
Abstract
The mental health of aging men is an understudied social issue. Although it is widely accepted that meaningful family relationships are associated with fewer depressive symptoms and greater positive affect, scholars have largely overlooked relationships between grandfathers and grandchildren as being beneficial to men’s mental health. This study investigates the differences in the depressive symptoms and positive affect of 351 grandfathers. Using a cluster analytic technique, participants were categorized as involved, passive, and disengaged based on their frequency of contact, level of commitment, and participation in activities with grandchildren. Comparative analyses indicate that involved grandfathers had fewer depressive symptoms than disengaged grandfathers. Involved grandfathers had significantly higher scores on positive affect than disengaged grandfathers, and passive grandfathers had significantly higher scores on positive affect than disengaged grandfathers. This study provides evidence that grandfather–grandchild relationships influence aging men’s mental health. Implications for practitioners working with aging men are discussed.
The mental health of middle-aged and older men represents an understudied social issue, while the emotional and behavioral difficulties among members of this population are frequently underdiagnosed and undertreated (Apesoa-Varano, Hinton, Barker, & Unützer, 2010). Data from the Health and Retirement Study 2002 indicates that more than 11% of men aged 55 years and older experience clinically relevant depressive symptoms (He, Sengupta, Velkoff, & DeBarros, 2005; The Health & Retirement Study, n.d.). This percentage, likely an underestimate of the actual incidence of depression among middle-aged and older men (Hinton, Zweifach, Oishi, Tang, & Unützer, 2006), points to the prevalence of the illness in this population. In fact, depression is the most common mental illness and the greatest risk factor among men who commit suicide (Schmutte, O’Connell, Weiland, Lawless, & Davidson, 2009), is associated with sleep disturbances in older men (Paudel et al., 2008), and incorrect diagnosis and treatment of the disorder has been linked with higher public health care costs (Carta, Hardoy, Kovess, Dell’Osso, & Carpiniello, 2003). Given that older men often have smaller social networks than older women (Antonucci & Akiyama, 1987) and because loneliness is a strong predictor of depressive symptoms in men (Alpass & Neville, 2003), meaningful relationships with grandchildren may function to decrease depressive symptoms and increase positive affect in this population.
Although the influence of intergenerational family interaction on the mental health of aging men has received limited attention in the literature, there is evidence that the quality of family relationships has preclusive effects on depressive symptoms and beneficial impacts on positive affect in men (Bates, 2009b; Felton & Berry, 1992; E. Miller, Buys, & Roberto, 2006). In addition, recent research does suggest that the occurrence of negative family events (i.e., family feud, parental separation or divorce, or sudden relocation) that affect grandchildren is associated with increased incidence of depressive symptomatology in grandfathers (Drew & Silverstein, 2007; Drew & Smith, 2002). It stands to reason that positive interpersonal interaction between grandchildren and grandfathers is negatively related to the prevalence of depressive symptoms and increases the possibility for positive affect. The current study examines how various aspects of grandfather–grandchild interaction affect the depressive symptoms and positive affect of middle-aged and older men.
Literature Review
Very few American men remain grandchildless. According to nationally representative data, among men with children aged 40 years and older, nearly 94% are grandfathers (Szinovacz, 1998). These data also indicate that more than 78% of grandfathers’ families are composed of three generations and more than 14% have four or more generations. In addition, men today are living longer than those in previous generations, and some projections suggest that grandfathers will have more years to devote to grandparenthood than their predecessors (Cherlin, 2010). Notwithstanding these demographic realities, research on grandfathers is underdeveloped and has largely been limited to understanding how grandfathers impact grandchildren rather than understanding how grandfathers benefit from interaction with grandchildren, the main purpose of this study.
Although the literature is relatively small, scholars have identified two broad purposes of grandfathering. First, there is consensus that grandfathers socialize grandchildren to the dominant culture (Bates, 2009a; Bengtson, Copen, Putney, & Silverstein, 2009) and to family roles and responsibilities (Bates & Goodsell, forthcoming; Goodsell, Bates, & Behnke, 2011; Waldrop et al., 1999). Second, grandfathers serve an important supportive function for their children and grandchildren (Bates, 2009a; Sellers & Milton, 2007)—much like a safety line that can be extended when needed (Hagestad, 1985; Mann & Leeson, 2010). Grandfathers may offer support out of necessity, during times of individual and family crisis (Burton, 1992; Roberto, Allen, & Blieszner, 2001), or may attempt to support the typical development of grandchildren in the absence of parents (Bates & Goodsell, forthcoming; Chan, 2007).
There are various means by which grandfathers may attempt to accomplish these two purposes, and scholars consistently point out that the methods and strategies of socialization and support can be circumscribed by three key components of intergenerational relationships (Bates & Taylor, forthcoming; Douglas & Ferguson, 2003; King & Elder, 1997). They are contact frequency, participation in activities, and intergenerational commitment (see Bates & Taylor, forthcoming). For a grandfather to socialize and support a grandchild, he must have contact with the grandchild through in-person visits or non-face-to-face contact such as via telephone. Grandfathers must participate in activities with the grandchild and must be committed to the grandchild and to that relationship. These concepts are presumed to assess the relational (contact), behavioral and interactional (participation in activities), and social–cognitive (commitment) aspects of intergenerational relationships (Bates & Taylor, forthcoming). Following is a review of how these components are empirically related to mental health.
Mental Health and Family Relationships
Contact frequency
Most studies that investigate relations between contact frequency and mental health have taken a deficit perspective, centered primarily on grandparents’ grief over and decreased well-being subsequent to the loss of contact with grandchildren (Drew & Silverstein, 2007; Drew & Smith, 1999) and resulting changes in grandparental role identity (Drew & Silverstein, 2004; Reitzes & Mutran, 2004). Drew and Silverstein reported that grandparents who had lost contact with one set of grandchildren developed depressive symptoms at a more rapid rate than grandparents who had not lost contact with a set of grandchildren. Interestingly, grandfathers in this study developed symptoms more rapidly than did grandmothers. They also found that the elevation of depressive symptoms decreased over time, indicating a rebound in well-being, even if contact did not resume. A similar study in the United Kingdom also indicated that grandparents who had lost contact with grandchildren as a result of family feuds reported significantly more depressive symptoms than did grandparents who had not lost contact with their grandchildren (Drew & Smith, 2002).
Although most studies have only considered the deleterious effects of negative family events on mental health, one recent study reported that grandfathers’ contact with grandchildren was associated with higher quality relationships, which was in turn associated with fewer depressive symptoms (Bates, 2009b). Although this particular study did not examine positive affect, it is probable that the frequency of contact with grandchildren is also an important factor in the prevalence of positive affect.
Participation in activities
Participation in various activities with family members has been shown to be associated with mental health outcomes. For instance, in a recent study of rural men 65 years and older living in the United States and Australia, E. Miller et al. (2006) reported that the unavailability of someone (family member or close friend) to share confidences and trust was strongly and significantly linked to greater depressive symptoms. Similarly, Felton and Berry (1992) reported that older adults (63-90 years old) with family members who acted as pleasant companions, sympathizers, and who assisted with household or personal tasks experienced significantly greater positive affect than when provision of these activities came from nonkin. Recent research indicates that grandfathers’ participation in recreational activities, teaching activities, and comforting activities are associated with higher quality relationships with grandchildren, which, in turn, is associated with fewer depressive symptoms (Bates, 2009b).
Commitment
Scholars have noted wide variations in grandparents’ engagement in grandchildren’s lives (Cherlin & Furstenberg, 1986; Mueller, Wilhelm, & Elder, 2002; Neugarten & Weinstein, 1964). One possible reason why grandparents are more or less engaged is that they are more or less committed to the grandchild. Presumably, a greater level of commitment equates to greater overall involvement. Interestingly however, besides efforts to theorize about commitment in grandfather–grandchild relationships (Bates & Taylor, forthcoming), scholars have made little effort to operationalize and directly assess commitment in intergenerational relationships.
The bulk of scholarship on commitment has been located in the literature on intimate couples, which has indicated strong associations between commitment and relationship-based outcomes (e.g., Frank & Brandstätter, 2002; Stanley, Markman, & Whitton, 2002). These noted relationship outcomes have implications for levels of positive affect and the persistence of depressive symptoms (Antonucci, Lansford, & Akiyama, 2001; Spotts et al., 2005; Zlotnick, Kohn, Keitner, & Della Grotta, 2000), such that greater levels of commitment are associated with few depressive symptoms and greater positive affect. Furthermore, recent grandparent research has indicated that commitment to grandchildren was negatively associated with grandfathers’ depressive symptoms such that greater levels of commitment were associated with fewer symptoms (Bates, 2009b).
The Current Study
There is sufficient evidence that intergenerational contact frequency, participation in activities with family members, and commitment to family relationships are individually associated with fewer depressive symptoms and greater levels of positive affect. However, to date, scholars have yet to consider how these factors operate together. Because behavioral and interactive aspects of intergenerational relationships do not occur in isolation, this study considers how these factors operate in unity to influence depressive symptoms and positive affect. To do so, the first task is to develop a typology of grandfather involvement using a cluster analytic technique.
Cluster analysis is a person-centered, holistic approach in the sense that individual participants are treated as indivisible wholes (Mueller & Elder, 2003). It is a technique used to group people with similar configurations or patterns on key variables (Mueller et al., 2002) and stands in contrast to classification analyses that group variables (e.g., discriminant function analysis, exploratory factor analysis [EFA]). The key variables in this study are contact frequency, participation in activities, and commitment, and the cluster grouping technique allows for the comparison of men with other men on group characteristics. The first research question is as follows:
Research Question 1: Can distinct groups of grandfathers be identified from self-reported contact frequency, participation in activities, and commitment?
The second task is to test for differences in depressive symptoms and positive affect. The second research question is as follows:
Research Question 2: Are there group differences in grandfathers’ depressive symptoms and positive affect?
Addressing this question is a first step in determining which aspects of intergenerational relationships are most vital to improving the mental health of aging men. In comparing the mental health of grandfathers with other grandfathers as a function of interpersonal interaction, this study contributes to the literature on men’s mental health by drawing attention to the potentially important positive effects that interaction between extended family members has on decreasing depressive symptoms and increasing positive affect.
Method
Participants and Recruitment
Data are drawn from the Grandfather Involvement and Health Survey. Data collection occurred primarily in Central New York, although grandfathers lived in various locations throughout the United States. A sample of 351 grandfathers were recruited in a variety of ways including being invited by the researchers in presentations to an American Legion post and a senior-citizens center, through personal associations, and recruitment at two large churches (one predominantly Black and one predominantly White) in urban and suburban regions of Central New York. Undergraduate students, serving as contacts persons, also recruited grandfathers through personal associations. Participants completed either a written version of the questionnaire on their own or over the telephone with contact persons. Grandfathers were asked to select one grandchild and answer questions in the survey about their relationship with that particular grandchild. Background information about the grandchild, their parents, and the grandfathers is presented in Table 1.
Background and Demographic Characteristics of Grandfathers and Grandchildren

Missing = 1.
Missing = 28.
Missing = 30.
Missing = 5.
Missing = 7.
Missing = 22.
Missing = 2.
Measures
Before data reduction analyses occurred, normality (i.e., skewness, kurtosis) of the composite variables was assessed and will be discussed in subsequent sections. In addition, the extent of missing data was explored. Missing data occurred in each item less than 5% of total cases and as such, missing data were replaced with the mean as recommended by Tabachnick and Fidell (2007). It was not appropriate to do a mean replacement on background and demographic variables.
Contact frequency
The frequency of contact with the selected grandchild was assessed with 4 items on a 7-point ordinal scale ranging from 1 (Never or almost never) to 7 (Daily). Items included the following: “In general, how often . . .” (a) “do you visit this grandchild at your home or at his or her home?” (b) “do you talk on-on-one?” (c) “do you call or receive a telephone call from this grandchild?” and (d) “do you send to or receive cards, letters, or packages from this grandchild?” All the items were normally distributed as was the composite variable. Scores were summed in the creation of the composite variable (M = 17.43, SD = 4.01, range = 4-27). Internal consistency was adequate (α = .66).
Participation in activities
Participation in activities was measured with 34 items on a 4-point Likert-type scale ranging from 1 (Strongly disagree) to 4 (Strongly agree). Items assessed a wide range of activities based on six generative grandfathering work ethics (see Bates, 2009b). Examples of items from each work ethic included the following: “As a grandparent, I . . .” (a) “tell this grandchild stories from my life,” (b) “teach this grandchild new practical skills,” (c) “listen to this grandchild and be a confidant,” (d) “play enjoyable games or activities with this grandchild,” (e) “pass on family traditions to this grandchild,” and (f) “invest in this grandchild’s future.” Eleven items showed varying degrees of negative skewness (five of which were moderately to severely leptokurtic), indicating that many grandfathers were rating high on these items. However, these skewed items had negligible effects on the skewness and kurtosis of the composite variable, which was normally distributed. Scores were summed for the composite variable (M = 111.19, SD = 17.23, range = 47-136). Internal consistency was very good (α = .95).
Intergenerational commitment
The operationalization of commitment was based on the three aspects of Johnson’s (1999) conceptualization of personal dedication. Commitment to the grandchild, commitment to the relationship with the particular grandchild, and satisfaction with the grandfather identity were assessed with 5 items on 4-point Likert-type scales ranging from 1 (Strong disagree/Very unsatisfied) to 4 (Strongly agree/Very satisfied), one item was negatively worded and was thus reverse coded. Example items included the following: “I am committed to this grandchild” and “How satisfied are you with the role you play as your grandchild’s grandparent.” Two items showed a slight negative skew and one item had a severe negative skew and was strongly leptokurtic, indicating that many grandfathers were rating their commitment high. However, this item had a negligible effect on the skewness and kurtosis of the composite variable, which was normally distributed. Scores were summed to create the composite variable (M = 17.14, SD = 2.94, range = 5-20). Internal consistency of the remaining four items was good (α = .83).
Mental health
Grandfathers completed the Center for Epidemiologic Studies–Depression Scale (CES-D; Radloff, 1977), which has 20 items assessed on a 4-point scale that was coded 1 (Rarely or none of the time [less than 1 day in the past week]) to 4 (Most or all of the time [5-7 days in the past week]). The CES-D has been widely used with older adults to assess depressive symptoms (Radloff & Teri, 1986). There are 4 positively worded items and 16 negatively worded items. Scholars have identified multiple latent constructs in the CES-D including depressive symptoms and positive affect (Love & Love, 2006; T. W. Miller, Markides, & Black, 1997; Radloff, 1977). Researchers make convincing arguments for conducting EFA on data collected from middle-age and older men with the CES-D to determine the appropriate structure of latent constructs for a given sample (Love & Love, 2006). Thus, an empirical, data-driven approach was taken to determine the structure of any latent constructs within our CES-D data. A principal axis EFA was conducted with an oblique rotation and the analysis constrained to two factors. Items loading below .40 and those that loaded on multiple factors with a difference of ≤.20 were removed. Kaiser’s Measure of Sampling Adequacy, recommended above .60, was strong at .83, and the two factors produced had eigenvalues above 1.0. According to the standardized regression coefficients, 13 of the 16 negatively worded items loaded on the first factor, accounting for 75% of the variance and three items were removed because loading scores did not reach .40. These 13 items formed the latent construct that will be referred to as depressive symptoms (M = 16.62, SD = 4.40, range = 13-44). This variable was positively skewed, indicating relatively low depressive symptomatology. This would be expected with a community-dwelling sample of older adults, thus making a transformation to attenuate for nonnormality inappropriate. Internal consistency of these items was good (α = .84). All four of the positively worded items loaded on the second factor. These items comprised the latent variable that will be referred to as positive affect (M = 13.35, SD = 2.77, range = 4-16) and was normally distributed. Internal consistency of these items was adequate (α = .76). These two composite variables were only weakly associated (r = −.28, p < .0001), further justifying separation into two unique latent variables.
Analytic Strategy
Means of the three variables (contact frequency, participation in activities, and commitment) were converted into standardized z-scores as recommended for cluster analysis. A hierarchical cluster analysis using a Ward’s method of agglomeration was performed in SAS. Ward’s method groups participant scores based on a maximization of the regression coefficient (R2) between clusters. A dendrogram of clusters was created and three clusters were requested to be output for use in subsequent comparative analyses. To determine if clusters were statistically different from each other, three 1 (z-score of dependent variable) × 3 (cluster level) analyses of variance (ANOVA) were conducted. Follow-up t tests with Bonferroni adjustments were computed in pairwise comparisons of z-scores. These analyses indicate whether the three clusters actually form three unique groups of participants.
Two ANOVAs were conducted with follow-up t tests with cluster level as the independent variable and depressive symptoms and positive affect as dependent variables. These analyses determined differences between cluster groupings on mental health variables. Consideration was given to performing two analyses of covariance (ANCOVA), which would employ a number of background and demographic variables as covariates, with the goal of reducing the confounding effects of independent variables on depressive symptoms and positive affect. One of the key assumptions of ANCOVA is that covariates should be correlated with dependent variables (r ≥ .30) and not correlated with independent variables (Musil & Ahmad, 2002; Tabachnick & Fidell, 2007). This assumption is particularly important to observe in nonexperimental studies because violations of it may lead to reduced statistical power to detect group differences (Owen & Froman, 1998) and to threats to validity (Pedhazur & Schmelkin, 1991). After computing zero-order correlations between covariates and study dependent and independent variables, it was determined that none of the demographic variables (grandfather age, grandchild age, distance from grandchild via car travel, number of grandsons and granddaughters) and none of the background variables (grandfather physical health, Big Five personality markers, parent support of relationship, spouse support of relationship, and community involvement) met the ANCOVA assumption (full correlation matrix is available from the first author). Thus, results of the ANCOVAs are not reported. See Table 2 for correlation coefficients among key study variables.
Zero-Order Correlations

p < .01. **p < .001. ***p < .0001.
Results
Typology of Grandfather Involvement and Cluster Comparisons
The dashed line depicted in Figure 1 “breaks” the dendrogram plot into three clusters. The standardized means and standard deviations for contact, activities, and commitment of each cluster are presented in Table 3 and are plotted in Figure 2. Grandfathers in Cluster 1, nearly a third of the participants, scored highest on contact, activities, and commitment and were given the name involved. More than half of the grandfathers, those in Cluster 2, were named passive because they scored near the mean of 0 on contact, activities, and commitment. Sixteen percent of grandfathers scored more than a full standard deviation below the mean on activities and commitment and nearly a full standard deviation below the mean on contact. This cluster of low scoring men, Cluster 3, was given the name disengaged.

Dendrogram of cluster procedure
Means and (Standard Deviations) of Standardized Variables by Cluster

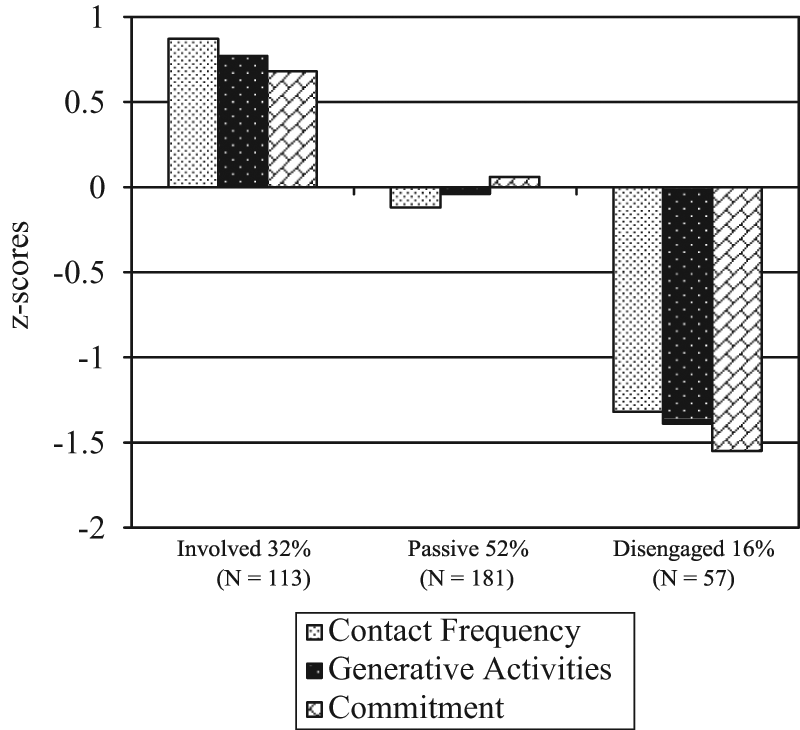
Standardized scale means by grandfather typology
Results of the omnibus comparison tests where cluster is the independent variable and the standardized contact, activities, and commitment are the dependent variables indicated significant between-subjects differences on contact, activities, and commitment. Univariate Fs and follow-up t tests in Table 4 indicate that involved grandfathers had significantly more contact, greater participation in activities, and higher levels of commitment than passive and disengaged grandfathers. Passive grandfathers had significantly more contact, greater participation in activities, and higher levels of commitment than disengaged grandfathers. These findings provide strong evidence that there are indeed three distinct types of grandfathers in this sample. Therefore, the response to the first research question is that a tripartite typology of grandfather involvement was identified with these data.
Univariate F’s and t tests of Comparisons of Standardized Scores by Cluster

Note. Bonferroni adjustments made for multiple t-test comparisons.
p < .001. **p < .0001.
Mental Health ANOVAs
ANOVAs indicated significant cluster effects for depressive symptoms, F(2, 348) = 3.36, p < .05, and positive affect, F(2, 348) = 3.78, p < .05. As presented in Table 5, follow-up t tests with stringent Bonferroni adjustments indicated that grandfathers in Cluster 1 (involved) had significantly fewer depressive symptoms than grandfathers in Cluster 3 (disengaged). No other comparisons were significant for depressive symptoms.
Adjusted Mean Comparisons

Note. Stringent Bonferroni adjustments were made for multiple t test comparisons.
p < .07, **p < .05
Mean comparisons with Bonferroni adjustments indicated that grandfathers in Cluster 1 (involved) had significantly greater levels of positive affect than grandfathers in Cluster 3 (disengaged). Additionally, grandfathers in Cluster 2 (passive) were trending toward significantly greater levels of positive well-being than those in Cluster 3 (disengaged). There was no evidence for differences between grandfathers in Cluster 1 (involved) and Cluster 2 (passive) on positive affect. These findings address our second research question such that more highly involved grandfathers had fewer depressive symptoms and greater positive affect than less involved grandfathers.
Discussion
Research on the mental health of aging men is limited, and research on the mental health of grandparents has generally taken a deficit perspective showing how negative occurrences in intergenerational relationships are associated with greater depressive symptomatology. This study is a first step in highlighting how positive aspects of interaction between grandfathers and grandchildren are related to fewer depressive symptoms and greater positive affect.
To make comparisons among grandfathers, three groups of participants were inductively created from information about their frequency of contact with, participation in activities with, and commitment to a target grandchild. The cluster of men with the highest scores on contact, activities, and commitment was given the name of involved, those with the lowest scores were given the name disengaged, and those scoring in between the two were named passive. Not only are these groups conceptually distinct, but our findings indicate that they are also statistically unique on all three of the variables. The wide variations in these scores are consistent with previous grandparent research that report wide variations in grandparent engagement with grandchildren (Mueller et al., 2002). Given that much of the current grandparent literature has focused on grandmothers’ roles in the family system (Bates, 2009a), the typology developed here extends existing research and indicates that grandfathers are not equally engaged in grandfatherhood.
Findings from this study also indicate that combined scores on relational, behavioral, and social–cognitive aspects of intergenerational relationships are indeed associated with two dimensions of aging men’s mental health. According to the comparison tests, involved grandfathers reported significantly more positive affect than disengaged grandfathers, and passive grandfathers had greater levels of positive affect than disengaged grandfathers. In addition, involved grandfathers had significantly fewer depressive symptoms than disengaged grandfathers.
One way to interpret these findings is that grandfathers benefit emotionally from the interaction they participate in with their grandchildren. Involved grandfathering may not only improve positive affect but it may have preclusive effects on the development of depressive symptoms. A second consideration is that grandfathers with fewer depressive symptoms are emotionally more capable of participating in their grandchildren’s lives. Emotionally, healthy grandfathers may engage in more contact and activities with grandchildren and demonstrate more commitment than grandfathers who are emotionally unhealthy.
The findings of this study also suggest that men who have limited interaction with their grandchildren may be most at risk for the development of depressive symptoms. Those experiencing depressive symptoms are less likely to initiate social interaction and may thus further isolate themselves from grandchildren and other family members.
Implications for Practice and Service Delivery
Implications for practitioners can be drawn from the findings of this study. Mental health professionals working with grandfathers who suffer with depressive symptoms can encourage their clients to become more involved with their grandchildren. For instance, practitioners can establish specific goals to help grandfathers engage in more frequent contact with grandchildren, participate in activities with grandchildren, and find ways to develop and demonstrate greater commitment. In addition to working with grandfathers, practitioners, operating within a systems theory perspective, may consider teaching children and grandchildren how to encourage grandfathers’ efforts to be more involved intergenerationally. In reaching out to grandfathers, adult children and grandchildren may help grandfathers work through challenges related to mental illness.
Some grandfathers may not be involved with grandchildren because of fears over the generation gap and the digital divide (Aarsand, 2007; Harwood & Lin, 2000). It is important for communities to make outlets for men available where they can share their grandfathering experiences with other grandfathers. Grandparents raising grandchildren often find support groups helpful in coping with the challenges of custodial care and finding ways to connect with grandchildren (Park, 2009). However, to our knowledge there are no opportunities for traditional, noncustodial grandfathers to learn from other grandfathers about how to become more involved. Senior citizen centers and other community organizations should consider planning special events and activities where grandfathers can learn how to be more involved with their grandchildren and become more familiar with technological communication. Helping facilitate times and locations for grandfathers to meet together and talk about their experiences may provide avenues for them to learn from each other. Learning may lead to becoming more involved with grandchildren and eventually to opportunities to enhance positive well-being and decrease feelings associated with depression.
Limitations and Future Research Opportunities
This analysis has several limitations. First, the sample was taken by convenience and may not necessarily be representative of grandfathers living throughout United States or those of minority status. Thus, caution should be taken when generalizing to other populations. Although a large and diverse sample of grandfathers was recruited, future research should seek to recruit more minorities. Indeed, there is great underrepresentation in the aging literature on the mental health of men of color (Kosberg & Mangum, 2002; Love & Love, 2006). In addition, the use of undergraduate students as contact persons to recruit a sample of convenience may have introduced some bias into the sample. Future research should employ random sampling techniques to recruit grandfather participants. Second, the sample was community-dwelling with a relatively limited incidence of clinically relevant depressive symptoms. Future research should investigate institutionalized grandfathers and/or those who suffer from more severe depression. Third, because grandfathers were free to select any of their grandchildren on which to report, many grandfathers selected a grandchild with whom they interacted and had developed sentiments of closeness. Men with multiple grandchildren with whom they have equally close relationships might benefit emotionally from the cumulative effects of all such relationships. Although it would be difficult to determine that with these data, such an effect may confound well-being outcomes for those who do not have multiple grandchildren. Finally, the comparison of clusters of men was based on cross-sectional data. As such, it is not possible to determine historical ebbs and flows either in mental health or in interpersonal interaction with grandchildren. Future research should investigate grandfather–grandchild relationships longitudinally to gain insights into the effects of time and history on intergenerational relationships and mental health.
This study is a first step in understanding which aspects of intergenerational interaction are associated with depressive symptoms and positive affect. It can be concluded from the findings of the study that combinations of contact, activities, and commitment formed three distinct grandfather clusters. It can also be concluded that meaningful and involved interaction with grandchildren is an important contribution to the mental health of aging men and that those who interact least with grandchildren may be at greater risk for depressive symptomatology.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a USDA Hatch grant to the first author through the Agricultural Experiment Station at South Dakota State University.