
Abstract
This paper provides an overview of the mixed-methods evaluation of the Better Access to Psychiatrists, Psychologists and General Practitioners through the Medicare Benefits Schedule initiative (Better Access) that we conducted in 2021–2022. It is the first of 10 papers in this special issue of the Australian and New Zealand Journal of Psychiatry; the other nine report on individual studies that were components of the evaluation. This paper summarises the key findings, highlighting that although many of those who use Better Access achieve positive improvements in symptoms, levels of functioning and quality of life, there are inequities in access to the programme. Based on our findings, we made 16 recommendations relating to: complementary service delivery models; workforce capacity, composition and distribution; therapies available through Better Access; referring people to the most appropriate care; fostering communication and collaboration between providers; affordability; session numbers; session modality; services for people in residential aged care facilities and routinely assessing outcomes. We report on the Australian Government’s response to these recommendations.
We evaluated Australia’s largest primary mental health care programme, the Better Access to Psychiatrists, Psychologists and General Practitioners (GPs) through the Medicare Benefits Schedule (MBS) initiative (Better Access) in 2021–2022. The evaluation involved 10 studies, and this Australian and New Zealand Journal of Psychiatry issue reports on nine of them (Arya et al., 2026; Chilver et al., 2026; Currier et al., 2026; Harris et al., 2026; Pirkis et al., 2026a; Pirkis et al., 2026b; Newton et al., 2026; Tapp et al., 2026a; Tapp et al., 2026b). This paper synthesises the evaluation’s key findings, cross-referencing other papers in the issue. It also outlines our recommendations and the Australian Government’s response to these and highlights lessons that may apply in international contexts.
Better Access
Introduced in 2006, Better Access aims to improve mental illness treatment in the community. It enables people with diagnosed mental disorders to access evidence-based mental health treatment (psychological therapy services and focussed psychological strategies) from eligible providers (clinical and registered psychologists, social workers, occupational therapists, GPs, prescribed medical practitioners [PMPs] and psychiatrists). Better Access services are funded by Medicare (Australia’s universal health insurance scheme) which subsidises the cost of hospital services, medical services, tests, imaging and scans through the MBS, via a series of item numbers which are associated with a schedule fee. Eligible consumers can claim 100% of this fee as a benefit for GP services and 85% for non-GP services. Providers can charge above the schedule fee, so consumers often pay a co-payment.
The commonest Better Access pathway involves a GP or PMP preparing a mental health treatment plan (MHTP) and referring the consumer to an allied health professional. The consumer can then access a designated number of treatment sessions with the allied health professional. This is a maximum of 10 individual and 10 group sessions per calendar year, with the initial referral of up to six sessions. After this, and upon receipt of a written report from the allied health professional, the GP may refer the consumer for further sessions (up to the maximum) after reviewing the consumer’s MHTP.
Better Access ‘rules’ have changed over time. Two key changes occurred in response to the mental health impacts of the COVID-19 pandemic, which overlapped with our evaluation period. First, the number of available sessions temporarily increased from 10 to 20; the additional 10 sessions ceased as planned in 2022. Second, sessions could be provided by phone/telehealth rather than just face-to-face; these arrangements have continued. Eligibility for telehealth services for group psychological therapy services and focussed psychological strategies is based on the Modified Monash Model (MMM) (Australian Government Department of Health and Aged Care, 2024b). During the telehealth appointment, an eligible consumer must be located in an MMM 4–7 area and be a minimum of 15 km away by road from the allied health professional.
Better Access is complemented by other Australian Government-funded services (e.g. mental health services commissioned by Primary Health Networks [PHNs]), public hospital and community mental health services funded by state/territory governments, and private hospitals.
The evaluation
We were commissioned by the (then) Department of Health and Aged Care on 9 August 2021 to evaluate Better Access and delivered our final report on 8 December 2022 (Pirkis et al., 2022). The evaluation was overseen by a Stakeholder Engagement Group and a Clinical Advisory Group.
As noted, this Australian and New Zealand Journal of Psychiatry issue reports on nine of the evaluation’s 10 studies. These are analysis of MBS data (Tapp et al., 2026b); analysis of linked administrative data (Chilver et al., 2026); a study using routinely-collected consumer outcome data (Pirkis et al., 2026a); a survey of consumers who had used Better Access in the previous year (Pirkis et al., 2026b); re-analysis of data from two randomised controlled trials (Harris et al., 2026); analysis of data from two longitudinal studies (Arya et al., 2026); qualitative interviews with users/non-users of Better Access (Newton et al., 2026); a survey of providers/referrers (Tapp et al., 2026a) and a consultative virtual forum on future Better Access reforms (Currier et al., 2026). The tenth study was a routine outcome data collection pilot, described in our final report (Pirkis et al., 2022).
Key findings
The evaluation revealed consistent findings about Better Access regarding outcomes and access. Those who received treatment through Better Access tended to have positive outcomes, irrespective of how outcomes were measured (Arya et al., 2026; Harris et al., 2026; Pirkis et al., 2026a; Pirkis et al., 2026b). These outcomes were not related to levels of socioeconomic advantage/disadvantage, which is positive (Arya et al., 2026; Harris et al., 2026; Pirkis et al., 2026a; Pirkis et al., 2026b). Instead, they were associated with levels of need (operationalised in various ways, usually via cut-offs on standardised measures), with those with relatively severe depression, anxiety and/or psychological distress showing the greatest improvement over episodes of Better Access care (Arya et al., 2026; Harris et al., 2026; Pirkis et al., 2026a; Pirkis et al., 2026b).
There were also indications that relatively greater session numbers may lead to better outcomes, but this was not so clear-cut. Most of the studies that considered outcomes showed that higher session numbers were associated with improvement in outcomes (Harris et al., 2026; Pirkis et al., 2026a; Pirkis et al., 2026b). However, because session numbers were aggregated in different ways and the relationship between session numbers and improvement was not linear, it was not possible to identify ‘optimal’ session numbers.
Regarding access, we observed that Better Access has continued to expand, with over 10% of Australians receiving any Better Access service in 2021 and around 5% receiving at least one session of psychological treatment through the programme (Chilver et al., 2026; Tapp et al., 2026b). However, this should be considered in the context of 21% of adults experiencing a mental disorder in 2021 (Australian Bureau of Statistics, 2022). Not all of these people would have needed care, and some may have sought care elsewhere, but there are certainly people who would have benefitted from Better Access who were not accessing it. At the same time, Better Access appeared to be providing services to some people with relatively lower levels of need who could potentially have been supported through other means.
The evaluation suggested that increases in Better Access treatment utilisation disproportionately favoured people on relatively higher incomes in major cities (Chilver et al., 2026; Tapp et al., 2026b). Affordability was consistently raised as an issue by consumers and providers (Currier et al., 2026; Newton et al., 2026; Pirkis et al., 2026b; Tapp et al., 2026a). In 2021, 65% of Better Access treatment services attracted a co-payment compared with 53% in 2018 (Tapp et al., 2026b). The median co-payment for these services sat at $74 per session in 2018–2021 but increased significantly in the first half of 2022 to $90 (Tapp et al., 2026b).
Recommendations
On the basis of our evaluation findings and in the context of relevant reviews and policy frameworks (Australian Commission on Safety and Quality in Health Care, 2022; Australian Government Department of Health, 2022; Commonwealth of Australia and the States and Territories, 2022; Australian Government Department of Health and Aged Care, 2022a; Australian Government Department of Health and Aged Care, 2022b; House of Representatives Select Committee on Mental Health and Suicide Prevention, 2021; Medicare Benefits Schedule Review Taskforce, 2020; Productivity Commission, 2020), we made 16 recommendations (Table 1). These related to complementary service delivery models; workforce capacity, composition and distribution; therapies available through Better Access; referring people to the most appropriate care; fostering communication and collaboration between providers; affordability; session numbers; session modality; services for people in residential aged care facilities; and routinely assessing outcomes (Pirkis et al., 2022).
Recommendations from the evaluation and the Australian Government’s response.
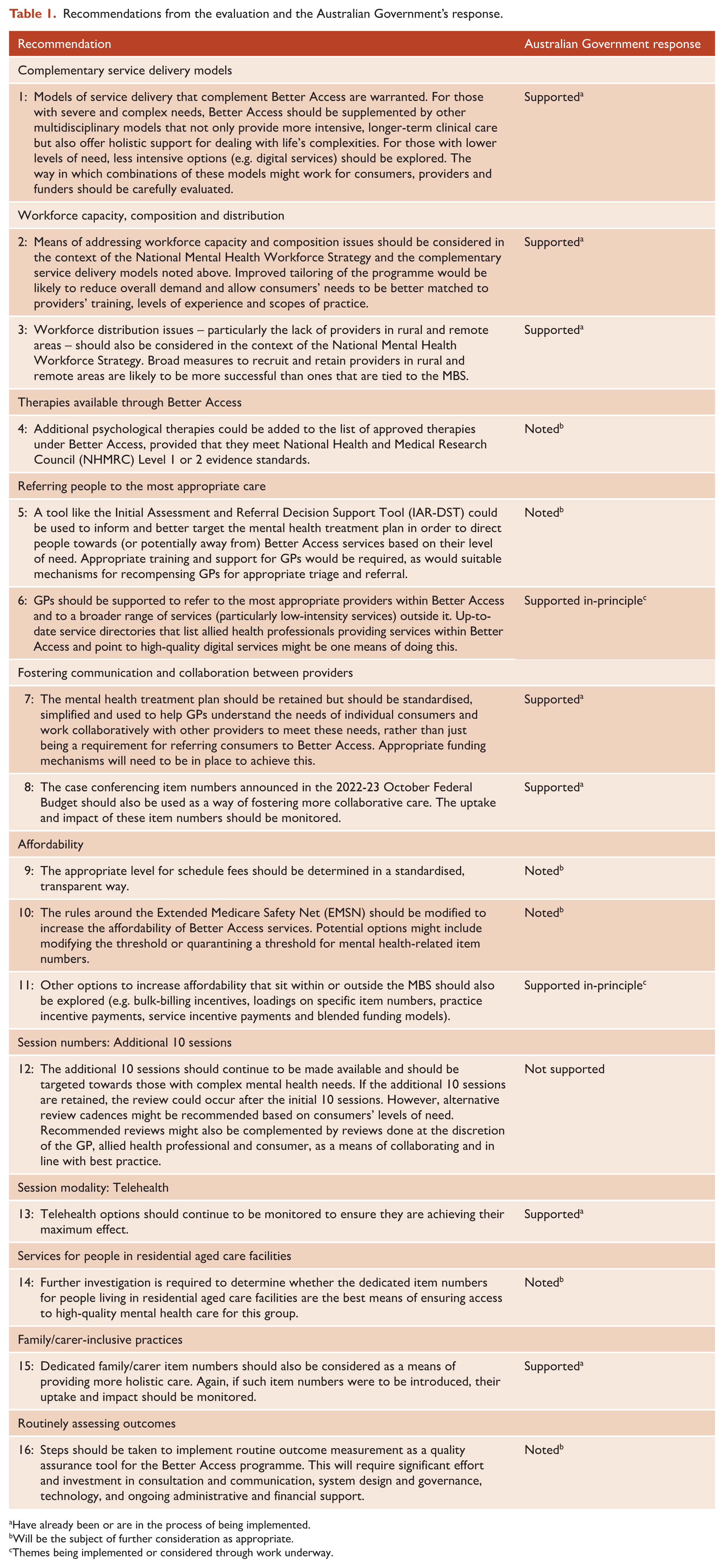
Have already been or are in the process of being implemented.
Will be the subject of further consideration as appropriate.
Themes being implemented or considered through work underway.
The Australian Government responded to these recommendations on 16 August 2024 (Australian Government Department of Health and Aged Care, 2024a), supporting seven of them, providing in-principle support for two, noting six and not supporting one (Table 1). Additional changes to Better Access have occurred since, with the most recent relating to services delivered by GPs and PMPs (Australian Government Department of Health, Disability and Ageing, 2025).
Examples are provided below from three areas in which we made recommendations that relate to the whole Better Access programme or major components of it (complementary service delivery models; affordability; and session numbers). The examples outline our rationale for the recommendations and the Australian Government’s response to them.
Our rationale
Our evaluation showed that Better Access is delivering care to people with varying needs (Arya et al., 2026; Chilver et al., 2026; Harris et al., 2026; Pirkis et al., 2026a; Pirkis et al., 2026b). We provided evidence that Better Access benefits people with severe and complex mental health conditions, with several studies showing that improvements in outcomes were greatest for those with the highest levels of need (Arya et al., 2026; Harris et al., 2026; Pirkis et al., 2026a; Pirkis et al., 2026b). However, consumers and providers who participated in the evaluation suggested that people with complex needs may require more multidisciplinary and holistic care than Better Access can deliver (Currier et al., 2026; Newton et al., 2026; Tapp et al., 2026a).
Our evaluation also suggested that Better Access may not always be ideal for people with lower levels of need. Several of our studies suggested that this group is likely to show the least benefit regarding changes in symptoms, levels of functioning and quality of life (Arya et al., 2026; Harris et al., 2026; Pirkis et al., 2026a; Pirkis et al., 2026b). We argued that some people with lower levels of need might be well served by other services (e.g. digital options).
Australian Government response
The Australian Government supported Recommendation 1 (Australian Government Department of Health and Aged Care, 2024a). It is investing in complementary models that offer multidisciplinary care (e.g. providing $29.9M over 4 years from 2024-2025 to expand Medicare Mental Health Centres and $71.7M over the same period to enable PHNs to provide free, multidisciplinary, wrap-around care through primary care settings). It is also providing $588.5M over 8 years from 2024-2025 and $113.4M per year ongoing for a new national early intervention service for people experiencing mild mental health concerns or transient distress. This service will be free, will not require a diagnosis and will capitalise on phone, video and online technologies.
Our rationale
A key evaluation finding was that although Better Access has enabled many people to access mental health care, cost remains an issue. Those who are relatively more socioeconomically disadvantaged are less likely to use Better Access treatment (Chilver et al., 2026; Tapp et al., 2026b), despite their comparatively higher levels of need (Chilver et al., 2026). People on low incomes are less likely to receive treatment following a MHTP than their wealthier counterparts and to wait longer for their first treatment session if the MHTP is followed by treatment (Chilver et al., 2026). This disparity is likely to have been exacerbated recently by co-payment increases, noted above (Tapp et al., 2026b). Consumers, providers and other stakeholders indicated that affordability was a major concern (Currier et al., 2026; Newton et al., 2026; Pirkis et al., 2026b; Tapp et al., 2026a), with participants in our consultative virtual forum ranking improvements to affordability as the highest priority for future Better Access reforms (Currier et al., 2026).
Providers who contributed to our evaluation noted that they set their fees above schedule fee levels because the schedule fees have not always kept pace with indexation, and private practice running costs have risen (Currier et al., 2026; Tapp et al., 2026a). This has impacted out-of-pocket costs for consumers.
Australian Government response
The Australian Government noted Recommendations 9 and 10, indicating that the MBS Continuous Review programme will inform future MBS policy, making mention of other activities funded through a $361M mental health package that expands the range and reach of free mental health services, and committing to establishing a working group to review Medicare Safety Nets. The Australian Government supported in-principle Recommendation 11, citing changes to Better Access that will allow GPs to use standard consultations for mental health care (increasing the MBS benefit for GP mental health consultations) and provide incentives for them to bulk-bill concession card holders and children. The Australian Government also noted that it is reviewing general practice incentives.
Our rationale
As noted, 10 additional sessions with an eligible provider became available during the pandemic. The evaluation considered the advantages and drawbacks of these additional sessions. On one hand, the additional sessions were welcomed by many stakeholders. For example, three-quarters of the participants in the consultative virtual forum felt that the additional sessions should be retained, and 90% indicated that potentially even more sessions should be available for people with complex needs (Currier et al., 2026). In the main, our outcome-related studies indicated that levels of improvement were associated with the number of sessions consumers received (Harris et al., 2026; Pirkis et al., 2026a; Pirkis et al., 2026b).
On the other hand, the evaluation suggested that provision of additional sessions to existing consumers may have limited providers’ capacity to offer treatment to new users; the number of continuing users of Better Access services and the number of sessions provided for them increased markedly in 2020 and 2021, whereas the figures for new users remained stable (Chilver et al., 2026). There was also evidence that the additional sessions were not specifically targeted to consumers with complex needs. In our survey of Better Access consumers, patterns of self-reported baseline mental health were almost identical for those who did and did not receive the additional sessions (Pirkis et al., 2026b).
Australian Government response
The Australian Government did not support Recommendation 12. Its decision was influenced by the fact that the number of new consumers decreased while the additional 10 sessions were available and revolved around concerns that reinstating the additional sessions risked further entrenching inequities. It noted that people with complex needs might be better served by alternative options delivered through a whole-of-system mental health response, including through the new Medicare Mental Health Centres and PHNs. It also noted that the new national early intervention service will improve service availability across the stepped-care continuum.
Lessons from the evaluation
Better Access sits within Australia’s broader mental health system and is embedded within Medicare’s fee-for-service framework. Other countries deliver primary mental health care differently, via other systems (Chodos, 2017). Nonetheless, some lessons from our evaluation may apply internationally.
Consumers in any primary mental health care scheme are likely to have a range of needs. Our evaluation showed this was the case with Better Access (Arya et al., 2026; Chilver et al., 2026; Harris et al., 2026; Pirkis et al., 2026a; Pirkis et al., 2026b). Those with severe and complex needs are likely to require more intensive, holistic care than those with relatively lower levels of need. The scope of any primary mental health care scheme should be clearly articulated, as should the way it complements and is augmented by other parts of the mental health system.
Balancing access and outcomes is important. Our evaluation suggested that those who receive Better Access care tend to have positive outcomes (Arya et al., 2026; Harris et al., 2026; Pirkis et al., 2026a; Pirkis et al., 2026b), but that there are inequities in access relating to socioeconomic disadvantage and living outside cities (Chilver et al., 2026; Tapp et al., 2026b). Other primary mental health care schemes are likely to experience similar issues. Various policy levers may be required to boost equity of access without detrimentally affecting outcomes.
The way in which any primary mental health care scheme operates will create incentives/disincentives for providers and consumers (Ashcroft et al., 2014; Flodgren et al., 2011). Better Access providers told us they found it increasingly necessary to charge co-payments to cover their costs (Currier et al., 2026). Consumers indicated that they were sometimes disinclined to seek care for financial reasons (Newton et al., 2026). Consideration should be given to the provider and consumer behaviours that any scheme is likely to lead to.
Conclusions
Moving forward, it will be important to maintain positive outcomes for those who use Better Access while increasing access for those who are currently missing out. Improved targeting of Better Access and consideration of how it interfaces with other elements of the mental health system warrant attention. Maximising affordability to reduce inequities will be critical.
Footnotes
Acknowledgements
The Better Access Evaluation was funded by the Australian Government Department of Health, Disability and Ageing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The evaluation of Better Access was funded by the Australian Government Department of Health, Disability and Ageing.
Data accessibility statement
The data sets generated and analysed for the evaluation are not available.