
Abstract
Objective:
Up to one in five children experience mental health problems. Social and cultural factors may influence emergence of mental health problems. The 21st century has led to changes in many of these factors, but it is unclear whether rates of internalizing and externalizing problems have also changed in recent cohorts of young people.
Methods:
A comprehensive literature search was undertaken to locate cohort or population studies that examined changes in mental health of children over time, where participants were aged 18 years and under, and the time frame for change was at least 10 years, with data for at least one time point in the 21st century being statistically compared to at least one time point in the 20th century. Studies were reviewed for quality and outcome.
Results:
Nineteen studies met criteria for review. These included studies of toddlers, children, and adolescents. Seventeen studies examined internalizing problems, and 11 studies examined externalizing problems. For both children and toddlers, recent cohorts did not exhibit worsening of mental health symptoms. In adolescents, the burden of externalizing problems appear to be stable. However, the majority of studies report an increase in internalizing problems in adolescent girls. The findings for internalizing problems in boys were mixed.
Conclusions:
These findings suggest that recent cohorts of adolescent girls are experiencing increases in internalizing symptoms compared to previous cohorts. Approaches for prevention and early intervention should be explored.
Introduction
Research indicates that up to one in five children worldwide experience mental health problems (Kieling et al., 2011; Sawyer et al., 2000). Data from a range of sources suggest that the burden of mental health problems may be increasing. For example, psychosocial problems identified by primary care practitioners in the USA increased from 7% in 1979 to 19% in 1996, with increases observed in both internalizing and externalizing problems (Kelleher et al., 2000). Other studies suggest an increase in rates of depressive disorders (Fombonne, 1995) or suicide attempts (Prosser and McArdle, 1996) in the late 20th century. Another study reported that between 1987 and 1999, adolescent females exhibited an increase in psychological distress (West and Sweeting, 2003).
A number of social changes have occurred in the 21st century that could negatively influence mental health symptoms in current generations of young people and contribute to a persistent rise in mental health burden. For example, Australia and many other developed economies have experienced rising affluence and worsening income inequality (Organisation for Economic Cooperation and Development, 2011), both of which have been associated with mental health problems (Langton et al., 2011; Luthar and Barkin, 2012; Pickett and Wilkinson, 2007; Wilkinson and Pickett, 2010). Changes in the family environment may also contribute to mental health symptoms in children, such as increased rates of single parenting (European Commission: Eurostat, 2012), family conflict (Rutter and Smith, 1995; Sweeting et al., 2010), parental mental health problems (Fatori et al., 2013; Schepman et al., 2011), or emergence of parenting styles that place a lower value on child obedience (Twenge and Campbell, 2009). Other changes that may be implicated in mental health problems include increasing exposure to screen time, internet, and social media (American Academy of Pediatrics, 2009; Carli et al., 2014; O’Keeffe and Clarke-Pearson, 2011; Primack et al., 2009) and increasing pressure within contemporary school settings (Ferrada de Noli, 2013; Sweeting et al., 2010; West and Sweeting, 2003). However, some studies have not been able to identify factors explaining increasing mental health problems across cohorts (Collishaw et al., 2007, 2012). Other commentators have discussed more broad concerns about the negative impact of Western culture on child and adolescent development (Eckersley 2008) or the emergence of narcissism in college students (Twenge et al., 2008).
Despite the growing interest in establishing causes of shifting trends in child and adolescent mental health problems, it remains of primary importance to identify whether the burden of mental health problems in children and adolescents is actually increasing in the 21st century. Narrative reviews of diverse clinical and population studies (Maughan et al., 2005; Prosser and McArdle, 1996; Twenge, 2011) point towards a potential increase in rates of suicide, deliberate self-harm, and substance use. However, it is not clear whether these findings reflect a true increase in the incidence of mental health problems in young people or whether it reflects changes in recognition and diagnosis (Maughan et al., 2005).
To assess whether rates of internalizing and externalizing problems are increasing in prevalence, studies are needed that reliably assess mental health symptoms in repeated cross-sectional community samples or prospective multiple birth cohorts (Wangby et al., 2005). In addition, assessing change over sufficiently long time periods is required – Eimecke et al. (2011) suggest that periods exceeding 7 years are necessary to identify secular change. A number of studies utilizing these approaches are emerging (e.g. (Sourander et al., 2008; Sweeting et al., 2009; Tick et al., 2007b), with mixed results. No published review has attempted to systematically assess whether mental health symptoms in young people are increasing in the 21st century. To address this gap, we aim to conduct a systematic review of recent population and community studies that examine long-term time trends in mental health problems in children and adolescents.
Methods
Search strategy
An extensive search for published and unpublished literature was conducted. The primary databases searched were Medline (Ovid) and PsycINFO (Ovid). The search strategy was: (“mental disorders”.sh OR “behavioral symptoms”.sh OR “child behavior disorders”.sh OR mental OR psychiatric OR internalizing OR externalizing OR psychopathology) AND (child OR adolescent OR youth OR pediatric) AND (“cohort studies”.sh OR prevalence OR incidence OR “population study”) AND (“time factors”.sh OR increase OR decrease OR “over time” OR “time trend” OR “secular trend”). Other databases and government websites searched were Australian Bureau of Statistics, Australian Institute of Health and Welfare, Department of Health UK, Centers for Disease Control and Prevention, TROVE (National Library of Australia; http://trove.nla.gov.au/), TRIP: Turning Evidence Into Practice (www.tripdatabase.com/), and Google Scholar. Syntax was adjusted for specific databases. Reference lists were searched for potentially relevant articles. A search of all content within the University of Queensland libraries was also searched, utilizing the Summon tool, which permits searching all databases and resources within an institution (Serials Solutions; www.serialssolutions.com/en/services/summon/).
Inclusion and exclusion criteria
Criteria for inclusion in the review were: (a) sampling approach used was a consecutive and representative community or school sample, or successive birth cohort data characterized by similar sample selection methodology; (b) age range of participants between 0–18 years; (c) repeated use of similar assessment methods; (d) use of diagnostic interview or formal questionnaire to assess mental health symptoms (self, parent, or teacher report); (e) a time frame for change of 10 years or more; and (f) data for at least one time point in the 21st century was statistically compared to at least one time point in the 20th century.
Studies were excluded from review if: (a) participants were aged more than 18 years or insufficient detail was provided to ascertain participant age; (b) no statistical analysis was conducted; and (c) outcomes analysis only utilized health service data or incidence of suicide, crimes, or drug use rather than mental health symptoms.
Data extraction
All identified abstracts were read for their applicability to the inclusion and exclusion criteria. Potentially relevant articles were then obtained and examined. Articles meeting the inclusion criteria were scrutinized to extract the following information: sample characteristics (age range, sampling source, time frame of study), assessment instruments, and study findings. In studies which utilized multiple assessment questionnaires, outcomes are reported for the instruments with the greatest validity. Directional findings meeting statistical significance (p<0.05) are reported in the results. Effect size was calculated for each study. Cohen’s d was calculated from means and SD or from proportional data, as recommended by the Campbell Collaboration (Wilson, 2014). For studies where multiple measures were used for the same domain, the effect size reported represented the mean effect size for each domain. Study quality was assessed using an 8-point checklist developed by Loney et al. (1998). This checklist includes items that assess sampling approaches, sample size and representativeness, and response rate. Total scores range from 0 (poor quality) to 8 (high quality). Each study was rated by two authors; any differences in classification and scoring for specific items were then discussed until agreement was reached.
Results
Studies identified
Formal database searches yielded 2349 abstracts, which yielded 51 potentially relevant articles. Of these, 15 met inclusion criteria and were included in the final review (Figure 1). Additional searching of reference lists and government databases yielded four additional studies that met inclusion criteria. A number of potentially relevant studies utilized the same dataset and key outcomes of interest. In these cases, the primary study reporting key mental health outcomes was included for review, and additional papers focusing on secondary analyses were excluded (n=7). Overall, 19 articles met criteria for inclusion in review.
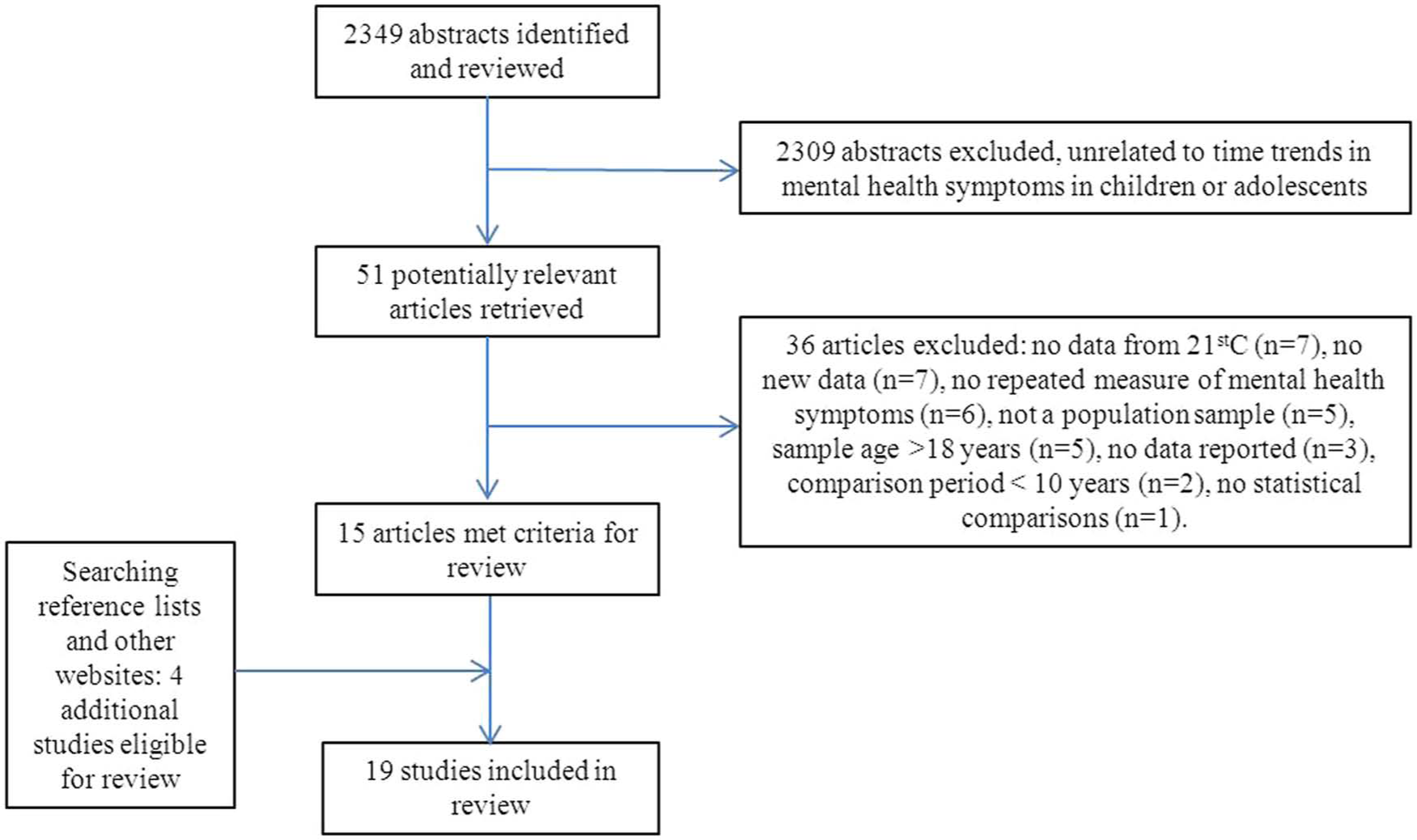
Flow chart of reviewed articles.
Quality scores ranged from 3 to 6 (mean±SD 4.84±1.12). Most studies utilized random sampling methods, unbiased school- or population-based sampling frames, and large sample sizes. Outcomes were typically assessed by questionnaires, completed by the child, parents, or teachers. Some studies utilized questionnaires that cover a range of internalizing and externalizing behaviours, such as the Child Behavior Checklist (CBCL; Achenbach, 2009), the Rutter Questionnaire (Rutter, 1967), or the Strengths and Difficulties Questionnaire (Goodman and Goodman, 2009). Other studies focused on internalizing symptoms only, using questionnaires such as the General Health Questionnaire (GHQ; Goldberg, 1978), and some studies utilized a series of questions specifically developed for the study (Table 1). No studies used formal diagnostic interviews or strategies to reduce interview bias such as using blinded interviewers. Included studies reported results as either change in mean symptom scores, or using threshold ratings. Only one study reported confidence intervals for key prevalence estimates. Participant ages ranged from 2 to 18 years. The majority of studies focused on adolescents, aged from 11–18 years (12 studies). Most eligible studies were conducted in northern Europe. However, studies from Australia, North America, and China were also among included studies.
Summary of studies included in the review, by developmental stage.
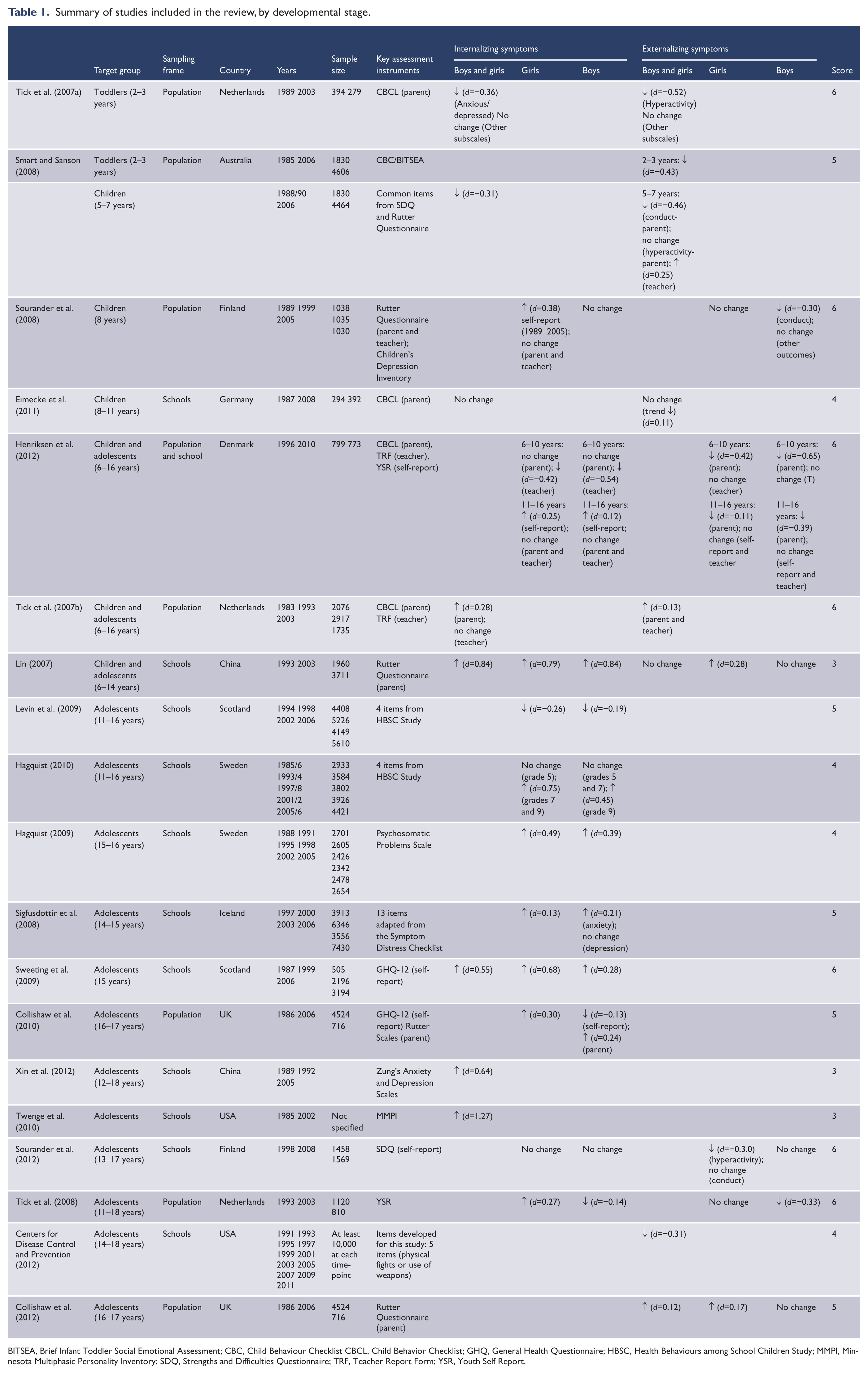
BITSEA, Brief Infant Toddler Social Emotional Assessment; CBC, Child Behaviour Checklist CBCL, Child Behavior Checklist; GHQ, General Health Questionnaire; HBSC, Health Behaviours among School Children Study; MMPI, Minnesota Multiphasic Personality Inventory; SDQ, Strengths and Difficulties Questionnaire; TRF, Teacher Report Form; YSR, Youth Self Report.
Toddlers
Two studies assessed changing mental health symptoms in toddlers between the 1980s and 2000s (Smart and Sanson 2008; Tick et al., 2007a). Between 1989 and 2003, Tick et al. (2007a) reported a significant improvement in parent-reported hyperactivity symptoms and anxious/depressed ratings. No significant gender interactions were reported. Similarly, Smart and Sanson (2008) reported an improvement in aggression ratings of Australian pre-school children from 1985 to 2006 (Table 1) and also reported improvements in a range of temperament ratings including sociability, persistence, reactivity, and sleep problems (Table 1). Neither study reported any increase in mental health symptoms. The quality ratings of both studies were in the upper range for the studies meeting inclusion criteria (ratings of 5 and 6 out of a possible total of 8). The effect sizes (Cohen’s d) for reported reductions in mental health symptoms ranged from 0.36 to 0.52.
Children
Four studies examined changes in both internalizing and externalizing symptoms in children (aged 6–11 years). Eimecke et al. (2011) reported no changes in either parent-rated internalizing or externalizing symptoms, between 1987 and 2008. Outcomes were not separately reported for boys and girls. Between 1989 and 2005, Sourander et al. (2008) reported an increase in self-reported internalizing symptoms in girls (d=0.38). No increases were reported in parent or teacher ratings of internalizing symptoms for girls, and no changes were reported in any internalizing symptoms in boys. In contrast, ratings of externalizing symptoms did not increase: parent and teacher ratings of conduct problems in boys improved over time (d=−0.30), mainly improving between 1989 and 1999. Hyperactivity problems in boys also improved over the same period, but returned to baseline levels by 2005. In girls, no changes were observed in externalizing behaviours over time. Smart and Sanson (2008) also examined children aged 5–7 years, in 1988 and 2006. They reported a worsening of teacher-rated conduct and hyperactivity problems (d=0.25); however, parent-rated conduct problems improved (d=−0.46), and parent-rated hyperactivity problems exhibited no change. Both parent and teacher reports of anxiety symptoms exhibited improvements over time (d=−0.38), and they also reported improvements in the temperament domains of sociability and reactivity (Smart and Sanson, 2008). A Danish study (Henriksen et al., 2012) examined change from 1996 to 2006, and reported findings for children aged 6–10 years. Parent-reports of externalizing symptoms were lower in 2010, in both boys (d=−0.65), and girls (d=−0.42), whereas no changes were observed in teacher reports of externalizing problems. In contrast, teacher reports of internalizing problems reduced over time in both boys (d=−0.54), and girls (d=−0.42), with no change in parent reports (Henriksen et al., 2012).
Three of these studies were conducted in northern Europe, and one was conducted in Australia. Study quality of included studies ranged from 4–6. Neither of the two highest-quality studies (Henriksen et al., 2012; Sourander et al., 2008) reported an increase in externalizing problems. The only discrepancy between these studies is for internalizing symptoms in girls: Sourander et al. (2008) reported an increase in self-reported symptoms, whereas Henriksen et al. (2012) described no change or reductions in parent and teacher reports of internalizing symptoms.
Mixed samples of children and adolescents
Two studies reported changes in mental health symptoms in mixed samples of children and adolescents (age range 6–16 years), focusing on the overall sample rather than separating age groups. Tick et al. (2007b) reported an increase in parent ratings of both internalizing and externalizing symptoms. Secondary analysis suggested that these findings may not be uniform across age groups and time periods: certain scales, including withdrawn/depression subscale, aggressive subscale, and externalizing problems, actually decreased in children between 1983 and 1993, while increasing in adolescents during the same time period. Findings were not reported separately for gender. Using a Chinese version of the Rutter Scales, Lin and Wang (2007) reported an increase in internalizing symptoms from 1993 to 2003 in both girls and boys. Externalizing symptoms in girls also increased over time, whereas no change in externalizing symptoms was observed in boys, and the group as a whole. Effect sizes for the higher-quality study (Tick et al., 2007b) were smaller than those reported for the lower-quality study (Lin and Wang, 2007) (Table 1).
Adolescents
Twelve studies examine changes in mental health symptoms of adolescents. Eight of these studies examined internalizing symptoms only. Of all studies that reported on internalizing symptoms, only one of these reported a consistent improvement in mental health in recent decades. A Scottish study (Levin et al., 2009) utilized four questions from the Health Behaviours among School Children Study (HBSC) (Wold et al., 1994) incorporating confidence, helplessness, feeling left out, and feelings about life. They reported a significant improvement in girls and boys between 1994 and 2006.
In contrast, a Swedish study (Hagquist, 2010), also utilizing four questions from the HBSC (items on sleep problems, feeling low, irritability, and feeling nervous), reported a worsening of symptoms in older groups of girls (grades 7 and 9) and boys (grade 9) from 1985 to 2005. Analysis indicates that for most items, the lowest scores were observed in 2001, with a minor improvement between 2001 and 2005. No changes over time were observed for younger grades (Table 1). Another Swedish study (Hagquist, 2009), utilized the Psychosomatic Problems Scale and reported that severity of internalizing problems worsened in girls and boys between 1988 and 2005. Three European studies reported worsening internalizing symptoms in recent cohorts of girls (Collishaw et al., 2010; Sigfusdottir et al., 2008; Sweeting et al., 2009), but the pattern in boys was less consistent. Sigfusdottir et al. (2008) reported an increase in boys anxiety, but not depression, whereas Collishaw et al. (2010) reported an improvement in self-reported internalizing symptoms, but worsening of parent-reported symptoms. Sweeting et al. (2009) reported a worsening between 1999 and 2006, and also a worsening in the analysis which combined genders. Two studies, one from China (Xin et al., 2012) and one from the USA (Twenge et al., 2010) both reported an increase in internalizing symptoms in recent cohorts, but did not separate analysis by gender.
Three studies reported on both internalizing and externalizing symptoms in adolescents (Henriksen et al., 2012; Sourander et al., 2012; Tick et al., 2008), and two focused on externalizing symptoms only (Centers for Disease Control and Prevention, 2012; Collishaw et al., 2012). Sourander et al. (2012) reported no change in self-reported internalizing symptoms, in both girls and boys. A reduction in hyperactivity ratings over time was observed in girls, with no change in other externalizing indicators in girls and boys (Table 1). A Dutch study (Tick et al., 2008), utilizing the Youth Self Report Questionnaire in 1993 and 2003, reported that internalizing symptoms increased in girls but decreased in boys. Externalizing symptoms also decreased in boys across cohorts, but did not change in girls. A US study reported the trends for externalizing behaviours were declining during the 1990s, with consistent stability (no increase) in the last decade (Centers for Disease Control and Prevention, 2012). The study of Danish adolescents (Henriksen et al., 2012) found an increase in self-reported internalizing symptoms in boys and girls, but no change in parent- or teacher-rated symptoms. In contrast, there was a reduction in parent-rated externalizing behaviours in both girls and boys, but no change in teacher or self-reports. Collishaw et al. (2012) assessed externalizing symptoms only using the Rutter Questionnaires. Between 1986 and 2006, ratings worsened in girls and in the group as a whole; no change was detected in boys (Table 1).
Study findings are not consistently influenced by study quality. For example, the three highest-rated studies examining internalizing symptoms in adolescents reported increased internalizing symptoms in boys (d=0.28) and girls (d=0.68) using the GHQ (Sweeting et al., 2009), no change in internalizing symptoms using the SDQ (Sourander et al., 2012), and increased internalizing problems in girls (d=0.27), but decreased symptoms in boys (d=−0.14) using the YSR (Tick et al., 2008). Overall, of the eight studies examining internalizing symptoms separately in boys and girls, six studies reported increased symptoms in girls. The two studies reporting a decrease or no change (Levin et al., 2009; Sourander et al., 2012) did not exhibit consistent differences from the other studies with regard to study location or study quality. Reports of internalizing symptoms in boys were more diverse, with only two studies reporting a clear increase (Hagquist, 2009; Sweeting et al., 2009) (Cohen’s d 0.28–0.39, study quality ratings 4–6). Two studies reported a consistent decrease in symptom burden (Levin et al., 2009; Tick et al., 2008) (quality ratings 5 and 6). The remaining studies reported mixed findings or no change (quality ratings 3–6). Further description of findings for studies that examined internalizing symptoms using standardized questionnaires are presented in Table 2.
Data for self-reported and parent-reported internalizing symptoms in adolescents for studies that used standardized questionnaires in boys and girls.
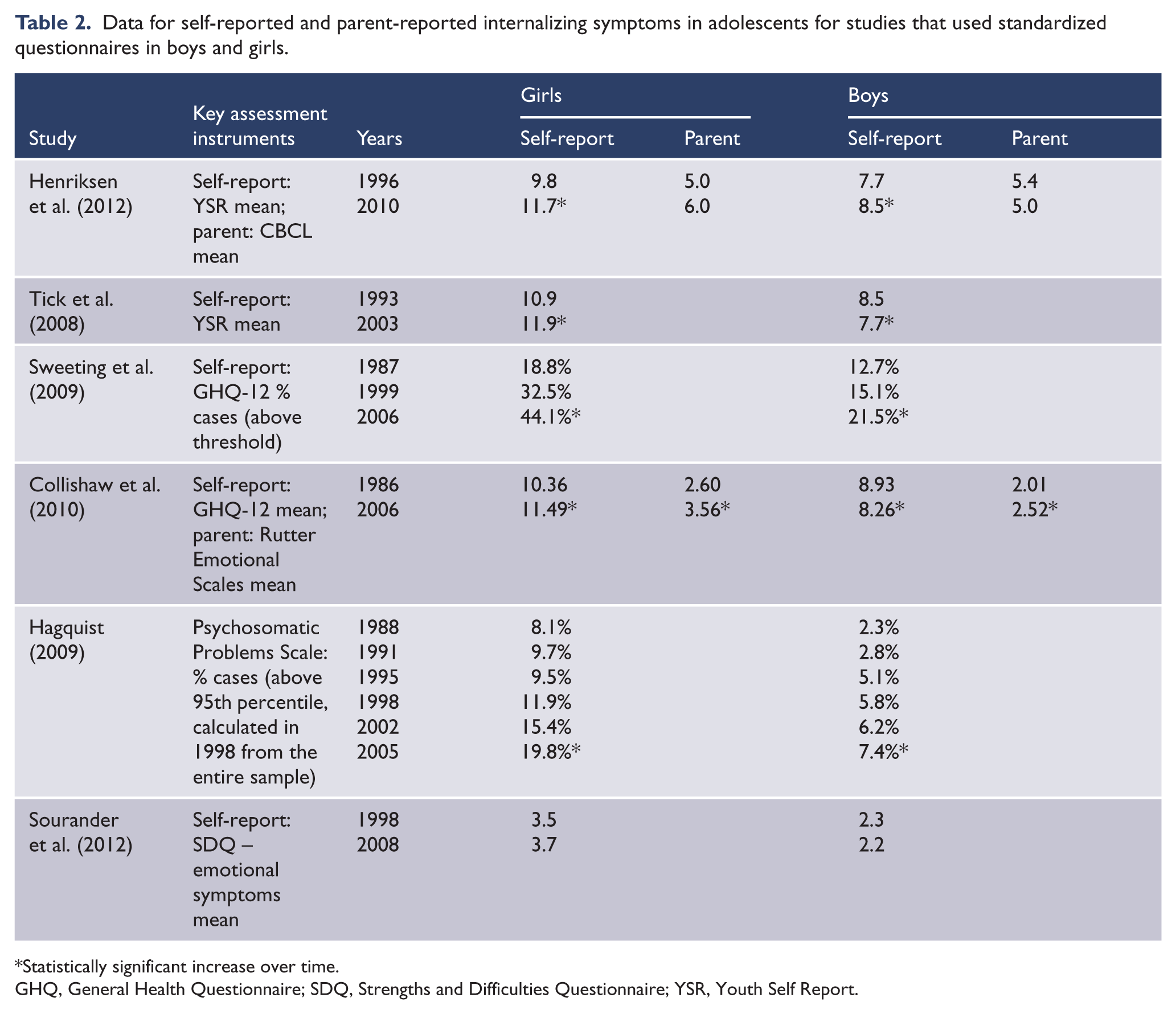
Statistically significant increase over time.
GHQ, General Health Questionnaire; SDQ, Strengths and Difficulties Questionnaire; YSR, Youth Self Report.
Neither of the two highest-quality studies examining externalizing symptoms reported an increase in problems (Sourander et al., 2012; Tick et al., 2008), with symptom ratings exhibiting a decrease (Cohen’s d between −0.33 and −3.0) or no change. Both of these were conducted in northern Europe. Only one study (Collishaw et al., 2012) (quality rating of 5), conducted in the UK, reported an increase in externalizing problems, in girls (d=0.17) and the combined group (d=0.12). No change was reported in boys.
Discussion
This review of time trends of young people’s mental health into the 21st century examines 19 epidemiological studies conducted across 12 countries. Overall, results indicate that the changing trajectory of mental health burden in young people depends on symptom type, gender, and developmental stage. Generally, in both children and toddlers, recent cohorts do not exhibit worsening of mental health symptoms, with most studies reporting an improvement or no change across a variety of indicators.
The overall findings for adolescents are different. The burden of externalizing problems appears to be stable: no studies reported an increasing burden of behaviour problems in boys, and only two studies reported an increase in girls. However, the findings for internalizing problems suggest an increasing symptom burden in recent cohorts of adolescents, especially girls. Five of eight studies reported an increase in internalizing symptoms in adolescent girls, with the others reporting mixed findings, a decrease or no change. In boys, three studies report an increase, two report a decrease, and four report mixed findings or no change. The studies included in this review are diverse with respect to country of origin, sample, and method of outcome assessment. Yet, most studies point to a deterioration in internalizing problems occurring in adolescent girls.
Our findings raise the question of why recent generations of adolescent girls may be at greater risk of internalizing problems. It is well established that there are gender differences in rates of depression and anxiety disorders, with women more likely to experience these disorders than men (Zahn-Waxler et al., 2008). Gender differences in adolescent experience of mood-related indices may increase with age (Torsheim et al., 2006). However, it is not clear why recent generations of adolescent girls are at greater risk than earlier cohorts. West and Sweeting (2003) suggest that accumulation of worries about success in education and personal issues such as weight and appearance combine to create increasing pressures on adolescent girls. Girls may be more negatively influenced by school performance pressure, with one study reporting that two-thirds of girls experienced significant school pressure compared to only one-third of boys (Wiklund et al., 2012). Recent generations of girls are exposed to earlier sexualization, which has been associated with poor self-esteem and depressed mood (American Psychological Association, 2010; Hatch, 2011; Reist, 2009; Sweeting et al., 2007). Many commentators have highlighted how other societal changes negatively affect women, such as changing media and consumer culture (Hamilton, 2008), and changing nature of transitions and cultural expectations for adolescent girls (Eckersley 2008). Hankin et al. (2008) suggest that girls are more socio-emotionally attentive than boys, where negative cognitive style and rumination can interact to predispose girls to depression. Research also suggests that the current generation of girls may be experiencing onset of puberty earlier than previous generations (Euling et al., 2008), which may be associated with increased risk of depressive disorders (Crockett et al., 2013; Galvao et al., 2014; Patton et al., 2008). Our review is not able to address potential causes of increased internalizing problems in adolescent girls – it is possible that factors such as these all contribute to risk of mental health symptoms.
Another possible explanation for the increased symptom reports observed in this review is increased readiness to report symptoms. It has been suggested that changing attitudes and awareness of mental health problems may increase frankness of reporting, leading to greater likelihood of disclosing symptoms or behaviours. It is not possible to exclude this issue from these studies. However, study findings do not suggest that increased symptom reporting is a generalized effect, given that observed increases are restricted to certain items (Collishaw et al., 2010) and do not occur consistently across income groups (Langton et al., 2011). Qualitative studies suggest that girls are not necessarily more willing than boys to report emotional symptoms (Maclean et al., 2010). In our study, increases in mental health symptoms were limited to problems in adolescent girls, with no clear increases in most other subgroups. Collectively, these factors suggest that increased frankness of reporting is unlikely to be a key explanatory factor for our finding.
Limitations
One of the limitations of this study is the reliance on studies that utilized symptom and behaviour ratings rather than more objective measures such as diagnostic interviews. In some cases, such as those studies utilizing the HBSC datasets, ratings were made using a small number of items, with limited validation. Although short scales and symptom questionnaires may detect a lower threshold of problems than diagnostic interviews, they do identify the presence of symptoms which may be distressing or burdensome. In children, many symptom questionnaires have been shown to have good predictive capacity (Goodman, 2001) and to identify groups of young people at higher risk for adverse outcomes (Goodman and Goodman, 2009; Haugland and Wold, 2001; Hofstra et al., 2001). In adolescence, reporting single symptoms of depression is associated with later onset of a diagnosis of depressive disorder (Wolitzky-Taylor et al., 2014). In adults, subsyndromal symptoms of depression are associated with a similar degree of social dysfunction and disability as a diagnosis of depression (Lewinsohn et al., 2000). Given that the number of studies eligible for inclusion was small, restricting our approach to include only diagnostic studies or studies that utilized questionnaires such as the CBCL would limit our understanding of this issue. However, this limitation does highlight the importance of future studies assessing time trends in mental health symptoms and the value of long-term population studies that utilize consistent methodologies across multiple cohorts.
Conclusion
This systematic review of secular changes in mental health symptoms suggests that the burden of internalizing symptoms is increasing in adolescent girls. Observed increases were not restricted to Western nations. From our findings, it is unclear whether this is also occurring for boys. This finding has a number of public health implications. The association between symptom reports in adolescents and adverse outcomes reinforces the importance of prevention, identification, and treatment programmes. It is unclear whether observed increases would translate into increased demand for mental health services during adolescence or later in adulthood. Nonetheless, it remains essential for further research to regularly monitor trajectories of mental health symptoms in young people to permit appropriate public health responses and for policy makers to ensure that evidence-based approaches to prevention and treatment are adequately resourced and implemented.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.