
Abstract
Background/Aims:
Hypnotics are used to treat perioperative sleep disorders. These drugs are associated with a higher risk of adverse effects among patients undergoing surgery. This study aims to quantify the use of hypnotics and factors influencing the administration of hypnotics in relation to colorectal cancer surgery.
Method:
A retrospective cohort study of 1979 patients undergoing colorectal cancer surgery.
Results:
In all, 381 patients (19%) received new treatment with hypnotics. Two of the six surgical centres used hypnotics less often (odds ratio (95% confidence interval), 0.24 (0.16–0.38) and 0.20 (0.12–0.35)). Active smokers (odds ratio (95% confidence interval), 1.57 (1.11–2.24)) and patients receiving perioperative blood transfusion (odds ratio (95% confidence interval), 1.58 (1.10–2.26)) had increased likelihood of receiving hypnotics. In the uncomplicated cases, a multivariable linear regression analysis showed that consumption of hypnotics postoperatively was significantly associated with increased length of stay (1.5 (0.9–2.2) days).
Conclusion:
One in five patients began treatment with hypnotics after colorectal cancer surgery. Postoperative use of hypnotics was associated with an increased length of stay for uncomplicated cases of colorectal cancer surgery.
Introduction
Benzodiazepines were introduced in the 1950s; more recently, the now preferred hypnotics, the benzodiazepine-like drugs, have been developed for treating primary and secondary insomnia. In the elderly, hypnotics may be associated with significant adverse effects such as impaired cognition, drowsiness, sedation and prolonged hospitalization.1–3 Insomnia, anxiety and emotional disturbances are also key factors in postoperative delirium, and identifying these conditions as precursors of delirium can be difficult and might wrongly result in administration of hypnotics to these patients. Especially for elderly patients, the use of these hypnotics can contribute to the development of postoperative delirium.4–7
In the fast-track surgery principles, which are broadly accepted and well documented, mobilization of the surgical patient is crucial 8 and sufficient mobilization is only possible with unimpaired cognition and psychomotor skills. 8 It has, to our knowledge, not previously been shown that postoperative use of hypnotics is associated with an increased length of stay after uncomplicated colorectal cancer surgery. This study aimed to quantify the use of hypnotics in the perioperative period in patients undergoing colorectal surgery. Furthermore, we wished to investigate the factors associated with administration of these drugs.
Design and methods
This is a cohort study based on the data from the Danish Colorectal Cancer Group’s (DCCG) database. Information on medications was obtained from electronic medical records. The DCCG database contains prospective, nationwide data with a completeness rate of 99%. 9 The data included for this study consist of data from the six major surgical centres responsible for colorectal cancer surgery in the eastern part of Denmark (population 2.5 million – approximately 45% of the national population). In 2003, electronic medical records were introduced in Denmark, and by 2006, the systems were fully implemented in the six surgical departments.
The data for this study were collected simultaneously with data collected for two more studies: one study concerning the risk of anastomosis leakage associated with postoperative nonsteroidal anti-inflammatory drugs (NSAIDs) 10 and one study examining the effect of statins on the risk of anastomosis leakage. 11 Therefore, the population in this study consists of patients with a primary anastomosis after colorectal resection for cancer as this was the predefined inclusion criteria in the three studies.
The data were extracted on patients undergoing resection of the colon or rectum with primary anastomosis from 1 January 2006 to 31 December 2009.
From the database, we compiled information on demographic factors, co-morbidities, American Society of Anesthesiologists – risk score (ASA score), tobacco use, alcohol consumption, intraoperative blood transfusion, procedure and resection type, length of stay, intraoperative morbidity and complications, and anastomosis leakage (defined as a clinically significant leakage requiring surgical intervention).
To determine the use of hypnotics, individual search for each patient was made in the electronic medical records. Three researchers carried out the search. All three were blinded for the above extracted patient data. The name and administration of one dosage of a hypnotic were recorded, in a preset period of 7 days before and 7 days after surgery. It was registered as pre- or postoperative administration, not being able to give the date on the specific day.
We focused on hypnotic-naive patients, that is, the patients who did not use hypnotics on a regular basis preoperatively. Thus, patients who used hypnotics prior to surgery were excluded from the study. Patients diagnosed with anastomosis leakage and patients who required transfusions during surgery were considered as complicated cases.
Statistical analyses were performed using SPSS version 17 (SPSS Inc., Chicago, IL, USA). Data are presented as median (interquartile range) and as numbers and percentages, unless stated otherwise. We tested for differences between groups, using Mann–Whitney’s test for continuous variables and chi-square and Fisher’s exact tests for dichotomous variables. Univariate logistic regression analyses were performed to identify risk factors for postoperative treatment with hypnotics. Finally, a multivariate logistic regression analysis (method: backwards, likelihood ratio) was performed, including all variables with a p-value <0.2 from the univariate analyses. The results from the logistic regression analyses are presented as odds ratios (OR) with 95% confidence intervals (CIs) and p-values. Multivariable linear regression analysis was performed for factors presumably associated with a prolonged length of stay.
Before initiation, the study was approved by the Scientific Council of the DCCG and by The Danish Data Protection Agency (j.no. 2008-41-2484). Because the study design involved no patient contact or biological material, approval from the ethical committee was not needed.
Results
In all, 2278 patients underwent surgery; of these, 299 were excluded due to preoperative hypnotics use. Thus, 1979 hypnotic-naive patients were included in the analyses. Demographic variables and patient characteristics are presented in Table 1. The median age of the entire study population was 69 years (interquartile range (IQR), 62–76 years) with slightly more men (54%) than women. In 381 patients (19%), new treatment with hypnotics was initiated after surgery.
Population characteristics and data completeness.
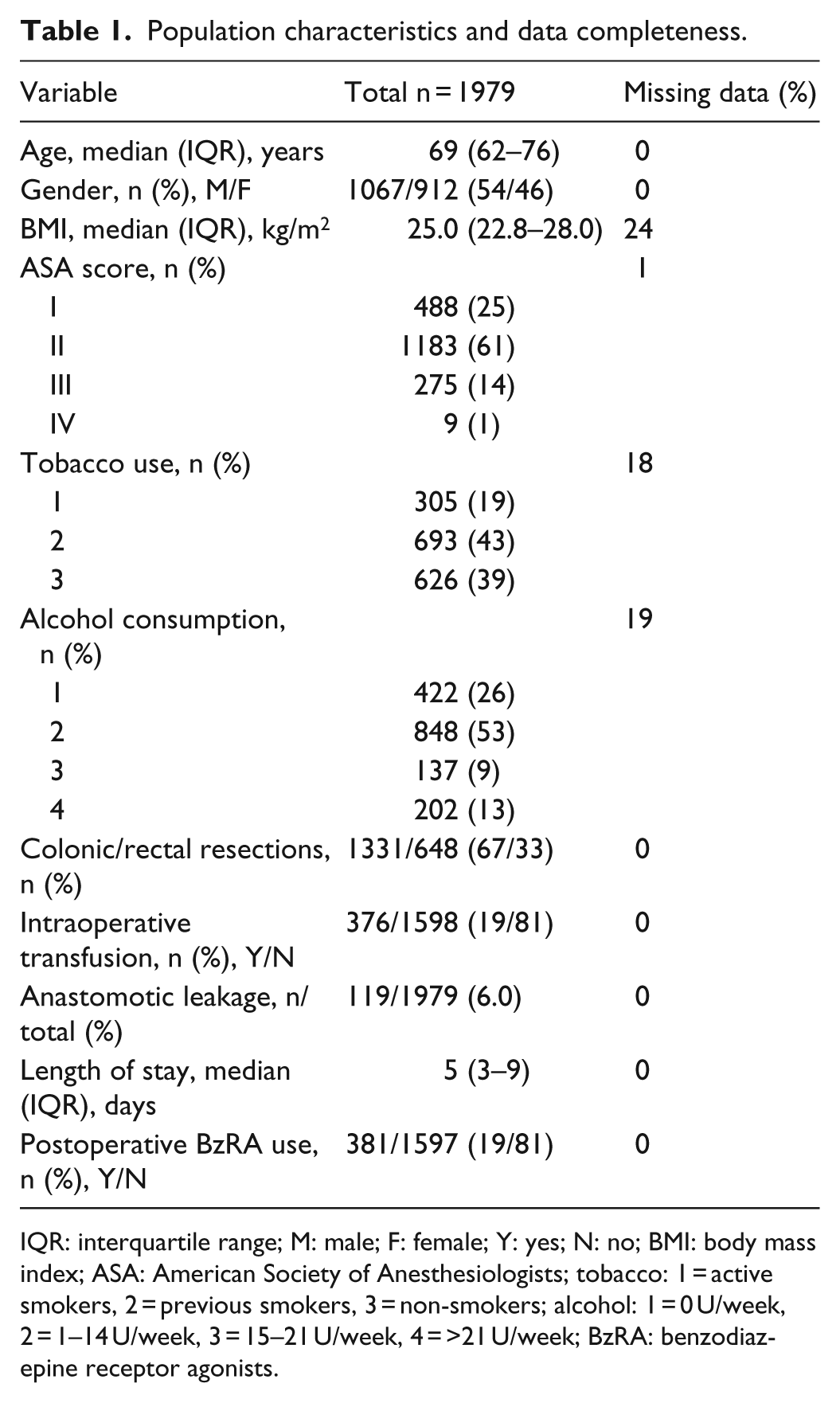
IQR: interquartile range; M: male; F: female; Y: yes; N: no; BMI: body mass index; ASA: American Society of Anesthesiologists; tobacco: 1 = active smokers, 2 = previous smokers, 3 = non-smokers; alcohol: 1 = 0 U/week, 2 = 1–14 U/week, 3 = 15–21 U/week, 4 = >21 U/week; BzRA: benzodiazepine receptor agonists.
In Table 2, hypnotic users are compared to controls. Patients in the hypnotic group were slightly younger (68 (61–75) years vs 69 (62–77) years; p = 0.047) and there were more active smokers among the hypnotic users (23% (73) vs 18% (232); p = 0.041). The remaining demographic and operative factors were comparable, with the exception of the length of stay, which was significantly longer in patients receiving hypnotics after surgery (7 (4–10) days vs 5 (3–8) days; p < 0.001).
Population characteristics according to hypnotics usage.

IQR: interquartile range; M: male; F: female; Y: yes; N: no; BMI: body mass index; ASA: American Society of Anesthesiologists; tobacco: 1 = active smokers, 2 = previous smokers, 3 = non-smokers; alcohol: 1 = 0 U/week, 2 = 1–14 U/week, 3 = 15–21 U/week, 4 = >21 U/week.
To identify individual factors associated with use of hypnotics, univariate logistic regression analyses for the following variables were performed: age, gender, ASA score, tobacco use, alcohol consumption, intraoperative transfusion, surgical centre and colonic or rectal resection. The results are given in Table 3. Based on a p-value less than 0.2, age, gender, tobacco use, intraoperative transfusion, surgical centre and anastomosis leakage were included in the final multivariate analysis.
Univariate logistic regression analyses with odds ratios indicating the risk of postoperative treatment with hypnotics.

CI: confidence interval; ASA: American Society of Anesthesiologists.
Odds ratio with 95% CI for an increment of 10 years is given.
Odds ratio with 95% CI for an increment of 5 days is given.
The multivariate analysis (Table 4) showed significantly decreased risk of postoperative hypnotics use at two of the six surgical centres (OR (95% CI), 0.24 (0.16–0.38) and 0.20 (0.12–0.35)). Furthermore, active smoking (1.57 (1.11–2.24)) and receiving intraoperative transfusion (1.58 (1.10–2.26)) increased the risk. Finally, increasing age decreased the risk of hypnotics use after surgery by 14% (3%–24%) for every 10 years of age increment (p = 0.013).
Multivariate logistic regression analyses with odds ratios indicating the risk of postoperative treatment with hypnotics – variables with p < 0.2 in the univariate analyses were included in the model.

CI: confidence interval.
Variables from the univariate analyses (Table 3) with p < 0.2. Intraoperative transfusions were included in the model.
Odds ratio with 95% CI for an increment of 10 years is given.
Odds ratio with 95% CI for an increment of 5 days is given.
To investigate which factors were associated with a prolonged length of stay, we performed a multivariable linear regression analysis. The length of stay would normally be markedly prolonged in the occurrence of postoperative complications. Therefore, for this analysis, we excluded the complicated patient courses, defined as those courses where anastomosis leakage was diagnosed and/or where blood transfusion was given during operation. By excluding these 444 complicated cases, 1530 homogeneous cases remained for analysis. In this cohort, the length of stay was median (IQR) 5 (3–8) days. A total of 283 patients (18.5%) received hypnotics after surgery. In the linear regression, the following factors were included as independent variables: surgical centre, ASA score, gender, colonic or rectal resection and postoperative use of hypnotics. Age was included as a continuous covariate. The analysis showed a significant association between hypnotics use and prolonged length of stay, with the length of stay being prolonged 1.5 (0.9–2.2) days (p < 0.001; Table 5). In a subsequent analysis where the complicated cases (anastomosis leakage and/or blood transfusion) were included, postoperative hypnotics consumption was no longer associated with a significantly prolonged length of stay (data not shown). To test for possible selection bias, we correlated the use of hypnotics for each surgical centre to the postoperative length of stay.
Multivariable linear regression identifying factors associated with increased length of stay (only ‘uncomplicated’ cases, that is, cases without anastomosis leakage or intraoperative blood transfusion).

CI: confidence interval; ASA: American Society of Anesthesiologists.
We found that 12 different agents were administered with zopiclone being the preferred prescribed hypnotic (94.2%).
Discussion
In this study, based on prospective data from the DCCG database and mandatory registration of medicine administration, we have shown that one in five hypnotic-naive surgical patients received hypnotics in the postoperative phase. Hypnotics consumption in patients with otherwise uncomplicated postoperative courses was significantly associated with increased length of stay. The preferred drug of choice was zopiclone with 94.2%. The hypnotic users did not differ significantly from the controls with regard to demographic or perioperative factors. There was a large difference between surgical centres (OR, 0.23–1.04; Table 3), suggesting that culture and local habits may play a role. Other risk factors for hypnotics administration included current tobacco usage, while increasing age decreased the chances of hypnotics administration.
To our knowledge, no previous studies have examined the effect of hypnotics on the length of stay after major surgery. In a prospective, double-blinded study, a sample of 110 patients undergoing ambulatory surgery were randomized to placebo or the benzodiazepine receptor antagonist flumazenil at the end of surgery. 12 Amnesia and sedation were reduced in the flumazenil group, whereas time to discharge was not influenced by flumazenil administration. As this study was based on ambulatory patients, comparison with our results is not possible. It is well established, however, that postoperative hypnotics consumption increases the risk of postoperative delirium, which again may increase the length of stay. 13
It was demonstrated in a prospective cohort study 14 that an increased risk of delirium (OR (95% CI), 3.0 (1.3–6.8)) was found in patients treated with benzodiazepines. The development of delirium is multifactorial 13 with hypnotics consumption contributing as an independent factor.
Sleep disturbances are frequent after major surgery and the consequences may be serious.15,16 However, administration of hypnotics is associated with significant risk of adverse effects, including cognitive impairment with confusion and memory impairment.2,7,17 Psychomotor skills can also be affected,7,17 and studies have shown that memory is particularly sensitive to the use of hypnotics. Especially, anterograde amnesia can be a result, resulting in compromised patient compliance.18,19 Administration of supra-clinical doses has shown to produce rebound insomnia after discontinuation,18,19 where just one to two nights of supra-clinical dose of triazolam (0.5 mg) or zolpidem (15 mg) have resulted in a rebound effect. 18 In the elderly, the use of hypnotics results in up to 50% increased risk of hip fracture.9,17,20 Considering the pharmacokinetics of zopiclone, the choice of drugs is not ideal due to a mean elimination half-life of 3–6 h,21,22 compared with zolpidem with a mean elimination half-life of 1.5–2.4 h.21,22 Finally, the use of hypnotics while admitted increases the likelihood of long-term use after discharge, with almost one in four patients starting on hypnotics during their hospital stay still use the drug 3 months later.3,23–25
The strength of this study lies in the large number of patients and the high quality of data from the DCCG database and digital mandatory records of medicine administration. The digital medicine administration system records both the prescription and the administration, thus ensuring that the data reflect the actual consumption of the drugs. We have defined the term ‘naive users’ as patients who were not registered as hypnotic users at admission. However, we were not able to control if the patients had used hypnotics prior to 1 week before admission; therefore, there may be heterogeneity in the hypnotics group. With regard to the linear regression analysis on the length of stay, the strength lies in the homogeneity of the uncomplicated cases. We did not, however, hold data on minor surgical or medical complications, which may have influenced the length of stay and thereby could influence the regression analysis. Also, we cannot exclude that the association shown was a result of a simple relationship between the length of stay and hypnotics distribution, the latter being more likely to occur as the length of stay increased. However, as the association disappeared when the complicated cases, being patients diagnosed with anastomosis leakage and patients who required transfusions during surgery, were included in the analysis, the use of hypnotics independently may have influenced the length of stay and was not merely a consequence of confounding by indication.
In conclusion, we have shown that one in five surgical patients received new treatment with hypnotics in the postoperative phase. The rate of administration differed widely between surgical departments, suggesting a difference in culture being responsible for some of the administrations. Furthermore, our results show that hypnotics are associated with an increased length of stay in otherwise uncomplicated cases.
Generally, the use of these drugs should be reduced as much as possible, and if needed, hypnotics with shortest half-life and lowest possible cognitive side effects should be chosen.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.