
Abstract
Introduction
Osteoarthritis is the most common form of arthritis and the leading cause of pain, loss of mobility, and disability worldwide (O'Neill et al., 2018). The goal of contemporary management for patients with osteoarthritis remains control of the pain and improvement in function and health-related quality of life. However, for severe hip osteoarthritis, total hip replacement (THR) is the recommended intervention (American College of Rheumatology Subcommittee on Osteoarthritis Guidelines, 2000). For most people, total joint replacement is a highly successful procedure that may last the rest of their lives. It provides good pain relief and restores mobility (Günther et al., 2021; Shan et al., 2014) but may fail to restore full physical function (Nilsdotter et al., 2003; Okoro et al., 2012; Trudelle-Jackson et al., 2002). Impairments that can persist for 1 year following the THR operation include decreased muscle strength and postural stability on the replaced hip side (Trudelle-Jackson et al., 2002), especially when performing daily living activities that demand increased muscle strength (Winther et al., 2020). Other functional limitations that can persist after THR include reduced walking speed and ability to climb stairs (Judd et al., 2013). This study examines the improvement trajectory of functional ability—self-care and mobility—from presurgery to postrehabilitation.
Positive psychology recognizes human strengths—positive psychological variables, such as courage, honesty, positive affect, optimism, and hope, that enhance coping with stressful situations and act as buffers against mental illness (Seligman & Csikszentmihalyi, 2000). Recently, increased attention turned to identifying positive psychological variables that contribute to better rehabilitation outcomes (Kortte et al., 2012). However, only a few studies have identified the positive psychosocial predictors associated with functional recovery following elective THR surgery.
Systematic reviews on the effects of psychological factors on THR outcomes included mainly mental health, depression, anxiety, and patient expectations, and no conclusion was reached because the results were limited and sometimes conflicting (Vissers et al., 2012). Optimism at admission to an acute rehabilitation facility following an elective hip or knee replacement did not correlate with functional ability (per the FIM® motor domain of Functional Independent Measure [mFIM]) at discharge among adults aged 39 to 93 years (Waldrop et al., 2001). Similarly, hope measured 1 month prior to a knee or hip replacement surgery was not predictive of functional recovery 6 weeks postsurgery (Hartley et al., 2008). To our knowledge, positive affect, defined as the self-perception of the experience of emotional contentment and happiness (Clark et al., 1989) related to a specific object or situation (Fredrickson, 2004), has not been examined among THR patients.
The International Classification of Functioning Disability and Health provides a holistic view of people's activity and participation that bio-psycho-social factors can influence (World Health Organization, 2001). Thus, many studies have documented body structure and function as physical factors limiting successful rehabilitation outcomes, such as range of motion, strength, postural stability, pain pre- and post-operation, and musculoskeletal comorbidities (Judd et al., 2013; Nilsdotter et al., 2003; Smith et al., 2012). Negative emotional functions, such as negative preoperative emotions, anxiety, and depressive symptoms, were also well examined and documented (Benditz et al., 2017; Duivenvoorden et al., 2013; Stark et al., 2016). However, only a few studies examined the role of positive emotional functions in acute rehabilitation outcomes among older adults after THR.
Hence, this study adopts a broader perspective incorporating emotional functions, referred to herein as positive affect, as well as body structure and function, to expand our understanding of possible modifiable factors that may inform the rehabilitation practice (Figure 1). This study's objectives are to (a) examine the improvement trajectory of functional ability, including activities of daily living (ADL) functioning and mobility, from presurgery of elective THR to postrehabilitation and (b) determine which physical and psychological factors at admission would predict functional ability at discharge and length of stay in rehabilitation (LOS). In light of the literature, we hypothesized that higher positive affect levels would contribute to better rehabilitation outcomes.
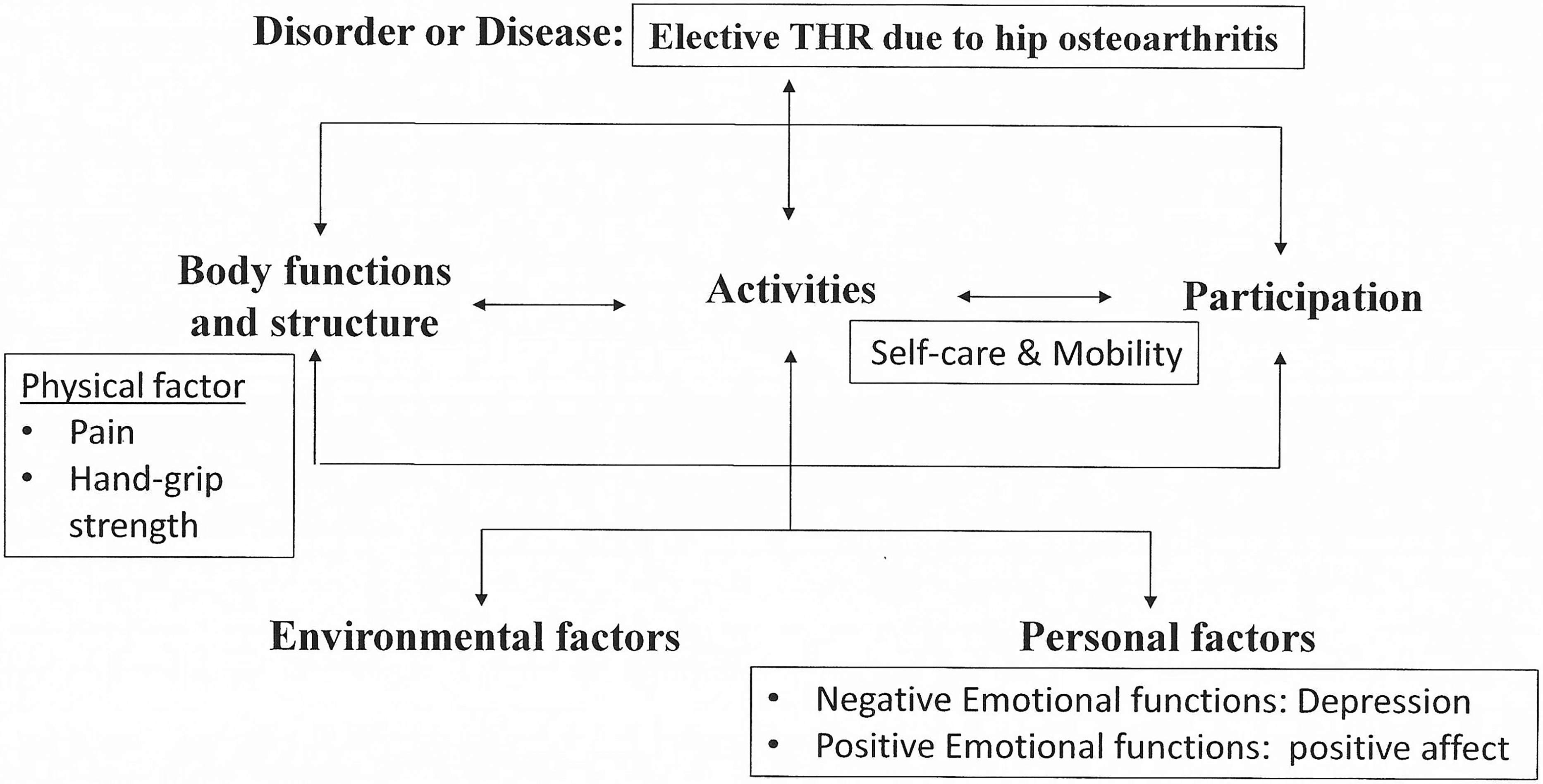
Study variables in the International Classification of Functioning Disability and Health (WHO, 2001) frame of reference.
Methods
Participants and Procedure
The institutional review board, Helsinki committee (0511-13-RMC) of the Rabin hospital approved this prospective cohort study. Thirty participants who sustained a THR due to hip osteoarthritis participated. They were consecutively recruited from the Beit Rivka Geriatric Medical Center, a university-affiliated inpatient rehabilitation center in Israel that receives postacute patients from nearby hospitals. The inclusion criteria for the study were aged 65 years and older who had been able to leave their homes independently before the surgery, a score of 24 or higher on the Mini Mental State Examination (MMSE; Folstein et al., 1975) upon admission, and a signed informed consent form. We excluded from the study patients admitted from nursing homes or had neurological impairments or histories of metastatic cancer. Other exclusion criteria included a nonambulatory status prior to surgery, non-weight-bearing status postsurgery, or other medical complications during rehabilitation. These broad exclusion criteria were established to prevent potential influences on the outcomes and psychological factors.
The researcher identified the hospitalized patients who fit the criteria and invited them to participate in the study. Those who agreed signed consent forms and completed the research questionnaires. The mean number of days between the surgery and arrival at the rehabilitation was 5.23 days (SD = 2.63), and the mean LOS was 25.63 days (SD = 8.33). The multidisciplinary team provided medical, nursing, physical therapy, occupational therapy, and social work interventions for all participants. Rehabilitation care included physiotherapy for improved transferring, walking the length of a room, climbing stairs, equilibrium, and joint range of motion. In addition, patients received occupational therapy for ADL, cognitive evaluation and stimulation, safety education, and using assistive devices.
Between March 2014 and August 2017, 38 patients met the inclusion criteria and signed consent forms. Five were excluded due to medical complications, one left the hospital before completing rehabilitation, one had a bilateral hip replacement, and one had missing data, leaving 30 participants in the study. The author interviewed all the patients individually 10 days after their admission to rehabilitation, allowing them to adjust physically and mentally to geriatric inpatient rehabilitation.
Measures
The presurgery mFIM was based on retrospective reports at admission to rehabilitation, and the mFIM admission and discharge scores were collected from the patients’ charts based on scoring by a skilled multidisciplinary team. In addition, demographic, clinical, and functional data were collected from the hospital charts. The participants completed the Positive Affect questionnaire, Geriatric Depression Scale (GDS), hand-grip strength measures, and Numeric Pain Rating Scale.
Functional independence measure
Functional status was assessed by the FIM (Hamilton et al., 1987), a standardized measure of 18 items covering three domains: basic ADL (eight items); mobility level (five items) comprising the motor FIM (mFIM) in the current study; and cognitive function (cFIM) (five items). Items are scored on a 7-point scale ranging from 1 (complete dependence) to 7 (complete independence). Total FIM scores range from 18 to 126, with higher scores indicating greater functional independence. The mFIM at discharge indicates the level of functional ability; therefore, it was used in the current study as an outcome measure. The internal consistency of the FIM instrument is 0.93 (Dodds et al., 1993), and test–retest and interrater reliability are 0.95 (Ottenbacher et al., 1996).
Positive affect questionnaire
The positive affect questionnaire is a four-item summary scale related to the degree of positive feeling about a subject during the last week (Radloff, 1977). It is scored on a 4-point scale from 0 (rarely or none of the time) to 3 (most of the time). Summary scores range from 0 to 12, with higher scores indicating a more positive affect. This measure has been used in previous studies of the acute rehabilitation of persons with stroke (Seale et al., 2010). In the current study, the four positive affect items showed moderate-high internal consistency (α = 0.779).
Geriatric depression scale
The GDS (Burke et al., 1991) is a self-report scale consisting of 15 yes-or-no questions regarding depression symptoms experienced lately. The total GDS score ranges from 0 to 15, with higher scores representing more depressive symptoms. The sensitivity is 93%, and the specificity is 48% for cognitively intact adults; therefore, it can serve as a screening tool (Burke et al., 1991). The internal consistency in the current study was moderate-high (α = 0.810).
Hand-Grip strength
Hand-grip strength, a physical predictive measure (Taekema et al., 2010), was measured using a Camry electronic hand dynamometer. In this study, patients were instructed to keep their shoulders adducted and elbow extended with the wrist in a neutral position and squeeze the grip with maximal strength. The results, measured in kg, were the mean of two trials using the dominant hand in a seated position.
Numeric pain rating scale
The Numeric Pain Rating Scale (Childs et al., 2005) is a self-report rating scale with scores ranging between 0 (no pain) and 10 (worst pain). In this study, participants rated their pain in the surgical area while walking.
Statistical Analyses
Statistical analyses were performed using IBM SPSS Statistics (Version 21), with the significance level set at p < .05. The normal distribution curve, examined by a one-sample Kolmogorov–Smirnov test, was normal for the GDS, pre-mFIM score, and FIM at admission and discharge, but not normal for positive affect or LOS. Hence, we used parametric analysis, repeated measures, and one-way analysis of variance (ANOVA) with Bonferroni correction pairwise comparisons (p < .05) to evaluate differences in functional ability at three time points. Pearson correlations were conducted to examine the relations between the background, physical and psychological, and outcome variables. This was done to verify that all independent variables were associated with the dependent variables and to rule out the possibility of multicollinearity. In addition, we tested the correlations between the three predicted variables to ensure they were unique and did not represent the same variable.
We found that they were correlated with each other but only mildly. The correlation between LOS and ΔmFIM was r = .40 (p < .5); between LOS and mFIM at discharge was r = −.37 (p < .5); and between ΔmFIM and mFIM at discharge was r = −.46 (p < .1). Further, we conducted three hierarchical linear regressions to examine the study variables’ unique and combined contributions to predicting rehabilitation outcomes. The background variables (age, gender, and education) were entered in Step 1; function and physical factors (pre-mFIM, admission mFIM, pain, and hand-grip strength) in Step 2; and psychological factors (depression and positive affect) in Step 3. Because the sample was small, adding predictors could cause a prediction of error. Therefore, we used the stepwise method in each step. This allowed only the predictors contributing to the specific predicted variable (rehabilitation outcomes) to be entered. We also ran the regressions with all predictors, and the results remained the same.
Results
Thirty participants (70% female) with a mean age of 76.20 years (SD = 6.09) were included in this study. The average years of education were 12.73 (SD = 3.90), and the average MMSE score was 27.53 (SD = 1.83). Table 1 presents demographic characteristics, physical and psychological variables, functional ability, and rehabilitation outcomes. A repeated-measures one-way ANOVA showed significant differences in mean functional ability at all three time points, F(1, 29) = 88.82, p < .0001, η2p = .754. The post-hoc Bonferroni test (p < .05) showed a significant decrease in functional ability from presurgery to rehabilitation admission (p = .001) and a significant increase between rehabilitation admission and discharge (p < .001). However, a significant difference remained from presurgery to discharge from rehabilitation (p < .001).
Means, Standard Deviations, and Correlations With Confidence Intervals.
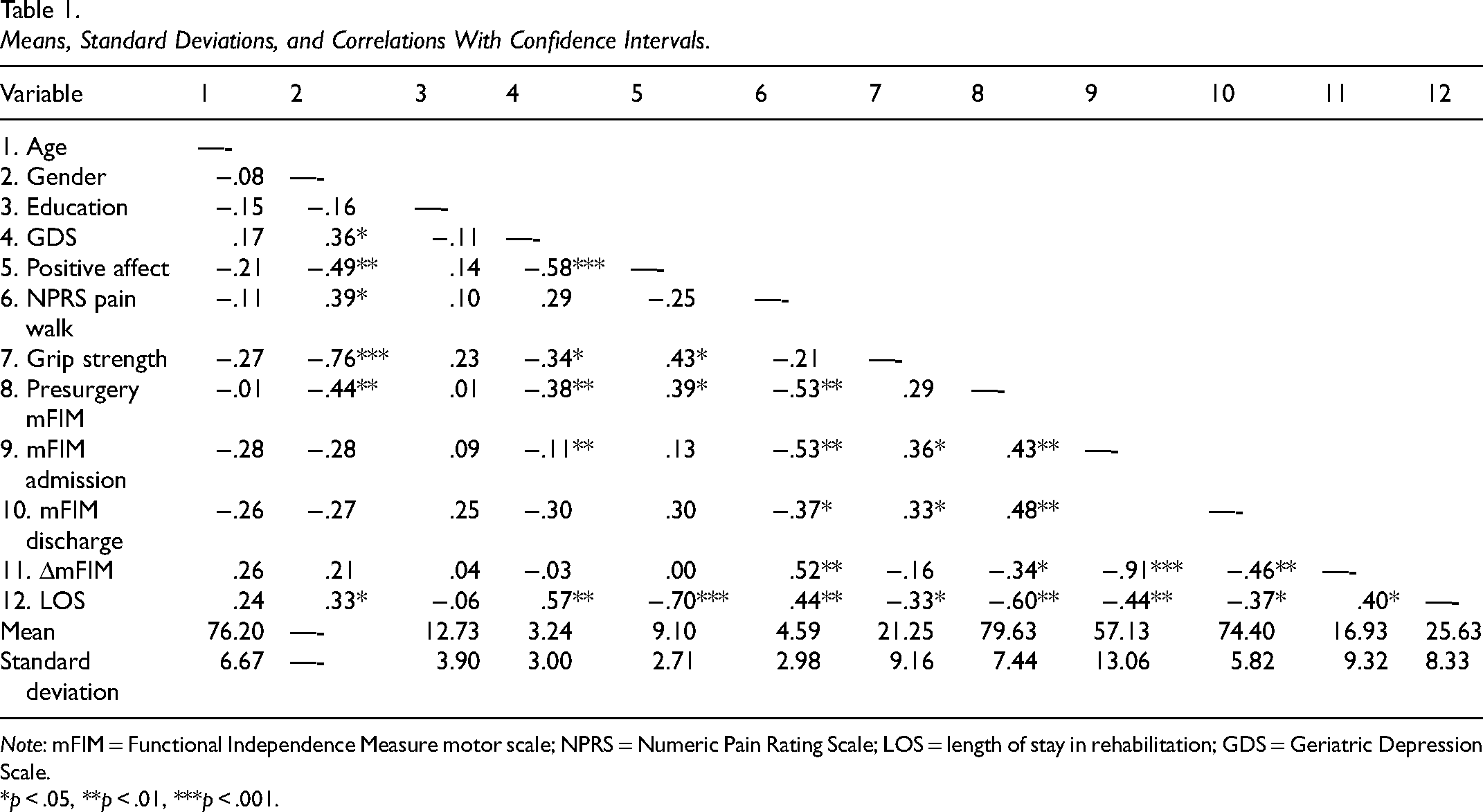
Note: mFIM = Functional Independence Measure motor scale; NPRS = Numeric Pain Rating Scale; LOS = length of stay in rehabilitation; GDS = Geriatric Depression Scale.
*p < .05, **p < .01, ***p < .001.
Table 1 also presents the Pearson correlations for intercorrelations among all study variables and their descriptive statistics (means and standard deviations for dichotomous variables were omitted; their frequencies are presented in the text). Significant correlations were found between all independent variables and rehabilitation outcomes. In addition, we found no particularly high correlations between the independent variables that might indicate multicollinearity.
Regression Models
Table 2 presents the results of the three hierarchical regression analyses of the independent variables’ unique and combined contributions to explaining the variance in rehabilitation outcomes. In the first regression, predicting improvement in mFIM between rehabilitation admission and discharge, only the mFIM at admission entered the regression. It accounted for 83.4% of the variance, adjusted R2 = .827, F(1, 25) = 125.199, p < .001. In the second regression, predicting mFIM at discharge, only the mFIM at admission entered the regression, accounting for 61.3% of the variance, adjusted R2= .598, F(1, 25) = 39.682, p < .001. In the last regression predicting LOS, the presurgery mFIM entered into the regression at Step 1, accounting for 36.3% of the variance, adjusted R2= .337, F(1, 25) = 14.245, p = .001. Importantly, positive affect added another 26.1% to the variance above and beyond the presurgery mFIM in Step 2, adjusted R2= .593, F(1, 24) = 19.928, p < .001. There was no multicollinearity because both VIF were lower than 2.
Hierarchical Linear Regression for Prediction of ΔmFIM, mFIM at Discharge, and Length of Stay (N = 30).
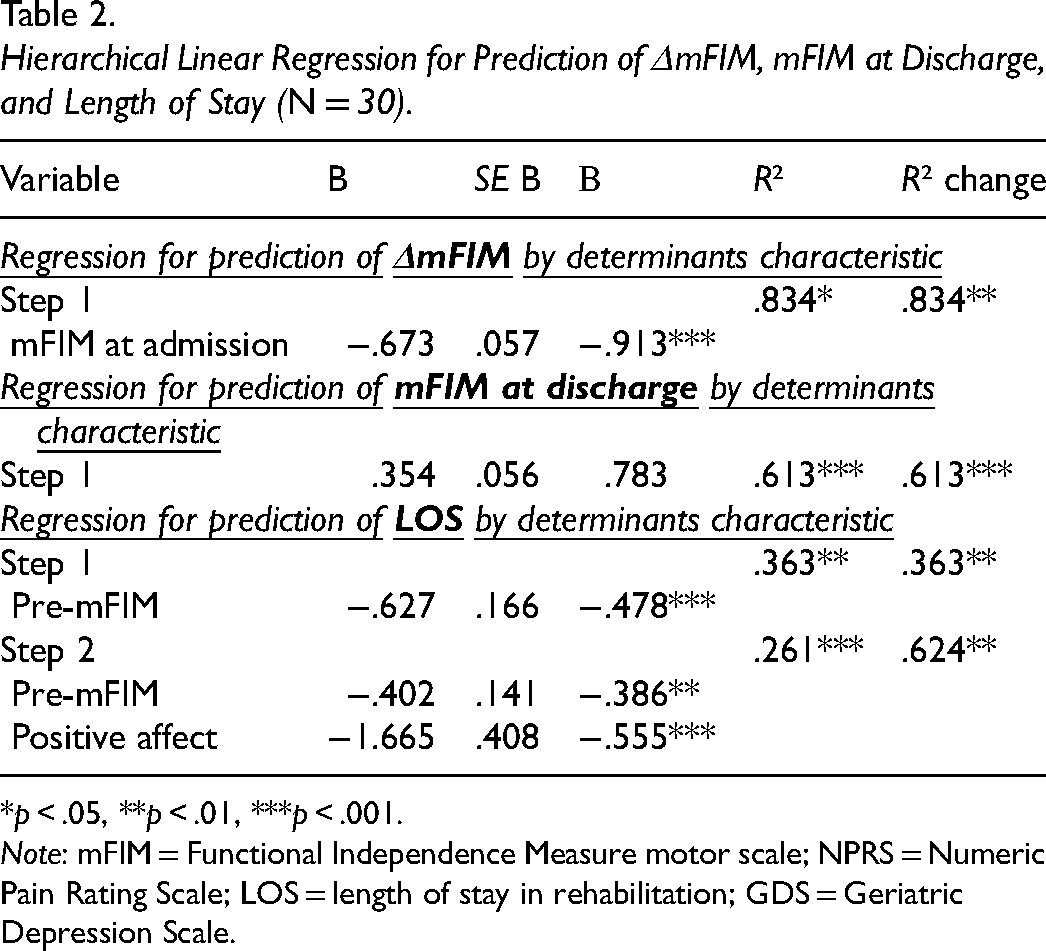
*p < .05, **p < .01, ***p < .001.
Note: mFIM = Functional Independence Measure motor scale; NPRS = Numeric Pain Rating Scale; LOS = length of stay in rehabilitation; GDS = Geriatric Depression Scale.
Discussion
This article described the improvement trajectory of functional ability, including ADL functioning and mobility, from presurgery to postrehabilitation among older adults attending acute rehabilitation following elective THR surgery. The results show decreased functional ability between presurgery and admission to rehabilitation, then improved functional ability between rehabilitation admission and discharge. However, the participants did not achieve their presurgery functional ability level upon discharge from rehabilitation as had participants in other studies. Inconsistent with the current results, improvement was found from presurgery among older adults 5 weeks (Benditz et al., 2017) and 6 weeks after THR surgery (age M = 60.28 years, SD = 12.20; Hartley et al., 2008) when measured by the Harris Hip score, which measures pain, motion, and function (Harris, 1969).
Moreover, Benditz et al. (2017) found improvement in functional ability even 1 week following THR, probably due to the younger age of participants in that study (M = 62.18 years, SD = 11.48). There is agreement in the literature that continuous rehabilitation regimes carried out in early or late phases after THR surgery can lead to significant improvement in muscle strength and function. These regimes include exercise programs and functional tasks at the rehabilitation center or home (Okoro et al., 2012) or individualized physical therapy rehabilitation programs associated with occupational therapy (Marcu et al., 2021). However, not achieving pre-surgery functional ability levels could be explained by the participants in the current study being relativity older; having high functional ability before surgery, according to their pre-surgery mFIM scores (M = 79.63) and, therefore, needing to improve relatively more to regain their previous function; or having persistent muscle atrophy about the hip even 2 years after THR (Rasch, et al., 2009).
In recent years, studies examining positive psychological variables among a variety of rehabilitation populations have increased. However, only a few included THR patients. The variables they considered were mainly optimism (Waldrop et al., 2001), self-efficacy, hope (Hartley et al., 2008), resilience (displaying courage and adaptability in the wake of life's misfortunes; Benditz et al., 2017), and mental health as a component of health-related quality of life (Vissers et al., 2012). To our knowledge, positive affect as a predictor has not been examined among THR patients. Therefore, the second goal of this study was to determine which study variables predict the three rehabilitation outcomes: improved functional ability, functional ability at discharge, and LOS. The innovative and significant result was that higher positive affect predicted lower LOS above and beyond physical factors or depressive symptoms; it can lead to effective ways to shorten LOS, thereby saving hospitalization costs.
Today's shorter hospital stays may challenge patients and health care systems. Arthroplasty is followed by a postoperative recovery period, including an acute rehabilitation scenario or rehabilitation at home to restore physical function (Okoro et al., 2012). Stark et al. (2016) reported a mean LOS following THR of only 8 days (SD = 6) among patients with an average age of 65 years (SD = 12) in some European countries. In contrast, the current study's mean LOS (25 days) was much higher because it included the in-hospital rehabilitation period and the study participants' mean age was much higher. However, the current LOS was shorter than for the hip-fracture population in Israel. With a mean age of 78.58 years (SD = 6.09), the general population's mean LOS in acute rehabilitation is 32.58 days (SD = 10.3; Segev-Jacubovski et al., 2022). Another explanation for the longer LOS in Israel might be that the State Health Insurance Law allows inpatient rehabilitation for those with medical conditions that require supervision and nursing care (Israel Ministry of Health, n.d.). This financing system allows relatively long hospitalization periods and, perhaps, does not press the patients or rehabilitation team to progress quickly.
According to this study's results, participants with higher positive affect had a greater benefit from rehabilitation activities in a shorter time than did other participants. Higher positive affect may have shortened the LOS in acute rehabilitation for several reasons. Ramanathan-Elion et al. (2016) found that positive affect facilitated therapeutic engagement after a variety of physical injuries. In addition, positive affect predicted resilience following severe physical injuries in inpatient rehabilitation (Quale & Schanke, 2010). Generally, people with high levels of positive affect tend to exercise more, maintain healthier lifestyles, and adhere more to medical regimens (Ostir et al., 2001), resulting in less severe illness and faster recovery (Pressman & Cohen, 2005).
Although positive psychological factors can facilitate successful adaptation and good outcomes from physical injury rehabilitation (Fredman et al., 2006; Kortte et al., 2010; Ostir et al., 2002; Seale et al., 2010), positive affect was not correlated with functional ability at admission or discharge or with improved functional ability. Possibly, the positive affect was related to leaving the hospital and returning home. The participants might have seen how much progress they had made after 10 days and anticipated their likelihood of going home early. It is important to note that positive psychology interventions can effectively enhance subjective and psychological well-being by strengthening psychological and social recourses and building resilience, positive affect, and optimism (Bolier et al., 2013). Those interventions include expressing gratitude and blessings, practicing kindness, setting personal goals (Bolier et al., 2013; Mohammadi et al., 2018), cognitive-behavioral therapy, and life review (Hernandez & Overholser, 2021).
Unsurprisingly, functional ability at admission predicted functional ability at discharge from acute rehabilitation and improvement in functional ability. Functional ability at admission, as measured with mFIM, was a strong predictor because it reflects the person's strengths and limitations, as the top–down approach claims (Weinstock-Zlotnick & Hinojosa, 2004). Consistent with this study's current result, Waldrop et al. (2001) found that the admission FIM score predicted significant variance in the discharge FIM scores among THR patients. Moreover, Brembo et al. (2017) found that physical function pre-THR-surgery predicted physical function 3 months later. Similarly, in other physical-injury rehabilitation, higher FIM scores at admission to rehabilitation were associated with higher FIM scores at discharge following a hip fracture (Hershkovitz et al., 2020) and stroke (Chumney et al., 2010).
Several limitations of this study should be noted. First, the sample was small, and the participants were recruited from a single location. Second, the mFIM scores presurgery, at admission, and at discharge were measured by different methods, and we did not test the internal consistency because we had only the total score. Further, inter-rater reliability was not tested because we relied on an experienced, skilled multidisciplinary team that regularly performs this scoring. Third, the sample consisted of participants only from a hospital, whereas a significant portion of THR patients receives rehabilitation treatment at home (Okoro et al., 2012). Further studies should use a larger, generalizable sample to include patients with in-home rehabilitation and other elective-surgery populations, such as total knee replacement. We also recommend examining the efficacy of interventions to increase positive affect and rehabilitation outcomes in a randomized controlled study.
Conclusion
This article describes the improvement trajectory of functional ability from presurgery to postrehabilitation among older adults attending acute rehabilitation following elective THR surgery. However, the participants did not achieve their presurgery functional ability level at discharge from rehabilitation. Therefore, throughout the rehabilitation program, occupational therapy and physical therapy should focus on self-care and mobility (Marcu et al., 2021).
Occupational therapists already have an important role in improving functional ability in rehabilitation by practicing daily living activities with limited body structure and function (American Occupational Therapy Association, 2020). An additional occupational therapy implication can be seen in this study's novel result that positive affect predicted LOS in acute rehabilitation among older adults following THR. Thus, occupational therapy practice can include evaluation of positive affect, which can assist in estimating LOS to prepare families and the health care system for the patient's return home. Additionally, comprehensive rehabilitation programs should bolster patients’ positive affect to facilitate shorter hospitalization during acute rehabilitation. The philosophy of occupational therapy greatly emphasizes the connections between the client's mind, body, and spirit and their participation in daily life occupations. Hence, occupational therapists can lead interventions to improve positive psychological factors and enhance functional ability in the rehabilitation process.
Key Messages
This study emphasizes the mind–body–spirit, reflecting the philosophy of the occupational therapy profession.
When presurgery functional ability levels are not regained, occupational therapy in the rehabilitation program should focus on self-care and mobility.
Because positive affect influences LOS in acute rehabilitation following elective THR, a positive affect assessment should be added to the occupational therapy evaluation and treatment.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.