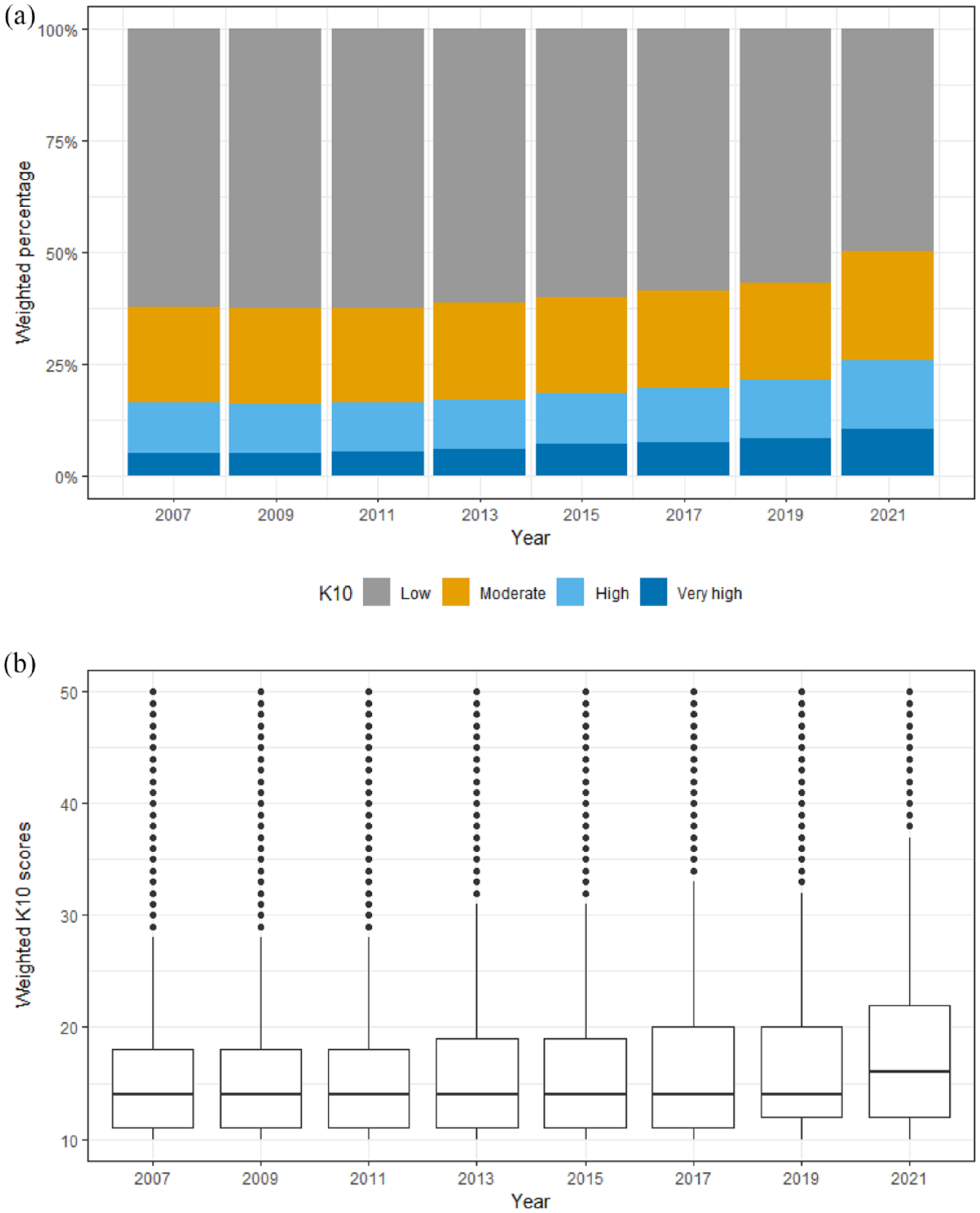
Changes in weighted percentage for K10 subgroups and weighted K10 scores from 2007 to 2021: (a) K10 subgroups and (b) K10 scores.
Dividing the cohorts by age groups, the increases in K10 scores were evident for the three younger age groups (15–25, 26–35 and 36–65 years), but not for those aged >65 years (Figure 2). Our age group of interest (15–25) had the most substantial increase, more than doubling in the percentage of high and very high K10 (from 20% in 2007 to 42% in 2021). The overall weighted K10 scores (the median (IQR) K10 score also increased, from 15 (12–20) in 2007 to 19 (14–27) in 2021). Since there was no substantial change in K10 for the older cohort, we excluded the >65 years age group from the age group specific analysis.
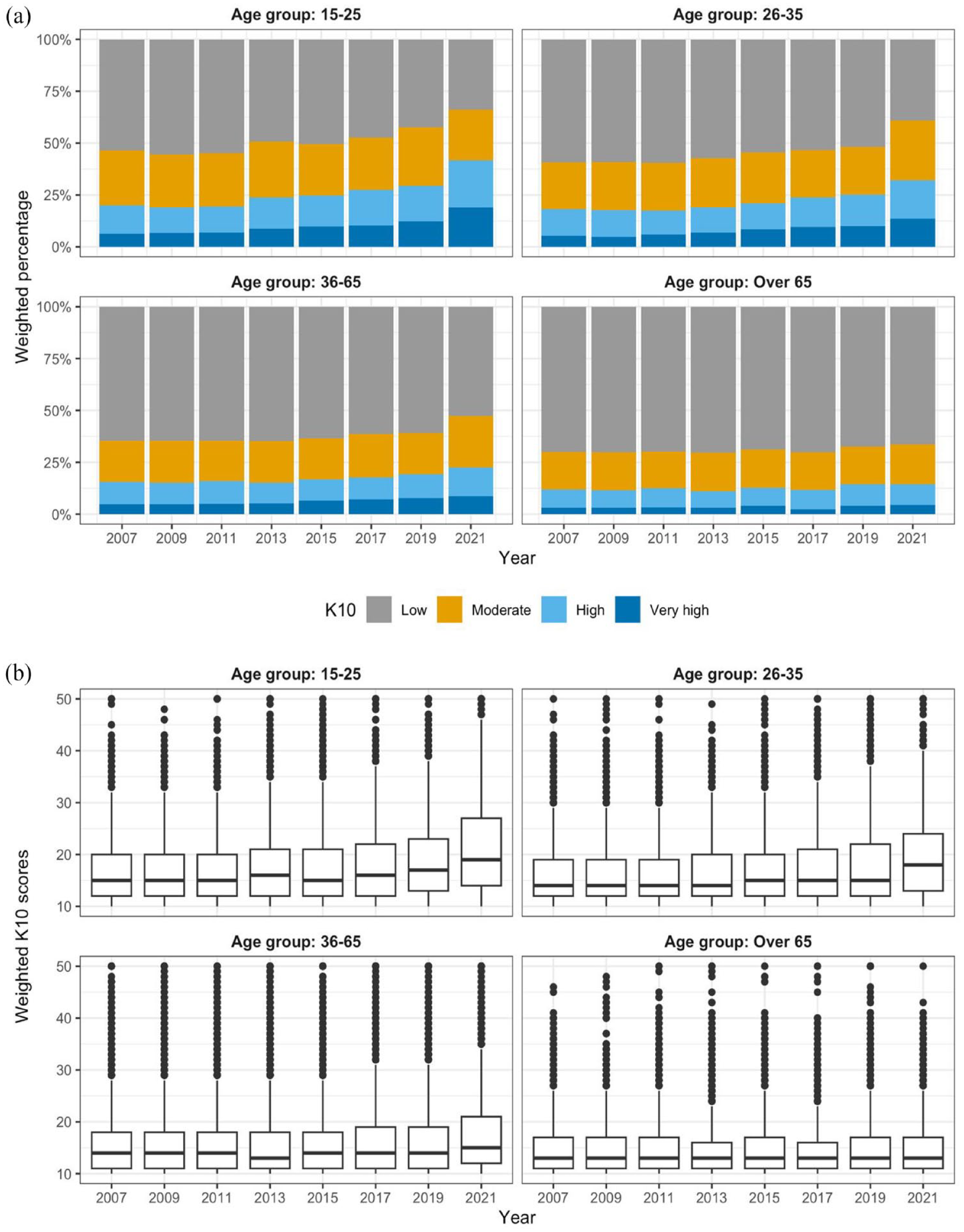
Changes in weighted percentage for K10 subgroups and weighted K10 scores from 2007 to 2021 by age group: (a) K10 subgroups and (b) K10 scores.
Prevalence of social determinants
The prevalence of several of the social determinants (including loneliness and lack of social support, poor family relationships and receiving government benefits) fluctuated throughout the years 2007 to 2021 (see Figure 3). In 2021, more people received government benefits overall and for all three comparison age groups, a likely result of increased government benefits in response to the COVID-19 pandemic. In 2021, 31% of young people aged between 15 and 25 years reported feeling lonely and a lack of social support, up from 21% in 2019. There was also a slightly increasing trend in reported poor family relationships in 2021 compared with earlier years across all age groups, particularly among those aged between 15 and 35 years.
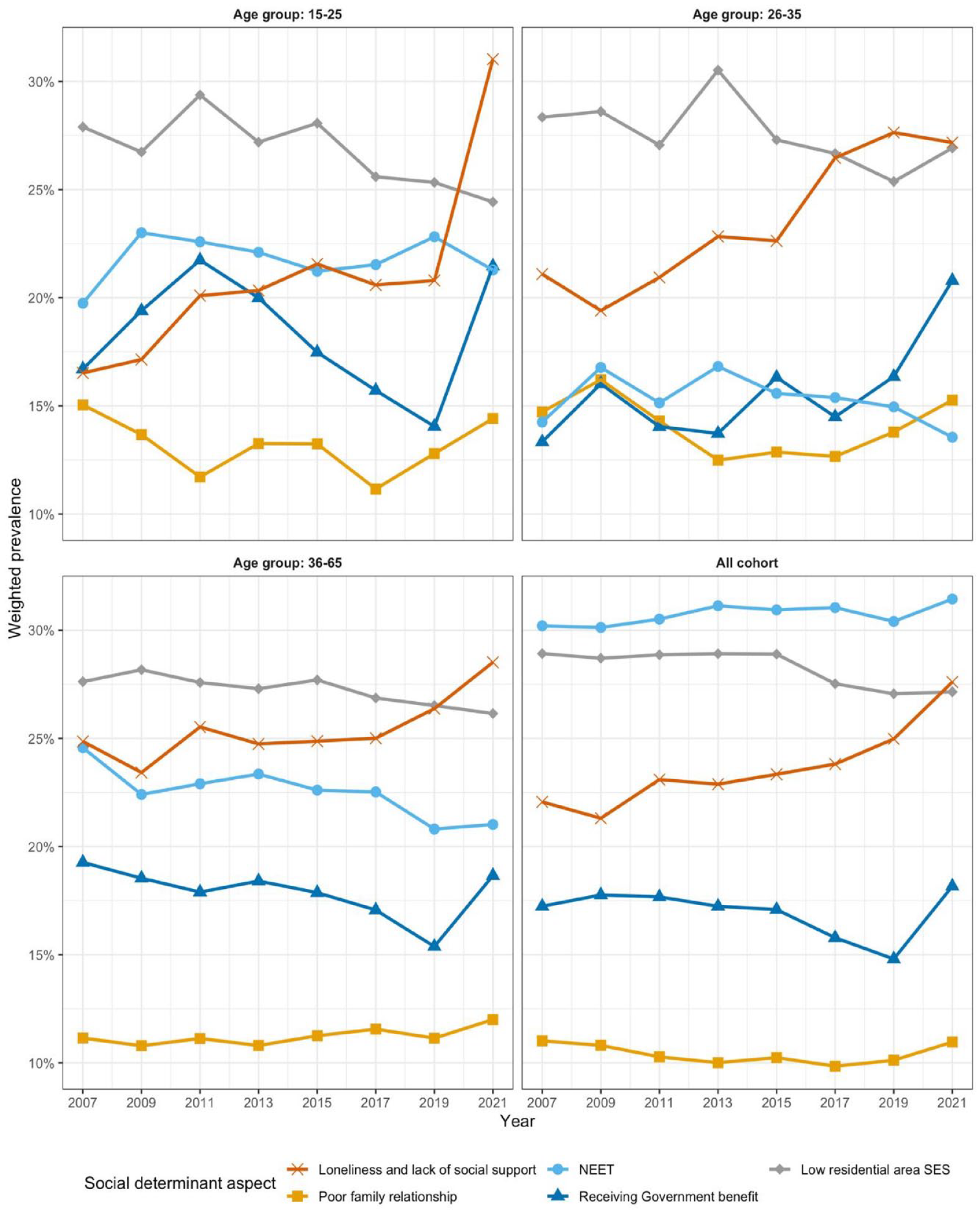
Weighted prevalence of each social determinant aspect by age group from 2007 to 2021.
Association between social determinants and psychological distress
Across the years, prevalence of high or very high K10 scores were substantially higher for participants who had experienced the five social determinants, compared to those who did not (see Figure 4). These differences were most profound for those who reported loneliness and lack of social support. In 2011, the rate of high or very high psychological distress among young individuals (aged 15–25) who did not experience loneliness and lack of social support was under 10%, in contrast to around 56% among those who reported feeling lonely and lack of social support. These numbers increased to ~28% vs ~72% in 2021. A similar trend was also observed between those who reported poor vs good family relationships. Financial factors (receiving government benefits and living in low socio-economic areas) seemed to impact mental health more for people aged between 26 and 65 years.
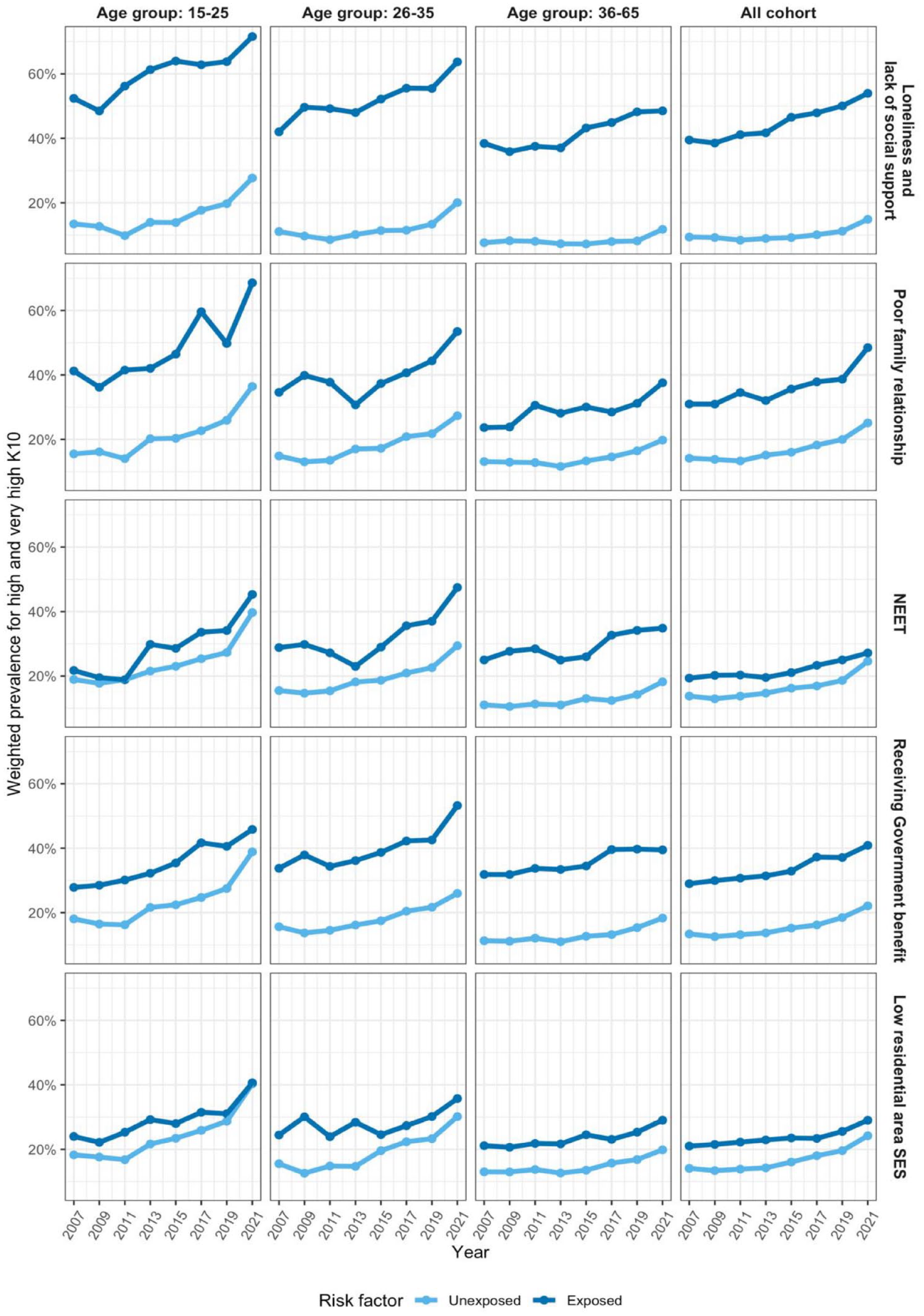
Weighted prevalence of high and very high K10 subgroups by social determinant risk factors from 2007 to 2021 across different age group.
Association of psychological distress and social determinant factors
In both uni- and multivariate linear regression models of K10 scores and the social determinants, loneliness and lack of social support had the largest and most increasing effect on the K10 among all five social determinants (univariate beta [95% CI] for 2007 = 5.82 [5.36, 6.28], and for 2021 = 7.44 [7.03, 7.84], see Figure 5). Poor family relationships and the receipt of government benefits were also significantly associated with psychological distress. Whereas IRSAD, which represents socio-economic status, had less effect on K10 scores, particularly in adjusted models when factors such as NEET and receiving government benefits were taken into consideration.
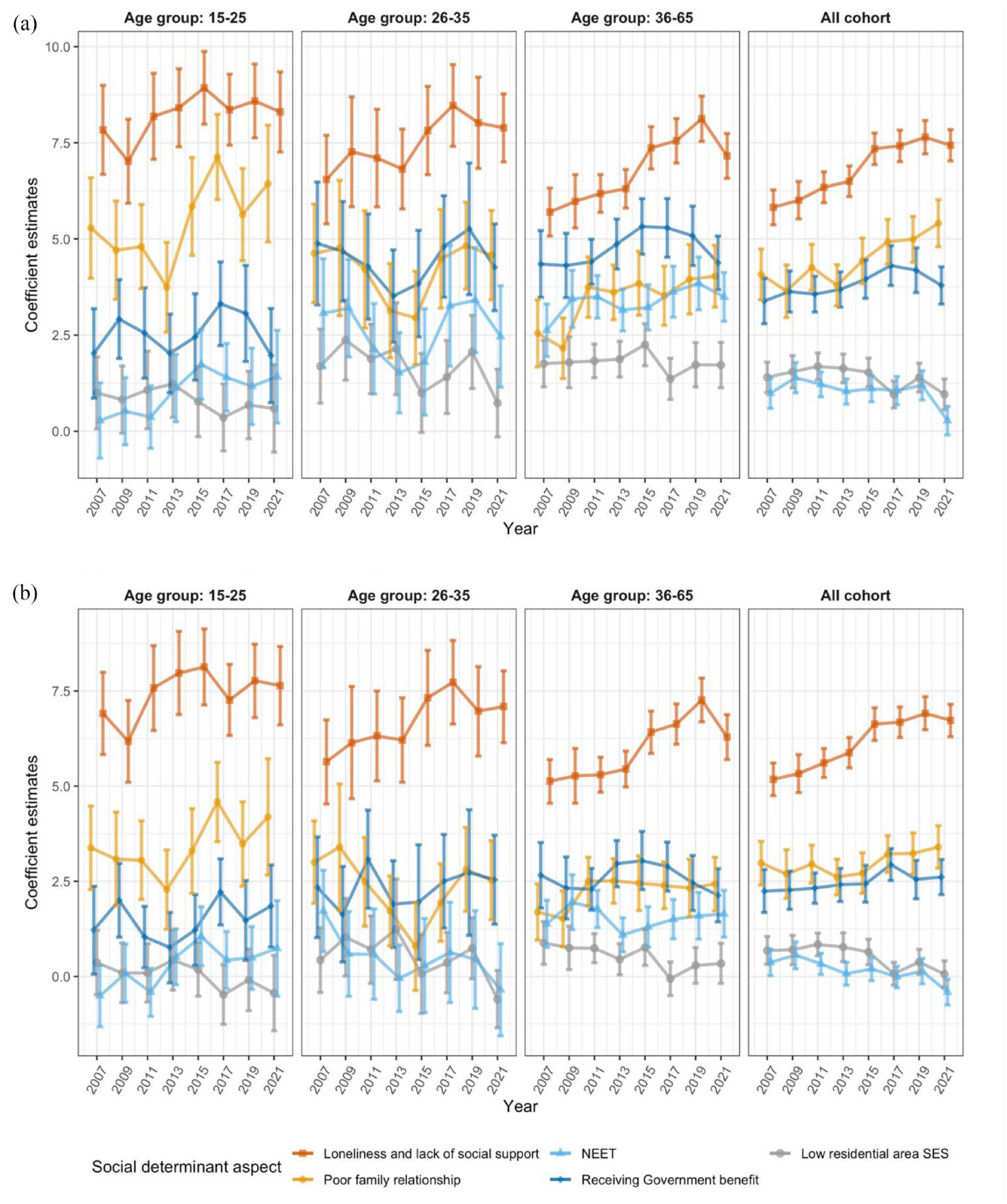
Weighted linear regression of K10 scores against social determinant aspects from 2007 to 2021 by age group. (a) Univariable unadjusted regression considering each social determinant aspects separately in each model and (b) multivariable regression considering all social determinant aspects in the same model.
For young people between 15 and 25 years, loneliness and lack of social support had a stronger effect on psychological distress compared with other age groups (univariate beta [95% CI] for those aged 15–25 years in 2021 = 8.30 [7.26, 9.35]), followed by family relationships (univariate beta (95% CI) for those aged 15–25 years in 2021 = 6.44 [4.92, 7.95]). While the prevalence of loneliness and lack of social support increased substantially during the pandemic, the strength of these associations during the COVID-19 pandemic (2021) remains comparable with the year before (2019). It is worth noting that for government benefit and IRSAD, there were significant decreases in coefficient estimates for all age groups as well as the whole cohort from 2019 to 2021, which is potentially due to changes in participants’ profiles over time.
Discussion
There has been a significant increase in youth mental ill-health in recent years, particularly post the COVID-19 pandemic, in Australia and worldwide (Gunnell et al., 2018; McGorry et al., 2023; Power et al., 2020). In our analysis of data collected from a large population cohort since 2001, we explored associations between social determinants and psychological distress to understand whether these have contributed to these increases. Our findings indicate an upward trend in the self-reported experience of psychological distress (using the K10 scale) among people aged 15 and 65 years. The largest increase was found among young people (15–25 years), with a doubling in the proportion of young people reporting high and very high levels of psychological distress between 2007 and 2021. This is similar to the increase evident in the National Survey of Mental Health and Wellbeing (Australian Bureau of Statistics, 2022). The period under evaluation includes the Global Financial Crisis in 2008 and spans to the second year of the COVID-19 pandemic. While these two global events had an acute impact on young people’s mental health, we also found a worsening trend in mental health across the intervening period. This trend is linked to social determinants.
Our analysis of social determinants of mental health found that loneliness and a lack of social support, as well as poor family relationships, are the two primary risk factors for psychological distress among young people. Notably, these factors are not only becoming more common but also intensifying in their impact. This pattern may elucidate the dilemma of rising mental ill-health among young people despite the expansion of mental health services. It is possible that the issues have not stemmed from services themselves being ineffective. Instead, it may be rooted in society’s failure to adequately address the rapidly evolving social risks impacting mental health (particularly for young people), and to equitably distribute resources to assist those with greatest need (Gao et al., 2023).
Loneliness and lack of social support was the most important social determinant across all indicators evaluated in this survey cohort. This is consistent for all age groups, with the strongest associations observed in young people. Indeed, a substantial body of literature supports the fact that loneliness and lack of social support are key causal factors for poor mental health (Hards et al., 2022; Matthews et al., 2023; Pearce et al., 2021), particularly among young people, with long-term impacts extended to poor physical, social and educational outcomes (Eccles & Qualter, 2021; Hutten et al., 2021). While the COVID-19 pandemic has markedly highlighted loneliness and lack of social support as significant contributors to the current surge in mental health issues (Farrell et al., 2023), it is crucial to emphasise that these trends were already in motion before the pandemic. The pandemic certainly exacerbated these issues significantly, especially among young people.
Available financial resources, at both individual and family level can also impact an individual’s mental health. Relative socioeconomic advantage is a fundamental determinant of mental health outcomes (Kirkbride et al., 2024). Across the lifespan, poorer mental health is one of the first health impacts of socioeconomic disadvantage (Kivimäki et al., 2020). The mental health benefits of increased financial stability were evident during the COVID-19 pandemic. The temporary increase in the number of people receiving welfare support payments and the amount received during the COVID-19 pandemic (Ullah & Harrigan, 2022) was associated with lower levels of reported psychological distress in the cohort overall. This pattern was not uniformly evident across age groups.
Among the remaining social determinants analysed, a young person’s perceived quality of parent/carer relationship was also a factor. Despite prevalence of poor familial relationships remaining relatively low in this cohort, it is increasingly a predictor of higher psychological distress, particularly among young people. Insecure family relationships have been identified as a contributing factor in experiences of loneliness among adolescents and young adults (Korzhina et al., 2022). We found that lower levels of satisfaction with parent or step-parent relationships were associated with higher levels of psychological distress. While the impact was not as great as loneliness and a lack of social support, it is an important insight considering the emphasis placed on the protective role of family for young people (e.g. experience of and confidence in relationships). These relationships are especially important in early adolescence during a young person’s transition to secondary school (Matthews et al., 2023) and for role modelling relationships for young people in forming friend, partner and peer relationships for social support (Binte Mohammad Adib & Sabharwal, 2024).
It is essential to understand that mental health and social determinants exhibit dynamic, bi-directional and circular relationships (Lim et al., 2019), that is, there exists a complex interplay where each factor can influence and be influenced by the other, leading to cycles that may perpetuate or exacerbate mental health conditions and social challenges (Pearce et al., 2021; Rahmani & Groot, 2023). These overlaps point to a need to provide support responses that take a holistic approach to a young person’s individual wellbeing, as well as their social and vocational participation.
Interventions to support young people experiencing psychosocial challenges can be intrapersonal, interpersonal and socially-focused (Eccles & Qualter, 2021). Examples of interventions across these three domains include: addressing a young person’s thinking and behaviour; improving their social skills; and providing social support and opportunities for social contact (Pearce et al., 2021). Most of the available evidence for loneliness interventions is for older people with more research needed with young people and the use of universal, selective and indicated approaches (Kirkbride et al., 2024; Rezaei & Saghazadeh, 2022). There is some evidence that psychological (intrapersonal) treatment can reduce loneliness for young people experiencing mental ill-health (Bauer et al., 2021). There is more evidence for improving social skills (interpersonal) including as a preventative measure (Kirwan et al., 2023), to support young people experiencing loneliness (Pearce et al., 2021) and to improve related mental health outcomes (Bauer et al., 2021). Connecting young people experiencing both loneliness and mental ill-health with organised social activities (referred to as social prescribing) is popular, however, the evidence is weak (Bickerdike et al., 2017). Caution is needed in facilitating social contact as an intervention for loneliness, to ensure consideration is given to the quality of relationships young people experience (Pels & Kleinert, 2016).
Policy implications
Understanding and responding to social determinants of health is a challenge for policymakers. A ‘comprehensive shift’ in political commitment is required to deliver the systemic change necessary to address social determinants of health (McCartney et al., 2023). This shift will require a whole-of-government commitment as investment in one portfolio will likely have some level of benefit for another portfolio (e.g. the potential reduction in future health costs as a result of a school retention program). Benefits will not necessarily be evident within short-term budget cycles, but rather result in health improvements over a person’s life course (Milstein & Homer, 2020). The focus on social determinants of health has been identified as a barrier to investment from non-health portfolios; requiring the broader objective of population wellbeing (Kottke et al., 2016).
The significance of loneliness and a lack of social support as a social determinant has led to the development of priority actions to develop evidence-informed policy, service and practice responses (Lim et al., 2023). Identity and social-emotional skills are important in developing supportive peer relationships during adolescence, and school environments are considered a ‘compelling’ setting for prevention programs (Mitic et al., 2021). To allow for the identification of, and targeted responses to, the multiple, intersecting social determinants, the implementation of multi-dimensional tools such as the Filia Social Inclusion Measure (F-SIM16; Filia et al., 2022), is required in settings where young people can be reached, such as school and community health settings. The F-SIM16 is an example of a useful tool that can be used to guide care, monitor progress, evaluate effectiveness of interventions and provide data regarding different populations. Identified causes of involuntary loneliness among adolescents and young adults (illness, personal barriers, negative life experiences and life transitions) also provides direction for the development of interventions (Korzhina et al., 2022). Understanding the role of virtual and online social environments in meeting young people’s need for social connection, including the development of social support in early adolescence requires more research (Mitic et al., 2021).
Strengths and limitations
The HILDA survey provides a rich database for analysing the social, health and economic experiences of Australian households over more than two decades, with an average total analysed sample of more than 16,000 respondents. This study approached each time point as cross-sectional data, leveraging the weighting framework to gain insights into characteristics that might be representative of the Australian population as a whole, in a well-developed and long-established survey (Watson, 2021). However, the impact of participants joining, remaining and leaving the cohort was not considered, which may be associated with attrition and participation bias.
Additionally, as this study relied on secondary data analysis, we were limited in the construction of variables by questions that had been defined in the survey, a common limitation of this type of data. Finally, due to the sensitive nature of social inclusion, psychopathology and the length of the survey, several variables were missing some data. However, this was addressed with multiple imputations with a significant number of datasets (n = 20). The sensitive nature of these characteristics might also increase the risk of social desirability bias, which may have differed across years due to possible variations in delivery methods.
Despite these limitations, the sample size, survey duration and range of available variables has enabled us to contribute to a greater understanding of the role of social determinants on the increasing prevalence of mental ill-health experienced by young people.
Supplemental Material
sj-docx-1-isp-10.1177_00207640241280910 – Supplemental material for The changing impacts of social determinants on youth mental health in Australia
Supplemental material, sj-docx-1-isp-10.1177_00207640241280910 for The changing impacts of social determinants on youth mental health in Australia by David G Baker, Mengmeng Wang, Kate M Filia, Shu Mei Teo, Rikki Morgan, Myriam Ziou, Pat McGorry, Vivienne Browne and Caroline X Gao in International Journal of Social Psychiatry
Footnotes
Acknowledgements
This paper uses unit record data from the Household, Income and Labour Dynamics in Australia Survey [HILDA] conducted by the Australian Government Department of Social Services (DSS). The findings and views reported in this paper, however, are those of the authors and should not be attributed to the Australian Government, DSS or any of DSS’ contractors or partners. DOI: 10.26193/24EJST.
Author contributions
David G. Baker: Conceptualization, Writing – original draft, Writing – Review & Editing; Mengmeng Wang: Conceptualization, Methodology, Software, Formal Analysis, Writing – original draft, visualization, Writing – Review & Editing; Kate M. Filia: Conceptualization, Writing – Review & Editing Shu Mei Teo: Conceptualization, Validation, Writing – Review & Editing; Rikki Morgan: Conceptualization, Writing – Review & Editing; Myriam Zhou: Conceptualization, Validation, Writing – Review & Editing; Pat McGorry: Conceptualization, Writing – Review & Editing; Vivienne Browne: Conceptualization, Writing – Review & Editing; Caroline X. Gao: Conceptualization, Supervision, Methodology, Formal Analysis, Writing – original draft, Writing – Review & Editing. All authors contributed to and have approved the final manuscript.
Conflict of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: rygen is funded by the Australian Government Department of Health and Aged Care to provide technical advice and policy direction on a number of youth mental health topics, including social determinants. This is relevant for DB, RM and VB.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Orygen funded the paper, which involved data analysis, data interpretation and writing of this paper.
Ethical approval
Not applicable.
Research data and analysis code
Research data is available at https://dataverse.ada.edu.au/dataverse/DSSLongitudinalStudies. All analysis code is available at ![]() .
.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.