
Abstract
Objective:
This study presents estimates of the prevalence, severity and correlates of mental health conditions in Australian emerging adults within geographic regions.
Methods:
We analysed data from 16- to 24-year-olds (N = 1620) of the 2020–2022 Australian National Study of Mental Health and Wellbeing, a national cross-sectional household survey. Estimated prevalence, population counts and unadjusted odds ratios of the 12-month Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) mental and substance use disorders (mental health conditions) are presented for Modified Monash Model categories (geographic region). Multivariable logistic regression models explored correlates of any mental health condition in the full sample, metro subgroup and regional, rural and remote subgroup.
Results:
Over one-third of emerging adults met criteria for a mental health condition. Anxiety disorders were most prevalent (29.2%), then mood disorders (13.7%) and substance use disorders (7.8%). Prevalence was high across metro areas (36.1%); regional centres (35.4%); large rural towns (38.4%) and medium rural towns, small rural towns and remote communities (38.1%). Lifetime exposure to suicide or sexual assault was associated with mental health condition in all regions. In metro but not regional, rural and remote areas, female sex, neighbourhood disadvantage, household financial hardship, no engagement with education/employment, lifetime physical domestic or family violence, less social support and bodily pain were associated with mental health condition.
Conclusion:
Mental health conditions are prevalent among Australian emerging adults in metro, regional, rural and remote regions. Equitable solutions bringing together the full continuum of care in mental health, suicide prevention, sexual violence and bodily pain are needed to reduce their significant impact.
Introduction
The mental health and wellbeing of young people in western, high-income nations is deteriorating (Bor et al., 2014; McGorry et al., 2024). Recent analysis of the 2020–2022 Australian National Study of Mental Health and Wellbeing (NSMHWB) shows a significant increase in the prevalence of anxiety and mood disorders among emerging adults (aged 16–24) between 2007 and 2022, with over one-third of Australian emerging adults now meeting criteria for a 12-month mental or substance use disorder (Slade et al., 2024). Increasingly high rates of psychological distress and hospital presentations for intentional self-harm and suicidal ideation have also been reported among Australian youth (Butterworth et al., 2020; Delaney et al., 2022; Sara et al., 2023). Suicide now represents 39.9% of all deaths among 18- to 24-year-old Australians (Australian Institute of Health and Welfare, 2021c). Characterising mental health conditions in emerging adults, including consideration of geographic region, is vital to inform mental health prevention initiatives, service planning and evidence-based decision-making (Whiteford et al., 2023).
Health disparities have not only been observed across different age groups in Australia but also between geographic regions, with the total age-standardised burden of disease increasing with remoteness (Australian Institute of Health and Welfare, 2021a). A lack of epidemiological research characterising mental health conditions within the geographic contexts in which emerging adults live may create barriers to understanding the experiences of those facing intersecting mental health inequalities. Most mental health research with Australian youth has been conducted in metro areas, despite nearly one-quarter of young people living in regional, rural or remote areas (Australian Institute of Health and Welfare, 2021b; Hielscher et al., 2024; Kasturi et al., 2023). Lack of data availability contributes significantly to the lack of sufficient sample size to detect heterogeneity across regions – a common issue in rural health research (Zahnd et al., 2019). Consequently, population estimates of mental health conditions among emerging adults have rarely been presented within geographic regions of residence in Australia.
Research exploring the intersection between emerging adulthood and geographic region spanning metro, regional and rural areas and using up-to-date national cross-sectional data has the potential to provide insight into the current mental health experiences of Australian emerging adults to guide policy and practice (Golden and Wendel, 2020; Whiteford et al., 2023). Marmot (2015) describes the need to address the causes of social and economic inequalities, or ‘the causes of the causes’, as a means of addressing health inequalities across the lifespan. This framework, known as the social determinants of health, highlights that populations who face health inequity are not inherently less healthy than other populations; rather, it is the intersections of the socio-economic gradient and power relations that can be considered determinants of health (Marmot et al., 2008).
Given the aforementioned gaps in knowledge, this study seeks to analyse available national cross-sectional household survey data to move beyond ‘downstream’ identification of priority populations and instead explore potential ‘upstream’ social determinants of health that may be prevented or interrupted at a population level (Allen et al., 2014). That is, we seek to identify the social and economic conditions that may underlie the mental health experiences of emerging adults within the geographic contexts in which they live. There is a body of evidence, alongside concerns raised by community members (see section ‘Methods’ for more information), supporting a relationship between key social determinants and mental health, including gender and sex recorded at birth (Campbell et al., 2021; Martin and Hadwin, 2022; Newcomb et al., 2020) and socio-economic factors such as neighbourhood disadvantage (Pearce et al., 2018), financial hardship (Butterworth et al., 2012) and engagement with education and employment (Drake and Wallach, 2020; Lawrence et al., 2016). This relationship also holds for psychosocial factors, including exposure to suicide (Andriessen et al., 2017), sexual assault (MacGregor et al., 2015), physical domestic and family violence (Trevillion et al., 2012) and social support (Preston and Rew, 2022). Finally, the relationship between bodily pain and mental health has also been well-documented in youth (Beynon et al., 2020; Corser et al., 2023; Vinall et al., 2016). This paper aims to present contemporary estimates of the prevalence, severity and key correlates of mental health conditions in Australian emerging adults and examine these within geographic regions.
Methods
Sample and survey design
We analysed data from a subset of 1620 respondents aged 16–24 years (born between 1996 and 2006) from the face-to-face Australian NSMHWB, conducted during 2020–2022 (Slade et al., 2024). Representing an estimated total population of 2.7 million emerging adults, the NSMHWB is a cross-sectional national household survey aiming to provide insight into the mental health of Australians. The Australian Bureau of Statistics (ABS) used a stratified, multistage area probability sampling method to randomly select households from private dwellings for participation but excluded households in very remote areas, discrete Aboriginal and Torres Strait Islander communities and non-private dwellings. Emerging adults (aged 16–24) had a higher probability of sampling than other age groups to ensure sufficient sample sizes required for the reliability of estimates.
In total, 52% of the sample responded fully. The age-stratified response rate was not available for reporting. The ABS weighted data and matched it against population benchmarks for sex recorded at birth, 10- to 15-year age groups and geographic region of residence by capital city/rest of state, except for the Northern Territory, which was benchmarked at the territory level. Weights also accounted for the probability of survey completion (Slade et al., 2009, 2024). The ABS approved and provided data access for this study.
Measures
Diagnostic assessment
The ABS used the World Mental Health Survey Initiative version of the Composite International Diagnostic Interview version 3 (WMH-CIDI 3.0) (Kessler and Ustün, 2004) to assess diagnosis of mental and substance use disorders (‘mental health conditions’; Volkow et al., 2021). We report on the 12-month Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) diagnostic information without hierarchy for the purpose of assessing co-occurring mental health condition classes, consistent with prior research (Sunderland et al., 2024). The ABS generated mental health condition classes by categorising each disorder into one of three classes: anxiety disorders (including panic disorder, agoraphobia, social phobia, generalised anxiety disorder, obsessive-compulsive disorder or post-traumatic stress disorder), mood disorders (including depressive episode, dysthymia or bipolar affective disorder) and substance use disorders (including harmful alcohol use/abuse and/or dependence or drug use/abuse and/or dependence). We used the presence of more than one mental health condition class to indicate co-occurring mental health condition classes.
Severity
The ABS classified mental health conditions by symptom severity on a scale of 1 to 10 using DSM-IV criteria and a composite of clinical information collected in the WMH-CIDI 3.0 (described in detail elsewhere; Buist-Bouwman et al., 2008; Slade et al., 2009). Following this prior research, we categorised symptom scores into mild (1–3), moderate (4–6) or severe (7–10) for each respondent who met criteria for a mental health condition.
Sex recorded at birth
Respondents’ sex recorded at birth (male/female) was collected as part of the interview. Sample size was insufficient to report on those who described their sex as another term or to report on respondents’ gender.
Geographic region of residence
We operationalised geographic region of residence by linking household SA1 area codes to Modified Monash Model (MM Model) categories, as stakeholders use this model for regional, rural and remote health resource allocation (Australian Government Department of Health Aged Care, 2023; Versace et al., 2021). We classified geographic regions as: metro areas (MM1: including the Central Coast, Maitland, Wollongong and Geelong); regional centres (MM2; population: > 50,000); large rural towns (MM3; population: 15,000–50,000) or medium rural towns, small rural towns and remote communities (MM4–MM6; population: ⩽ 15,000), collapsed into a single category due to low cell counts. Data were not collected for very remote communities (MM7). Due to additional low cell counts when assessing substance use disorder prevalence and severity, we combined large rural towns with medium rural towns, small rural towns and remote communities (MM3–MM6). Furthermore, we combined all regional, rural and remote (MM2–MM6) categories to create a binary geographic region of residence variable (metro areas; MM1/regional, rural and remote areas; MM2–MM6) for regression models. An overview of geographic remoteness access indexes used in Australia has been reported elsewhere (Versace et al., 2021).
Socio-economic correlates
Neighbourhood disadvantage of household SA1 area of residence was measured using the Socio-Economic Indexes for Areas (SEIFA) Index of relative socio-economic disadvantage (IRSD), operationalised both as quintiles and a continuous measure (Australian Bureau of Statistics, 2023). We presented prevalence estimates as quintiles for ease of interpretation but used the continuous measure in regression analysis to reduce degrees of freedom. The 12-month household financial hardship (yes/no) was constructed based on endorsement of any of the following due to a shortage of money: could not pay bills on time; could not pay the mortgage or rent on time; pawned or sold something; went without meals; was unable to heat home; asked for financial help from friends or family or asked for help from welfare/community organisations (Butterworth and Crosierb, 2005; Butterworth et al., 2012). Current engagement with education or employment was classified by the ABS as: fully engaged (including full-time study and full-time employment; primarily engaged through full-time study; primarily engaged through full-time employment or part-time study and part-time employment), partially engaged (including part-time study only or part-time employment only) or no study or employment.
Psychosocial correlates
Lifetime exposure to suicide (ever close to someone who has taken or attempted to take their own life; yes/no) was included for the first time in the 2020–2022 NSMHWB. Lifetime experience of sexual assault (including rape; yes/no) and lifetime experience of physical domestic or family violence (including ever badly beaten as a child by a parent or guardian; ever badly beaten by a spouse or romantic partner or ever witnessing any serious physical fights at home as a child; yes/no) were constructed from the WMH-CIDI 3.0 PTSD module. Social support (ability to get support from family or friends when needed: excellent; very good; good; fair; poor) was dichotomised into ‘excellent’ or ‘less than excellent’.
Bodily pain
Bodily pain experienced in the past month (none; very mild; mild; moderate; severe; very severe) was dichotomised into ‘moderate or worse’ or ‘mild or less’.
Positionality and informal community engagement
Researchers have called for the acknowledgement of subjectivity and the incorporation of reflexivity into quantitative research practice (Jamieson et al., 2023). Accordingly, we position this study from the context of the lead author, who is a PhD candidate at an Australian university. She is a white cisgender woman from a metro area (Gadigal Country, Sydney), with lived experience of mental health conditions. She belongs to the same birth cohort as study respondents. The lead author visited Dubbo, Wiradjuri Country, an MM Model large rural town, for 2-week-long trips in 2024 to conduct informal community engagement. Her goal was to learn about how youth mental health and wellbeing are conceptualised and practised in Dubbo. She spoke with professional and community networks, including health, school and community workers, Aboriginal community leaders and young people upon invitation. Community members raised concerns they identified as impacting youth mental health and wellbeing. The lead author used social determinants of health framework to identify salient community concerns, including poverty, education, employment, geographic region, suicide, substance use, sexual assault and domestic and family violence. We acknowledge these concerns are not unique to Dubbo. These concerns, together with the availability of data meeting ABS disclosure requirements in the NSMHWB and existing literature, informed the selection of correlates and measures. Community members were also concerned about research positioning regional, rural and remote experiences as noteworthy only in comparison to metro experiences. This informed our decision to conduct multiple subgroup analyses, thereby creating space to report on patterns and correlates within each geographic region, rather than make comparisons between regions.
Data analysis
Data were supplied through the ABS DataLab and analysed using R version 4.2.1 (R Core Team, 2024). Estimated prevalence, population counts (EPCs), univariable and multivariable odds ratios (ORs) are presented by sex at birth, geographic region of residence and correlates. In response to concerns raised of metro-centrality in prior research, and in community engagement, in which regional, rural and remote findings have often been positioned as meaningful only in comparison to metro findings (Judd et al., 2002), we chose to conduct multivariate within-group analyses, rather than directly investigate comparisons across regions. This decision has enabled us to centre the experiences of emerging adults where they live as meaningful in and of themselves, without assuming consistent patterns between variables in each subgroup. Three multivariable logistic regression models explored correlates of any 12-month mental health condition: Model 1: full sample (N = 1620); Model 2: metro subgroup (n = 1316) and Model 3: regional, rural and remote subgroup (n = 304). 95% confidence intervals (CIs) for prevalence estimates and ORs were generated using the jackknife replication method (Rust and Rao, 1996) to account for complex sampling. All correlates were included in all models, excluding geographic region in models 2 and 3. All models were assessed for adequate sample size, separation and multicollinearity (Senaviratna and Cooray, 2019). Less than 0.01% of the data were missing.
Results
Respondent characteristics are described in Tables 1 and 2. Of note, rates of neighbourhood disadvantage, lifetime exposure to suicide and lifetime experience of physical domestic or family violence were significantly higher in regional, rural and remote areas compared to metro areas (Wald chi-square = 6.62–43.72; p < .05).
Characteristics of Australian emerging adults, including socio-economic and psychosocial correlates (N = 1620).
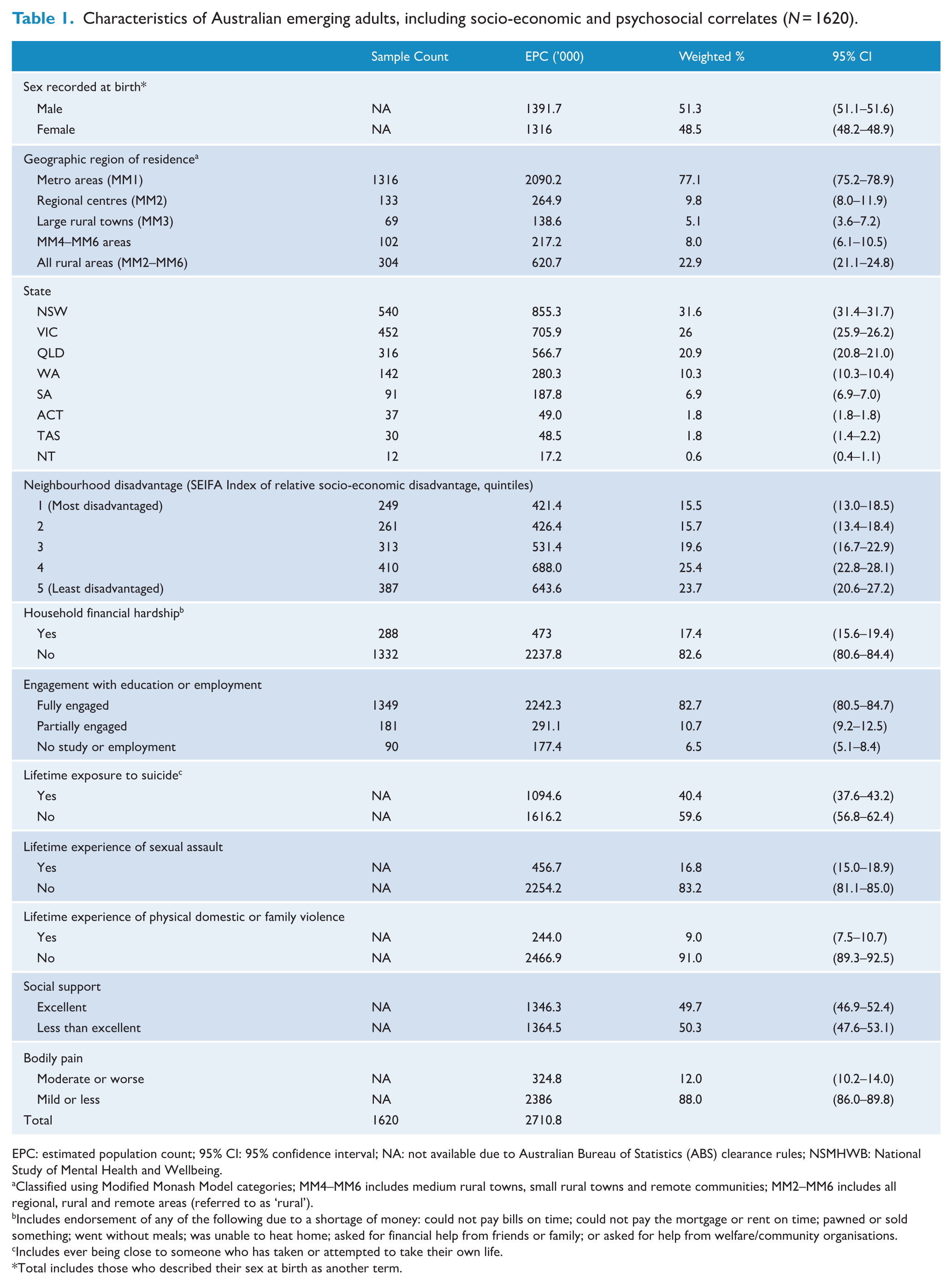
EPC: estimated population count; 95% CI: 95% confidence interval; NA: not available due to Australian Bureau of Statistics (ABS) clearance rules; NSMHWB: National Study of Mental Health and Wellbeing.
Classified using Modified Monash Model categories; MM4–MM6 includes medium rural towns, small rural towns and remote communities; MM2–MM6 includes all regional, rural and remote areas (referred to as ‘rural’).
Includes endorsement of any of the following due to a shortage of money: could not pay bills on time; could not pay the mortgage or rent on time; pawned or sold something; went without meals; was unable to heat home; asked for financial help from friends or family; or asked for help from welfare/community organisations.
Includes ever being close to someone who has taken or attempted to take their own life.
Total includes those who described their sex at birth as another term.
Characteristics of Australian emerging adults, including socio-economic and psychosocial correlates, by geographic region of residence (N = 1620).
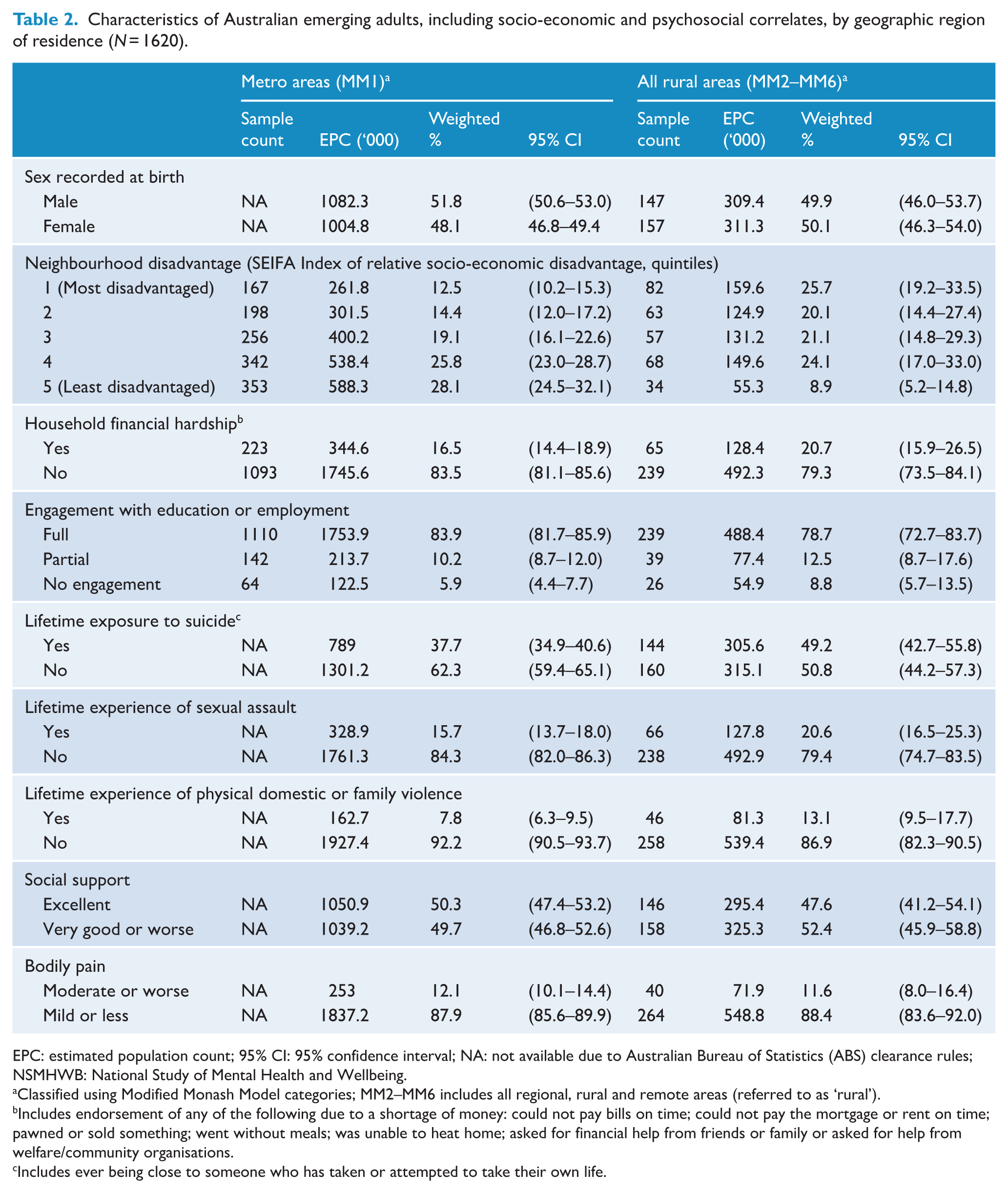
EPC: estimated population count; 95% CI: 95% confidence interval; NA: not available due to Australian Bureau of Statistics (ABS) clearance rules; NSMHWB: National Study of Mental Health and Wellbeing.
Classified using Modified Monash Model categories; MM2–MM6 includes all regional, rural and remote areas (referred to as ‘rural’).
Includes endorsement of any of the following due to a shortage of money: could not pay bills on time; could not pay the mortgage or rent on time; pawned or sold something; went without meals; was unable to heat home; asked for financial help from friends or family or asked for help from welfare/community organisations.
Includes ever being close to someone who has taken or attempted to take their own life.
Prevalence
Prevalence of any 12-month mental health condition by sex recorded at birth and geographic region of residence is presented in Table 3. The prevalence of any 12-month mental health condition among emerging adults was 36.3%. Anxiety disorders, with a prevalence of 29.2%, were the most common disorder class, representing 80.3% of emerging adults who met criteria for a mental health condition. Mood disorders were the next most common (13.7%), followed by substance use disorders (7.8%). The prevalence of two or more mental health condition classes was 12.7%.
The 12-month prevalence of DSM-IV mental health conditions among emerging Australian adults by sex recorded at birth and geographic region of residence (N = 1620).
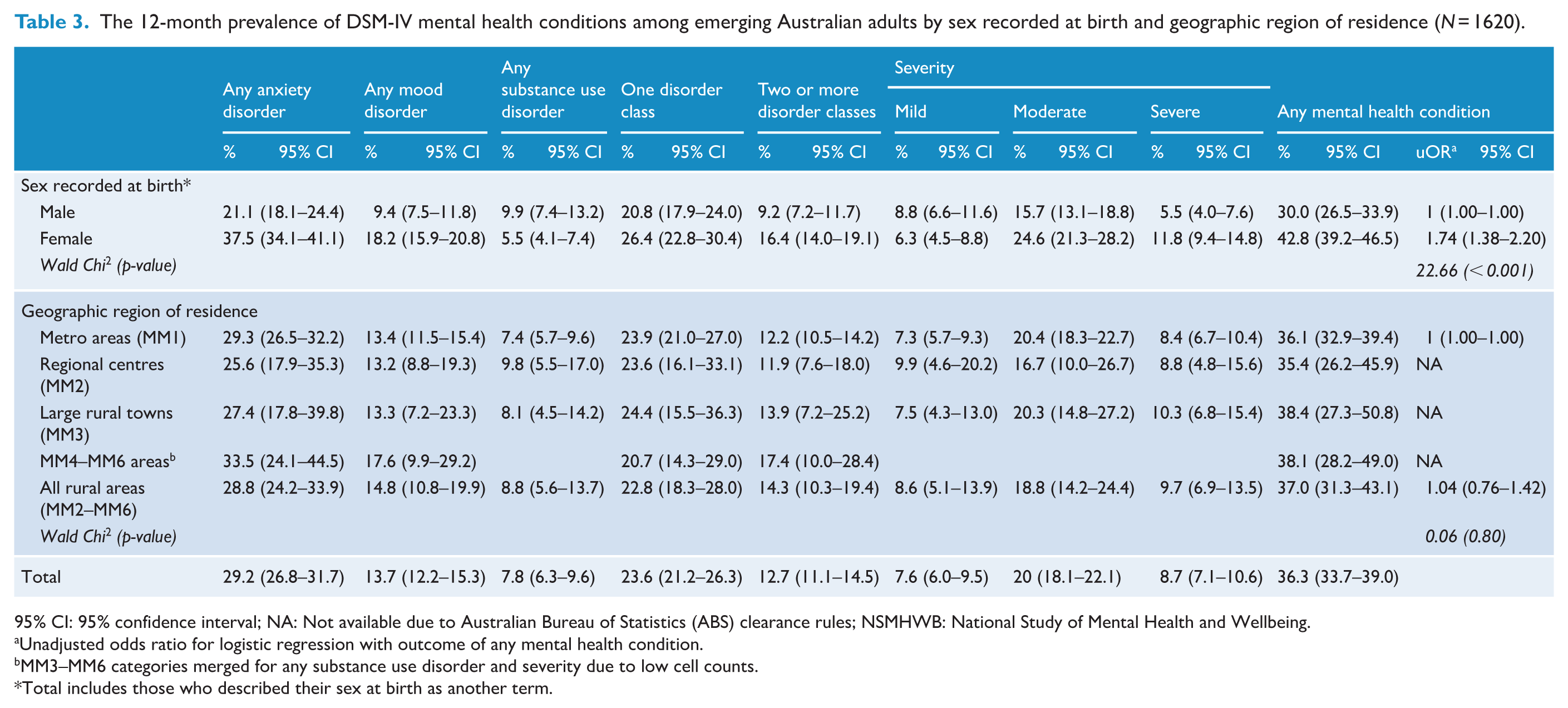
95% CI: 95% confidence interval; NA: Not available due to Australian Bureau of Statistics (ABS) clearance rules; NSMHWB: National Study of Mental Health and Wellbeing.
Unadjusted odds ratio for logistic regression with outcome of any mental health condition.
MM3–MM6 categories merged for any substance use disorder and severity due to low cell counts.
Total includes those who described their sex at birth as another term.
Sex recorded at birth
The 12-month prevalence of any mental health condition was higher among females than males (42.8% in females vs 30.0% in males, Wald chi-square = 22.66, p < 0.001; Table 3). Females had a higher prevalence of any anxiety or mood disorder than males (anxiety disorder: 37.5% in females vs 21.1% in males, Wald chi-square = 42.26, p < 0.001; mood disorder: 18.2% in females vs 9.4% in males, Wald chi-square = 16.24, p < 0.001). Males had a higher prevalence of substance use disorders than females (9.9% in males vs 5.5% in females, Wald chi-square = 8.43, p < 0.01).
Geographic region of residence
The 12-month prevalence of any mental health condition was similar across geographic regions of residence (35.4–38.4%; Wald chi-square = 0.06; p = 0.80; see Table 3). All geographic regions had a similar prevalence of any anxiety disorder (25.6–33.5%; Wald chi-square = 0.02; p = 0.90), mood disorder (13.2–17.6%; Wald chi-square = 0.31; p = 0.58) and substance use disorder (7.4–9.8%; Wald chi-square = 0.37; p = 0.54). Similarly, there were no differences in the prevalence of two or more mental health condition classes across geographic regions (11.9–17.4%; Wald chi-square = 0.64; p = 0.42). Of note, variance appears higher around rural regional, rural and remote estimates than metro estimates (see Table 3).
Severity
Symptom severity by sex recorded at birth and geographic region of residence is presented in Table 3. Symptoms of any 12-month mental health condition were reported as moderate by 20.0% of the sample, representing 55.1% of emerging adults who met criteria for a mental health condition. Similar numbers of emerging adults met criteria for severe (8.7%) and mild symptoms (7.6%).
Sex recorded at birth
Females reported higher rates of moderate and severe symptom severity compared to males (moderate: 24.6% in females vs 15.7% in males; Wald chi-square = 14.91; p < 0.001 and severe: 11.8% in females vs 5.5%; Wald chi-square = 13.20; p < 0.001 in males).
Geographic region of residence
There were no differences in symptom severity across geographic regions of residence (mild: 7.3–9.9%; moderate: 16.7–20.4% and severe: 8.4–10.3%; Wald chi-square = 0.20–0.53; p = 0.47-0.66). Notably, 32.1% of emerging adults with a lifetime experience of physical domestic or family violence had severe symptoms of a mental health condition (95% CI = [22.9–43.0]; Supplementary Table 3b).
Correlates
Prevalence and unadjusted odds of meeting criteria for a mental health condition are presented for each correlate in Supplementary Table 3b. Notably, 73.0% of emerging adults with a lifetime experience of physical domestic or family violence met criteria for a 12-month mental health condition (95% CI = [64.8–79.9]), followed by 67.8% of those with a lifetime experience of sexual assault (95% CI = [59.6–75.0]), 63.0% of those with moderate or worse bodily pain in the past month (95% CI = [54.7–70.6]), 51.2% of those with lifetime exposure to suicide (95% CI = [46.2–56.0]) and 51.1% of those experiencing household financial hardship (95% CI = [42.8–59.4]).
Multivariable models
Results from three multivariable logistic regression models examining the association between any 12-month mental health condition and key correlates are presented in Table 4 (Model 1: full sample; Model 2: metro subgroup; Model 3: regional, rural and remote subgroup).
Multivariate logistic regression models investigating any 12-month DSM-IV mental health condition among Australian emerging adults in the full sample, metro subgroup and rural subgroup.
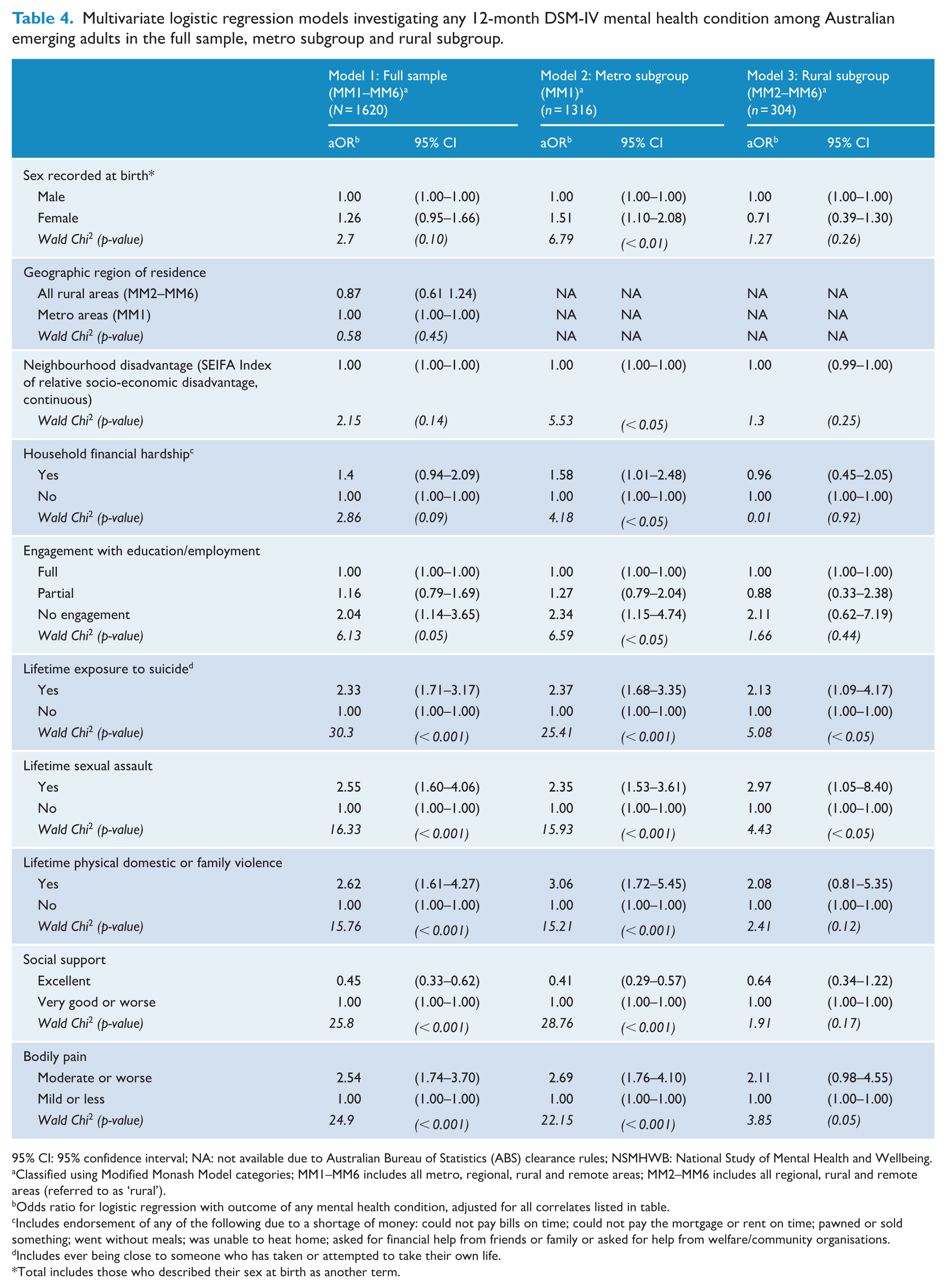
95% CI: 95% confidence interval; NA: not available due to Australian Bureau of Statistics (ABS) clearance rules; NSMHWB: National Study of Mental Health and Wellbeing.
Classified using Modified Monash Model categories; MM1–MM6 includes all metro, regional, rural and remote areas; MM2–MM6 includes all regional, rural and remote areas (referred to as ‘rural’).
Odds ratio for logistic regression with outcome of any mental health condition, adjusted for all correlates listed in table.
Includes endorsement of any of the following due to a shortage of money: could not pay bills on time; could not pay the mortgage or rent on time; pawned or sold something; went without meals; was unable to heat home; asked for financial help from friends or family or asked for help from welfare/community organisations.
Includes ever being close to someone who has taken or attempted to take their own life.
Total includes those who described their sex at birth as another term.
Lifetime exposure to suicide and sexual assault was uniquely associated with a 12-month mental health condition in all three models (ORs = 2.13–2.97). In all models, those who had ever been close to someone who had taken or attempted to take their own life had significantly higher odds of a 12-month mental health condition compared to those who had not (ORs = 2.13–2.37). In all models, those who had ever experienced sexual assault had significantly higher odds of a 12-month mental health condition compared to those who had not (ORs = 2.35–2.97).
Bodily pain was associated with meeting criteria for a 12-month mental health condition in the full sample and the metro subgroup. Those who experienced moderate or worse bodily pain in the past month had significantly higher odds of a 12-month mental health condition compared to those who experienced less bodily pain (ORs = 2.54–2.69). In the regional, rural and remote subgroup, there was little evidence of an association between bodily pain and mental health condition.
Engagement with education or employment, lifetime physical domestic or family violence and social support were associated with meeting criteria for a 12-month mental health condition in the full sample and metro subgroups. Compared to being fully engaged in education or employment, those not in education or employment had higher odds of any 12-month mental health condition (ORs = 2.04–2.34). Those with a lifetime experience of physical domestic or family violence had higher odds of any 12-month mental health condition compared to those without (ORs = 2.62, 3.06). Finally, those with excellent social support had lower odds of any 12-month mental health condition compared to those with less than excellent social support (ORs = 0.45–0.41).
In the metro subgroup only, female sex recorded at birth, higher neighbourhood disadvantage scores and household financial hardship were associated with higher odds of a 12-month mental health condition (see Table 4). We found no evidence of unique associations between any correlates and 12-month mental health condition in the regional, rural and remote subgroup only.
Discussion
Over one-third of Australian emerging adults experienced at least one DSM-IV mental health condition in the past 12 months. Prevalence was consistently high across metro areas, regional centres, large rural towns and medium rural towns, small rural towns and remote communities. Four in five emerging adults experiencing a mental health condition met criteria for an anxiety disorder. The majority (55%) of those with a mental health condition experienced moderate symptoms. While Australia has focussed heavily on barriers and treatment for depression (Teesson et al., 2024), the high prevalence of anxiety disorders in emerging adults across regions suggests increased and equitable efforts should be dedicated to preventing and treating anxiety disorders.
Lifetime exposure to suicide was uniquely associated with meeting criteria for a 12-month mental health condition in all regions. Although directionality cannot be inferred using cross-sectional data, longitudinal evidence demonstrates that suicide bereavement is a risk factor for developing poor mental health (Erlangsen et al., 2017; Kõlves et al., 2020). Lifetime exposure to suicide (ever being close to someone who has taken or attempted to take their own life) is common among Australian emerging adults, experienced by two-fifths (37.7%) of those in metro and half (49.2%) of those in regional, rural and remote areas, suggesting its potential to be an important target for intervention. Past research has shown that young people want to talk about suicide but find adults dismissive, unwilling or hesitant to talk about it (Gibson et al., 2019), despite evidence of the flow-on effects of exposure to suicide (Mitchell et al., 2023). Although there is scarce evidence of effective interventions for those bereaved by suicide to date (Andriessen et al., 2019), these data indicate identifying effective postvention for young people after exposure to suicide is an important avenue for future research.
The 12-month mental health conditions were uniquely associated with lifetime experience of sexual assault in all regions. Although the current study cannot determine the causality of this relationship, Grummitt et al. (2024) have recently demonstrated that a large proportion of mental health conditions in Australia can be attributed to childhood maltreatment, including child sexual abuse (sexual abuse occurring before the age of 18). Australian research has found that one-quarter of Australian emerging adults have experienced childhood sexual abuse, with females experiencing double the rates of males (Mathews et al., 2023). Emerging longitudinal evidence estimates that preventing mid-adolescent sexual violence would reduce the prevalence of psychological distress in 17-year-old girls by 14.0–18.7% and boys by 3.7–10.5% (Bentivegna and Patalay, 2022). Taken together, these data indicate that efforts preventing sexual violence are critical to consider among interventions aimed at improving the mental health of Australian emerging adults.
Moderate or worse bodily pain in the past month was associated with having a 12-month mental health condition in the full and metro population. Bodily pain has often been associated with mental distress in youth (Corser et al., 2023; Vinall et al., 2016) and is a determinant of health within the general population (Schou-Bredal et al., 2014). While it is impossible to ascertain the directionality of bodily pain and mental health from cross-sectional data, somatic symptoms such as bodily pain may indicate the presence of a mental health condition in and of themselves. For example, evidence has been building for the validity, reliability and clinical usefulness of somatic symptom disorder, a diagnosis added to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) in 2013 (Löwe et al., 2022). Furthermore, medical anthropological research suggests somatic symptoms are indicative of distress across cultures and may indicate major depression or an anxiety disorder (Kirmayer, 2001). Notably, Australian Aboriginal and Torres Strait Islander understandings of wellbeing frame pain as a multidimensional concern, in which the physical, emotional and spiritual wellbeing of individuals, communities and environments cannot be separated from each other (O’Brien et al., 2023). Consequently, future research may explore the possible integration of physical and mental health care and service systems within their broader social and environmental contexts in Australia.
There is an indication that socio-economic and psychosocial factors are experienced differently by emerging adults in different geographic regions of residence. In metro but not regional, rural and remote areas, female sex recorded at birth, neighbourhood disadvantage, household financial hardship, lack of engagement with education or employment, lifetime physical domestic or family violence, less than excellent social support and moderate or worse bodily pain were associated with meeting criteria for a mental health condition. This suggests the possibility of low power in this study to detect differences in the regional, rural and remote samples for some factors (e.g. bodily pain); however, it likely indicates real differences in the experiences of emerging adults across regions for other factors. For example, despite significant sex differences in mental health condition prevalence in the full and metro samples, sex was not uniquely associated with mental health condition in the regional, rural and remote sample, suggesting other correlates in the model may have accounted for sex differences. This highlights the importance of considering interventions with a gendered, place-based lens that is sensitive to socio-economic and psychosocial factors, as is often called for by rural researchers (Gullifer et al., 2021).
The high prevalence of mental health conditions among emerging adults in the current study, compared to previous Australian population estimates (Slade et al., 2024), does raise considerations about whether these findings reflect genuine worsening of mental health or measurement artefact. Although this is the subject of current academic debate, a recent Lancet review (McGorry et al., 2024) and a review of longitudinal cohort and population studies (Bor et al., 2014) demonstrating global worsening of youth mental health add veracity to the current findings. The contemporary socio-economic and cultural environment may be creating the unique conditions influencing poor mental health among today’s emerging adult population, which has changed from previous generations. As proposed by Allen et al. (2014), strategies that empower both communities and individuals may be a compelling way forward. The similarly high rates across geographic regions emphasise the importance of strategic and equitable investment across the country to address this significant trend.
Strengths and limitations
This is one of the few studies providing estimates of 12-month mental health conditions in Australian emerging adults by geographic region. The large national cross-sectional sample used in this study is a strength. Importantly, selection of correlates, framing and interpretations of the data have been informed by drawing together research evidence, the social determinants of health framework and a lived experience lens. The authorship team is led by an emerging adult belonging to the same birth cohort as the study sample and includes rural and metro perspectives. By investigating socio-economic and psychosocial factors that are potential upstream determinants of mental health, rather than priority populations, this study has acknowledged the potential universality of such experiences, rather than pathologising specific socio-demographic populations. These factors can also be targeted by policymakers using a multisectoral approach to health and wellbeing. The researchers examined three separate regression models, to enable both similarities and differences in the experiences of emerging adults to emerge across regions. Doing so provided important information about correlates within, and not merely between, regions.
The current study also had limitations. Methodological measures may not have entirely compensated for sampling and response bias, limiting our confidence in the representativeness of the data and the generalisability of our findings. For example, given that age-standardised rates of death by suicide are substantially higher in regional, rural and remote areas compared to metro areas (Australian Institute of Health and Welfare, 2024; Cheung et al., 2012), one might expect the prevalence of mental health conditions to follow this pattern, in contrast to the findings we have reported. Notwithstanding the complexity of identifying risk factors for suicide (Franklin et al., 2017), this could suggest that emerging adults meeting criteria for mental health conditions in regional, rural and remote areas may have been less likely to be sampled or to respond to the survey request than those living in metro areas. Furthermore, the study appears to have oversampled those living in the least disadvantaged communities relative to the most disadvantaged communities. In addition, we report lower prevalence of sexual assault and physical domestic or family violence than prior research (Haslam et al., 2023). This is perhaps due to differences in study design, measurement and sampling methods, including our repurposing of the CIDI 3.0 PTSD module, which was designed to diagnose PTSD, not as a comprehensive measure of maltreatment. Although they are 25% of the Australian population, regional, rural and remote respondents made up less than one-fifth of the survey sample. Acknowledging that insufficient sample size is a common concern in regional, rural and remote health disparities research, relatively low cell counts in some analyses may have limited our ability to detect regional differences in bodily pain and experience of physical domestic or family violence. Additional limitations including the possibility of bias introduced by the response rate have already been reported in the 2020–2022 NSMHWB main outcomes paper (Slade et al., 2024).
Conclusions
Mental health conditions are common among emerging adults in all regions of Australia, with differing patterns of correlates within metro and regional, rural and remote areas. The findings highlight the importance of bringing together geographic context-specific conversations about mental health, suicide prevention, sexual violence and bodily pain to deepen our understanding of the poor mental health and wellbeing of emerging adults. We anticipate that a deeper understanding of these interrelated issues and the mechanisms underlying them will pave the way for innovative and equitable multidisciplinary and multisectoral solutions.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251385365 – Supplemental material for Mental health and substance use conditions among emerging adults in Australia 2020–2022: Prevalence, severity and psychosocial correlates within geographic regions
Supplemental material, sj-docx-1-anp-10.1177_00048674251385365 for Mental health and substance use conditions among emerging adults in Australia 2020–2022: Prevalence, severity and psychosocial correlates within geographic regions by Julia Macauley, Marlee Bower, Maree Teesson, Emma Webster and Cath Chapman in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
I am grateful to Uncle ‘Riverbank’ Frank Doolan, respected Wiradjuri Elder, for his guidance and support in the early framing of this paper. I would also like to acknowledge those whose lived experience informed the framing of this paper. I would like to thank those who took part in the survey and to extend this thanks to the Dubbo community for sharing their stories with me.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval and informed consent statements
Human ethical approval was not required, as this study is an analysis of secondary data and did not involve additional data collection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research is supported by an Australian Government Research Training Program (RTP) Scholarship. This work was supported by a headspace National Youth Mental Health Foundation evidence-building PhD scholarship. M.T. and C.C. receive NHMRC Fellowship funding.
Data accessibility statement
The detailed microdata used in this study can be obtained by seeking approval from the Australian Bureau of Statistics.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.