
Abstract
The combination of socioeconomic profile, rurality, and Better Access sessions accounted for a small but significant percentage of variance (7%) in the number of ATAPS sessions delivered, with a non-significant independent contribution of Better Access sessions to the prediction of ATAPS sessions. Weak but significant relationships between ATAPS sessions and each of socioeconomic profile (r = 0.22) and rurality (r = −0.24), respectively, were identified.
In comparison, socioeconomic profile, rurality, and ATAPS sessions accounted for a much larger and significant percentage of variance (46%) in number of Better Access sessions delivered, with a non-significant independent contribution of ATAPS sessions to the prediction of Better Access sessions. Moderate significant relationships between Better Access sessions and each of socioeconomic profile (r = 0.46) and rurality (r = −0.66), respectively, were identified.
The introduction of Better Access appears to have halted the steady increase in the number of ATAPS sessions previously observed. This finding should be interpreted alongside the fact that ATAPS funding is capped.
Keywords
Over the past decade significant milestones in Australian mental health reforms have been addressing gaps in the provision of accessible and evidence-based psychological treatment. The responsiveness of the reforms constitute increasing recognition that mental health is a serious public health concern as evidenced by the significant and increasing prevalence of mental disorders [1,2] and the corresponding substantial contribution to Australia's burden of disease [3]. The reforms also represent increasing acknowledgement of the effectiveness of psychological treatments [4–7] delivered by psychologists [8] and other appropriately trained mental health professionals.
In an effort to improve access to effective primary mental health care, the Better Outcomes in Mental Health Care programme was introduced in July 2001, followed by the initiation of the Better Access to Psychiatrists, Psychologists and General Practitioners (GPs) through the Medicare Benefits Schedule (Better Access) programme in November 2006. Both programmes enable GPs to refer consumers to psychologists and other allied health professionals for (government subsidized) evidence-based sessions of focussed psychological strategies. Key characteristics of both programmes are elaborated below.
The Better Outcomes in Mental Health Care programme
The Better Outcomes in Mental Health Care programme, introduced in 2001, aims to improve consumers’ access to high quality primary mental health care via two components: provision of referral pathways to allied health professionals; and access to patient management advice from psychiatrists [9]. The referral pathway component is formally known as Access to Allied Psychological Services (ATAPS) and supports GPs and allied health professionals (predominantly psychologists, but also social workers, mental health nurses, occupational therapists and Aboriginal and Torres Strait Islander health workers) to collaborate to provide optimal mental health care. Specifically, this component enables GPs to refer consumers with high prevalence mental disorders to allied health professionals for up to 12 (or 18 in exceptional circumstances) individual and/or group sessions of government subsidized evidence-based focussed psychological strategies per calendar year. This collaborative approach to mental health care is occurring through 106 ATAPS projects being conducted by the Divisions of General Practice (Divisions). Divisions receive set funding for these projects from the Australian Government Department of Health and Ageing. A range of service delivery models are used by the Divisions to implement the projects, which vary across several dimensions including: means of retaining allied health professionals (employment or contractual); location of allied health professionals; and referral mechanism [10].
The Better Access programme
The Better Access programme was introduced in November 2006 as a cornerstone of the Council of Australian Governments (COAG) reform package of $1.9 billion over five years, with $507 million committed specifically to the Better Access component of the package [11]. The Better Access programme is designed to improve access to psychologists, psychiatrists, GPs and other allied health providers for people with clinically diagnosed mental disorders via a series of new Medicare Benefits Schedule (MBS) item numbers [12].
Amongst the modifications to the MBS was the addition of a set of item numbers that make the services of registered psychologists (and selected social workers and occupational therapists) eligible for a rebate. Similar to the ATAPS projects, under the new item numbers, a GP can refer a consumer to an allied health professional for up to 12 (or 18 in exceptional circumstances) individual and/or group sessions of evidence-based focussed psychological strategies per calendar year. Allied health professionals who are registered with Medicare Australia (the body that administers the MBS) can directly bill Medicare or can bill the consumer who can then obtain a partial or full rebate from Medicare Australia [12].
Relationship between ATAPS projects and Better Access
Prior to the introduction of the Better Access programme, the uptake of the ATAPS projects was substantial and had increased over time, as more Divisions became involved, with particularly notably high uptake in rural areas, where proportionally larger numbers of consumers had received care [13]. Earlier examination of the impact of Better Access in its first five months on uptake of ATAPS demonstrated that service delivery was initially reduced, but then remained fairly constant and that the programmes were complementary in addressing a previously unmet need [14].
Furthermore, despite a general consensus that the Better Access programme is a timely and appropriate response to a serious public health problem, it has been subject to a number of criticisms. Two key criticisms pertain to equity of geographic and socioeconomic access, raising concerns about whether Better Access services are accessible to those most in need of financially supported psychological treatment [8,15]. In addition, the dramatic uptake of the Better Access programme raises the question about its potential to usurp the services provided by the ATAPS projects. These criticisms and concerns formed the impetus for the current study, which was strengthened by previous Australian research findings demonstrating inequity of access to psychological treatment. Specifically, socioeconomically advantaged female consumers are reportedly more likely to utilize allied health professionals (including psychologists and social workers) [16]. In addition, income support recipients are reported to have a higher prevalence of both psychological distress and diagnosable mental disorders while being no more likely to utilize services than non-recipients [17]. Furthermore, among other sociodemographic factors, location (rurality) has been found to predict help-seeking from a formal mental health professional, with help-seeking being more common amongst individuals living in medium-sized towns than those living in large regional cities [18]. This study aimed to explore the reciprocal impact of the uptake of psychological treatment under the two initiatives and the impact of location (rurality and socioeconomic profile) on the uptake of both programmes since the inception of the Better Access programme. The uptake of ATAPS before and after the introduction of the Better Access programme was also investigated.
Method
General Practice Divisional-level data on the number of sessions provided through the ATAPS projects were extracted from a web-based and password protected minimum dataset, which routinely captures de-identified consumer-level and session-level information from the projects. This dataset was developed for an ongoing independent evaluation of the ATAPS projects by the University of Melbourne, which is funded by the Australian Department of Health and Ageing. Session data on services rendered by allied health professionals under the Better Access programme were made available by the Medicare Benefits Branch of the Australian Department of Health and Ageing. Specifically, the Medicare Benefits Branch extracted monthly postcode-level session data and aggregated these data so that all of the postcode areas within a given Division were combined for a given month. Data were available from both sources for 105 Divisions from 1 November 2006 to 31 July 2008. ATAPS data from the minimum dataset were available from 1 January 2002 to 31 December 2008.
The Rural, Remote and Metropolitan Areas (RRMA) classification for each Division was sourced from the Division Benchmarking Tool developed by the Primary Health Care Research and Information Service [19]. The 2007–2008 Annual Survey of Divisions uses the RRMA classification system in order to allocate Divisions according to rurality, taking into account that multiple statistical local areas (SLAs) contribute to each Division [20]. The RRMA classification system was developed in 1994 as a remoteness classification based on 1991 population census data and SLA boundaries [21]. RRMA classifies SLA according to population and locality into three zones: Metropolitan, Rural or Remote. These zones are further divided into seven classes: Capital cities (RRMA category 1), Other metropolitan centres (RRMA category 2), Large rural centres (RRMA category 3), Small rural centres (RRMA category 4), Other rural centres (RRMA category 5), Remote centres (RRMA category 6), and Other remote areas (RRMA category 7).
An Index for Relative Socio Economic Disadvantage (IRSED) was provided for each Division by the Public Health Information Development Unit in Adelaide and have since been published online [22]. The indices were generated by using each relevant Socio Economic Index for Area (SLA), produced by the Australian Bureau of Statistics based on information collected in the Australian 2006 Census of Population and Housing. Population weighted average IRSED for each Division accounted for multiple SLAs, each with their own index.
Data management and analyses
Data from the four sources was synthesized into one SPSS file, which only included data from 105 Divisions where both ATAPS and Better Access data were available. Some Divisions (projects) did not have session data in the minimum dataset for specific months within the data analysis period. When this was attributable to the absence of a corresponding ATAPS project or data entry issues (as opposed to the actual absence of session delivery for that month), the corresponding monthly Better Access data for that Division was excluded from the analysis. Where it was definite that no sessions were delivered for that month, the ATAPS project was retained in the analysis and the number of sessions was correspondingly recorded as zero. There were four Divisions that had Better Access sessions but have never run an ATAPS project, therefore these Divisions were excluded.
Descriptive statistical analyses and two regression analyses were performed in order to examine the reciprocal impact of the two programmes and the impact of rurality and socioeconomic status on each programme.
To examine the change in uptake of ATAPS sessions since the introduction of the Better Access programme, a further two regression analyses were performed using data from the minimum dataset from January 2002 to December 2008. One regression examined the uptake of ATAPS from January 2002 to October 2006 (pre-Better Access) and the other examined the uptake of ATAPS from November 2006 to December 2008 (post-Better Access). This dataset included data from all ATAPS projects.
Results
Table 1 provides a descriptive comparison of session characteristics of both programmes. Of the ATAPS project sessions, 45% (or 92,990) were provided in rural areas, compared with 18% (or 439,890) of the Better Access programme sessions. Only a minority of sessions delivered under the ATAPS projects incurred a copayment (15%); comparable data was not available for sessions delivered through Better Access in the context of this study. The average copayment amount was smaller for sessions delivered under the ATAPS projects than for those delivered through Better Access, both in urban ($2.79 versus $19.03) and rural ($0.76 versus $15.31) areas.
Comparison of session delivery under ATAPS projects and Better Access
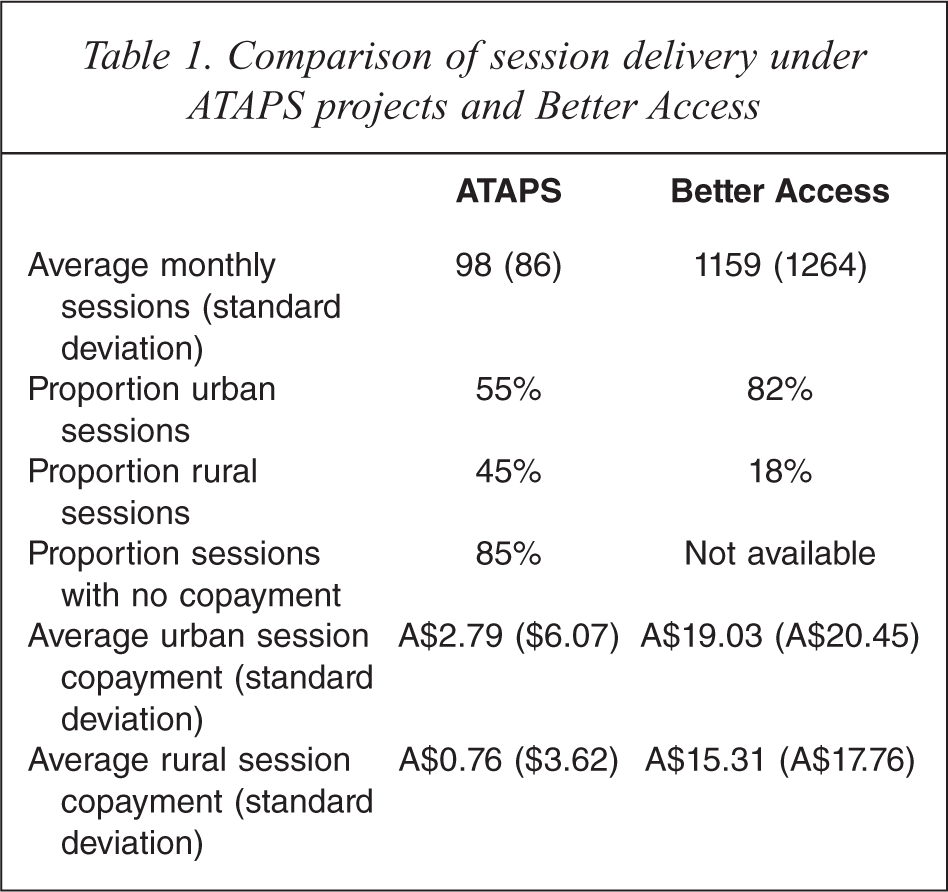
Figure 1 presents the overall number of sessions delivered under each programme in the 21-month observation period. It shows delivery of a total of 206,645 sessions in the analysis period through the ATAPS projects. In contrast, a much more pronounced increase in the number of sessions provided through the Better Access programme in the analysis period is observed, accounting for a total 2,443,835 sessions. This figure is an underestimate of sessions delivered by allied health providers through Better Access due to the data analysis approach described above, whereby Better Access sessions were excluded from the analysis for Divisions not operating ATAPS projects. The actual number of sessions delivered by allied health providers through Better Access in the data analysis period was 2,790,596 (data report available from Medicare website) [23]. It should be acknowledged that uptake of ATAPS sessions is limited by capped funding, whereas the uptake of Better Access is uncapped and demand driven.
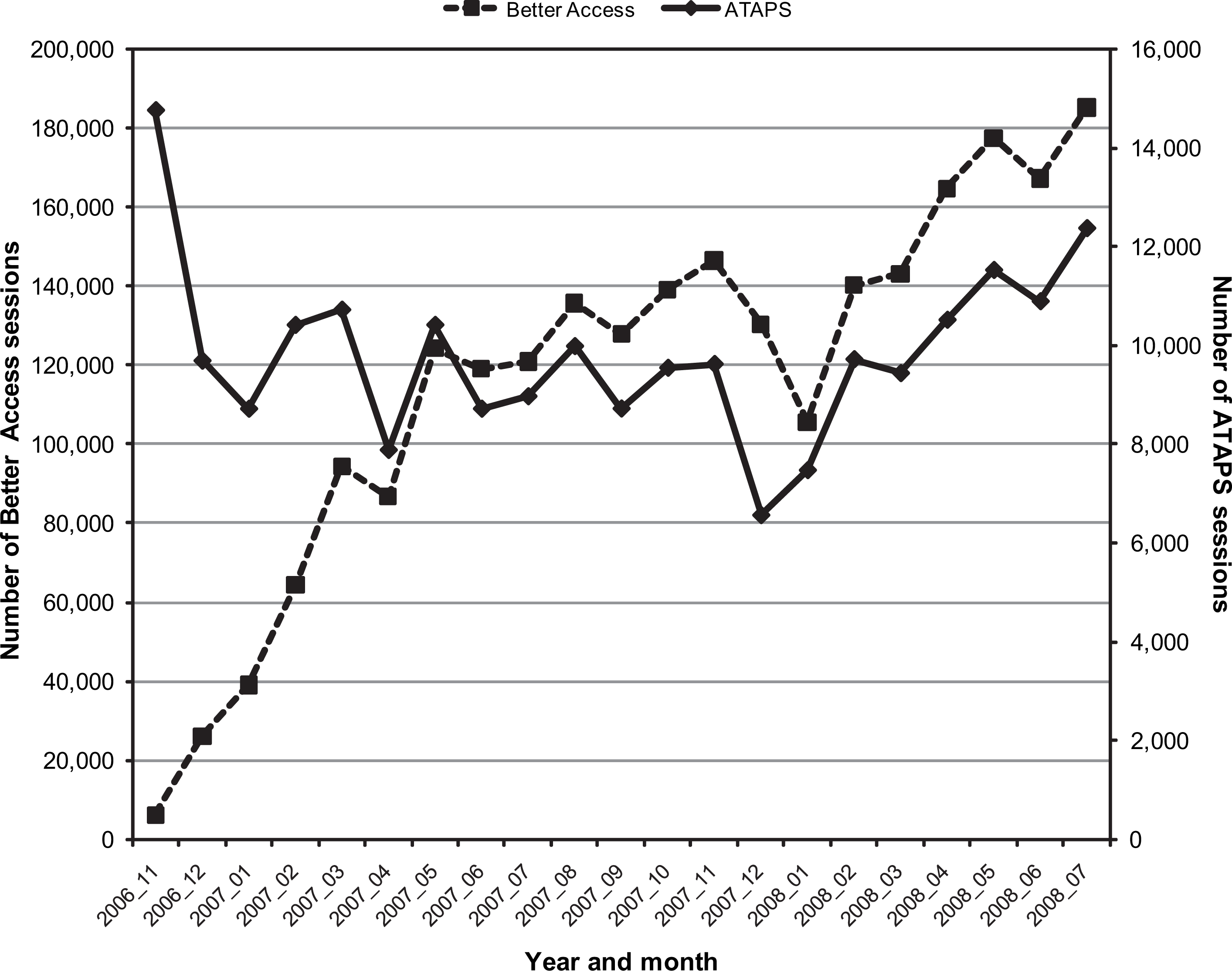
Overall number of sessions provided through Access to Allied Psychological Services projects and Better Access programme from 1 November 2006 to 31 July 2008.
Reciprocal impact of ATAPS projects and Better Access, and impact of location (socioeconomic profile and rurality) on both programmes
Two statistical linear (standard multiple) regression procedures, using SPSS Regression, were conducted. The first of these examined the contribution of IRSED, RRMA and Better Access sessions (independent variables) to the prediction of number of sessions delivered under ATAPS (dependent variable). The second regression examined the contribution of IRSED, RRMA and ATAPS sessions (independent variables) to the prediction of number of sessions delivered under Better Access (dependent variable). It is noted that one of the independent variables, RRMA, is not a continuous variable. However, RRMA may be considered to possess an underlying continuum of rurality. Moreover, particular care was taken to assess the adequacy of regression models, using standard regression model diagnostics. Initially the distributions of the total number of ATAPS and Better Access sessions for each Division were examined and both were found to be non-normal (i.e. significantly positively skewed). Following conventional practice, these distributions were (square root) transformed to better meet the assumptions of normality required for regression analyses [24].
Table 2 displays the correlations between the variables, with a small significant positive association between the numbers of sessions delivered by each programme. There are significant inverse associations between rurality and the number of sessions delivered by both programmes, with the magnitude of this effect being more than doubled for Better Access sessions. Similarly, significant positive relationships between socioeconomic profile and the number of sessions delivered by both programmes were found, with the magnitude of this effect being more than doubled for Better Access sessions.
Correlations between square root transformed numbers of both ATAPS and Better Access sessions, IRSED and RRMA
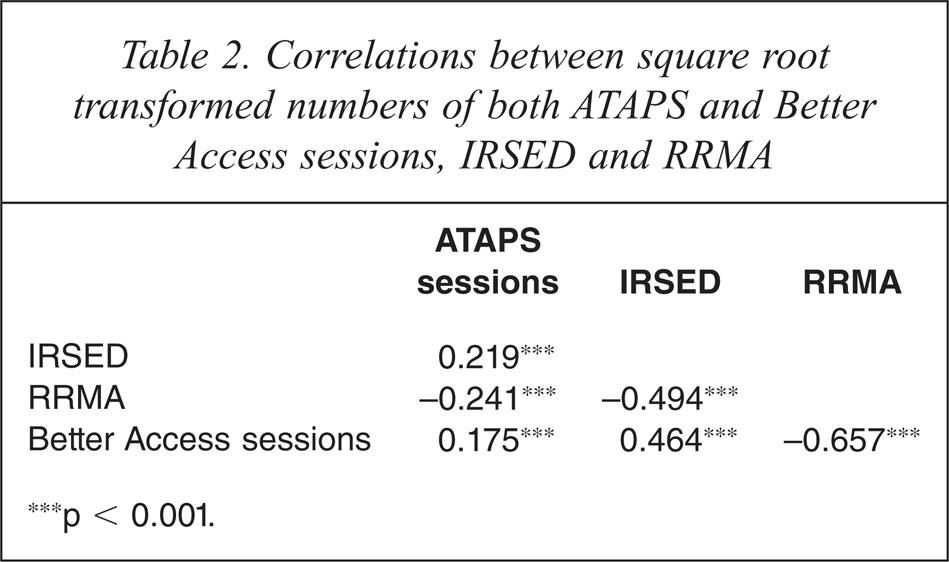
∗∗∗p < 0.001.
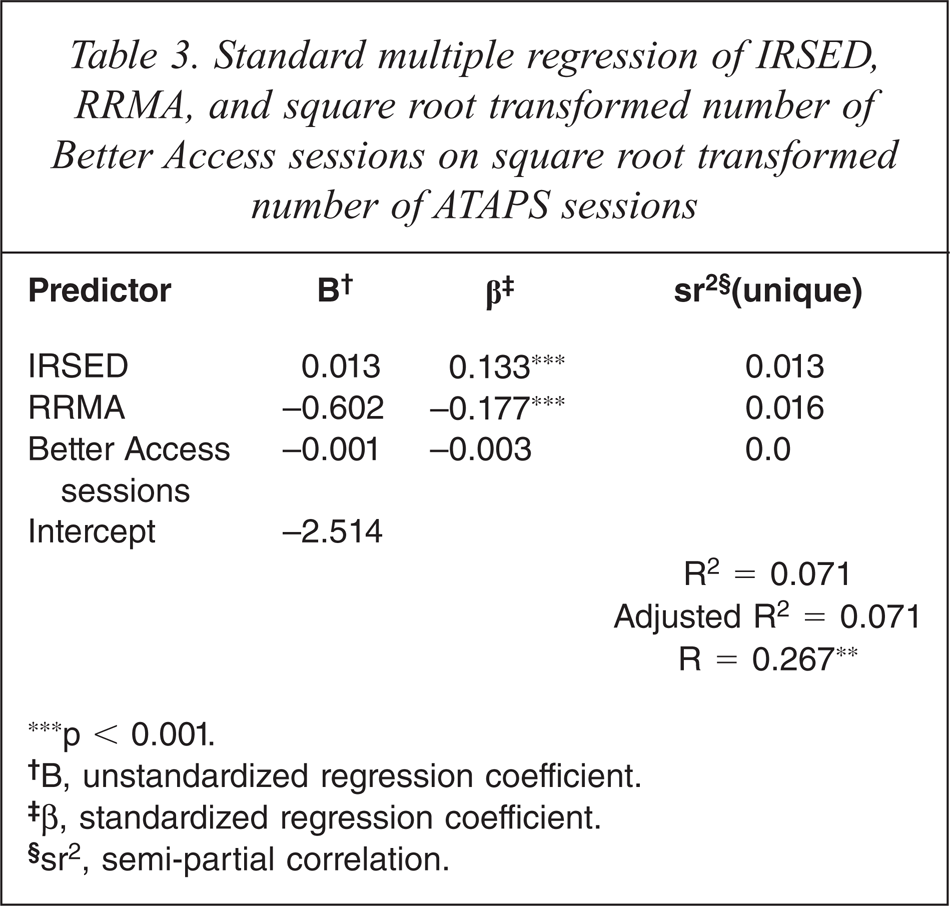
Table 3 presents the regression findings for the equation predicting the number of ATAPS sessions. R for the regression was significantly different from zero, F (3, 2083) = 53.22, p < 0.001. Only two of the independent variables contributed significantly to the prediction of number of ATAPS sessions, IRSED (sr2 = 0.013) and RRMA (sr2 = 0.016), with the three independent variables contributing another 0.041 in shared variability. Altogether, 7% of the variability in number of ATAPS sessions was predicted by knowing scores on these three independent variables. For the two regression coefficients that differed significantly from zero, 95% confidence intervals were calculated. The 95% confidence limits for IRSED were 0.008 to 0.018 and those for RRMA were −0.797 and −0.407.
Standard multiple regression of IRSED, RRMA, and square root transformed number of Better Access sessions on square root transformed number of ATAPS sessions
∗∗∗p < 0.001.
†B, unstandardized regression coefficient.
‡β, standardized regression coefficient.
§ sr2, semi-partial correlation.
Although the correlation between number of ATAPS sessions and number of Better Access sessions was significant (r = 0.175, p = 0.000), the number of Better Access sessions did not contribute significantly to the regression. Post hoc evaluation of the correlation revealed that it was significantly different from zero, F(3, 2083) = 21.49, p < 0.01. The relationship between the number of ATAPS and Better Access sessions is mediated by the relationships between IRSED, RRMA and number of ATAPS sessions.
Table 4 displays the regression findings for the equation, predicting the number of Better Access sessions. R for regression was significantly different from zero, F (3, 2083) = 584.67, p < 0.001. Only two of the independent variables contributed to the prediction of number of Better Access sessions, IRSED (sr2 = 0.026) and RRMA (sr2 = 0.236), with all three independent variables contributing another 0.194 in shared variability. Altogether, 46% of the variability in number of Better Access sessions was predicted by knowing the scores on these three independent variables. For the two regression coefficients that differed significantly from zero, 95% confidence intervals were calculated. The confidence limits for IRSED were 0.064 to 0.096 and those for RRMA were −9.117 to −8.002.
Standard multiple regression of IRSED, RRMA, and square root transformed number of ATAPS sessions on square root transformed number of Better Access sessions
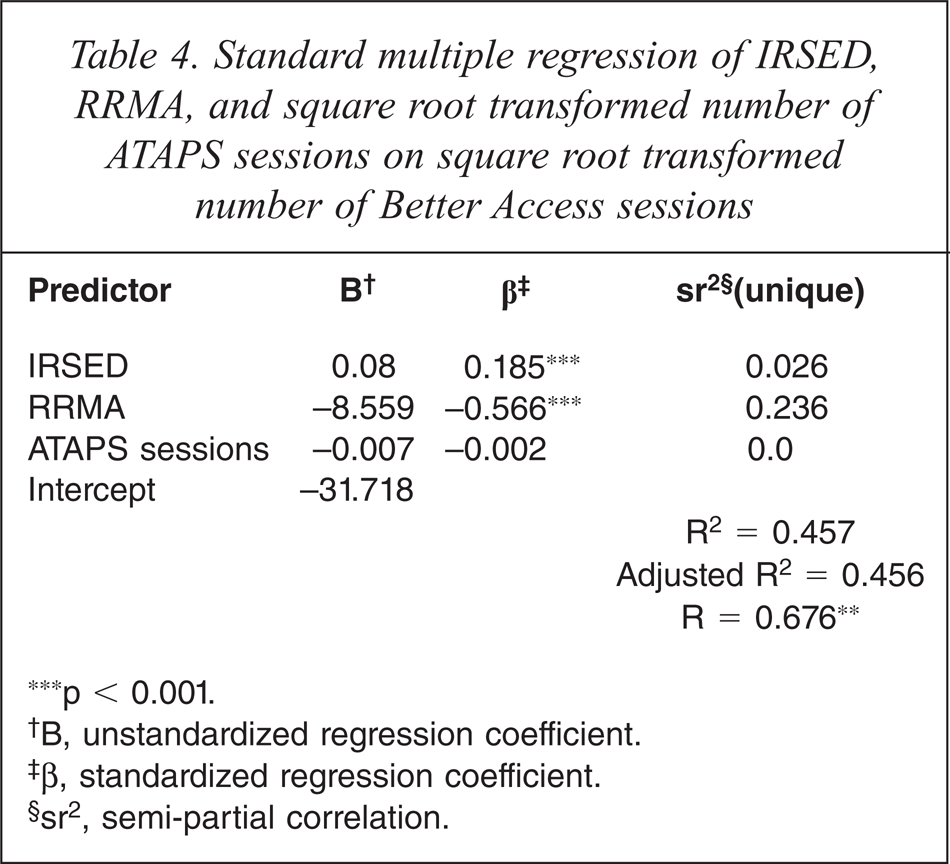
∗∗∗p < 0.001.
†B, unstandardized regression coefficient.
‡β, standardized regression coefficient.
§ sr2, semi-partial correlation.
In summary, although the combined contribution of Better Access sessions, socioeconomic profile and rurality (urbanicity) significantly contributed to the prediction of ATAPS sessions, with higher socioeconomic profile and urbanicity being associated with more service delivery, the magnitude of the contribution was small. The combined contribution of ATAPS sessions, socioeconomic profile and rurality (urbanicity) to the prediction of Better Access sessions was comparatively moderate, with a more pronounced effect of service delivery being associated with higher socioeconomic profile and urbanicity.
The uptake of ATAPS projects before and after the introduction of Better Access
The average number of sessions delivered per month by each Division from 1 January 2002 to 31 October 2006 (pre-Better Access) was 87 (SD = 89), with a range of between 1 and 1,290 sessions. The average number of sessions delivered by each Division per month from 1 November 2006 to 31 December 2008 (post-Better Access) was 98 (SD = 89), with a range of between 1 and 858 sessions. As previously noted, whilst the uptake of Better Access is demand driven, the uptake of ATAPS sessions is limited by capped funding.
To determine whether the introduction of the Better Access programme had an impact on services delivered via the ATAPS projects, the number of sessions delivered by each ATAPS project was regressed on time in months. Two separate analyses were performed, the first using (log transformed) data from January 2002 until October 2006 and the second using (log transformed) data from November 2006 to December 2008, namely before and after the introduction of the Better Access programme.
The trend in the number of ATAPS sessions delivered pre-November 2006 (B = 0.02, SE = 0.001) is steeper than the trend post-November 2006 (B = 0.001, SE = 0.01). There was strong evidence against the null hypothesis of zero trend pre-November 2006 (β = 0.40, p < 0.001) whereas there was no evidence against the null hypothesis of zero trend post-November 2006 (β = 0.02, p = 0.395). The pre-November 2006 trend explains a modest proportion of the variation (16%) in the number of ATAPS sessions delivered, whereas the post-November 2006 trend explains none of the variation (0%) in the number of ATAPS sessions delivered.
These findings suggest that there was a gradual increase in the number of ATAPS sessions delivered per month up to November 2006 but that the number of such sessions delivered per month essentially remained constant thereafter. Despite only a moderate proportion of variation in the number of ATAPS sessions being explained by time pre-November 2006, the effect of the introduction of the Better Access appears to have been to halt the increase in the numbers of ATAPS sessions per month which were subsequently maintained at a steady level until the end of the analysis period. Again it is noteworthy that any increase in the number of sessions delivered under ATAPS is a function of the availability of capped funding.
Discussion
This paper focused on the relationship between the ATAPS projects and the Better Access programme from the time of the introduction of the latter on 1 November 2006 to 31 July 2008, taking into consideration the impacts of rurality and socioeconomic profile of location. It also examined the uptake of ATAPS before and after the introduction of Better Access.
Divisional-level analysis of the number of sessions provided through both programmes in the 21 months since the introduction of the Better Access programme (1 November 2006) demonstrates that the uptake of the Better Access programme has been dramatic, particularly in urban areas. However, there has not been a commensurate decrease in the number of sessions provided through the ATAPS projects, except for an initial drop in the number of sessions, which has since increased to a steady level. Anecdotally, the initial decrease in session numbers may have been attributable to misconception among service providers about the redundancy of the ATAPS projects and their substitution by the Better Access programme. The subsequent steadying of ATAPS session numbers is probably due to the capped nature of funding for the ATAPS projects. A positive correlation, which was small but significant, was found between the numbers of sessions provided by both programmes. However, it is noteworthy that while the majority of sessions delivered through Better Access have been in urban areas, the provision of sessions through the ATAPS projects has been relatively more equally distributed. Notwithstanding the apparent urban bias in Better Access sessions, it has delivered almost a five-fold increase in services delivered in rural areas to that delivered by ATAPS alone.
The two programmes are reasonably independent of one another, as demonstrated by the lack of independent contributions made to the prediction of each other. However, when socio-economic profile and rurality were combined with each programme, a significant proportion of variance in the other programme was explained and this was much higher in the case of the Better Access programme. Socio-economic profile made a relatively small independent contribution to the respective prediction of the number of sessions delivered under the two programmes, which suggests that areas with higher socio-economic profile received more services, and this effect was relatively more pronounced under the Better Access programme. Rurality made a relatively larger independent contribution to the prediction of session delivery under both programmes, and the effect was much more pronounced for the Better Access programme, with fewer sessions delivered with greater rurality. The relatively greater reach of the ATAPS projects across location (by rurality and socio-economic profile) is probably attributable to the flexibility of service delivery models to match the needs of the local context (e.g. the ability of Divisions to use their funding to employ providers in areas in which private providers do not exist).
Examination of the uptake of ATAPS sessions before and after the introduction of the Better Access programme indicate that there was a gradual increase in the number of ATAPS sessions delivered up to November 2006 and that the number of sessions flattened out thereafter. Despite only a small proportion of variation in the number of ATAPS sessions being explained pre-November 2006, there appears to be a ‘real effect’ of the introduction of Better Access, namely to stop the observed increase and maintain the number of ATAPS sessions at a steady level up to the end of the analysis period. Although it should also be noted that the capped nature of ATAPS funding means that session numbers are likely to be maintained at a steady (i.e. capped) level.
Overall, the findings demonstrate that the uptake of the Better Access programme is increasing and that the uptake of ATAPS, which is relatively more responsive to consumers in rural and lower socioeconomic areas, remains steady. The two programmes are operating in a complementary fashion to meet the significant community need for primary mental health care.
Caveats
Caution should be exercised in interpreting the above findings based on a number of caveats. The true magnitude of the relationship between the numbers of sessions provided through both programmes is confounded by the fact that funding for the ATAPS projects is capped while Better Access services are not. Additionally, the large sample size (and session numbers) may produce false positive results. Furthermore, the analysis purely examined overall numbers of sessions delivered; the data available did not distinguish between trends for new and established consumers; and the analysis period ended at 31 December 2008 and so the extent of complementarity between the two programmes may have since changed.
The use of the RRMA classification system is potentially problematic as some Divisions categorized as rural may have large urban populations and this system was under review at the time of the current study [21].
Furthermore, the findings have not been interpreted in the context of population and health provider distributions across locations (by rurality and socioeconomic profile).
Conclusions
The findings indicate that the introduction of the Better Access programme does not seem to have reduced the demand for psychological services provided through the ATAPS projects and that while the demand for the Better Access programme continues to rise, the demand for ATAPS remains steady. There is likely to be a continued increasing need for psychological services given that the prevalence rates of affective disorders have remained consistent and anxiety rates have increased over the past decade [1,2]. In addition, significant proportions of people with these high prevalence mental disorders do not use services, therefore it is important to continue to offer a range of options to improve consumer access.2
The rising and steady uptake of the Better Access programme and the ATAPS projects, respectively, may also be attributable to an excess demand for psychological services that could not be met by the ATAPS projects due to the capped nature of their funding, which is being addressed, at least to some extent, by psychologists and allied health professionals providing care through the Better Access programme. This interpretation is consistent with other findings demonstrating that many Divisions have had to institute strategies to manage excess demand for ATAPS services [25]. Moreover, one of the reasons for the ongoing high demand for services provided through the ATAPS projects may be the evidence that they are achieving positive consumer outcomes [13]; comparable evidence of consumer outcomes achieved by the Better Access programme was not available in the context of this study.
The findings suggest that both programmes are warranted, and that they complement each other. This is supported by both the dramatic uptake of psychological treatment under the Better Access programme and the success of the ATAPS projects in providing equity of geographic and socioeconomic access for consumers most in need of subsidized psychological treatment.
Footnotes
Acknowledgements
The authors would like to express their gratitude to Strategic Data for developing the minimum dataset, and the Divisions of General Practice for managing the projects and providing the data.