
Abstract
Objective:
Gender-sensitive approaches to increasing men’s physical activity (PA) through sports settings have shown promise across cultural contexts. We examined changes to men’s walking and the contribution of walking towards self-reported PA after participating in the men-only European Fans in Training (EuroFIT) programme before exploring men’s experiences of sustaining walking to explain the quantitative findings.
Design:
A sequential mixed-methods design was used to collect self-reported PA questionnaire data as part of a randomised controlled trial at baseline, post-programme and 12-month follow-up, together with focus groups with participants.
Setting:
EuroFIT was delivered by football club/community coaches to overweight fans in football clubs across England, the Netherlands, Portugal and Norway.
Results:
Linear regression modelling demonstrated that self-reported walking was significantly higher at both post-programme (426 metabolic equivalents [METs], 95% confidence interval [CI]: 287–565, p < .001) and at 12-month follow-up (343 METs, 95% CI: 205–482, p < .001) in all countries in favour of the intervention group, despite a large decline in Norway from post-programme to follow-up. The contribution of walking towards total PA did not change after participating in EuroFIT. Qualitative analysis indicated that most men were positive about walking and had embodied learning from the EuroFIT programme, but also that some men also considered walking a transitional activity towards other more intensive forms of PA.
Conclusion:
EuroFIT succeeded in helping overweight, male football fans increase walking as part of their self-reported total PA. Although the percentage of walking in relation to total PA remained the same for participants in both groups, EuroFIT helped men to integrate walking into their daily lives.
Introduction
Sedentary lifestyles and low levels of physical activity (PA) remain important risk factors for men’s health, as a large proportion of men in developed countries are still not sufficiently physically active to harness the benefits of regular PA (Strain et al., 2024). As men are often difficult to reach with health behaviour interventions (Bottorff et al., 2015), there is a continued need for developing ways to promote PA that appeal to men across different ages and cultural contexts (Strain et al., 2024). One promising approach is the use of professional sports clubs to engage men in gender-sensitised lifestyle change interventions together with other fellow fans, which has been shown to be effective in increasing PA or daily steps across different age groups and cultural contexts (e.g. Caperchione et al., 2021; Hunt et al., 2014; Maddison et al., 2023; Petrella et al., 2024; Wyke et al., 2019). Of these, only Petrella et al. (2024) reported on increases in self-reported walking at 12-month follow-up, but they did not connect walking outcomes to men’s experiences of sustaining walking long term.
Walking is a light-to-moderate intensity PA that can be integrated into men’s everyday life to improve their health short- and long-term (Harris et al., 2018). It is a form of PA that is considered accessible and convenient for men of different ages (e.g. Mitchell et al., 2018). Increases in walking are associated with wide-ranging health benefits such as lowered risk of all-cause mortality and cardiovascular disease (CVD) morbidity and mortality across age, gender and weight, as well as reduced systolic and diastolic blood pressure and body weight (Banach et al., 2023; Paluch et al., 2022; Stamatakis et al., 2018). For example, a recent meta-analysis found that an increase of 3,867 steps per day improved all-cause mortality and only 2,337 steps per day improved CVD mortality (Banach et al., 2023), whereas another demonstrated that increases of 1,000 steps per days contributed to larger reductions in hazard ratios for all-cause mortality in adults with a daily step count less than 6,000 compared with those above 6,000 steps (Paluch et al., 2022). Walking can also have a positive effect on mental health, such as increased psychological well-being (Kelly et al., 2018), as well as decreasing anxiety, loneliness and symptoms of depression (Kelly et al., 2018; Robertson et al., 2012).
Building on positive evaluations of walking in the Football Fans in Training (FFIT) programme (Bunn et al., 2016; Hunt et al., 2013), we designed The European Fans in Training (EuroFIT) programme to promote walking as a safe and accessible PA and to be culturally sensitive to local PA norms 1 in England, the Netherlands, Portugal and Norway. We used contemporary motivational theories (Roberts and Nerstad, 2020; Ryan and Deci, 2017), evidence of successful behaviour change techniques (BCTs) promoting PA or walking (e.g. Samdal et al., 2017), and sociological understandings of masculinity in relation to health and health behaviour (Bunn et al., 2016) in programme development. EuroFIT was gender-sensitive in relation to male contexts (e.g. programme delivery in football clubs), programme content (e.g. a toolbox of BCTs and football-related PA) and style of delivery (e.g. facilitating interactional style familiar to men in predominantly male contexts) (Van Nassau et al., 2016). We delivered the EuroFIT programme in club or club community facilities at 15 professional football clubs across England, the Netherlands, Portugal and Norway; 5 of which were in England, 4 in the Netherlands and 3 in Norway and Portugal. EuroFIT successfully improved objectively measured PA by 678 steps (97.5% confidence interval [CI], 309–1,048; p < .001) and the self-reported total PA of 894 metabolic equivalents 2 (METs: 95% CI, 571–1,216; p < .001) in favour of the intervention group, but did not reduce sedentary time at 12-month follow-up (Wyke et al., 2019). Although the programme succeeded in increasing PA, changes to walking and the contribution of walking to the overall improvement of PA were not part of the main analysis. Given the considerable health benefits of relatively small increases to daily steps (Paluch et al., 2022), it is important to understand whether the EuroFIT programme succeeded in increasing and integrating walking as a form of PA into participants’ daily lives.
With this two-step mixed-methods study, we first examine changes to walking, and the contribution of walking towards total self-reported PA for overweight football fans at 12-month follow-up in the EuroFIT randomised controlled trial (RCT) across the four countries, before we subsequently explore participants’ experiences of sustaining walking to help explain the quantitative findings.
Methods
Study design
We undertook secondary analyses of self-reported PA questionnaire data from the intervention and control group in the EuroFIT RCT and focus group discussions (FGDs) with trial participants using a sequential mixed-methods design. To investigate changes to walking and the contribution of walking to total PA, we used self-reported PA data as the different PA intensities (walking, moderate intensity [MPA] and vigorous intensity physical activity [VPA]) was not subtractable from the objectively measured activePAL data.
Integration of walking in the EuroFIT programme
EuroFIT introduced walking as a way to increase men’s daily steps during the first session, in which men were invited to take part in a group walk around the club grounds or club facilities (Van Nassau et al., 2016). As part of the 12 weekly EuroFIT sessions, which included group-based discussions and different forms of PA (e.g. walking football), men were encouraged to set individually personalised daily step goals incrementally (e.g. register a baseline for walking and increase 1,500 steps from baseline on 3 days the following week) using the SMART goal approach and to share on their weekly efforts with coaches and participants.
We developed the SitFIT, a pocket-worn, self-monitoring device to provide real-time feedback on steps and (non-sedentary) upright time, allowing participants to actively monitor their steps throughout the programme and during PA, and compare their step count to their goals. Coaches supported participants in discussing and reflecting on the benefits of doing PA that the men considered meaningful and personally valuable to themselves (e.g. walking alone, walking with friends or a group, hiking; cycling; playing (walking) football). Men were also encouraged to use action planning to mitigate setbacks or difficult life events, and to identify sources of support that could influence their daily steps or walking positively and facilitate maintenance long term (e.g. establishing walking groups with other men or EuroFIT members).
Participants
Men were eligible to participate in the EuroFIT RCT if they were aged between 30 and 65 years old, had a self-reported body mass index (BMI) of 27 kg m−2 or more, consented to the study procedures and provided at least 4 out of 7 days of usable activity monitor data at baseline. Participant recruitment procedures for the EuroFIT RCT are detailed elsewhere (Van Nassau et al., 2016; Wyke et al., 2019).
We recruited men to participate in the focus groups based on having attended six or more EuroFIT sessions when the programme ended. We purposively selected men across different age ranges (i.e. 30–40, 41–50, 51–65) and attempted to recruit the same men at post-programme and 12-month follow-up. Number of FGD participants and clubs compared by country are detailed in Table 1.
Number of FGD participants at post-programme and 12-month follow-up, and descriptions of themes generated by the qualitative analysis.
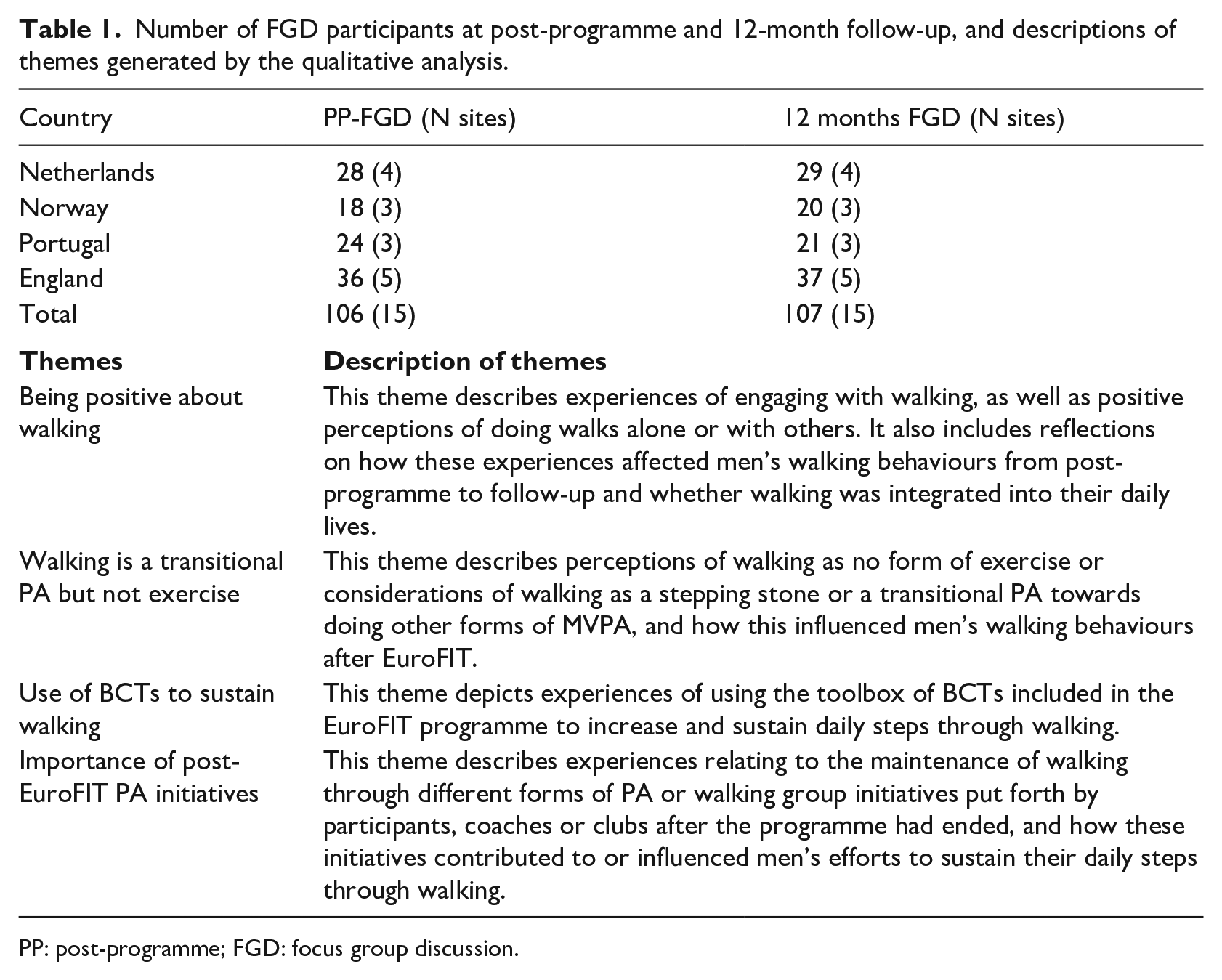
PP: post-programme; FGD: focus group discussion.
Data generation and measures
Self-reported questionnaire data and focus group data were collected on different occasions, but at the same time (i.e. baseline, post-programme and 12-month follow-up) across all countries (for further details, see Van De Glind et al., 2017; Van Nassau et al., 2016).
All 1,113 RCT participants (560 allocated to intervention and 554 to comparison group) were asked to complete self-report questionnaires at all three time-points. We assessed self-reported PA using the International Physical Activity Questionnaire Short Form (IPAQ-SF), which was administered to trial participants in-person at all measurements (Craig et al., 2003). The IPAQ-SF focuses on the amount of PA performed over the past 7-day period and includes questions about the time spent engaging in vigorous PA, moderate PA and walking in 10-minute bouts or longer. Within these domains, participants are asked to consider all types of PA, including activities performed during leisure time, domestic and gardening activities, work-related activities and transport-related activities. Relevant examples of activity performed at the different intensities were mentioned in the items. Data obtained from the IPAQ-SF were used to estimate the total amount of PA completed over 7 days by weighting the reported minutes per week in each domain by a MET energy expenditure estimate. The weighted MET minutes per week was then calculated by multiplying the duration (min), frequency (days) and MET intensity and then summing the three domains, namely, vigorous (8 METs), moderate (4 METs) and walking (3.3 METs), to produce a weighted estimate of total PA per week (min∙week−1). Data cleaning and processing were carried out in accordance with the guidelines published by the IPAQ Research Committee (IPAQ, 2022).
As part of the process evaluation, we conducted 15 FGDs with trial participants (4–8 participants per group) post-programme, and an additional 15 FGDs at 12-month follow-up in all countries (see Table 1). We developed standard operating procedures for the FGDs to facilitate data collection consistency across the participating countries. A semi-structured interview guide was used to prompt discussion on what men thought of the EuroFIT programme, which programme components they believed were helpful or unhelpful and whether the programme had impacted on their lives. All focus groups were held in club facilities or in stadia at the professional football club, and were moderated by one or two trained qualitative researchers who were fluent in the local language, assisted by note takers. Regular team debriefing meetings with feedback were organised across the consortium to facilitate reflexive discussion of how we collected data.
Analysis
In an intention-to-treat analysis, we used linear regression modelling to calculate standardised mean differences for different forms of self-reported PA to determine the intervention effect, and to estimate the percentage of walking towards total PA, where we adjusted for baseline values and age. We included participants from both randomised groups regardless of compliance with the intervention in the models that were run for post-programme, 12 months and per country. Participants with missing data were excluded from the analysis. SPSS v27 software package was used for all quantitative analysis.
Based on our quantitative findings, we used a structured, thematic framework analysis to explore participants’ experiences of sustained walking (Gale et al., 2013). The first step involved the qualitative research team re-familiarising themselves with the FGD transcripts collected as part of the process evaluation in the EuroFIT RCT. In an adaptation to our protocol detailed elsewhere (Van De Glind et al., 2017), one of the authors then generated a codebook draft comprising codes and code descriptions after reading all transcripts. Through collaborative online meetings via Zoom, in which researchers from other countries had re-read two transcripts, we discussed and revised the codebook, where we grouped codes together conceptually in preliminary themes while also discarding duplicate or irrelevant codes. For example, codes that focused on men’s perceptions of walking (e.g. walking is social; walking is doable) that contributed to maintenance were grouped into a broader theme. All codes and coding descriptions were in English. Coding decisions were consensus-based through critical discussion within the qualitative analysis team, which comprised one member from each country. These members were trained in social sciences, public health or health psychology and were all part of the implementation of the EuroFIT RCT. The first author then developed a consolidated codebook (online supplemental file 1). An experienced qualitative researcher with knowledge of the data, who did not take part in the initial coding discussions, reviewed the codebook for conceptually overlapping coding descriptions as a ‘critical friend’ (Smith and McGannon, 2018).
We re-coded transcripts according to the codebook and undertook further coding of the remaining transcripts. Throughout this iterative process, if changes to new codes or themes were requested by one of the researchers, the qualitative analysis team discussed and reflected on the changes via online meetings or e-mail exchanges to facilitate reflexivity before adjusting coding (Milford et al., 2017). For example, when we tied the analysis to the quantitative findings, we decided to split descriptions of walking as not being exercise and as a stepping stone towards other PA into a separate theme that could explain increases in VPA. Using a coding report template in English, each local researcher summarised the coded data descriptively and provided illustrative quotes of all codes pertaining to themes. All coding reports were sent to the first author who analysed the reports for differences and similarities across the four countries using a simplified matrix (Gale et al., 2013). At this stage, differences in experiences relating to post-EuroFIT PA generated a fourth theme that could explain differences in walking values between countries at follow-up. From this, the first author drafted the overall qualitative findings. The full draft was then circulated to co-authors for a critical review of interpretation.
Ethical considerations
We obtained ethical approval for the RCT and the process evaluation from appropriate country-specific ethics committees (Ethics committee of the VU University Medical Centre [2015.184]; regional committees for medical and health research ethics, Norway [2015/1862]; the Ethics Council of the Faculty of Human Kinetics, University of Lisbon [CEFMH 36/2015]; and the Ethics Committee at the University of Glasgow College of Medicine, Veterinary and Life Sciences [200140174]). All participants who participated in the RCT or in focus groups consented to do so in writing.
Results
Changes to walking and the contribution of walking to total self-reported PA
Participant demographics were published as part of the main trial evaluation (Wyke et al., 2019). The MET values (MET·min·week−1) for walking, MPA, VPA and total PA were significantly higher at both post-programme and at 12-month follow-up for the intervention group, compared to the control group (Table 2). Changes in self-reported total PA from baseline to follow-up could mostly be attributed to increases in walking and VPA. At 12-month follow-up, the difference in MET·min·week−1 of 343 for the intervention group compared to control constituted 103 minutes of walking at 3.3 METs.
Subjectively assessed physical activity outcome measures for participants allocated to the EuroFIT programme immediately (intervention) or after 12 months (control).
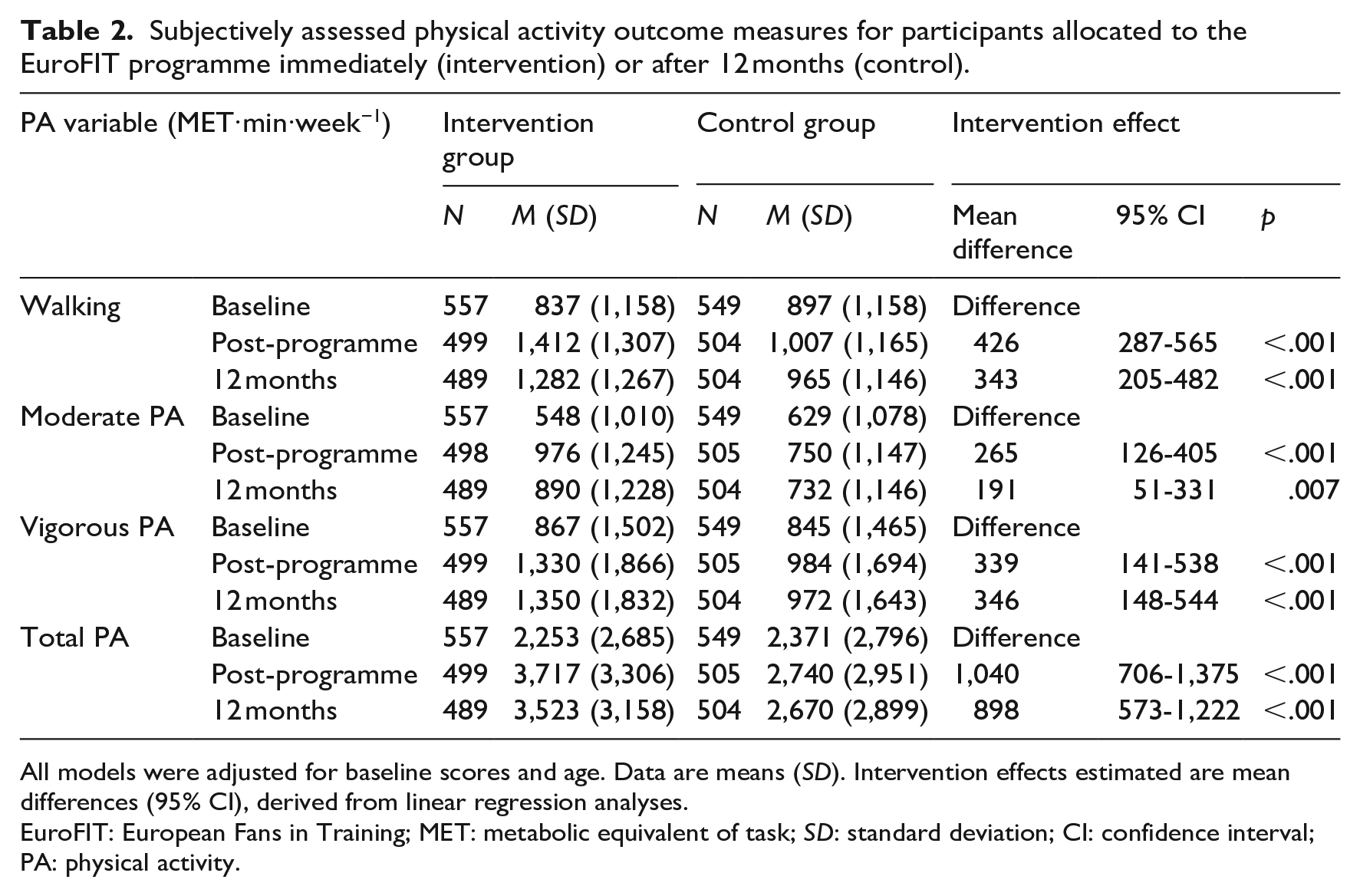
All models were adjusted for baseline scores and age. Data are means (SD). Intervention effects estimated are mean differences (95% CI), derived from linear regression analyses.
EuroFIT: European Fans in Training; MET: metabolic equivalent of task; SD: standard deviation; CI: confidence interval; PA: physical activity.
Although the intervention group showed a relatively large increase in walking from baseline through post-programme to 12-month follow-up compared to the control group, there was a substantially larger decline in Norway from post-programme to follow-up compared to the other countries (Table 3). Country-specific MET values for walking, MPA, VPA and total PA are available in online supplemental file 2.
Subjectively assessed walking for participants allocated to the EuroFIT programme immediately (intervention) or after 12 months (control) per country.
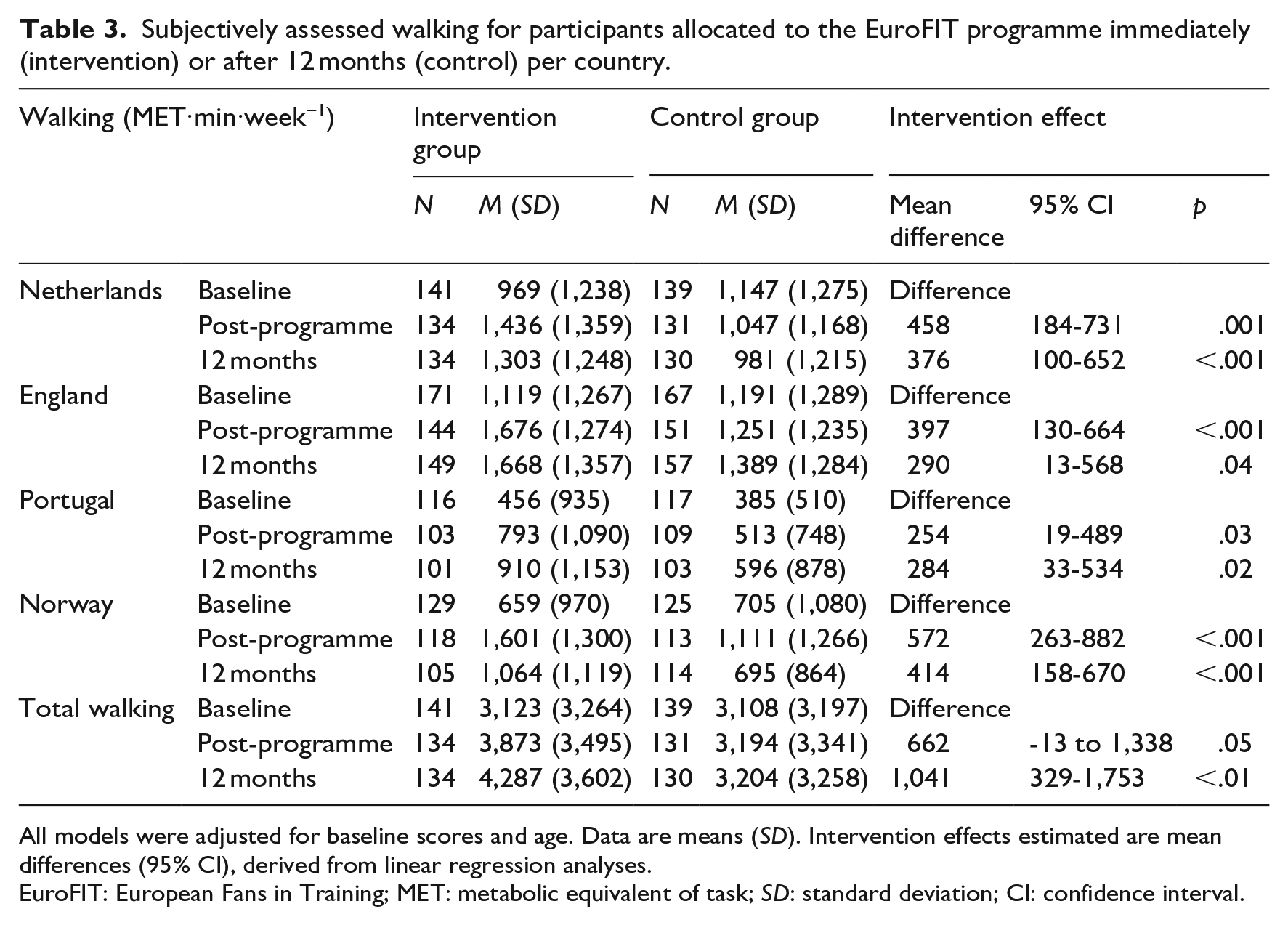
All models were adjusted for baseline scores and age. Data are means (SD). Intervention effects estimated are mean differences (95% CI), derived from linear regression analyses.
EuroFIT: European Fans in Training; MET: metabolic equivalent of task; SD: standard deviation; CI: confidence interval.
We did not find a significant difference between the intervention and control groups on the percent of walking of total PA (Table 4). The percent of walking of total PA constituted a relatively large proportion of both groups’ PA (44%–48%) levels, but did not change from baseline to post-programme and 12 months. We also found relatively small differences between countries on the percentage of walking in relation to total PA (37%: Portugal–49%: England) at 12 months, but these did not change from baseline.
Linear regression of the intervention effect on percent of walking of total PA, adjusted for baseline values and age, per country.
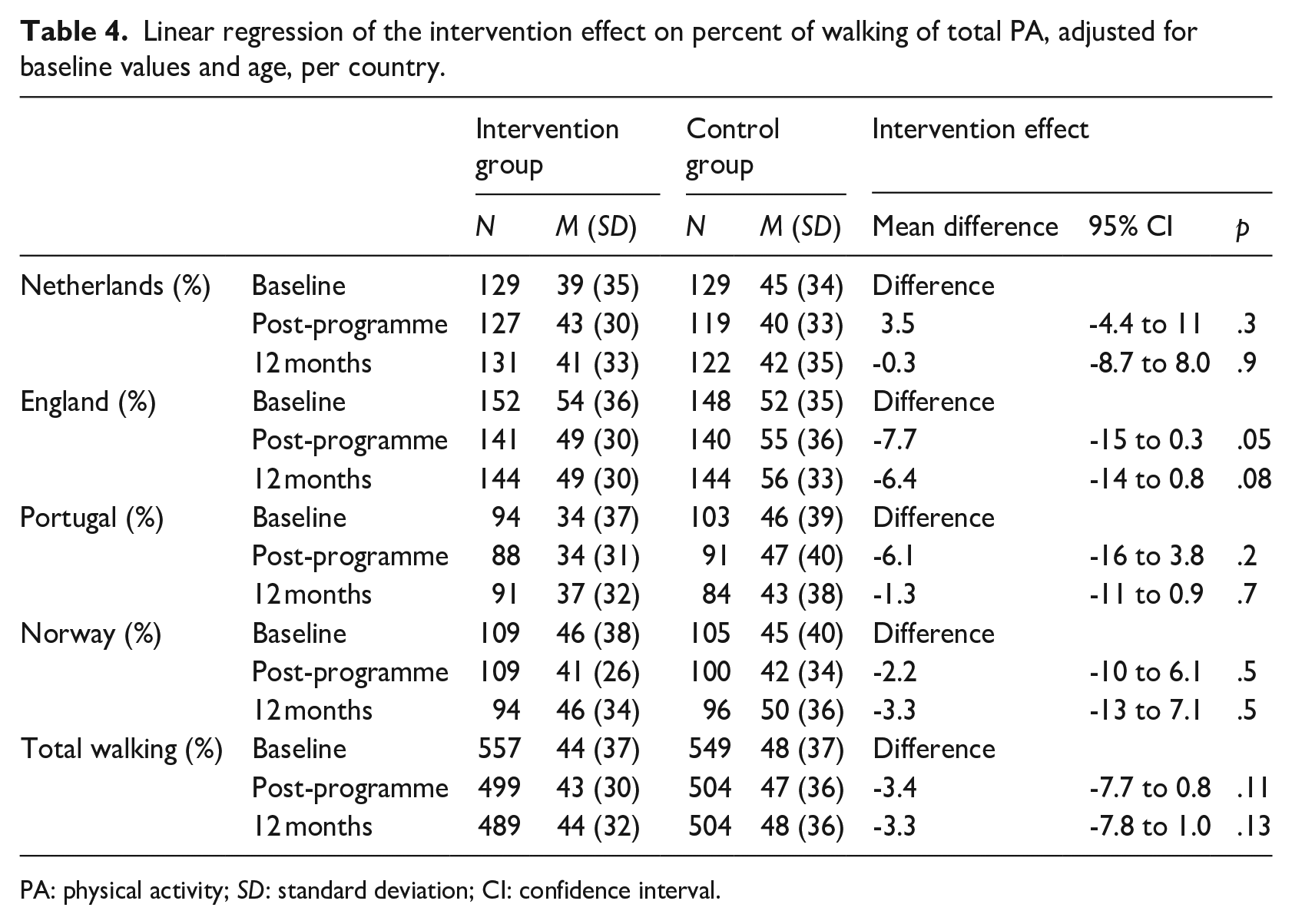
PA: physical activity; SD: standard deviation; CI: confidence interval.
Based on these findings, we explored men’s experiences of sustaining walking to understand what helped increase walking at 12-month follow-up, why their percentages of walking did not change and why walking declined substantially more in Norway compared to other countries from post-programme to follow-up.
Experiences of sustaining walking after participating in the EuroFIT programme
The qualitative analysis generated four broad themes that could help explain the quantitative findings. These were: (a) being positive about walking, (b) walking is a transitional PA but it is not exercise, (c) the use of BCTs to sustain walking and (d) importance of post-EuroFIT PA initiatives (see Table 1 for a description of themes). Supplementary illustrative quotations are available in online supplemental file 1.
Each quote reported denotes a participant ID (P [participant: PX if unidentified]; a club (ENG101-105, NL206-209 NOR310-312, POR413-415); and a data source (PP-FGD [post-programme focus group], 12M-FGD [12-month focus group]).
Being positive about walking
In line with the increases in self-reported walking at post-programme and 12-month follow-up, men in all countries reported being positive towards walking as a form of PA. When analysing what made men describe walking as something positive, they reported that walking had become a PA that they planned for during the week because they felt capable of doing it regularly as part of their everyday life, that they enjoyed it and that it had become important to them. Some men stressed the social nature of walking together with others, while others commented on how walking changed their perspective on commuting or distances in their neighbourhood and how walking helped in losing weight and/or improving their physical condition:
P7: . . . it was fantastic that we focused on walking. I lost my first 15 kilos walking. I did not run one metre. [. . .] it’s unbelievable that walking can get you so well into shape. I hadn’t believed that when we started last year. So . . . so it’s perhaps a very important point to say to other people who are in the same situation as us, that simply walking, quick (brisk) walking, that is basically the key, really. (NOR310_12M-FGD)
Some men commented on how the convenience of walking made it feel easy to start or increase daily steps during the EuroFIT programme. They described how walking only required making small changes in their lives which felt attainable, and how walking easily fitted into their everyday life after EuroFIT had ended:
P1: I do, I walk from [name of] station, I work in [where works], it’s about 50 minutes’ walk, instead of taking the bus all the time, I come out of the station and walk, now since the programme. I would say about 70 or 80 per cent of the time I just walk to the office, which is good, in the morning, and when I’m going home also. (ENG101_12M-FGD)
Some men in Norway and England also discussed how walking abated their feeling of doing PA as something unsafe or dangerous from a health perspective, as they were not afraid of bodily pains or the risk of injuries when walking. This seemed to positively influence these men’s confidence in the long term:
P1: If you have a bad back, it is not dangerous to move (to walk) [. . .] I have had some pain in my thighs and knees. I feel the pains, they’re there really, but nothing has happened [when walking]. And that makes me a little confident that I can do such things without stopping. (NOR311_PP-FGD)
Walking is a transitional PA but is not exercise
Although most of the men across all four countries appreciated walking as a form of PA, some considered walking as a transitional PA before taking up more VPA or other forms of exercise after the programme ended. These men reported that they considered walking an important stepping stone, but also described how walking had made them feel more physically able to do other forms of PA:
P3: . . . every Tuesday we play football and exercise. And I think that’s important because that’s something you look forward to every Tuesday. And yes, I have only benefited from it [walking], at EuroFIT so to speak. Because before I started EuroFIT I had no idea at all about how to approach it (becoming active). (NL206_12M-FGD)
Other men reported that they preferred other forms of PA (e.g. regular football) or more VPA rather than walking from the outset. Most of these men reported other preferences for PA because they considered themselves ‘too fit’ to walk: ‘P: [in terms of] the level of exercise, because walking . . . I can’t, it doesn’t work (PT413_12M-FGD)’. Unlike other participants in EuroFIT, these men said they found little value in walking or believed that walking would not improve their physical condition or make them any fitter:
P1: well, the [walking in] EuroFIT programme does not help if you do not do something in addition. Really, those Wednesdays, it is so limp . . . you do not get fit from that. (NOR312_PP-FGD)
As some men in all countries preferred other PA to walking, this could partly explain the increase in self-reported VPA at 12 months across all four countries.
Use of BCTs to sustain walking
One of the key components in the EuroFIT programme was the emphasis on learning how to use a ‘toolbox’ of BCTs to increase their step count. This included self-monitoring, goal setting, action planning and seeking social support. Most men in all countries reported that two of the change techniques were particularly helpful when doing walks post-EuroFIT: the combination of setting individualised incremental step goals, and self-monitoring steps using the SitFIT device. They reported that how using SitFIT raised their awareness of steps and made it easy to monitor their step count against their goals each week which seemed to incentivise walking:
PX: I was an anti-walker, so to speak. I rarely walked. As soon as I could sit in the car and park somewhere, I got in. I have to say that [now] I walk a lot these days . . . so in the evening, I sit on the couch and I look at SitFIT and then I look, hey, if I’m under ten thousand then I have to walk around somewhere. And then I just go for a walk. (NL206_PP-FGD)
Others described how monitoring their steps and setting weekly step goals over the follow-up period had become a routine and a habit that they valued, which could help explain the sustained walking values at follow-up:
P4: I think the step thing (SitFIT) has been really, really useful, and it’s almost second nature, when I get up in the morning, where’s the step thing, put it on straightaway, and the odd occasion when I forget it, I feel naked without it, so I shouldn’t be doing anything but I found the step thing really, really useful. (ENG102_12M-FGD)
While some men reported still using the SitFIT and the incremental goal setting combined, others had transferred to other self-monitoring devices after EuroFIT had ended, while some reported that they no longer needed the monitoring device for walking (despite being offered the opportunity to keep the SitFIT after the EuroFIT programme had ended). A couple of the men in England and Norway, however, expressed frustration with the use of incremental goal setting as they considered the increase in steps somewhat unrealistic for those with a high baseline step count or felt that some coaches did not provide sufficient support in setting individual step goals (see quotes in online supplemental file 2).
Men in Norway and England also discussed how the convenience of walking worked well in combination with action planning: it made it easier to plan for walks during holidays, the winter season or during other life events that reduced their overall PA level. This included making specific plans for walking to ‘earn’ themselves treats, to compensate for other unhealthy choices or actions, or to ‘even out the score’ during holidays or other celebratory life events (e.g. birthdays, weddings):
P3: We took the kids to [an amusement park] and trying to find anything that isn’t burger and chips there that doesn’t cost the earth, so it was literally the most unhealthy . . . But we made sure we walked everywhere. So rather than getting the bus to the park, we walked for ten, fifteen minutes. And then at nighttime, I tried to do a bit more walking, so I kind of compensated by doing more. (ENG103_12M-FGD)
Another BCT included in the programme was finding sources of social support to help men increase and sustain their walking behaviours. Men in all countries reported walking with their wives/partners, (grand)children or friends during and after the programme ended: ‘PX: . . . this weekend I am going to a walking event with my grandsons. It is going to be fun’ (PT415_12M-FGD).
Importance of post-EuroFIT PA initiatives
As part of the EuroFIT programme that focused on maintenance of PA and finding lasting sources of support beyond the programme, men were encouraged to plan for ways to sustain their daily step goals through walking or to initiate new forms of PA (e.g. walking football) after EuroFIT, together with other participants. Although men reported experiencing support related to walking from peers in their EuroFIT group during the programme, some described how they sought sources of social support elsewhere after the programme ended (e.g. by participating in other walking football programme outside the club). Post-EuroFIT walking groups and other organised forms of PA were reported to be set up by clubs, coaches or participants in the Netherlands, England and Portugal, but not in Norway (despite efforts made by some coaches and some participants) which may partly explain the decline the walking values in Norway:
PX: We gathered a group of friends, who were already from EuroFIT. We got together, no one knew each other, and, and now we have an activity, weekly, [Others: mhm], in which, in fact, we even created a club [name of club] . . . everyone bought balls, everyone did things, rented a pavilion, hmm, which is [name of location], here in [name of city]. (POR415_12MFGD)
Despite the efforts from coaches, men in Norway reported that none of the clubs supported them in organising walking groups or other PA sessions for participants after the programme ended:
P4: . . . it was something you sort of looked forward to, I mean, coming here [to the club] on those Tuesdays to do some exercise. And I notice that, I missed that after we finished, then it’s kind of, it became like nothing, it just got empty. And then I felt like I hit . . . hit the wall a bit again. My steps went down. It wasn’t as fun anymore, and we were like just done with the project. It kind of felt like, that’s it. And for many of us, we don’t have a sports club, we don’t have any activity beyond the workplace where we’re at and work. And then it becomes so much harder [to keep things up]. (NOR312_12M-FGD)
Contrary to men in other parts of the EuroFIT programme, most men in Norway did not pledge themselves to the attempts of putting together walking groups or engaging in (walking) football. Although men in the Netherlands, England and Portugal seemed committed to these kinds of post-EuroFIT PA initiatives, they also described how a lack of time, rainy days, or cold and dark nights, especially during the winter season, could hamper their efforts to walk regularly or join walking groups after the programme. This was particularly so in Norway, where many of the men reported doing fewer walks after EuroFIT because of the cold, the snow or the icy roads:
P2: . . . nothing came out of it (trying to gather a walking group), because I met up, but it had become so slippery [on the ground] that we didn’t dare to walk, so we walked some along the river, but it was only a handful that turned up. (NOR311_12M-FGD)
Discussion
In this article, we have demonstrated how EuroFIT contributed to significant increases in self-reported walking among overweight, male football fans from baseline to 12-month follow-up in four countries, despite a large decline in Norway from post-programme to follow-up. Although the percentage of walking in relation to total self-reported PA did not change at 12-month follow-up, we found that most men were positive towards walking as a form of PA, were committed to post-EuroFIT PA initiatives and used different BCTs intended to sustain walking behaviours, but that some considered walking as a transitional activity towards more MVPA. These findings demonstrate that gender-sensitive healthy lifestyle interventions can succeed in increasing self-reported walking for men across cultural contexts using professional football clubs, and that perceptions of walking and use of BCTs suggest that most men across all countries embodied learning from the EuroFIT programme. Our findings support recent meta-analyses (e.g. Samdal et al., 2017) and qualitative studies reporting how goal setting, action planning, social support and self-monitoring can be helpful in sustaining daily steps through walking (e.g. Mitchell et al., 2018; Procter et al., 2014), but also how some of the techniques (e.g. goal setting) may require careful support from coaches to ensure continued use (Mitchell et al., 2018).
We found no significant difference between the intervention and control groups on the percentage of walking in relation to total PA at 12 months. These findings could be explained by how some men referred to walking as a transitional PA towards other more VPA in the qualitative analysis, but also the significant increases to self-reported MPA and VPA at post-programme and 12 months, which substantially increased the MET values for total PA. As reported in FFIT (Hunt et al., 2013) and elsewhere (South et al., 2017), some men also reported that engaging with walking in EuroFIT had enabled them to take part in more VPA or other forms of exercise later. Some men also questioned the usefulness of walking to improve their health in the programme. Although coaches in EuroFIT specifically promoted walking as a convenient and accessible PA to increase daily steps, the most frequent reasons for participating in EuroFIT were regaining or improving fitness (Bunn et al. 2023), which could suggest that some men who joined the programme came from a healthier part of the population. This might also help to explain why some men in EuroFIT valued walking less than other forms of exercise, as other studies have demonstrated how adults living with severe overweight and obesity prefer walking to other forms of MVPA (e.g. Hussien et al., 2022). As men were encouraged to set self-chosen, personally relevant goals related to PA, it is possible that the improved physical condition of some men after participating in EuroFIT made them prefer higher intensity PA instead of walking, which could also partly explain the increases in MPA and VPA at 12-month follow-up alongside walking.
We also found a large decline in self-reported walking values in Norway from post-programme to 12 months compared to the other countries. The findings of our qualitative analysis indicated that there was little or no help in organising walking groups or PA sessions (e.g. walking football) from Norwegian clubs compared to the other countries. As we found large differences in community PA programmes for adults, such as walking football, in Norway compared to the England and Netherlands (Røynesdal et al., 2021), this could also explain the lack of initiatives from these clubs post-programme. Alongside the icy winters in some parts of Norway, the lack of support from clubs seemed to affect men’s efforts towards walking and their commitment towards walking groups or other PA initiatives post-EuroFIT. As other studies have underlined how walking groups (Meads and Exley, 2018), and the interaction with others (Bell et al., 2023) and social support (Ball et al., 2017; Wahlich et al., 2017) through walking groups or other low-intensity PA groups can contribute to sustained PA, the lack of these initiatives could partly explain the decline in walking in Norway compared to the other countries.
Strengths and limitations
A key strength of this study lay in its rigorous mixed-methods design, which integrated secondary analyses of data from a large sample of men recruited to a multi-site RCT and the use of focus group discussions conducted across four countries. As all the researchers who interpreted the qualitative data were also involved in the primary data collection, this added trustworthiness to the interpretation of data. One limitation, however, was that we were occasionally unable to identify the intensity of PA reported in the qualitative data when participants discussed making sustained changes to their step count, as it was unclear whether they were referring to walking or other forms of PA. Consequently, these data segments were excluded from the analysis, which may imply that the descriptions presented do not fully reflect the broad array of men’s experiences of sustaining walking. Another limitation is that we did not perform sensitivity analyses of missing values in the IPAQ data and that there was likely social desirability bias with regard to self-reported PA data, especially VPA, which could have led to an overestimation of the intervention effects. However, the use of qualitative data helped verify some of the findings in self-reported PA data.
Conclusion
Overall, the EuroFIT programme succeeded in helping overweight, male football fans increase self-reported walking at 12-month follow-up across four countries. Most men found that walking was a convenient form of PA that was perceived as useful across cultural contexts in increasing daily steps, whereas others considered walking a stepping stone towards more intensive PA. Although the percentage of walking in relation to total PA remained the same for participants in both groups, the EuroFIT programme helped men to integrate walking into their daily lives using BCTs.
Supplemental Material
sj-docx-1-hej-10.1177_00178969251323509 – Supplemental material for Changes to men’s walking and the contribution of walking to self-reported physical activity in the EuroFIT programme
Supplemental material, sj-docx-1-hej-10.1177_00178969251323509 for Changes to men’s walking and the contribution of walking to self-reported physical activity in the EuroFIT programme by Øystein B Røynesdal, Eivind Andersen, Hugo V Pereira, Sally Wyke, Cindy M Gray, Judith GM Jelsma, Kate Hunt, Nanette Mutrie, Marlene N Silva, Marit Sørensen, Glyn C Roberts, Hidde P van der Ploeg and Femke van Nassau in Health Education Journal
Supplemental Material
sj-docx-2-hej-10.1177_00178969251323509 – Supplemental material for Changes to men’s walking and the contribution of walking to self-reported physical activity in the EuroFIT programme
Supplemental material, sj-docx-2-hej-10.1177_00178969251323509 for Changes to men’s walking and the contribution of walking to self-reported physical activity in the EuroFIT programme by Øystein B Røynesdal, Eivind Andersen, Hugo V Pereira, Sally Wyke, Cindy M Gray, Judith GM Jelsma, Kate Hunt, Nanette Mutrie, Marlene N Silva, Marit Sørensen, Glyn C Roberts, Hidde P van der Ploeg and Femke van Nassau in Health Education Journal
Footnotes
Acknowledgements
We thank participants and coaches in the EuroFIT RCT. We thank Noa Schrier for her contributions to the initial codebook generation and colleagues in the EuroFIT consortium who contributed to data collection or delivering the trial across the four countries. We thank Christopher Bunn and Lisa McAuley for their work coordinating the English arm of the EuroFIT RCT, and Allan Gray, Frank Erik Abrahamsen, Heather Morgan, Irene van de Glind and Marta Antunes for their contributions to qualitative data collection in the EuroFIT RCT.
Data availability
Data from the EuroFIT RCT are available for secondary analysis. Applications to access the data can be made by contacting John Cleland, Director of the Robertson Centre for Biostatistics and Glasgow Clinical Trials Unit (
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: this work was supported by the European Union’s Seventh Framework Programme for research, technological development and demonstration under Grant Agreement Number 602170.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.