
Abstract
Objective:
The prevalence of common mental disorders (CMDs, depression/anxiety) among Australian adolescents is increasing. Evidence is needed to inform how prevention efforts can be focused for greatest impact. This study used a compartmental model to estimate how investments could be optimally allocated across interventions to prevent CMDs in adolescents, and the corresponding health and economic benefits.
Methods:
The Australian 0- to 19-year-old population was disaggregated by age (0–9, 10–14, 15–19), sex (male, female) and CMD experience (never, currently, previously). Twelve prevention interventions were included following targeted reviews. The model was calibrated to Australian population survey data and included sociodemographic risk factors from the literature that were relevant for included interventions (bullying, financial stress, poor school connectedness, racial discrimination, child maltreatment). An optimisation estimated how an additional AUD$50 million–AUD$1 billion per annum over 2024–2050 could be allocated across interventions to maximise the number of adolescents turning 20 without a lifetime experience of CMD.
Results:
The benefit–cost ratios of interventions varied widely depending on whether they impacted CMDs directly or indirectly by reducing a risk factor, and also whether CMD was their primary purpose or not (e.g. poverty interventions). Optimally investing AUD$50 million–AUD$1 billion p.a. over 2024–2050 could lead to 144,577–791,277 fewer adolescents experiencing a CMD by age 20 (AUD$5064–AUD$18,507/lifetime CMD experience averted), with lower bound benefit–cost ratios ranging from 5.0 to 19.2. Optimally, budget allocations should include combinations of interventions targeting different age groups, sub-populations and risk factors.
Conclusions:
Investing in evidence-based prevention interventions for adolescent mental health is likely to have a favourable return-on-investment.
Keywords
Introduction
Over the last decade the prevalence of mental disorders among Australian adolescents has been increasing. Data from the Mission Australia Youth Survey (Black Dog Institute, 2017; Mission Australia, 2024), a large national school-based survey showed that the proportion of 15–19 year olds meeting the criteria for having a probable serious mental disorder, as measured by the Kessler 6 [K6] measure of psychological distress, increased from 18.7% in 2012 [n = 14,635] to 21.6% in 2024 [n = 16,628]. Using the more stringent criteria of a diagnostic interview the 2020–2022 National Study of Mental Health and Wellbeing showed that among 16- to 24-year-old Australians [n = 2712], 38.8% met criteria for a mental disorder, up from 26.4% in 2007 (Australian Bureau of Statistics (ABS), 2007, 2020–2022). While different sample characteristics (e.g. age), definitions and measurement instruments make direct comparisons of prevalence across studies difficult they consistently point to rising trends in the prevalence of mental illness among adolescents (Australian Institute of Health and Welfare (AIHW), 2021a; Black Dog Institute, 2017; Jorm et al., 2017; Lawrence et al., 2015).
Demand for services and resource allocation towards mental health care in Australia has also increased. In the 2020/2021 Australian federal budget, AUD$2.3 billion was made available as part of the National Mental Health and Suicide prevention plan. Substantial allocations were made over 4 years (2020/2021–2024/2025) to adolescent mental health services, including AUD$13 million to ReachOut, an online platform for mental health support (ReachOut Australia, 2022), and AUD$279 million to increase headspace (2023) treatment capacity for adolescents aged 12–25 years. This is in addition to state funding of existing clinical services, including child and adolescent mental health services and various initiatives around school health services (AIHW, 2024a; Clare and McBride, 2023).
In Australia, the federal budget allocations primarily represent the cost of managing the increasing burden of poor mental health through funding a multitude of different treatment types, support services and delivery modalities for adolescents already experiencing some form of mental disorder. Notwithstanding the importance of these investments, the increasing health and economic burden of mental disorders highlights that new approaches are needed. The Productivity Commission’s Report into Mental Health (Productivity Commission, 2020) identified prevention and early intervention as a significant area for reform. If implemented effectively, prevention interventions could play an important role in combatting the increasing prevalence of mental illness in young people, minimising the impact of this on the lives of young people and reducing the costs of managing this health burden (Birrell et al., 2025; Productivity Commission, 2020). The need for prevention is clearly articulated in government reports (National Mental Health Commission, 2020) and the overall National Mental Health and Suicide Prevention Plan (Commonwealth of Australia, 2021), however, it is unclear how funding will be allocated to prevention efforts, whether it will be targeted to the most cost-effective evidence-based interventions, and the extent to which prevention, as opposed to early intervention, will be prioritised (Birrell et al., 2024, 2025).
Economic evaluations exist for some specific prevention interventions for common mental disorders (CMDs, depression and anxiety) in children and adolescents (Abou Jaoude et al., 2024; Chisholm et al., 2016; Le et al., 2021a; National Mental Health Commission, 2020), with estimated benefit–cost ratios ranging from 1.19 to 3.06 for Universal Guided Digital Cognitive behaviour Therapy (CBT), Universal School-based In-person CBT, a Selective Parenting Programme, and a School Bullying Programme (Comben et al., 2022; Skinner et al., 2023). More broadly, universal primary school mental health interventions have been estimated internationally to have benefit–cost ratios ranging from 1.3 to 11.6 (Abou Jaoude et al., 2024). However, the set of prevention interventions that has been evaluated is limited, and because interventions may target different age groups or risk factors for CMDs it is not clear whether there are synergies between them. This results in an evidence gap for understanding how investments can be optimally allocated across interventions to prevent CMDs in Australian adolescents.
The objective of this modelling study was to identify investment priorities for preventing CMDs in 10–19 year olds in Australia and the potential return-on-investment that could be achieved, to inform resource allocation decisions and national planning. Specifically, we aimed to estimate (a) the impact that scaling up a selection of evidence-based prevention interventions could have on the number of adolescents turning 20 without a lifetime experience of any CMD; and (b) how different investment envelopes could be optimally allocated across interventions to maximise the number of adolescents turning 20 without a lifetime experience of CMD, and the corresponding health and economic benefits.
Methods
The model considers the Australian population aged 0–19 years, disaggregated by sex (male or female) and age category (0–9, 10–14, 15–19 years), with historic and projected population sizes taken from the Australian Institute of Health and Welfare (AIHW) (2021a), and the 2021 Australian Census (ABS, 2011, 2016, 2021). The model does not disaggregate by gender identity or sexuality as these variables were not consistently collected in population level mental health surveys (Lawrence et al., 2015). In this study, the term CMDs is used to refer to the outcomes of any anxiety disorder and/or major depressive disorder (Goldberg, 1994), which are the most prevalent mental disorders in adolescents aged 10–19 years. We define a person experiencing a CMD as one meeting the diagnostic criteria of an anxiety disorder or major depressive disorder as measured by a diagnostic interview (Shaffer et al., 2000). The same definition of CMD has been applied across the age range 0–19. Data for these measures and their prevalence among adolescents are summarised by the AIHW (AIHW, 2021b) with estimates from the National Study of Mental Health and Wellbeing (ABS, 2007, 2020–2022) and the Young Minds Matter Survey (Lawrence et al., 2015).
Model overview
Each age group (0–9, 10–14 and 15–19 years) was categorised as never, currently or previously experiencing a CMD (Figure 1). Each year, people could enter the model through birth and exit due to ageing or death (suicide/accident/other) and could move between CMD categories based on estimated incidence rates (Robson et al., 2024), an annual recovery rate (Robson et al., 2024), and estimated recurrence rates. Once a person has experienced a CMD in the model it is not possible to return to the ‘never experienced CMD’ category which enables an estimate of lifetime experience of clinically significant CMDs by age 20. A deterministic compartmental model was used, following common approaches in epidemiological modelling (Vynnycky and White, 2010). The model was implemented in Python using the Atomica package (Atomica Team, 2025).
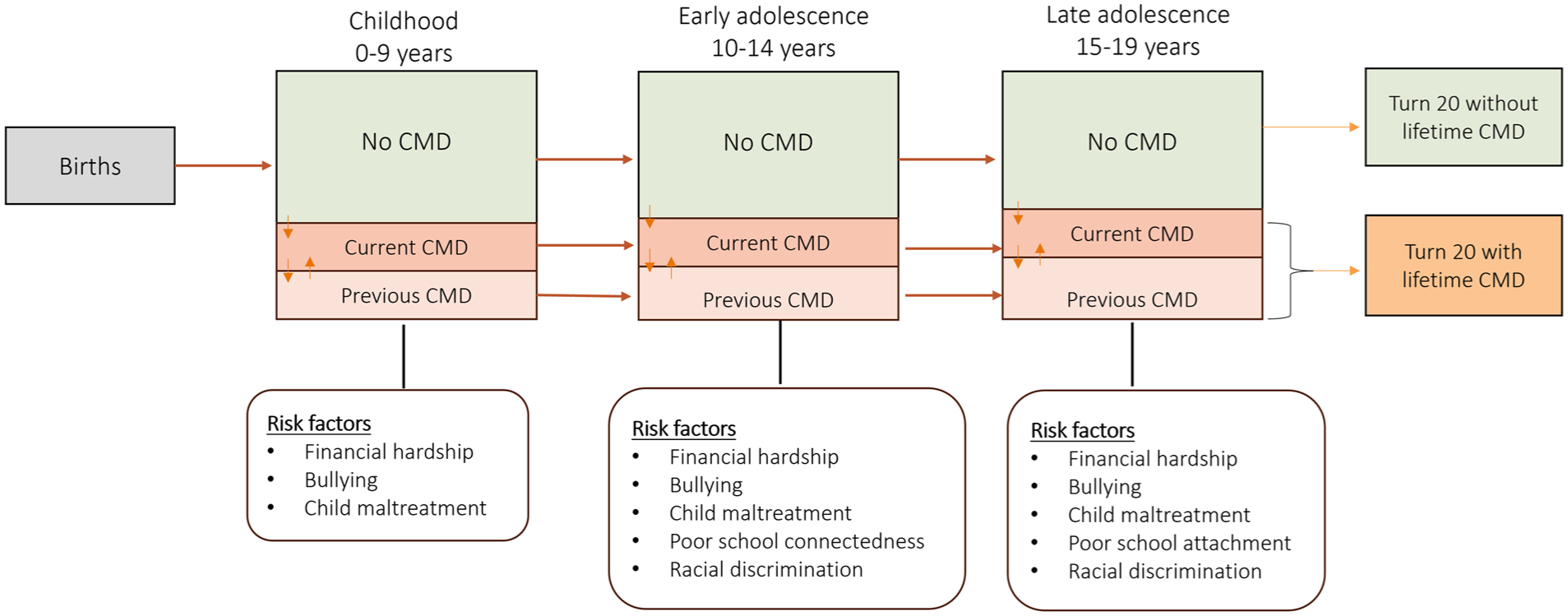
Model age groups and common mental disorder (CMD) states.
Risk factors for CMDs
There are many well documented associations between adolescent CMDs and socio-economic, health, demographic and other factors (Azzopardi et al., 2023; Moore et al., 2015; Priest et al., 2019; Reiss et al., 2019; The Lancet, 2017; Viner et al., 2012; World Health Organization and Calouste Gulbenkian Foundation, 2014). In the model, risk factors are parametrised with a prevalence and an effect on CMDs (e.g. an odds ratio or relative risk). The effects of risk factors on CMDs were not identified in causal modelling studies and are therefore considered associations. If there is evidence that an intervention reduces the prevalence of a risk factor, then this can lead to a reduction in CMDs by having a greater proportion of the population at a lower risk. For example, as bullying is a risk factor for CMDs (Bond et al., 2001), interventions that reduce bullying will have an indirect impact on CMDs in the model by increasing the proportion of people in the model who are not exposed to bullying, and are therefore at a lower risk of experiencing a CMD.
Rather than an exhaustive list, risk factors are only included if the set of modelled interventions influences them. Those included (Table 1) are therefore a subset of risk factors identified in the World Health Organisation’s Social Determinants of Mental Health (World Health Organization and Calouste Gulbenkian Foundation, 2014). Data were sourced from published studies and were reviewed by a panel of experts to ensure they were appropriate for inclusion. Further details on modelled risk factors are in Supplemental Appendix A.
Model risk factor prevalence and odds ratio estimates.
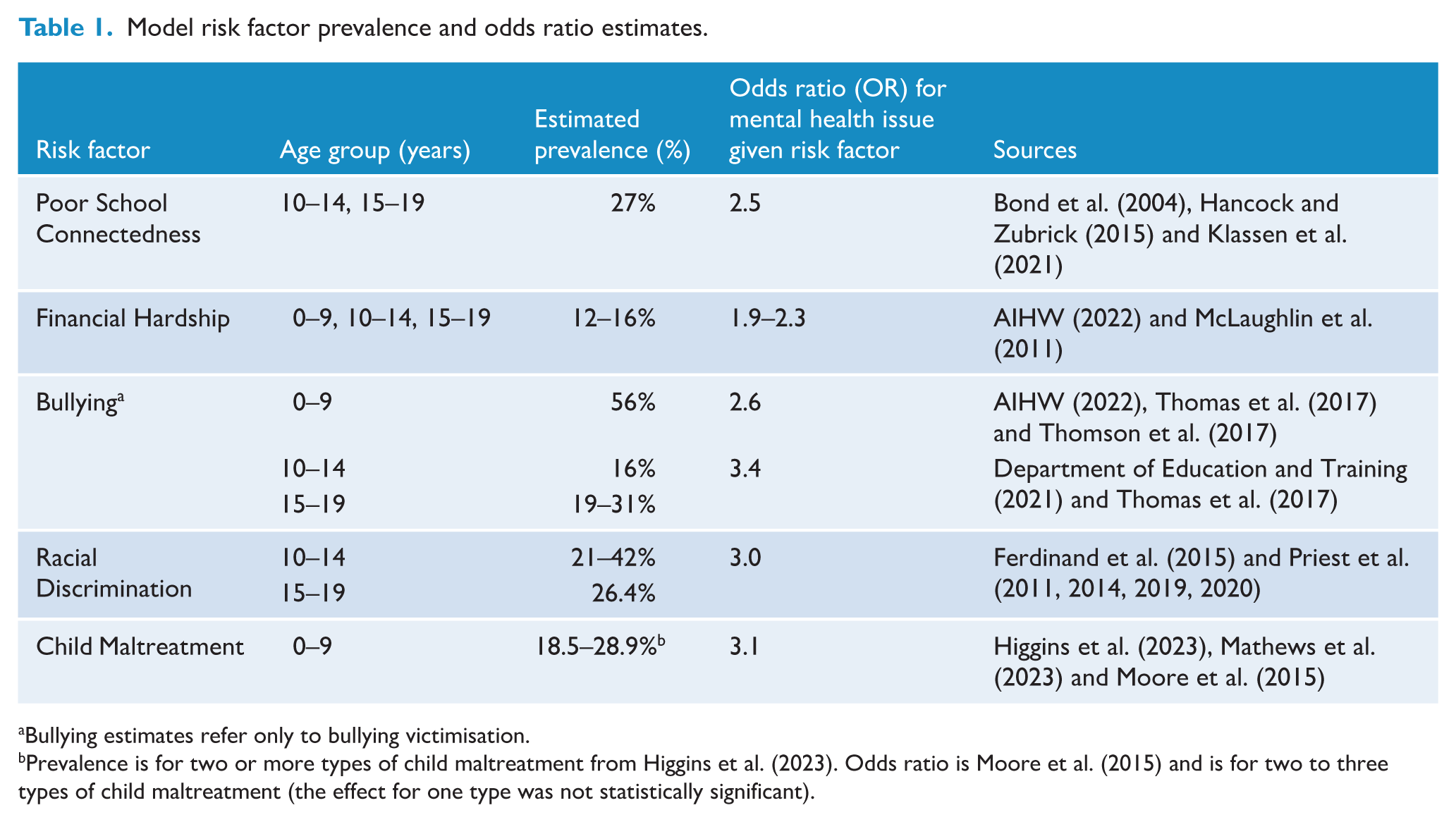
Bullying estimates refer only to bullying victimisation.
Prevalence is for two or more types of child maltreatment from Higgins et al. (2023). Odds ratio is Moore et al. (2015) and is for two to three types of child maltreatment (the effect for one type was not statistically significant).
Model calibration
The age- and sex-specific incidence of first CMD was calibrated to match incidence data of clinically significant symptoms of CMD from the Child to Adult Transition Study (CATS), a Victorian cohort study that has annually followed-up children from the age of 8 when recruited in 2012 (Mundy et al., 2013). Incident cases per 1000 person years (PY) were 82–170 among 10–14 year olds and 143–480 cases among 15–19 year olds. Cumulative incidences for males and females at age 15 and 18 years were 19.5–35.1% and 44.8–73.7%, respectively (Robson et al., 2024).
For each age and sex category, parameters for the rate of recovery and recurrence were then calibrated such that: (a) the prevalence of CMDs among the 0- to 9-year and 10- to 14-year age groups in the model aligned with the Young Minds Matter survey (anxiety or depression diagnosis identified by Diagnostic Interview Schedule for Children, Version-IV [DISC-IV] modules) for the; (b) the prevalence of CMDs among the 15- to 19-year age group in the model aligned with the National Survey of Mental Health and Wellbeing (proportion of 15–19 year olds experiencing any mental disorder in the last 12 months, as measured by the World Mental Health-Composite International Diagnostic Interview 3.0 [WMH-CIDI]); (c) the rate of recovery in the model aligned with estimates of adolescents reporting a CMD in one survey wave, but not in the next in the CATS study (Robson et al., 2024) (See Supplemental Appendix D for details); and (d) sex-specific incidence rates of CMDs among 10–14 year olds and 15–19 year olds in the model aligned with incidence rates from CATS (Robson et al., 2024). In the data, CMD prevalence was 16.5% and 10.6% among the 0- to 9-year male and female age groups, respectively, 15.9% and 12.8% among the 10–14 male and female age groups, respectively (Lawrence et al., 2015), 22.3–45.5% among 15- to 19-year-old females, and 22.8–32.4% among 15- to 19-year-old males (ABS, 2020–2022). The prevalence of adolescents reporting a CMD in one wave but not the next was 26.2% and 46.6% for 10–14 and 15–19 year olds, respectively (Robson et al., 2024).
Lifetime experience of CMD by age 20 was a model output based on the age- and sex-specific calibrated prevalence, recovery and estimated rate of recurrence. These model outputs were validated against other estimates from the literature (Supplemental Appendix F).
Interventions
Interventions were sourced from literature reviews and reviewed in consultation with a panel of experts. An initial list was developed that included interventions identified in the 2020 Australian Government Productivity Commission’s inquiry into Mental Health (Productivity Commission, 2020), the National Mental Health Commission (2020), and published systematic reviews on all mental health interventions such as Das et al. (2016) and Zhang et al. (2023), school-based interventions such as Christensen et al. (2011), Cuijpers et al. (2008), Durlak et al. (2011), Fazel et al. (2014), Raniti et al. (2022), Stockings et al. (2016), Taylor et al. (2017), Vreeman and Carroll (2007) and more specific reviews of interventions targeting risk factors such as child maltreatment (Van der Put et al., 2018). A panel of Australian mental health researchers and clinicians who were knowledgeable about prevention interventions reviewed the study scope, the set of included interventions, and the quality of evidence to inform their parametrisation. This resulted in 12 interventions to be considered (Table 2), each defined by a target population, effect size on either CMDs (direct effect) or a risk factor (indirect effect), a unit cost, and a maximum achievable coverage. Full details and derivations of intervention parameters are in Supplemental Appendix B.
Interventions included in analysis and their parametrisations.
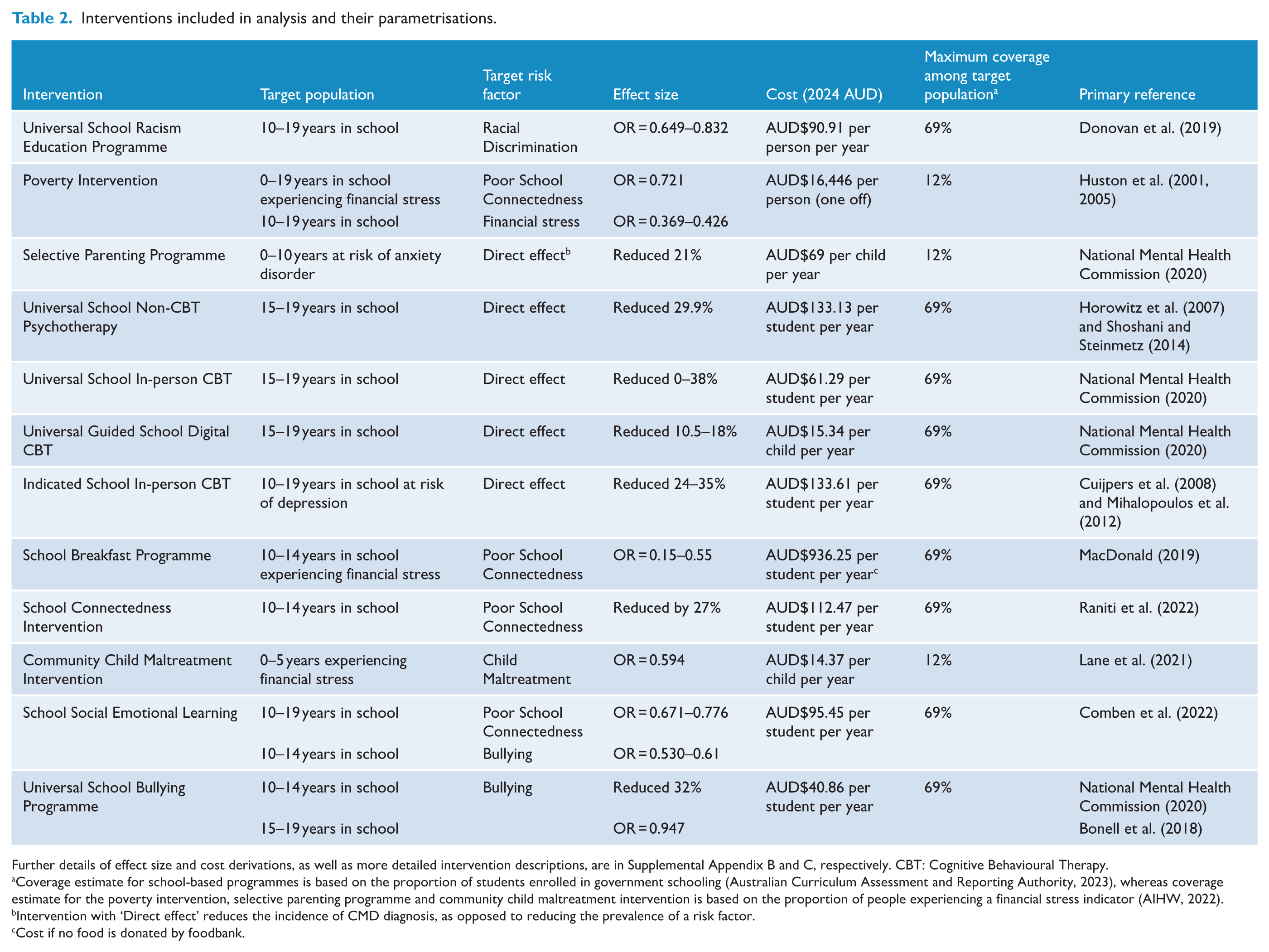
Further details of effect size and cost derivations, as well as more detailed intervention descriptions, are in Supplemental Appendix B and C, respectively. CBT: Cognitive Behavioural Therapy.
Coverage estimate for school-based programmes is based on the proportion of students enrolled in government schooling (Australian Curriculum Assessment and Reporting Authority, 2023), whereas coverage estimate for the poverty intervention, selective parenting programme and community child maltreatment intervention is based on the proportion of people experiencing a financial stress indicator (AIHW, 2022).
Intervention with ‘Direct effect’ reduces the incidence of CMD diagnosis, as opposed to reducing the prevalence of a risk factor.
Cost if no food is donated by foodbank.
Interventions with direct impacts are assumed to modify the incidence of CMDs, whereas interventions with indirect effects reduce the prevalence of a risk factor which contributes to a reduced incidence of CMDs (Figure 2).
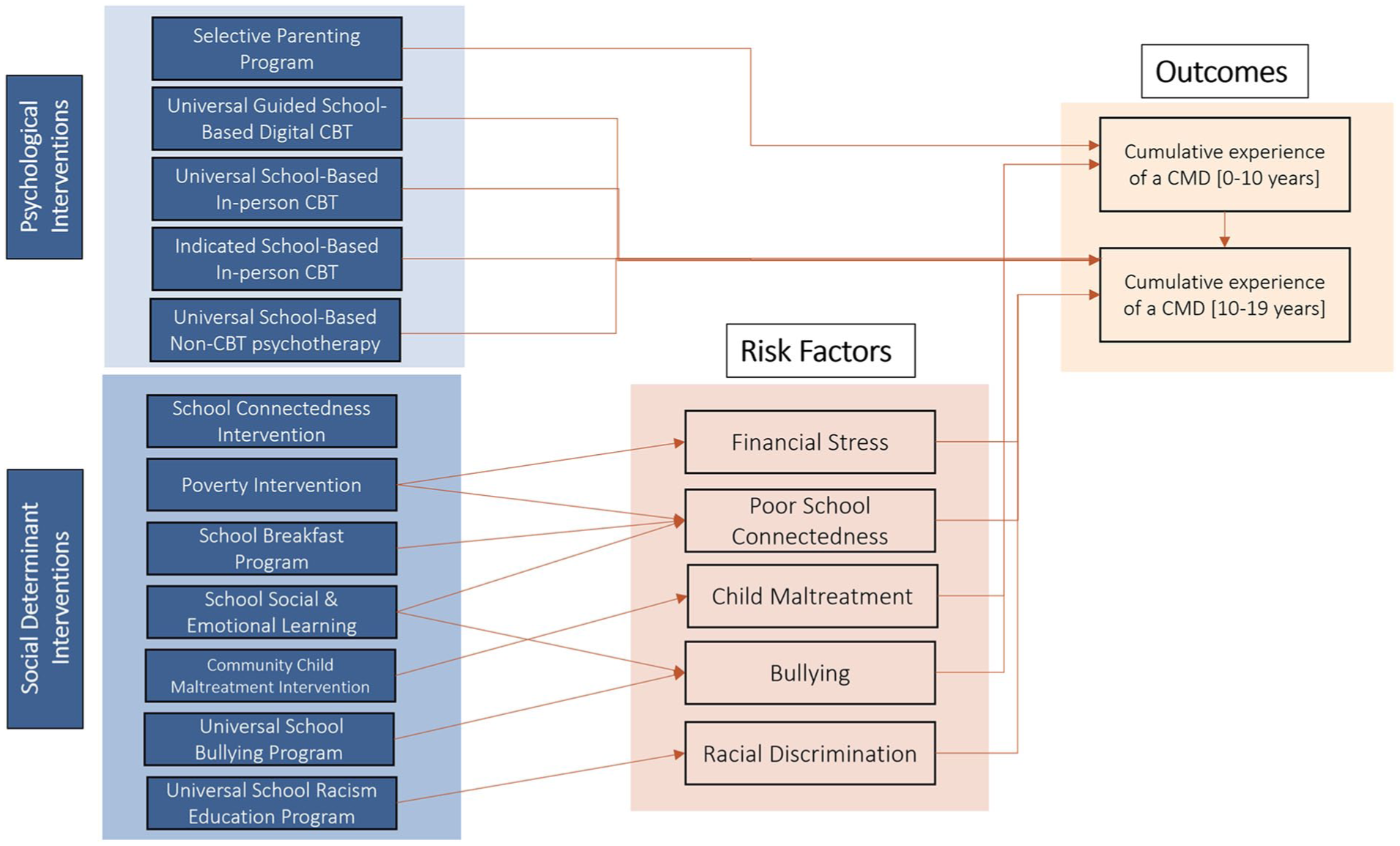
Interventions included in analysis and their corresponding (direct and indirect) effects.
Intervention effect sizes were commonly reported in the literature as measures of standardised mean differences for continuous data (Cohens d, Hedges G) or odds ratios/risk ratios/relative risks where the measured outcomes were dichotomised. Effect sizes were converted to a relative risk (Supplemental Appendix D).
Intervention costs were estimated in 2023 Australian Dollars (AUD) from a government or service provider perspective. A limitation of existing economic evidence for interventions is that the costing methodologies vary widely and are not comparable. To overcome this, an ingredients-based approach was used to estimate unit costs for each intervention by taking the resources described in each study and applying consistent ingredient costs (e.g. teacher or trainer salaries) (Supplemental Appendix C). Costs in future years were discounted at 5% per annum (Department of Health, 2016).
Modelling scenarios
Scenario type 1: individual intervention scale-up to maximum coverage
Each intervention was scaled up in isolation to maximum coverage (Table 2) among the intervention’s target population, and maintained for the period 2024–2050, to estimate the impact on the number of people turning age 20 with a lifetime experience of CMDs. The longer timeframe up to 2050 was used to capture the delayed benefits that some interventions targeting very young children (i.e. parenting programme) can have across their adolescence.
Scenario type 2: individual intervention scale-up by fixed investment
Each intervention was scaled up in isolation by a fixed incremental investment of AUD$2 million per annum for the period 2024–2050 (inclusive), to estimate the impact on the number of people turning 20 with a lifetime experience of CMDs. For this analysis it was necessary that the chosen incremental investment amount was small enough for the total amount not to have enabled more than the entire target population to be reached, since once this occurs additional investment cannot expand the intervention further.
Unlike scenario type 1 which ranks interventions based on total possible impact, scenario type 2 ranks interventions based on cost-effectiveness.
Scenario type 3: optimal allocation of funding across interventions
An optimisation algorithm, adaptive stochastic descent, was used to estimate how total budgets between AUD$50 million and AUD$1 billion per annum could be optimally allocated across the 12 interventions to maximise the number of people turning 20 over 2024–2050 without a lifetime experience of CMDs. Budget envelopes were arbitrary but selected to be comparable to the 2020/2021 national budget announcements of AUD$2.3 billion over 4 years. For each budget envelope, additional investment was introduced in 2024 and allocations remained fixed across the projection period.
Return-on-investment for intervention scale-up and optimal investment scenarios
For each scenario, cumulative intervention costs and quality-adjusted life years (QALYs) among people aged 10–19 years were estimated for 2024–2050 inclusive. Costs were from the perspective of the investor and only considered the interventions. Costs are presented in 2023 AUD, and both costs and QALYs were discounted at 5% per annum (Department of Health, 2016). Average health utilities were taken as 0.70 for adolescents currently experiencing CMDs and 0.8 for other adolescents (Le et al., 2021b) (Supplemental Appendix E).
Discounted QALYs gained from increased intervention coverage were converted to economic benefits based on the Australian Government value of a statistical life year (AUD$227,000) (Australian Government, 2022). A proportion of CMDs averted (55.9%; Islam et al. (2022)) were assumed to result in an additional benefit of prevented mental health related treatment costs (AUD$8162 per person per annum; AIHW (2023, 2024a)). The benefit–cost ratio (BCR) of each scenario relative to the baseline was calculated by dividing the total discounted economic benefits by the total discounted investment.
Critically, these BCRs are likely to significantly underestimate the true BCRs as while they consider full intervention costs, they only consider benefits relating to mental health (e.g. school breakfast programme, poverty reduction, parenting programme have substantive benefits in other domains). We therefore consider the BCRs to be a lower bound, and use a sensitivity analysis to estimate BCRs if mental health benefits represented 50% of the total benefits. Further sensitivity analyses exploring different rates of mental health recovery and benefit calculations were conducted in Supplemental Appendix F.
Results
Between 2024 and 2050 we expect ~8.2 million people to turn 20 in Australia. Based on the model calibration to recent survey estimates, approximately 4.1-million 20 year olds will have experienced a CMD.
Scenario 1: individual intervention scale-up to maximum coverage
If cost was not considered, the programme for reducing poverty had the greatest scope for impact; it is applicable to all people (0–19 years old) in the model, and, when scaled up to maximum coverage, led to a reduction of 384,293 (9.4%) people turning 20 with a lifetime CMD experience over 2024–2050 (Figure 3). The next most impactful intervention was the universal school non-CBT psychotherapy (211,762 reduction), followed by indicated school in-person CBT (208,775) and school breakfast programme (155,745 reduction). All other interventions resulted in approximately 5000–145,000 fewer people turning 20 with a lifetime experience of a CMD when compared with the status-quo (Table 3). For some interventions, total impact appears smaller because the interventions only target a small sub-set of the population and so have limited scope (e.g. the child maltreatment intervention).
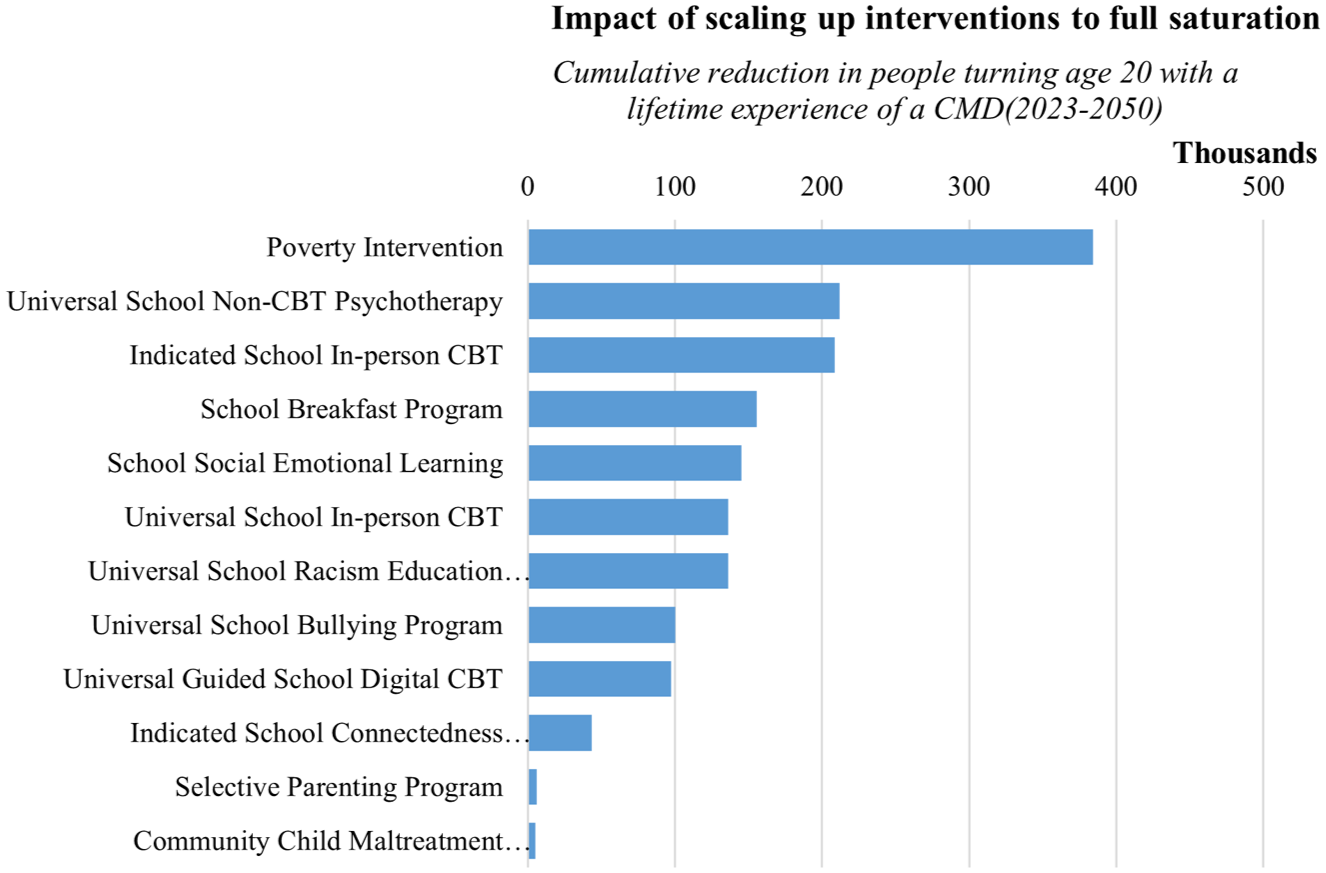
Impact of individual interventions when scaled up to maximum coverage, maintained 2024–2050.
Costs, health impact and economic benefits of individual interventions when scaled up to maximum coverage.
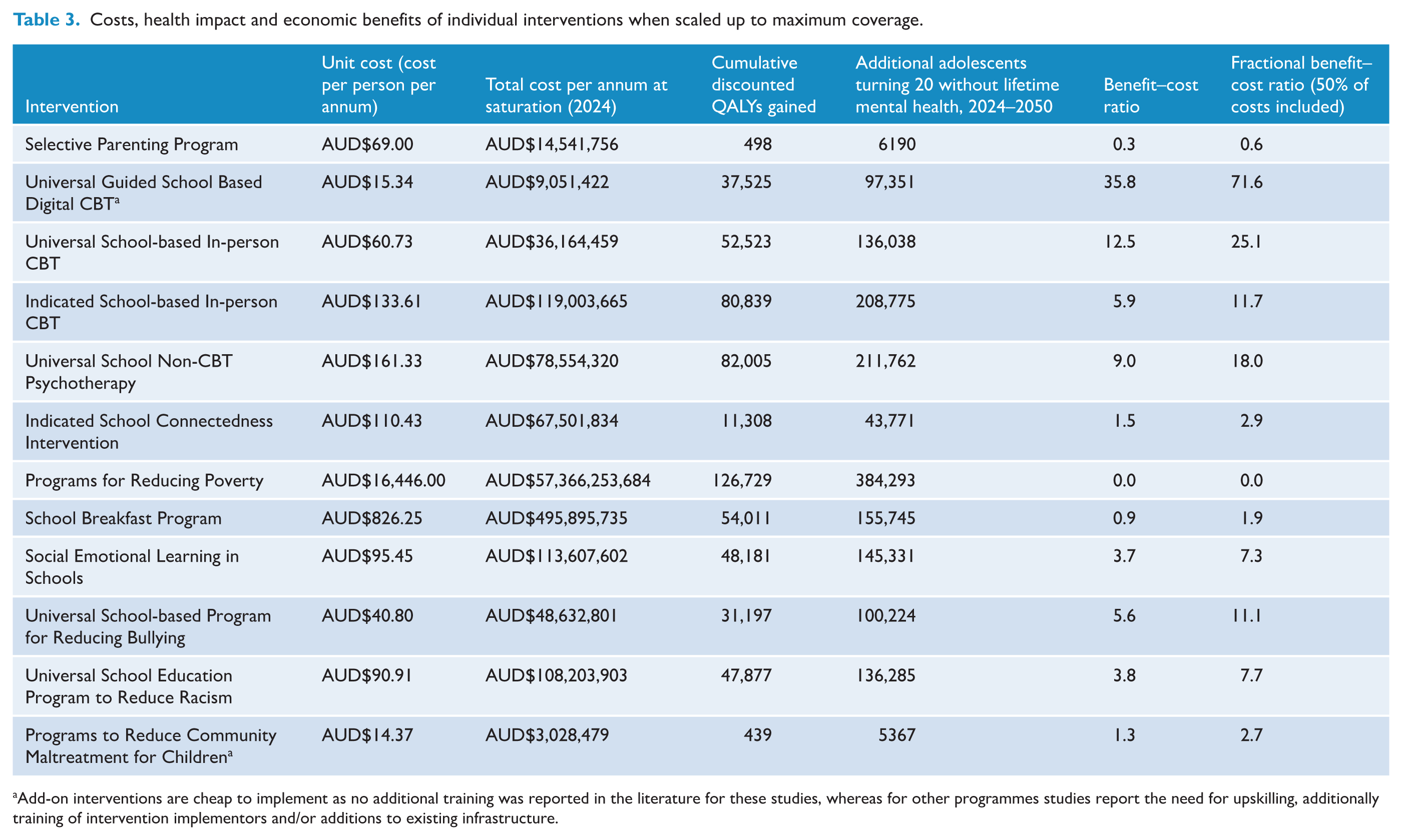
Add-on interventions are cheap to implement as no additional training was reported in the literature for these studies, whereas for other programmes studies report the need for upskilling, additionally training of intervention implementors and/or additions to existing infrastructure.
Scenario 2: individual intervention scale-up by fixed investment
When the same amount of money is spent on each intervention, this changes their impact rankings based on cost-effectiveness. With an investment of AUD$2 million per annum, the universal guided school digital CBT intervention exhibits the greatest cost-effectiveness, followed by the universal school in-person CBT intervention and universal school non-CBT psychotherapy intervention (Figure 4). The universal guided school digital CBT intervention is estimated to cost below AUD$16 per person per year, and so could achieve greater coverage for the same investment as some of the more expensive programmes (e.g. the universal school racism education programme at AUD$90.91 per person per year).
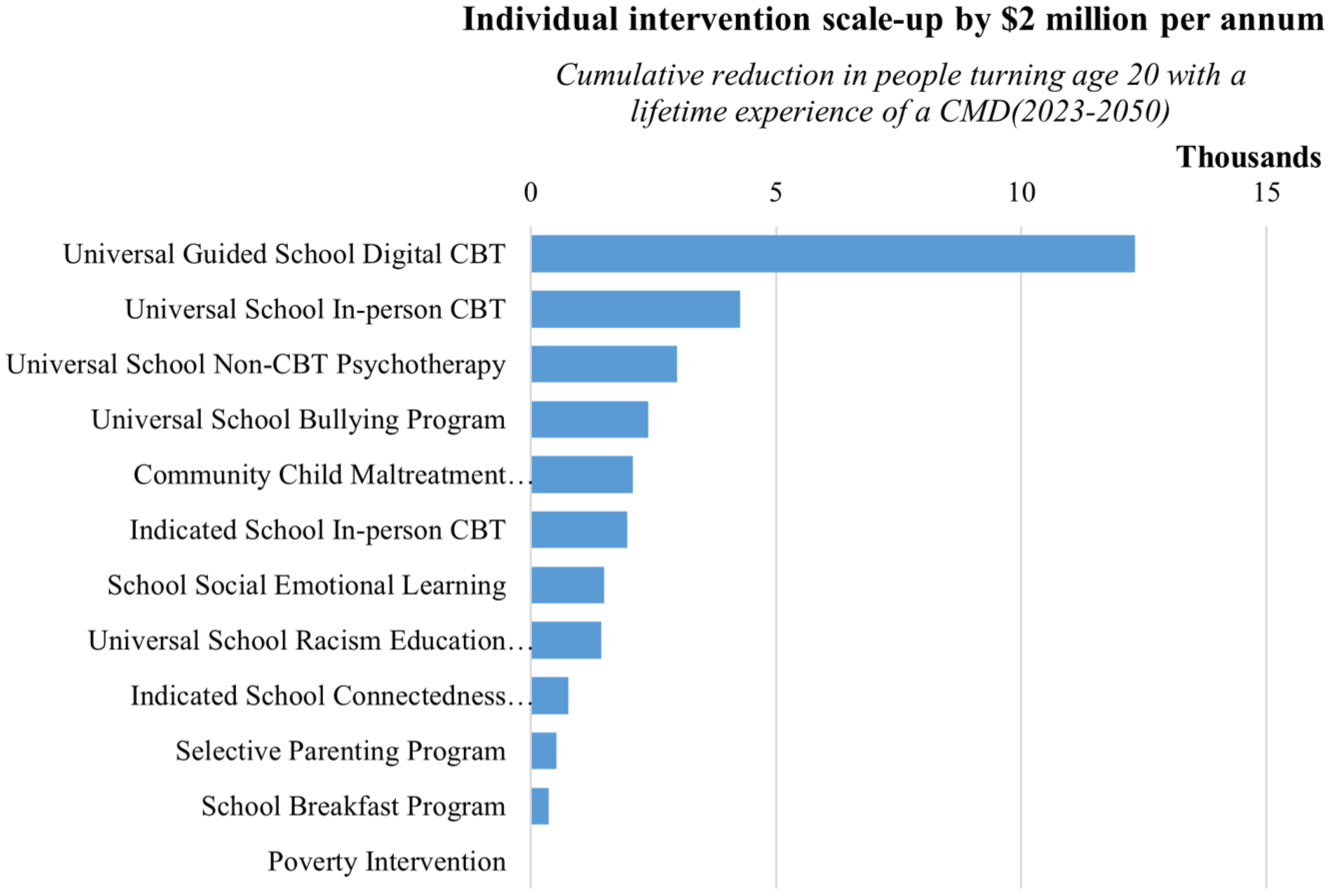
Impact of incremental scale up of interventions ($2 million per annum), maintained 2024–2050.
While universal guided school digital CBT appears among the most cost-effective, it is based on ‘add-on’ interventions to existing services; reliance on existing infrastructure and training reduces the costs, but limits how broadly it could be implemented.
Scenario 3: optimal allocation of funding across interventions
An investment of AUD$50 million per annum on prevention interventions was optimally allocated to a package including the universal guided school digital CBT and universal school in-person CBT (Figure 5) This prioritisation is consistent with the ranking of interventions for individual AUD$2 million investments. An optimised AUD$50 million per annum resulted in 142,539 fewer adolescents turning 20 with a lifetime experience of a CMD between 2024 and 2050.
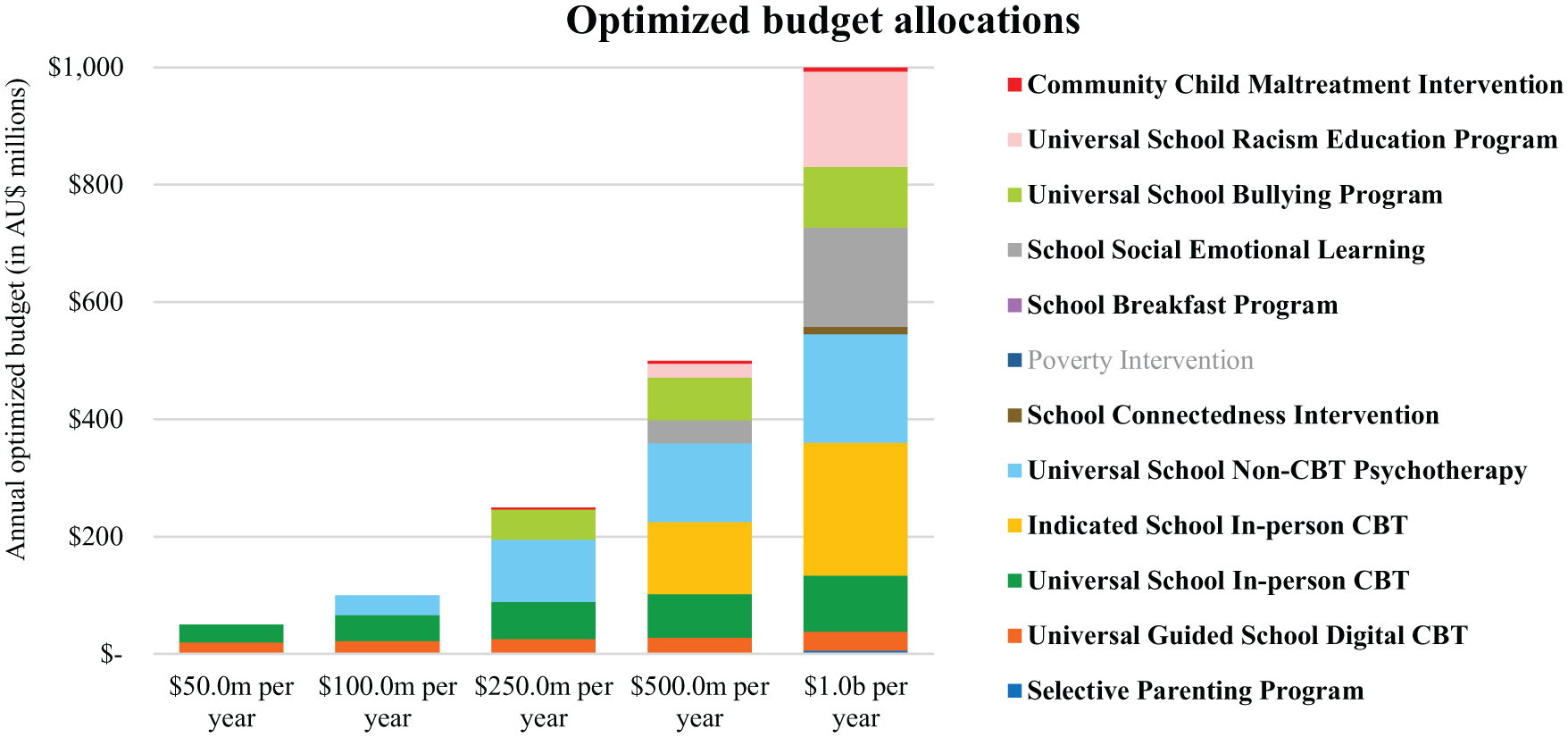
Investment optimisation allocation.
For AUD$100–AUD$250 million per annum investments, universal school non-CBT psychotherapy, universal school bullying programme and the community child maltreatment intervention are funded. For AUD$500 million to AUD$1 billion per annum, the indicated school in-person CBT, school social emotional learning, universal school racism education programme, school connectedness intervention, and selective parenting programme are funded.
Greater impact was achieved with more investment, however there were diminishing returns (Figure 6). Optimised investment of AUD$50 million– AUD$1 billion per annum was estimated to result in an additional 142,539–787,102 adolescents turning 20 without experiencing a CMD, at a cost of AUD$5137–AUD$18,604 per lifetime experience of CMD averted. This was a reduction in the percentage of people turning age 20 with a lifetime experience of CMDs from 50.3% in the baseline to between 40.6% and 48.6%.
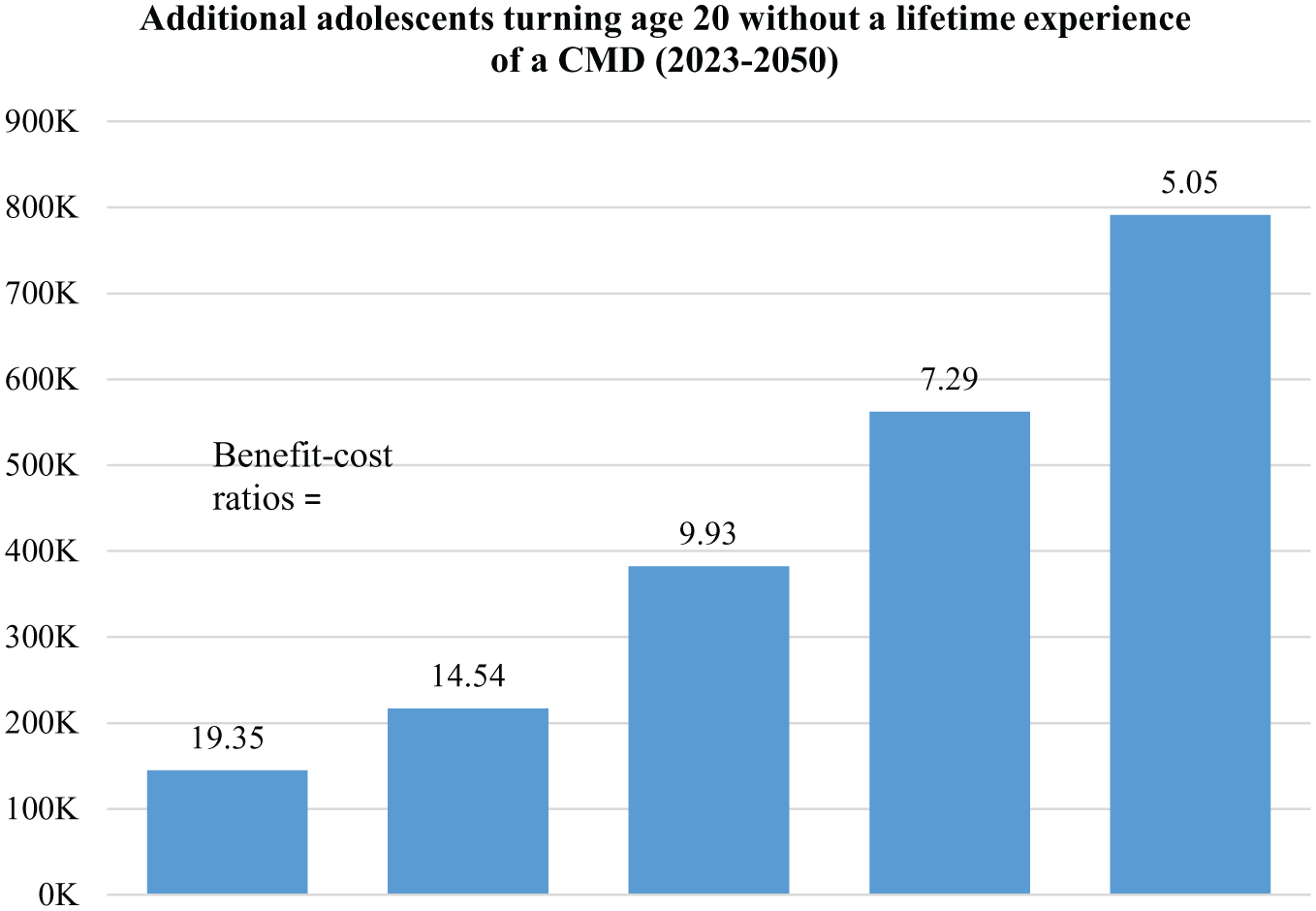
Investment optimisation impact.
In the optimised investment scenarios, total investment with discounting over 2024–2050 was AUD$0.73–AUD$14.64 billion. This resulted in 60,440–316,710 cumulative discounted QALYs gained, AUD$14.07–AUD$73.79 billion in societal economic benefits, and BCRs ranging from 5.0 to 19.2 (Table 4).
Costs, health impact and economic benefits for the optimised investment scenarios.
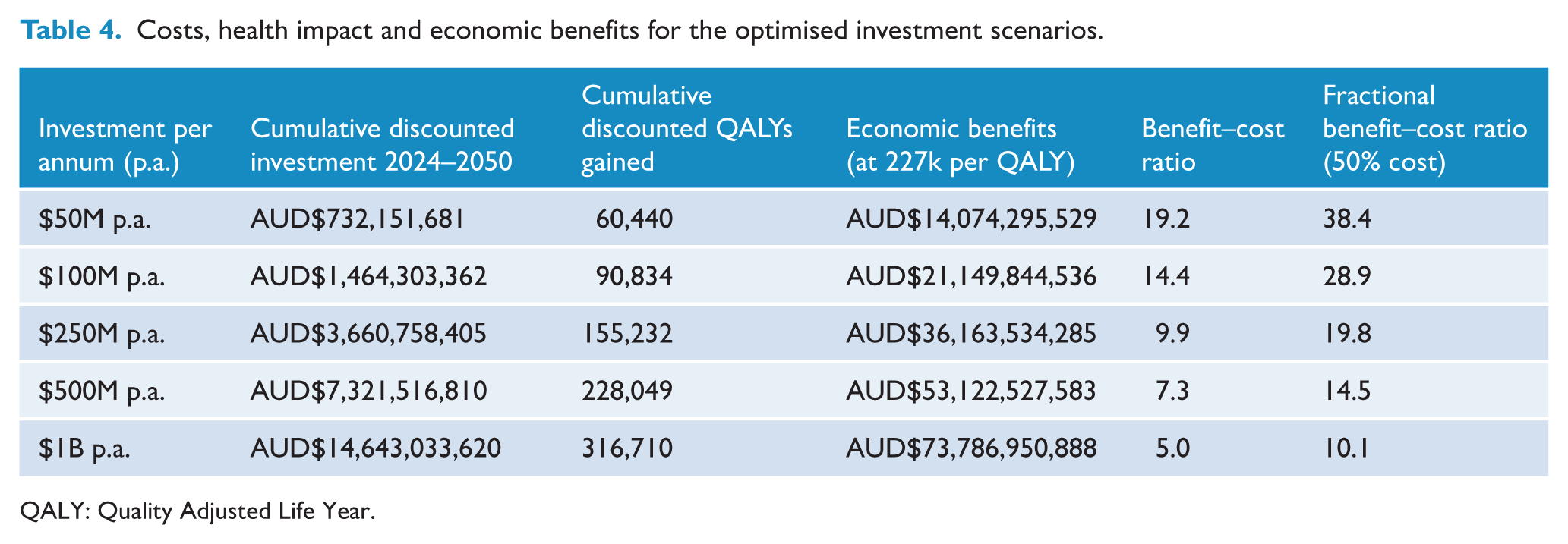
QALY: Quality Adjusted Life Year.
Uncertainty in optimisation results
There is uncertainty in optimisation results whereby different estimates for intervention costs and/or effect sizes can influence their BCRs and hence prioritisation. For example, despite the school breakfast programme resulting in greater impact than the universal school-based racism education programme when scaled up, it had a higher unit cost, resulting in a lower BCR and non-prioritisation within optimisation. If the school breakfast programme could be delivered for only a proportion of the estimated cost, perhaps through integration with other programmes, then the BCR would be proportionally greater, and the prioritisation could change. Similarly, if the reported effect sizes of some programmes were unlikely to be replicated due to implementation challenges, then their BCR would be lower than estimated and the prioritisation could change.
Discussion
This study estimated that investing between AUD$50 million to AUD$1 billion per annum on evidence-based interventions to prevent CMDs in adolescents could lead to 142,539–787,102 fewer adolescents experiencing a CMD by age 20, at a cost of AUD$5137–AUD$18,604 per lifetime experience of a CMD averted. This investment would represent about a doubling of current budget commitments to the National Mental Health and Suicide prevention plan and would likely have a favourable return-on-investment with lower-bound estimates for BCRs ranging from 19.2 with an optimised AUD$50 million per annum to 5.0 with an optimised AUD$1 billion per annum. Poverty intervention and Universal School Non-CBT Psychotherapy had the potential for greatest total impact, while universal guided school-based digital CBT and universal school-based in-person CBT had the greatest BCRs due to their lower costs. The BCRs for different prevention interventions varied widely depending on whether they impacted CMDs directly or indirectly through reduction of a risk factor, the contributions of different modifiable risk factors, the interventions target age, and whether mental health was the primary focus of the intervention or only one of many objectives.
A number of the preventive interventions considered in this analysis are likely to have benefits far greater than estimated as for many interventions, mental health is only one of many domains that they can improve. For example, interventions to reduce poverty, school breakfast programmes, and selective parenting programmes have much broader impacts but in the main analysis the whole costs of the interventions have been included but only a fraction of the benefits. From the available literature it is difficult to quantify what proportion of the overall benefits of these interventions mental health improvements represent, but sensitivity analyses show that the BCR would increase proportionally if they only considered this proportion of costs. The benefits of interventions may also be increased if they are targeted to areas or sub-populations with higher risk factors or poorer baseline mental health where the potential for benefit is greatest.
It is important that a mix of interventions is considered to account for the strengths and limitations of each, as well as the different sub-populations and times in the life-course that they target. For example, Universal Guided School Based Digital CBT and Universal School-based In-person CBT had the highest BCRs and were prioritised in the optimisation; however, both have limited reach as they only target 15–19 year olds. The optimisation combined these interventions with a mix of interventions including programmes to reduce community maltreatment for children less than 10 years old, and interventions to reduce risk factors for CMDs such as bullying and racism. Since these interventions fall under both state and federal responsibility, as well as a mix of education and health department responsibility, the optimisation highlights that a unified cross-sectoral response is required to achieve the greatest returns.
School-based interventions that target the prevalence of poor school connectedness (school connectedness and school social emotional learning intervention) were not as effective as the universal school bullying programme. This was due to the odds ratio for having a CMD with poor school connectedness being lower compared to other risk factors, suggesting it does not contribute as much to the probability of developing a CMD (OR = 2.5 for poor school connectedness vs 3.4 for bullying). However, there are complex interactions between risk factors that are difficult to quantify, and school-based programmes can be more comprehensive and include elements of multiple interventions that were modelled. For example, experiences of racism or bullying would likely impact student connectedness to their school, and interventions have been piloted that aim to both improve school connectedness as well as reduce experiences of bullying or racism (Aldridge and McChesney, 2018; Raniti et al., 2022).
Some outputs from this study can be validated against previous work. The 2020 National Mental Health Commission (National Mental Health Commission, 2020) estimated the BCRs of some of the interventions considered, specifically universal guided school digital CBT (BCR = 3.1 vs 35.8 in this study), universal school in-person CBT (BCR = 1.5–2.0 vs 12.5 in this study) and universal school bullying interventions (BCR = 1.6–2.2 vs 5.6 in this study). A major driver of these differences is that the Commission data were based on 2013 estimates of the prevalence of CMDs for 4–17 year olds (2.8–6.9%) (Lawrence et al., 2015), whereas this study uses more recently available estimates from among 16–24 year olds (32.4–45.5%) (ABS, 2020–2022) for the older age group, and was calibrated to match high cumulative incidence from recent studies (by age 18; 44.8–73.7%) (Robson et al., 2024). As these figures are notably higher, the scope for prevention benefits in this model are significantly greater (ABS, 2020–2022). The Commission also considered the selective parenting programme (BCR = 2.4 vs 0.3 in this study), however we used a different costing methodology in this study.
The increase in the prevalence of CMD which has occurred despite large annual spending on treatment of mental disorders ($13.2 billion in 2019–2020 (AIHW, 2024b)), suggests there is a need to think creatively about intervening to prevent mental disorders. This study demonstrates how cost-effective interventions are needed as part of a comprehensive response, particularly those that target upstream risk factors, that lie beyond clinical settings, and that are not modifications of individually oriented clinical interventions–even if their individual estimated impacts are not large.
There are several categories of limitations to this analysis. First, many prevention interventions could not be included due to limited quantitative evidence, such as those targeting intimate partner violence, incarceration/arrests, maltreatment of older adolescents, discrimination against LGBTQIA+ youth, or policy changes that could lead to positive impacts on mental health but cannot be costed. Among the interventions included, much of the evidence was weak, associative only, taken from non-Australian settings, and with limited information on cost. This clearly reinforces the need for more evaluations of prevention interventions to fill these evidence gaps. Second, there are also varying definitions and interpretations of prevention interventions. For example, many interventions, including those delivered through the health system, may aim to prevent mild or moderate symptoms from worsening, rather than preventing disorder. Independent evaluations of those interventions would be valuable for informing resource allocation decisions. Third, the model does not consider implementation factors, such as workforce with capacity to deliver interventions at scale, but assumes that interventions would be implemented with quality such that the effect sizes from the literature would be applicable and that interventions would reach a plausible number of the eligible population when scaled up (e.g. school-based interventions are only considered in government schools). The model also does not consider targeting of interventions to groups most likely to experience CMDs, or more severe CMDs, including LGBTQIA+ youth, meaning that the results represent population averages only. Fourth, the study only considered the most CMDs, anxiety and depression, rather than other mental health and developmental disorders such as conduct disorder, eating disorders, psychotic disorders, or attention deficit hyperactive disorder (ADHD). Fifth, this study used unit cost estimates derived from resource use reported in previous studies, rather than from actual costing studies which were found to be incomparable across the literature. Sixth, interventions only impact the incidence of new CMDs, due to limited available evidence on the effect of prevention interventions on CMD recurrence (Gili et al., 2015), which is likely to underestimate potential benefits. Seventh, risk factors are assumed to act independently on mental disorders and interactions are not considered due to limited data on the risk of developing CMDs given each combination of risk factor. Eighth, data on incidence and recovery that were provided in CATS (Robson et al., 2024) and used for model calibration are derived from a representative-sample of adolescents in Melbourne Australia, which may not necessarily represent the Australian adolescent population. Furthermore, CMDs in CATS were not measured using diagnostic measures and incidence data from the last two waves may be inflated as these measurements were taken during extensive, government mandated social restrictions to control the COVID-19 pandemic (Robson et al., 2024).
In conclusion, evidence for interventions to prevent CMDs in adolescents is sparse outside of psychotherapy interventions. However, by combining available evidence, it appears likely that investing in a broad set of evidence-based prevention interventions for adolescent mental health would have a favourable return-on-investment. Beyond more research on prevention of CMD outside of psychotherapy, this study highlights the need for greater research into interventions that prevent recurrence of CMDs in adolescence, for further prevention interventions that target risk factors, and for research investigating the interactions between risk factors and their impact on incident mental disorder in adolescents.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251370449 – Supplemental material for Return on investment from interventions to prevent common mental disorders among adolescents in Australia: A modelling study
Supplemental material, sj-docx-1-anp-10.1177_00048674251370449 for Return on investment from interventions to prevent common mental disorders among adolescents in Australia: A modelling study by Alexander J Thomas, Nicola Reavley, Tharindu Wickramaarachi, Kim Sweeny, Holly Erskine, Hanafi Mohamad Husin, Peter Azzopardi, Susan M Sawyer and Nick Scott in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We would also like to acknowledge the late Prof. George Patton, who was pivotal in the conception and planning of this work. We would like to acknowledge the panel of experts who reviewed the set of interventions included in this study; Dr Stephen Carbone, Prof. Anthony Jorm, Prof. Ben Matthews, Prof. Cathy Mihalopoulos, Dr Lakshmi Neelakantan, Dr Monika Raniti and Prof. Bruce Rasmussen.
Correction (November 2025):
This article has been updated to correct the placement of Figures 3 and 4, which were previously presented in the wrong order, and to correct the spelling of the author name Tharindu Wickramaarachchi.
Author contributions
NR, KS, PA, SS and NS conceived the study. AJT, TW and NS developed the model and ran scenarios. NR chaired workshops on model interventions. NR, KS, PA, HMH, HE and SS validated model outputs. AJT, TW and NS drafted the manuscript. All authors contributed to the final version of the manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PA, SS and NS hold National Health and Medical Research Council fellowships.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Health and Medical Research Council Centre for Research Excellence on Driving Global Investment in Adolescent Health (GNT1171981).
Ethical approval and informed consent statements
No ethical approval was necessary for this study as all data used are publicly available and only aggregate values were used for model parameters.
Data sharing statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.