
Abstract
Objective:
Brisk walking helps postmenopausal women to maintain body weight and fat mass losses as well cardiorespiratory fitness (CRF) and to feel better. However, these long-term benefits have not been fully examined. The aims of this study were to compare the effects of a 2-year follow-up with those of a 4-month walking programme on body composition, resting blood pressure (BP), CRF and perceived health of 248 sedentary postmenopausal women (60 ± 5 years) with overweight-to-moderate obesity (body mass index, BMI, 30 ± 4 kg/m2).
Method:
From the study-population, 196 women engaged in an outdoor walking programme consisting of three sessions of 45 minutes/week at 60% of their heart rate reserve (initially exercised, IEx, group), and another 52 formed the initial control group (ICo). Ninety-one IEx and 18 ICo women were re-examined 2 years later, for all outcomes.
Results:
In IEx women, decreased body weight, fat mass and BP versus the increased CRF (.0001 < p < .001) as well as improvements in four on six items of perceived health (.0001 < p < .05) were maintained at follow-up. In ICo women, reduced BP and improved perceived healthy balanced diet were the only benefits at follow-up (p < .05). Of the 91 IEx women, 70 remained physically active (60 minutes/week), and 46 of them engaged in physical activity more than 150 minutes/week. In ICo women, 16 became physically active (60 minutes/week), while 9 of them reached 150 minutes/week.
Conclusion:
The regular practice of brisk walking in greenspaces could thus be considered a useful health education strategy for middle-aged women.
Keywords
Introduction
Menopause, which is often characterised by body weight and abdominal fat mass expansion, is generally accompanied by numerous adverse effects (Hulteen et al., 2023). An increase in abdominal visceral fat mass and its related metabolic complications (Diniz et al., 2017), as well as a decrease in lean mass, have frequently been reported in postmenopausal women (Juppi et al., 2020). For most women, menopause is also related to a decreased health-related quality of life (HRQoL), sleep disturbances and a number of psychological disorders (Bromberger et al., 2011; Jones and Sutton, 2008).
Habitual physical activity is known to improve numerous indicators of health and HRQoL, prevent and treat conditions that typically occur in mid-life (Mendoza et al., 2016). In this regard, the World Health Organization (WHO, 2020) guidelines recommend at least 150 to 300 minutes/week of moderate-intensity-aerobic physical activity (PA) for adults and older adults to control body weight and fatness and to improve cardiorespiratory fitness (CRF). Among different types of exercise interventions, brisk walking is considered the most common and feasible form of sustainable dynamic continuous aerobic exercise at low-to-moderate intensity for sedentary individuals with overweight or obesity, because of its safety, popularity and accessibility to all members of the public including older adults (Hamer and Chida, 2008; Lee and Buchner, 2008). Research in France has shown that health benefits appear as early as 78 minutes/week of outside walk and increase with adherence to PA, in initially sedentary, postmenopausal women with moderate obesity (Garnier et al., 2015a). Furthermore, a meta-analysis based on eight clinical trials revealed that weight loss interventions based on a reduced-energy diet with exercise were associated with moderate weight loss at 6 months and its maintenance at 1-year follow-up (Franz et al., 2007). Another systematic review and meta-analysis based on 45 randomised controlled trials has shown that behavioural interventions including both diet and PA produce small benefits with respect to weight loss maintenance after 2 years, although the authors did not examine CRF and psychological effects (i.e. mental health) (Dombrowski et al., 2014).
That aerobic continuous training may promote modest weight loss (−2 kg) should also be highlighted as numerous health benefits derive from such programmes even in the absence of weight reduction (Swift et al., 2014). In addition, exercise alone does not necessarily improve weight loss and/or contribute to weight loss-maintenance mainly because of large individual differences in participants’ adiposity, and variability in terms of exercise intensity, type and duration (Cox, 2017). However, focusing on improvement in CRF and PA practice rather than on body weight loss seems to be a better strategy for obesity treatment, as recently suggested by Gaesser and Angadi (2021). Indeed, ‘the mortality risk associated with obesity is largely attenuated or eliminated by moderate-to-high levels of CRF and/or PA, and increases in these variables are consistently associated with greater reductions in mortality risk than is intentional weight loss’ (Gaesser and Angadi, 2021).
The theoretical foundations of this study lie in the field of perceived health, which can be summarised in terms of ‘what people say about their health’ (Hunt et al., 1980; Kaplan and Camacho, 1983), and HRQoL, which refers to well-being. Although there is no standard definition, HRQoL is accepted as a subjective, multidimensional assessment of the physical, psychological and social domains of health (Blissmer et al., 2006). Engagement with long-term and regular PA for inactive women is a great challenge to maintain weight loss and benefits in HRQoL initially observed following exercise. Adherence rates for exercise programmes ranged from 50% to 80% during the first 6 months and fell less than 50% at 1-year follow-up (Koeneman et al., 2011). Consistent improvements in psychological outcomes such as body image and HRQoL (especially vitality) have been shown to be closely related to weight change (Lasikiewicz et al., 2014). It is thus of importance to improve our understanding of changes in both objective and subjective responses following an aerobic exercise programme such as brisk walking. We hypothesised that initially exercised women would maintain their body weight loss as well improvements in CRF and perceived health, compared with controls, at 2-year follow-up. The main goal of this study was to examine the effects of brisk walking on body composition, physical fitness, and perceived health, of initially sedentary, healthy, and postmenopausal women with moderate obesity, 2 years subsequent to the initial 4-month walking programme. A secondary objective of the study was to examine women’s engagement in PA and the nature of exercise at 2-year follow-up.
Methods
Participants
Women were recruited through an announcement in local newspapers in Toulouse (France). From 350 postmenopausal women (amenorrhoea for at least 12 months), 50 to 65 years old, with overweight-to-moderate obesity (BMI, 29–35 kg/m2) assessed for eligibility, 270 met the following inclusion/exclusion criteria. Women had to be physically inactive (exercising less than 30 minutes/week), non-smokers, and moderate or non-consumers of alcohol (0–2 drinks/day) and caffeine (0–3 cups of coffee/day). Their body weight had to be stable (weight change < 2 kg) in the year before enrolment. None had any identified disease (cardiomyopathy, type 2 diabetes [T2D], endocrine disorders, or renal and hepatic dysfunctions) or orthopaedic limitations that would affect participation in PA. Women on medication that could potentially influence the outcomes of this study (beta-blockers, sympathomimetics, cholesterol lowering drugs including statins, corticosteroids other than inhalation products, antihypertensive drugs, thiazide diuretics, thyroxine for which a dose change had occurred during the last 6 months or was expected during the study, neuroleptics, and antidepressants including serotonin reuptake inhibitors) were excluded. Perimenopausal women (with an irregular menstrual cycle in the past 6 months) were also excluded.
Study design
The study design was approved by the institutional review board of the Fédération Française d’Education Physique et de Gymnastique Volontaire (FFEPGV). Participants gave their written informed consent form to participate in this study, in conformity with the Declaration of Helsinki of 1975, as revised in 2000.
The 4-month walking programme, which was planned according to WHO (2020) guidelines, consisted of 3 × 45 minutes/week non-consecutive sessions, at approximately 60% of heart rate reserve (HRR) where HRR is maximal heart rate (HR) minus the resting HR. Maximal HR was calculated by the following equation: 220 – age, where age is expressed in years. Walking HR was calculated as a percentage HRR + resting HR (Karvonen et al., 1957). Two weekly walking sessions were supervised by an FFEPGV exercise leader. The third weekly unsupervised session took place according to participants’ preferences on a pavement, the street, a forest trail or in a park. Participants’ assiduity was recorded in an exercise logbook, and their HR was continuously recorded using an HR monitor (Polar FS1, Polar Electro, Kempele, Finland) during each walking session (either supervised or not) to ensure compliance with the walking intensity. Monitoring HR allowed us to control the exercise intensity and to document the specific amount of exercise undertaken during each session. The mean number of missed supervised versus unsupervised sessions generated an adherence rate of 79% ± 17% versus 76% ± 17% (M ± SD), respectively (Garnier et al., 2015a). Missing sessions were mainly attributed to vacation, illnesses and other commitments that might interfere with participants’ availability to travel to the training centre for an exercise session. Mean walking HR intensity, which averaged 58% ± 7% HRR (M ± SD), was close to the 60% HRR planned in our intervention (Garnier et al., 2015a). Women were asked to maintain current lifestyle habits during the 4-month walking programme. Women who exercised increased their daily energy expenditure but did not modify their daily energy intake during this period (Garnier et al., 2015b). Control participants did not report any change in their daily energy balance.
As shown in Figure 1, of the 270 women meeting the inclusion criteria, 200 participated in the 4-month walking programme while 70 remained inactive during this time. Data were available for 248 participants. Of these, 196 women participated in the walking programme (initial exercise, IEx, group) while 52 formed the initial control group (ICo).
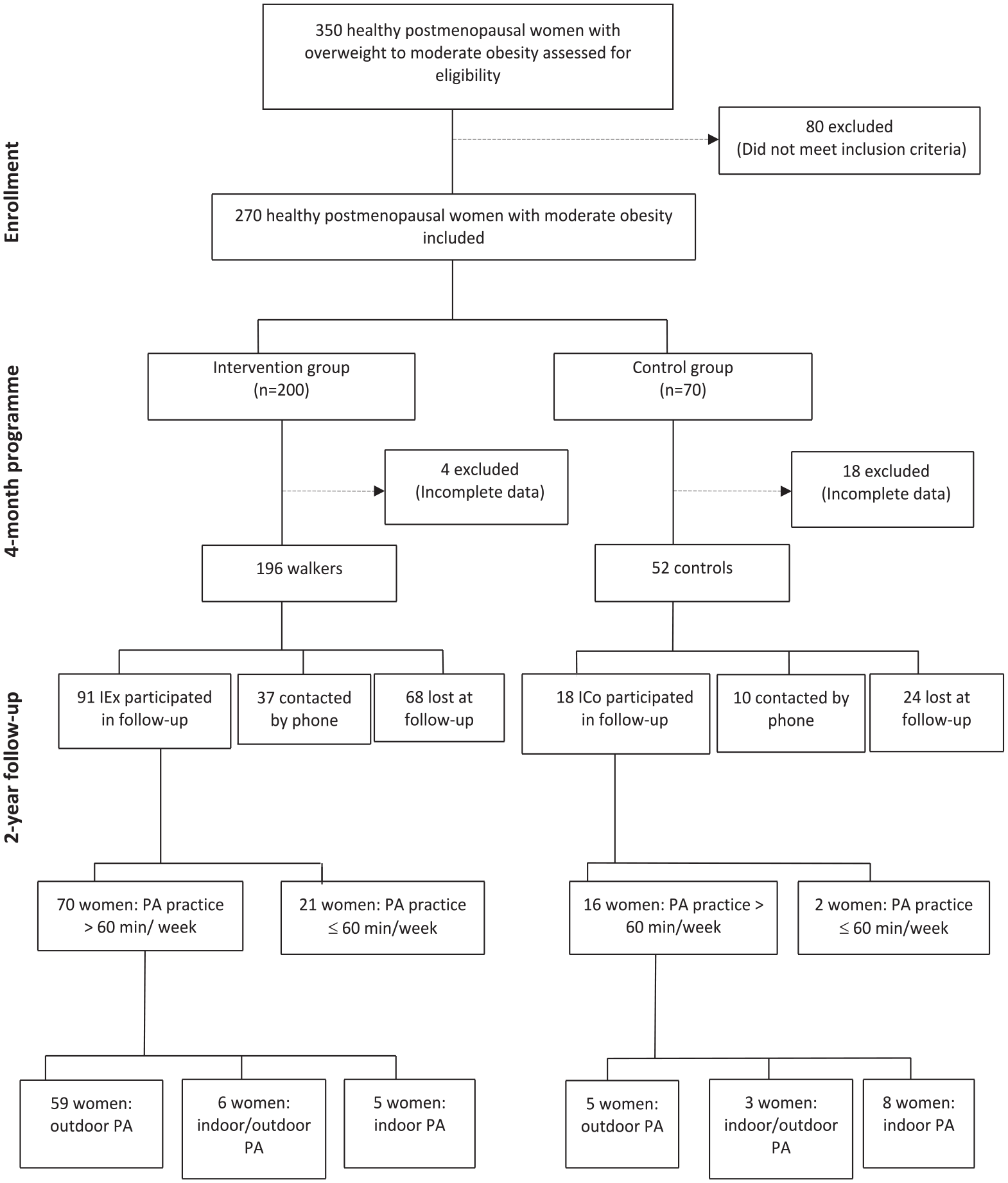
Participants’ flow diagram.
At the end of the 4-month study period, the IEx group was given an HR monitor (Polar FS1, Polar Electro, Kempele, Finland) as an incentive to continue walking, while the ICo group was offered the opportunity to participate in a walking programme or in gym sessions supervised by FFEPGV exercise leaders, for a 4-month period. Ninety-one IEx and 18 ICo women were followed up 2 years later, while 68 IEx and 24 ICo women were lost to follow-up. Thirty-seven IEx and 10 ICo women therefore answered a short questionnaire by phone.
Measurement
The following measurements were made before and after the 4-month study-period as well as 2 years later.
CRF was assessed by the 2-km walking test with the equation used to predict V̇O2max in women being the following: V̇O2max (mL O2/kg/min.) = 116.2 – 2.98 (time) – 0.11 (HR) – 0.14 (age) – 0.39 (BMI), where time is the elapsed time for a walk in minutes, HR was the value at the end of the walk (beats/min), age is expressed in years, and BMI was expressed in kilogrammes per metre squared (Laukkanen et al., 1992). CRF measurements were made by the same FFEPGV exercise leaders, for both study-periods (Garnier et al., 2015a).
Body weight and height were measured with participants in light clothing, without shoes and in a standing position, looking straight ahead, with shoulders and buttocks against the wall, as well as feet joined and arms hanging down on both sides. BMI was calculated as the ratio of weight (kg) to height squared (m²). Waist girth was measured at the narrowest circumference of the trunk, using a graduated flexible tape when subjects were in standing position. Fat mass and lean mass were determined by a standard bioelectrical impedance technique (Bodystat 1500, Bodystat Ltd., Douglas, UK). All measurements were made by the same operator, at rest, in the morning. Anthropometric and body composition measurements were undertaken in duplicate, and then averaged (Garnier et al., 2015a).
Systolic and diastolic blood pressures (SBP and DBP, respectively) were measured when participants were in a semi-recumbent position with the arms relaxed and supported, after a rest period of at least 10 minutes (NAIS, Blood Pressure Unit). Measurements were performed in duplicate, at 5-minute intervals, and then averaged (Garnier et al., 2015a).
Perceived health was assessed by means of a self-administered short questionnaire specifically designed to explore lifestyle, physical activity, and psychosocial orientation at both study-periods. Six sets of issues were investigated: (1) perceived physical fitness; (2) perceived ideal weight; (3) perceived healthy balanced diet; (4) perceived sleep quality; (5) perceived stress level; and (6) perceived general health. A 10-point Likert-type scale from 1 (not at all) to 10 (very well) was used to assess each item (Garnier et al., 2013).
A preliminary study conducted with a sample of postmenopausal women showed a good reliability for five out of six items of the Short Health Perceived Questionnaire (SHPQ) (Garnier et al., 2013). The intraclass correlation coefficient (ICC) was excellent for perceived ideal weight, physical fitness, stress level and general health (ICC ranging from .82 to .89; p
The SHPQ is available in both French and English language versions, copies of which are available from the corresponding author upon request.
At 2-year follow-up only, all women answered additional questions related to whether participants continued to walk regularly at the end of the 4-month walking programme, and if so, what was the frequency (times/week) and the intensity (perceived effort evaluated through a Likert-type scale) of their walking; whether participants were active or sedentary during their hobbies; and whether participants practised other physical activities and/or sports (further details are available from the corresponding authors upon request). As some women could not participate to follow-up, they agreed to answer a few questions by telephone related to their body weight, as well as their perceived physical fitness, healthy balanced diet and general health.
Statistical analyses
Sample size calculations were performed using predicted changes for one of the most important variables in the study, that is, the VO2max. In a population close to our own in terms of age and BMI, Lynch et al. (2002) reported a baseline VO2max of 22.2 ± 3.2 mL/ minutes/kg (M ± SD). Using a one-tailed model, type 1 alpha error = .05, power = .90, and targeting a 10% increase in VO2max (i.e. +2.23 mL/minutes/kg), in IEx compared with ICo women after the 4 month walking programme, calculations recommended a minimum of 36 participants for each group. Allowing for potential drop out at 2-year follow-up, we therefore believe that the number of IEx and ICo women (Figure 1) was sufficient for our purpose. A one-way analysis of variance (ANOVA) was performed to test between-group differences in baseline characteristics. Comparisons of perceived health items, anthropometry, body composition and CRF before and after the 4-month study-period, and 2 years later, between IEx and ICo women were made using a two-way ANOVA with repeated measures (pre- vs post-intervention vs follow-up), in line with the general linear model procedure. When an ANOVA was found significant, post hoc simple test effects were used to assess which conditions were statistically different (body weight at pre- vs post-intervention and 2-year follow-up, for example). Relative responses to the intervention (%) mentioned in the discussion were calculated as follows: (post-intervention – pre-intervention/pre-intervention) × 100 and (follow-up – pre-intervention/pre-intervention) × 100. All analyses were conducted using SAS statistical software (SAS Institute, version 9.1, Cary, NC, USA), and statistical significance was set at p ⩽ .05.
Results
To examine whether differences existed in individuals’ characteristics at baseline (online Supplemental Table A) and in response to the 4-month walking programme (Online Supplemental Table B), the cohort was divided into three subgroups, according to whether women participated in the 2-year follow-up, were contacted by phone, or lost at follow-up. As shown in online Supplemental Table A, no between-group differences were observed at baseline, for age, anthropometry, and body composition, resting BP and CRF, nor for most items in the perceived health questionnaire with the exception of perceived ideal weight. Online Supplemental Table B reveals that changes observed following the 4-month walking programme did not differ between IEx women who participated in the 2 year follow-up, were contacted by phone, or those lost at follow-up.
As depicted in Table 1, in IEx women, the decrease in body weight and fat mass observed after the 4 month walking programme persisted 2 years later (.0001 < p < .001), in contrast to the reduction in BMI and waist girth. CRF increase as well as both SBP and DBP decreases were also maintained after 2 years (p < .0001). The increase in perceived physical condition at the 4 month study-period was not maintained whereas the one in ideal weight persisted 2 years later (p < .05). Furthermore, the better perceived healthy balanced diet after 4 months was maintained (p < .0001) in contrast to perceived improved sleep quality which did not persist after 2 years. Both perceived stress levels and general health noted at the 4 month study-period remained higher 2 years later (p < .05).
Body composition, cardiorespiratory fitness, and perceived health between initially exercised and control women, after a 4-month walking programme and at 2-year follow-up.
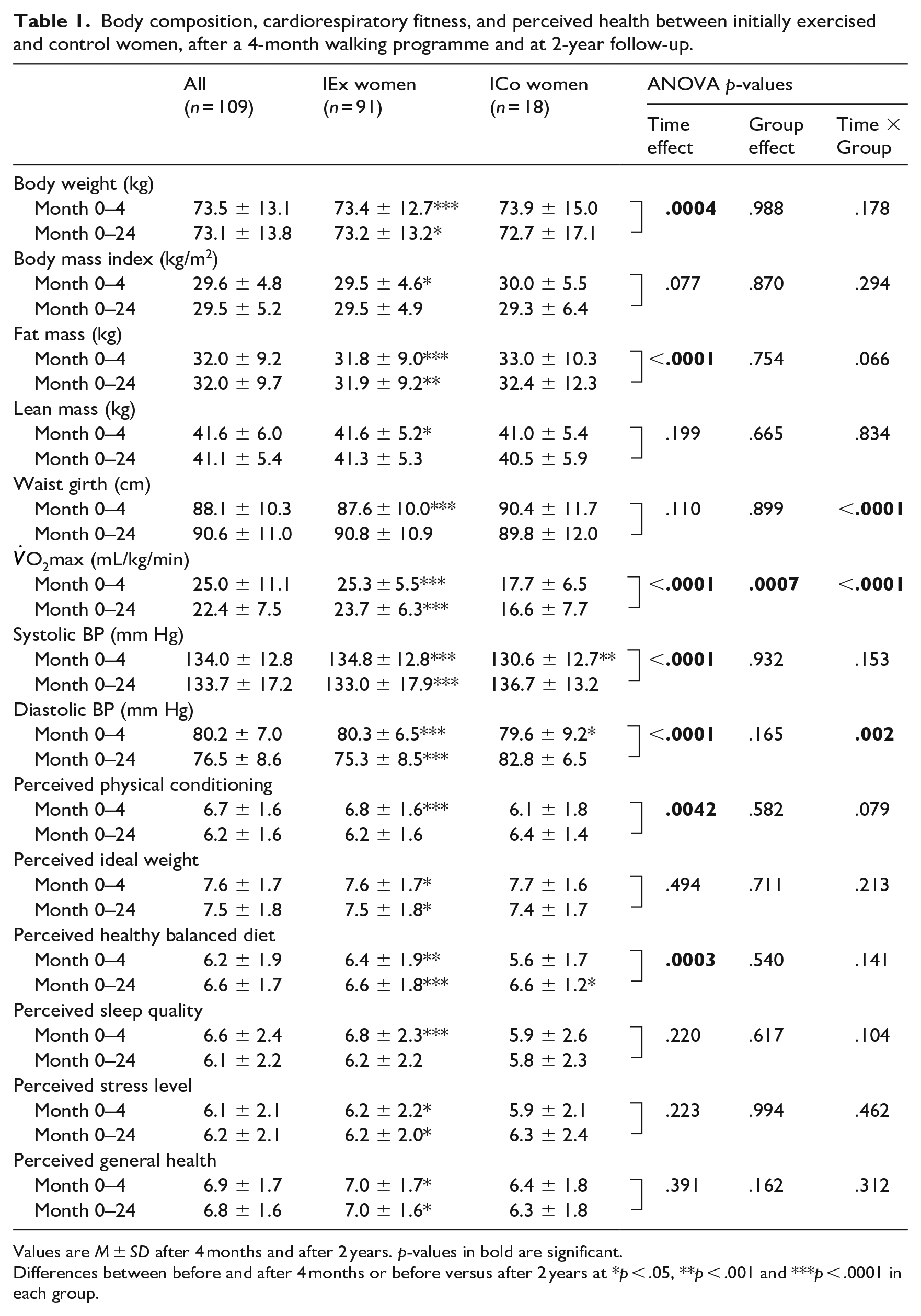
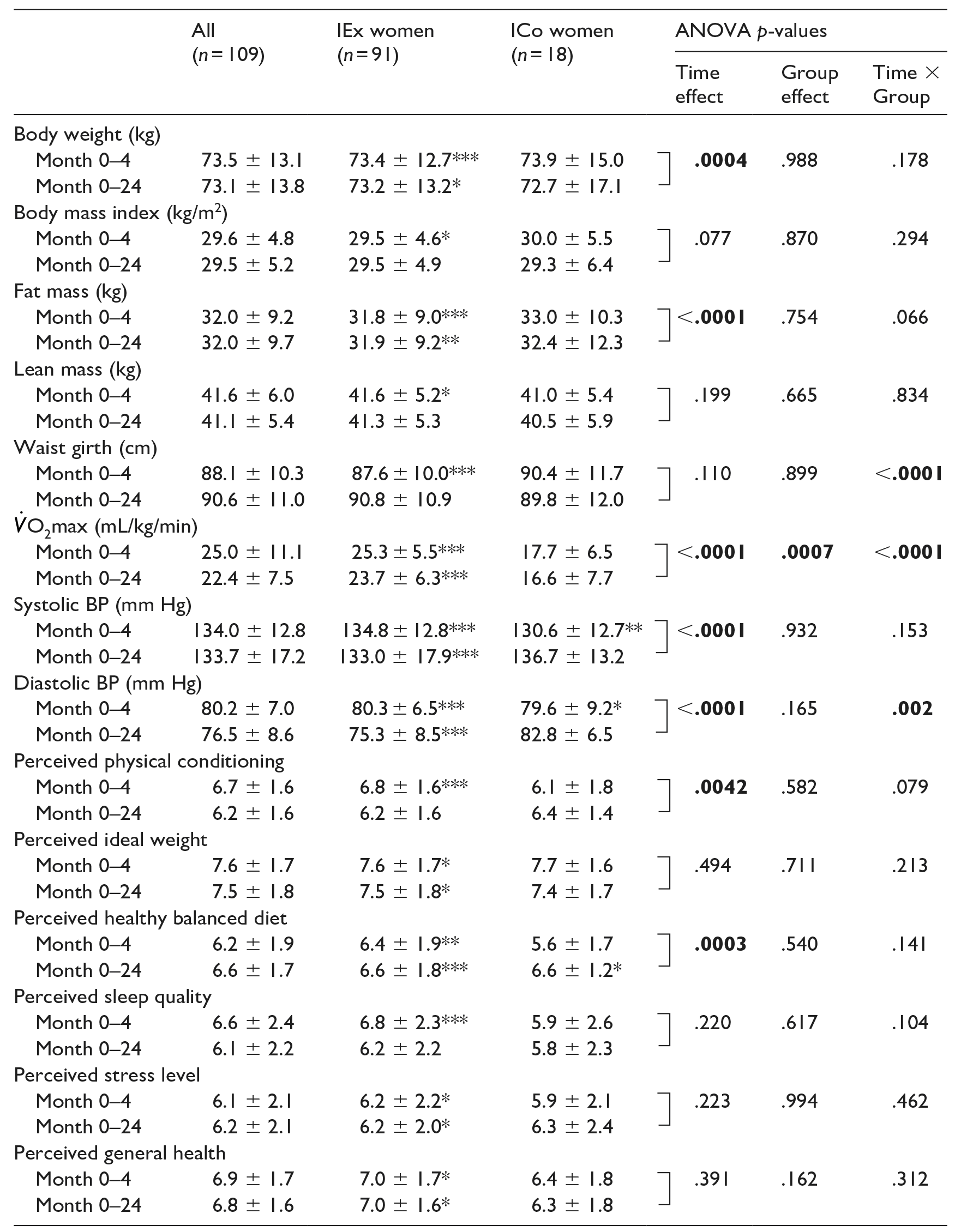
Values are M ± SD after 4 months and after 2 years. p-values in bold are significant.
Differences between before and after 4 months or before versus after 2 years at *p < .05, **p < .001 and ***p < .0001 in each group.
In ICo women, no differences were observed after the 4 month study-period and at 2 year follow-up in body composition and CRF, except for decreases in SBP and DBP after 4 months. In addition, an improvement in perceived healthy balanced diet was the only benefit observed at 2 year follow-up (p < 0.05).
Results from the additional questions asked about PA engagement 2 years later showed that in the IEx group, 70 women continued to be physically active at least 60 minutes/week (Figure 1), and among them, 46 exercised more than 150 minutes/week (data not shown). Of these 70 participants, 59 continued to walk regularly—among them four participants combined walking and jogging (i.e. outdoor PA) (data not shown), while six women linked exercising (i.e. indoor PA) consisting of warm-up, full body exercise, coordination, balance, stretching (90 minutes/week) with walking (45 minutes/week) and five women practised exercising only (120 minutes/week). Among the ICo women, 16 became physically active and practised at least 60 minutes/week (Figure 1) and nine of them reached 150 minutes/week (data not shown). Among these 16 ICo women, five walked regularly while three connected exercising with walking (120 minutes/week for each activity) and eight women practised exercising, only (120 minutes/week) (Figure 1).
Discussion
To the best of our knowledge, this is the first study to examine the effects of a brisk walking programme on both objective (CRF, body composition and resting BP) and subjective variables (perceived health items) as well as on PA engagement 2 years after the initial 4-month walking programme, in healthy, initially sedentary postmenopausal women with overweight to moderate obesity. Our data showed that body weight loss, CRF and perceived health improvements persisted at 2 year follow-up, in IEx women. The low difference between baseline and 2 year assessment in the ICo group could be due to the fact that the PA practice of the latter was probably less regular, performed at a lower walking intensity and not as long (less than 45 minutes) as that of the IEx group.
In IEx women, the body weight (−1.2 kg) loss observed after 4 months fits well with the values of −1.4 kg and −1.1 kg reported, respectively, by Murtagh et al. (2015) and Gao et al. (2016), in peri- and post-menopausal women. The CRF increase (+7 mL/kg/min) of our participants was greater than the one observed by Murtagh et al. (2015) (+3.0 mL/kg/min) or Oja et al. (2018) (+4.9 mL/kg/min). In addition, reductions in resting SBP and DBP (−8.8 and −5.7 mm Hg, respectively) were higher than those from the Murtagh et al.’s (2015) and Oja et al.’s (2018) meta-analyses. Differences between our results and those from the two latter meta-analyses could be partly due to lower CRF and BP in our participants. Improvements in perceived physical conditioning (+19%), ideal weight (+5%), healthy balanced diet (+16%), sleep quality (+17%), stress level (−12%) and general health (+9%) were aligned with the associations observed between increased walking and lower anxiety scores (Kelly et al., 2018), thus suggesting that regular PA practice such as brisk walking leads to better sense of well-being.
At 2-year follow-up, 77% of IEx women continued to engage in PA of at least 60 minutes/week, and among them, 93% exercised outdoors in greenspaces. After 2 years, the CRF increase (+5.7 mL/kg/min) and the body weight (−1.3 kg) and fat mass (−1.4 kg) losses were maintained but not the waist girth reduction. Similarly, decreases in SBP and DBP (−10.7 and −11.0 mmHg, respectively) were still observable. A few studies have examined weight loss maintenance 2 years later without any intervention: (1) Unick et al. (2015) showed that weight loss within the first 2 months of a lifestyle intervention is predictive of long-term weight loss success (i.e. 8 years later) in participants with T2D and (2) Jakicic et al. (2008) reported a weight regain after 24 months of 50% weight loss, during the initial 6 months of an intervention combining diet and PA, in 21- to 45-year-old women with obesity. Dombrowski et al. (2014) noted that behavioural interventions targeting diet and PA are moderately effective in limiting weight regain in adults after initial weight loss at a follow-up of 24 months, while Swift et al. (2014) highlighted the important role of PA in weight loss maintenance after a successful weight-reducing programme. More recently, Gaesser and Angadi (2021) have emphasised the importance of considering PA and CRF as variables of interest in the management of obesity, as both are well known to reduce the mortality risk associated with obesity.
Perceived physical conditioning (+9%), ideal weight (+6%), healthy balanced diet (+21%), stress level (−13%) and general health (+9%) all improved in IEx women. Our data are in good accordance with the enhanced emotional well-being observed after walking in greenspaces in Barton et al.’s (2009) study, and the improved long-term well-being noted in Pasanen et al.’s (2014) work which showed that repeated exercise in a greenspace was related to improved long-term well-being, compared with similar training modalities in indoor or outdoor built environments.
In addition to various health benefits, our study shows the long-term commitment to PA of a group of sedentary postmenopausal women with obesity. This can perhaps be explained by the period of menopause being one in which many women modify their life habits (Mendoza et al., 2016), the nature of PA involved such as walking on forests, trails or parks close to a participant’s home (Kelly et al., 2018), the development of relationships with others through walking (Morris et al., 2019) and/or the social benefits associated with walking in greenspaces (Eigenschenk et al., 2019). In this regard, the social relationships developed between participants through the regular practice of brisk walking and the support of a non-competitive sport federation, should be highlighted, as most women maintained a physically active lifestyle at 2-year follow-up. Finally, because of its benefits for the physical, mental and social health of participants, this brisk walking programme should be considered as having the potential to contribute to development of healthy lifestyle habits.
Strengths and limitations
The fact that all the measurements were carried out by the same investigators and in similarly controlled conditions is a major strength of this study. In addition, our attrition analyses did not reveal statistically differences in key variables between dropouts and completers (Supplemental Table B). As the training programme took place outdoors, and near to participants’ home, it likely has high ecological validity and the activities could be easily integrated into daily life habits of many individuals.
Several limitations should be noted however. First, as our obesity treatment programme focused on aerobic PA, participants recruited needed to be in good physical condition in order to perform regular walking, 3 days/week, for 4 months. Thus, the women selected for our study were relatively healthy and probably represented a group of volunteers more health-conscious and motivated to practise PA and lose body weight. Second, accurate determination of alcohol consumption is a well known problem in nutritional research so could have been underreported by participants. It therefore seems realistic to suggest that our findings cannot be generalised to the overall population, either to men or to premenopausal women. Third, the fact that only 109 women (i.e. 44%) were studied at follow-up is worthy of comment, since this rate is lower than those reported by Kaukua et al. (2003), Blissmer et al. (2006) and Jepsen et al. (2015), at 67%, 63% and 50%, respectively. Our relatively low rate may be partly explained by the fact that women did not receive any incentive to participate in the follow-up. Fourth, the reliance on self-report measurements concerning the weekly frequency of walking or other PA modalities and the lack of control for dietary habits during the 2 year follow-up could also be criticised. Finally, the fact that the investigator was not blind to group allocation may also have introduced a bias.
Conclusion
Data from this study demonstrate the long-term positive effects of a brisk walking programme including the maintenance of body weight loss, as well as improvements in physical fitness and perceived health at 2-year follow-up in a ‘real world situation’. Whether these benefits will still be observed 5 or 10 years later remains to be examined. As a health education strategy, however, integrating sedentary middle-aged women into an active social network through the regular practice of brisk walking in a green environment could help them develop a long-term engagement in PA.
Supplemental Material
sj-docx-1-hej-10.1177_00178969241269016 – Supplemental material for Two-year follow-up of a brisk walking programme on fitness, perceived health and physical activity engagement in postmenopausal women
Supplemental material, sj-docx-1-hej-10.1177_00178969241269016 for Two-year follow-up of a brisk walking programme on fitness, perceived health and physical activity engagement in postmenopausal women by Sophie Garnier, Sandra Joffroy, Bernard Thon, Gérard Auneau and Pascale Mauriège in Health Education Journal
Supplemental Material
sj-docx-2-hej-10.1177_00178969241269016 – Supplemental material for Two-year follow-up of a brisk walking programme on fitness, perceived health and physical activity engagement in postmenopausal women
Supplemental material, sj-docx-2-hej-10.1177_00178969241269016 for Two-year follow-up of a brisk walking programme on fitness, perceived health and physical activity engagement in postmenopausal women by Sophie Garnier, Sandra Joffroy, Bernard Thon, Gérard Auneau and Pascale Mauriège in Health Education Journal
Footnotes
Acknowledgements
The cooperation of women who participated to this walking programme is greatly appreciated. Special thanks go to exercise leaders involved in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: this study was supported by the Conseil Régional Midi-Pyrénées and the FFEPGV. The funders had no role in the design and conduct of the study; data collection, project management, analysis, the interpretation of the data; or the preparation, review and approval of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.