
Abstract
Background:
Clinical features of attention deficit hyperactivity disorder can be frequently observed in cases with bipolar disorders and associated with greater severity of bipolar disorders. Although designed as a screening tool for attention deficit hyperactivity disorder, the Wender Utah Rating Scale could, given its factorial structure, be useful in investigating the early history of impulsive, inattentive or mood-related symptoms among patients with bipolar disorders.
Methods:
We rated the Wender Utah Rating Scale in 276 adult bipolar disorder cases and 228 healthy controls and tested its factorial structure and any associations with bipolar disorder phenomenology.
Results:
We confirmed a three-factor structure for the Wender Utah Rating Scale (‘impulsivity/temper’, ‘inattentiveness’ and ‘mood/self-esteem’). Cases and controls differed significantly on Wender Utah Rating Scale total score and sub-scale scores (p-values < 10−5). About 23% of bipolar disorder cases versus 5% of controls were classified as ‘WURS positive’ (odds ratio = 5.21 [2.73–9.95]). In bipolar disorders, higher Wender Utah Rating Scale score was associated with earlier age at onset, severity of suicidal behaviors and polysubstance misuse; multivariate analyses, controlling for age and gender, confirmed the associations with age at onset (p = 0.001) and alcohol and substance misuse (p = 0.001).
Conclusion:
Adults with bipolar disorders who reported higher levels of childhood symptoms on the Wender Utah Rating Scale presented a more severe expression of bipolar disorders in terms of age at onset and comorbidity. The Wender Utah Rating Scale could be employed to screen for attention deficit hyperactivity disorder but also for ‘at-risk behaviors’ in adult bipolar disorder cases and possibly for prodromal signs of early onset in high-risk subjects.
Introduction
Bipolar disorder (BD) is highly heterogeneous in terms of its clinical expression, course and comorbidities. For most patients, onset occurs during adolescence or young adulthood (Bellivier et al., 2014; Etain et al., 2012), but some (non-specific) symptoms are likely to occur very early during childhood (Duffy, 2010; Duffy and Carlson, 2013; Scott et al., 2013). Retrospective assessment of childhood symptoms and clinical dimensions among adult cases with BD may shed light on several issues such as (1) understanding links between adult BD syndromes and various childhood-onset psychiatric conditions (typically attention deficit hyperactivity disorder [ADHD]), (2) the identification of (non-)specific precursors of BD according to staging models and (3) the investigation of associations between these dimensions and the severity of clinical trajectories of BD in adults. The Wender Utah Rating Scale (WURS) has been developed to retrospectively assess childhood symptoms of ADHD (Ward et al., 1993). Although typically employed as a screening tool, the WURS is not specific for ADHD and its factorial structure captures different childhood dimensions (impulsivity/temper, inattentiveness and mood lability) that transcend diagnostic categories. It is likely that trans-nosographic symptoms and dimensions assessed by self-report questionnaires such as the WURS can help detect features of a BD prodrome characterized by externalizing behaviors, inattention or emotion dysregulation.
It is noteworthy that BD and ADHD are frequently identified as co-occurring and ADHD is the second most common comorbid condition (after anxiety disorders) observed in pediatric BD (Frias et al., 2015). Furthermore, a recent Swedish population-based study with the largest BD cohort ever reported that ADHD was the most common Diagnostic and Statistical Manual of Mental Disorders (DSM) axis I comorbid condition in adults (Song et al., 2015). It is proposed that ADHD can be part of a typical developmental illness trajectory of BD, although this notion is controversial (Duffy, 2012; Skirrow et al., 2012) and the association may be an artifact arising from the overlap in clinical symptoms across the syndromes (for review, see Youngstrom et al., 2010). However, it is also possible that a shared genetic vulnerability could explain overlapping symptomatology and/or the existence of a clinically homogeneous sub-group of BD with ADHD-like features (Faraone et al., 2012). The use of the WURS in adult patients with BD can provide further insights regarding the frequency of such symptoms during childhood and clarify whether sub-dimensions are particularly encountered in children who subsequently develop BD.
Second, staging models of BD (Scott et al., 2013) describe a continuum from unaffected, but an at-risk state through to non-mood disorders or sub-threshold presentations (e.g. anxiety, ADHD symptoms) through to minor then major mood disturbances, depression and mania (Duffy et al., 2010). Longitudinal studies are necessary to help to identify clinical signs that predict transitions to nosographic clinical entities. However, such prospective studies are resource-intensive, often suffer from high dropout rates (Leopold et al., 2012) and very large samples of young people are required in order to capture the minority who will develop BD. Although methodologically weaker, retrospective studies in adults with established BD can help point toward some of the sub-syndromal states or precursors that form part of a neurodevelopmental pathway to BD. In this context, both prospective and retrospective studies can foster the identification of risk constellations prior to the development of BD that include multiple elements such as genetic risk, substance misuse, ADHD features, sub-threshold affective symptoms, changes in sleep and circadian rhythms and mood swings/affective lability (Leopold et al., 2012). The use of the WURS-derived dimensions in adult BD cases may thus help to clarify whether the inclusion of ADHD features in this pathway of childhood symptoms is clinically relevant and worth investigating prospectively.
Third, it has been suggested that a history of ADHD features in childhood may be associated with a more severe clinical trajectory for BD and a worse prognosis. For example, the presence of ADHD has been associated with earlier onset of BD (Masi et al., 2006; Perlis et al., 2004), and a recent systematic review has suggested that BD type I and comorbid ADHD were significantly associated with suicide attempts (SA) in children and adolescents with BD (Hauser et al., 2013). The latter finding has been reinforced by a Taiwanese nationwide longitudinal study that reported that ADHD was an independent risk factor for attempted suicide later in life among adolescents and young adults with BD (Lan et al., 2015). Also, compared to patients without a lifetime history of ADHD, BD cases with comorbid ADHD have higher comorbidity rates for axis I disorders, such as panic disorder and alcohol abuse/dependence (Perugi et al., 2013; Tamam et al., 2008; Torres et al., 2015). In a sample of 90 patients with BD, Karaahmet et al. (2013) demonstrated that ‘WURS-positive’ cases (defined by a total WURS score >36, which is the cut-off for the Turkish language version) had an earlier age at onset and a trend to higher rates of alcohol dependence (Karaahmet et al., 2013). In a study of 250 adult patients with mood disorders assessed with the WURS, Joo et al. (2012) showed that patients with BD II and recurrent depressive disorders scored higher on the WURS total score as compared to controls, with BD I cases displaying intermediate scores (Joo et al., 2012). However, with the exception of one study (Lan et al., 2015), these results have been obtained in small-scale studies, mixed samples of BD and non-BD mood disorders or studies using different assessments of ADHD (presence/absence of ADHD, WURS scores, etc.). The available research indicates that the influence of ADHD symptoms or sub-syndromal ADHD presentations on the clinical expression of adult BD requires further clarification and the use of an established tool such as the WURS might enhance our understanding and allow greater cross-study comparisons.
The aims of this study are (1) to explore the factorial structure of the 25-item WURS in an independent sample, (2) to compare total WURS and WURS sub-scale scores in BD cases and healthy controls and (3) to investigate any association between ADHD features and markers of the clinical severity of BD (e.g. suicidal behavior) and illness complexity (e.g. substance misuse).
Methods
The research protocol (INSERM C0829) received approval by the Ethical Committee and institutional review board; written informed consent was obtained from all study participants. The consent process involved a detailed description of the study by a psychiatrist supplemented by written information summarizing the protocol and project for the individual.
Sample
Individuals referred to the clinic services at four university-affiliated psychiatric departments in France (Paris/Créteil, Bordeaux, Nancy) with a presumed diagnosis of BD were interviewed using the French version of the Diagnostic Interview for Genetic Studies (DIGS) (Nurnberger et al., 1994) to assess lifetime Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) axis I diagnoses (American Psychiatric Association, 1994). The study sample comprised 276 outpatients who met the following inclusion criteria: aged ⩾18 years old; met DSM-IV criteria for BD I, II or NOS (not otherwise specified); currently euthymic (i.e. scoring ⩽5 on both the Montgomery–Asberg Depression Rating Scale and the Mania Rating Scale) (Bech et al., 1978; Montgomery and Asberg, 1979) and willing and able to give written informed consent.
Healthy controls (N = 228) were recruited from adult blood donors and the general population. Only those who were free of any personal history of DSM-IV axis I psychiatric disorders, as assessed with the DIGS (Nurnberger et al., 1994), and had no first-degree relatives with a history of mood disorders, schizophrenia or SA (as assessed with the Family Interview for Genetic Studies [FIGS]) were included in the study.
WURS
The WURS is a 25-item self-administered instrument that retrospectively measures ADHD symptoms experienced by individuals before the age of 12 years (Ward et al., 1993). Each item is rated on a 4-point scale. All participants completed the French version of the WURS, the psychometric properties of which have been previously described (Caci et al., 2010). A threshold of 46 is indicative of a possible ADHD in childhood and can be used to classify cases as ‘WURS positive’ (Ward et al., 1993).
Clinical indicators of the course of BD
We selected key clinical variables identified as important characteristics of BD and indicators of a more severe or complex course including subtype of BD, mode of onset (age at onset and polarity at onset), lifetime history of SA, rapid cycling, substance misuse (alcohol, cannabis and other drugs misuse) or psychotic features (lifetime presence during at least one mood episode).
Age at onset has been defined as the age at which the patient fulfilled for the first time the DSM-IV criteria for a depressive, (hypo)manic or mixed episode based on the DIGS.
The DIGS allows the recording of several variables for suicidal behaviors (lifetime history of and number of SA and lifetime occurrence of at least one violent SA), so we used this information to create a composite variable with a 0–3 rating, with higher scores indicative of more of the construct under study. The rating is the sum of the following: lifetime presence of SA (rated 0 if absent or 1 if present), lifetime presence of violent SA (rated 0 if absent or 1 if present) and presence of multiple SA (0 if only one SA; 1 if two or more SA). We used the term violent suicidal attempt for any attempt characterized by attempted hanging, the use of firearms, jumping from heights, severe deep cuts, car crash, burning, gas poisoning, drowning, electrocution and jumping under a train (Asberg et al., 1976). Drug overdoses were considered to be non-violent SA. Individuals with no SA received a score of 0, and those with lifetime presence of multiple SA including at least one violent SA scored 3.
We created a similar composite score for substance misuse, categorizing the patients according to no misuse (rated 0), presence of cannabis misuse (rated 1), presence of alcohol misuse (rated 2) and presence of cannabis and alcohol misuse or other drug (cocaine, opiates, amphetamines) misuse (rated 3). We used the term misuse for both abuse and/or dependence.
Statistical analysis
Data analysis was conducted using R program. To take multiple testing into account, we used a Bonferroni correction to determine the threshold for significance, which was set at p ⩽ 0.003.
Factor analysis
We began by conducting an exploratory factor analysis using a Principal Component Analysis (PCA) with promax rotation. To measure the appropriateness of PCA, we used the Kaiser–Meyer–Olkin index (KMO) and Bartlett’s test of sphericity. To define the number of factors to retain, we used Parallel Analysis (PA) (PA implies a Monte Carlo simulation process since ‘expected’ Eigenvalues are obtained by simulating normal random samples that parallel the observed data in terms of sample size and number of variables) combined with Cattell’s Scree Test (which identifies the inflexion point on the Eigenvalue graph). Factor loadings ⩾0.40 were considered as significant and thus were retained. As we consider independent factors, when an item has a factor loading ⩾0.40 for several factors, it was considered as unclassified. For analyses that required the inclusion of all WURS items, we classified items with loadings <0.4 with the factor they showed the highest loading for.
Case–control comparisons and analysis of WURS in the BD group
Between-group comparisons were performed using chi-squared tests for categorical variables and t-tests or non-parametric tests for continuous variables as appropriate. Odds ratios (OR) and 95% confidence intervals (95% CI) are given for selected categorical comparisons.
We used linear regressions to take into account the effects of age at interview and gender as appropriate, e.g., when exploring associations between suicidality ratings and WURS scores (as this behavior can vary according to age and gender). BoxCox power transformations were used for all scores to fulfill the normality assumption required for parametric procedures. When an association was identified for the WURS total score, this was further investigated for each sub-scale (representing the factors derived from the PCA).
Results
Sample
The BD group consisted of 276 patients with BD (62% female) and 228 healthy controls (51% female). Cases and controls showed significantly different gender distributions (p = 0.02), but mean age at interview was not significantly different (44.13 ± 12.2 vs 41.83 ± 12; p = 0.08). The clinical characteristics of BD cases are shown in Table 1.
Clinical characteristics of cases with bipolar disorder (BD).
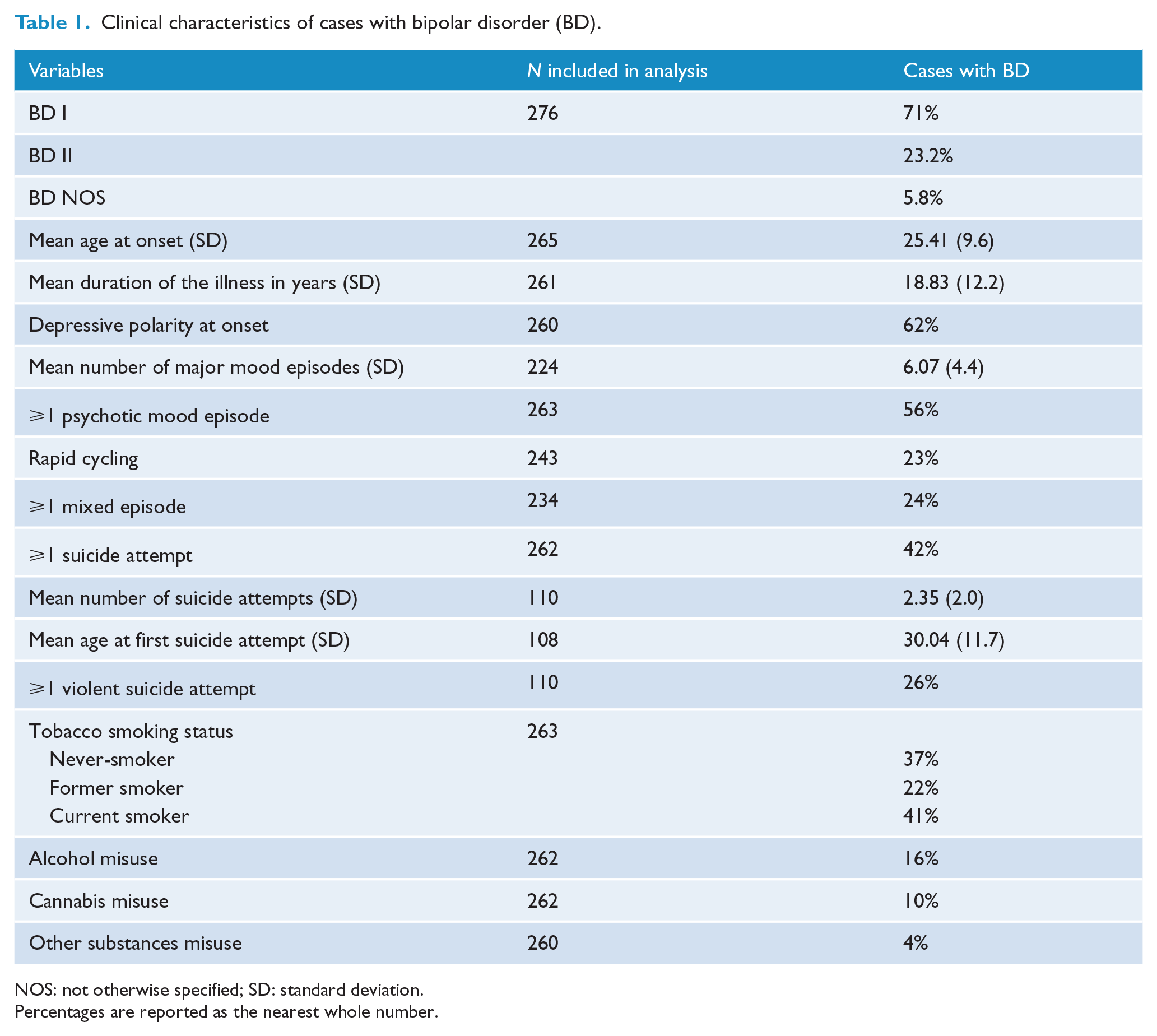
NOS: not otherwise specified; SD: standard deviation.
Percentages are reported as the nearest whole number.
Factor analysis
We established that PCA was an appropriate procedure (KMO equal to 0.93 and Bartlett’s test p < 10−6). Using both the PA and Cattell’s Scree Test, three factors were extracted, accounting for 52% of the variance. Items and PCA factor loadings in the whole sample are presented in Table 2.
Principal Component Analysis in the sample of cases and controls.
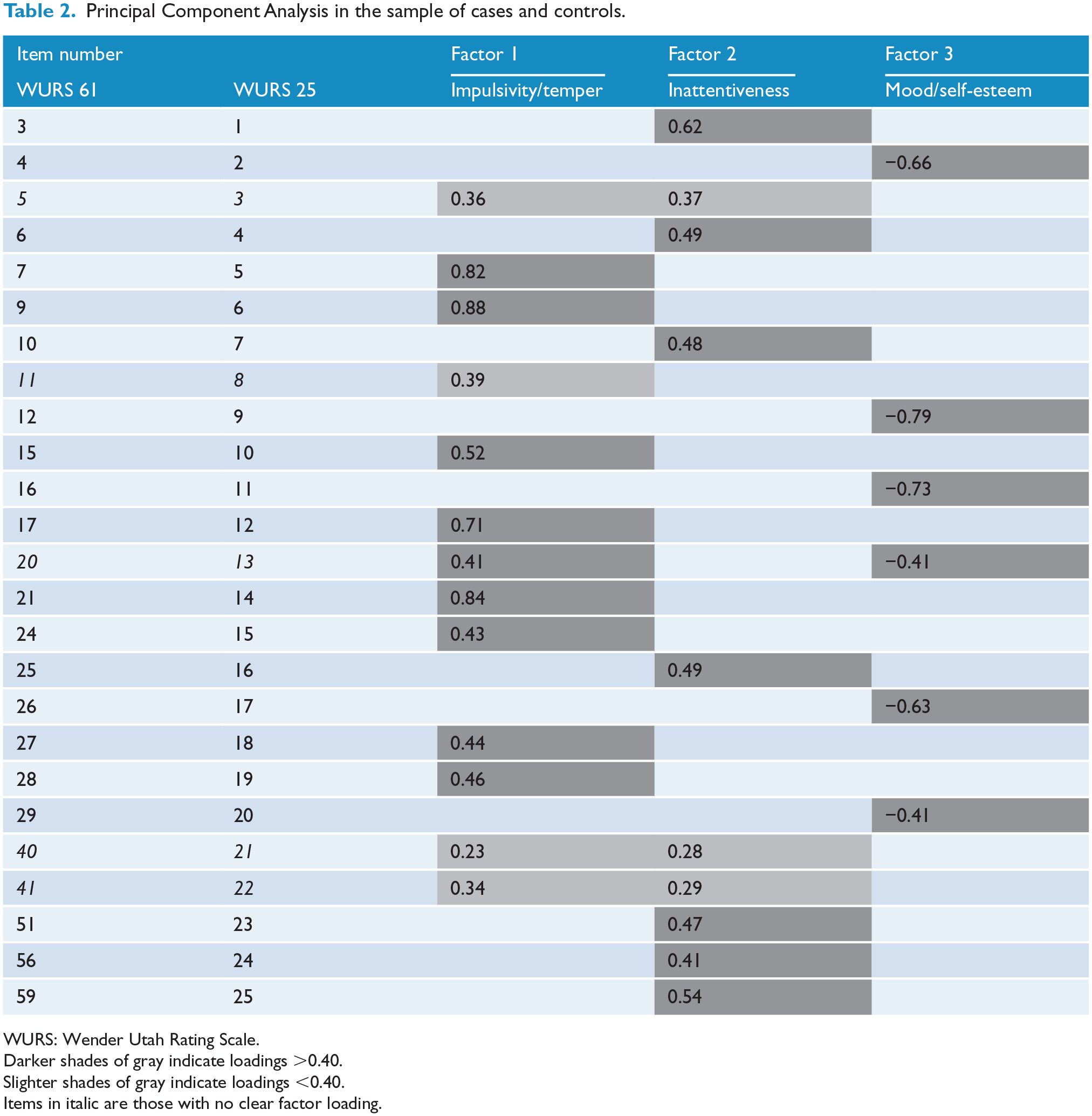
WURS: Wender Utah Rating Scale.
Darker shades of gray indicate loadings >0.40.
Slighter shades of gray indicate loadings <0.40.
Items in italic are those with no clear factor loading.
Factor 1 was labeled ‘impulsivity/temper’ and explained 37% of the variance. It included 11 items such as ‘having temper outburst, tantrums’ or ‘being hot tempered, low boiling point’. Factor 2 was labeled ‘inattentiveness’ and explained 8% of the variance. It contained 9 items such as ‘having concentration problems, easily distracted’ or ‘did not achieve up to potential’. Factor 3 was labeled ‘mood/self-esteem’ and explained about 7% of the variance, and the 5 items included ‘feeling sad or blue, depressed, unhappy’ or ‘having low opinion of myself’. Four items had loadings <0.40 (items 3, 8, 21, 22) and were allocated as noted in the methods. Item 13 (‘moody, ups and downs’) had equal loadings on two factors, so it was classified with the ‘impulsivity/temper’ factor as this was where it loaded in a previous study (Caci et al., 2010).
Case–control comparisons
As shown in Table 3, cases and controls were significantly different for all WURS scores. Furthermore, 22.5% of BD cases versus 5.3% of controls were classified as WURS positive (OR = 5.21; 95% CI = [2.73, 9.95]; p < 0.0001).
WURS scores in cases with bipolar disorder (BD) and healthy controls.
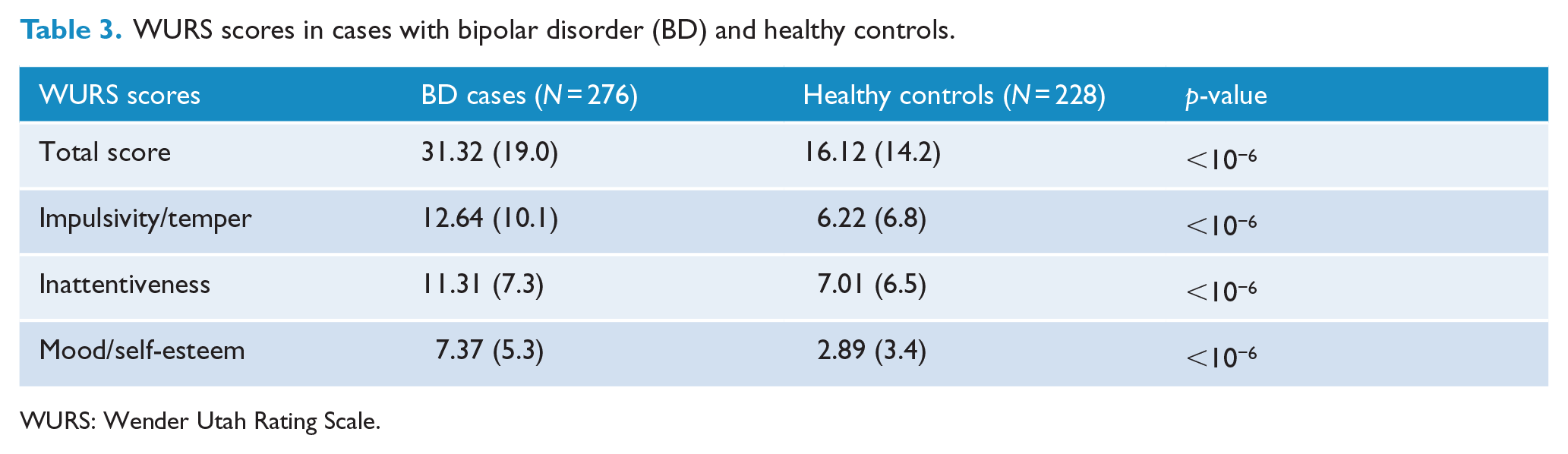
WURS: Wender Utah Rating Scale.
Linear regression showed that the differences between cases and controls remained significant when controlling for age and gender (see Table 4).
WURS scores in cases with bipolar disorder (BD) and healthy controls adjusted for gender and age at interview.
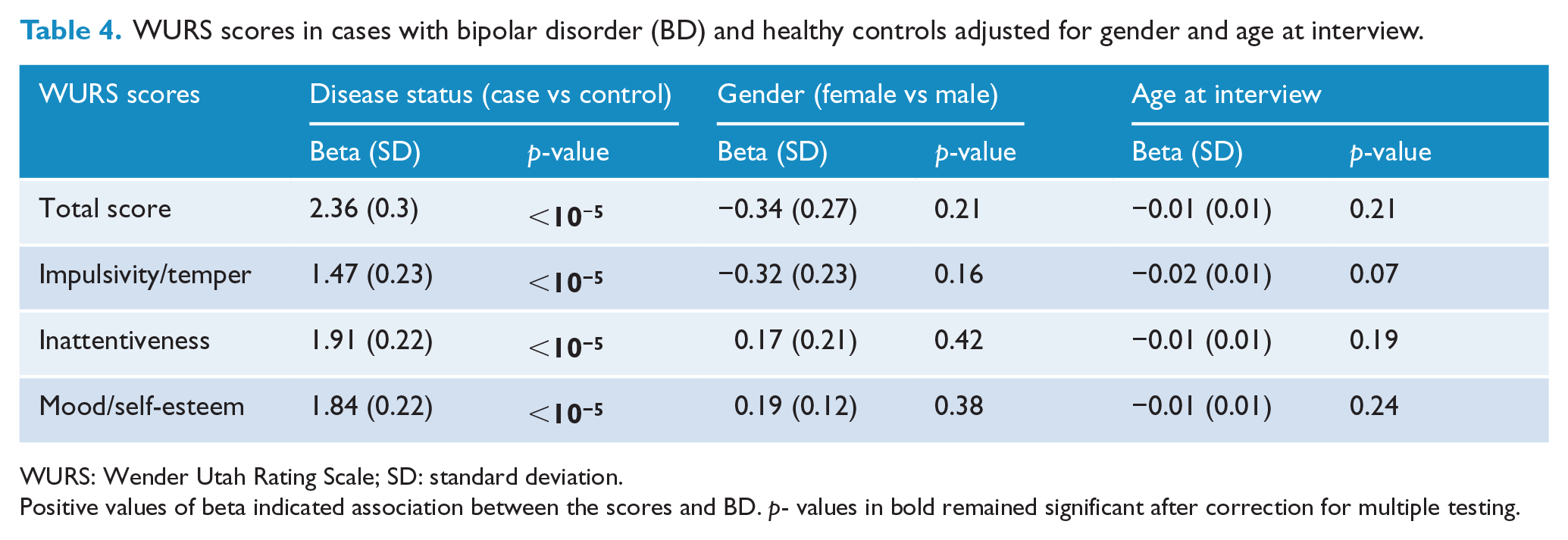
WURS: Wender Utah Rating Scale; SD: standard deviation.
Positive values of beta indicated association between the scores and BD. p- values in bold remained significant after correction for multiple testing.
Associations between WURS scores and clinical characteristics of BD
An earlier age at onset of BD was significantly correlated with a higher WURS total score (r = −0.23; p < 10−4). A ‘positive WURS’ was associated with early onset (onset before 22 years old) (32% vs 15% for later onset, OR = 2.70, 95% CI = [1.49, 4.89], p = 0.001).
A ‘positive WURS’ was also associated with alcohol misuse (38% vs 20% for no alcohol misuse, OR = 2.46, 95% CI = [1.22, 4.98], p = 0.01) and cannabis misuse (44% vs 20% for no cannabis misuse, OR = 3.01, 95% CI = [1.29, 7.05], p = 0.01).
An association was found between WURS total score and the composite scores for increasing severity of substance use (Figure 1) and for suicidal behaviors (Figure 2).
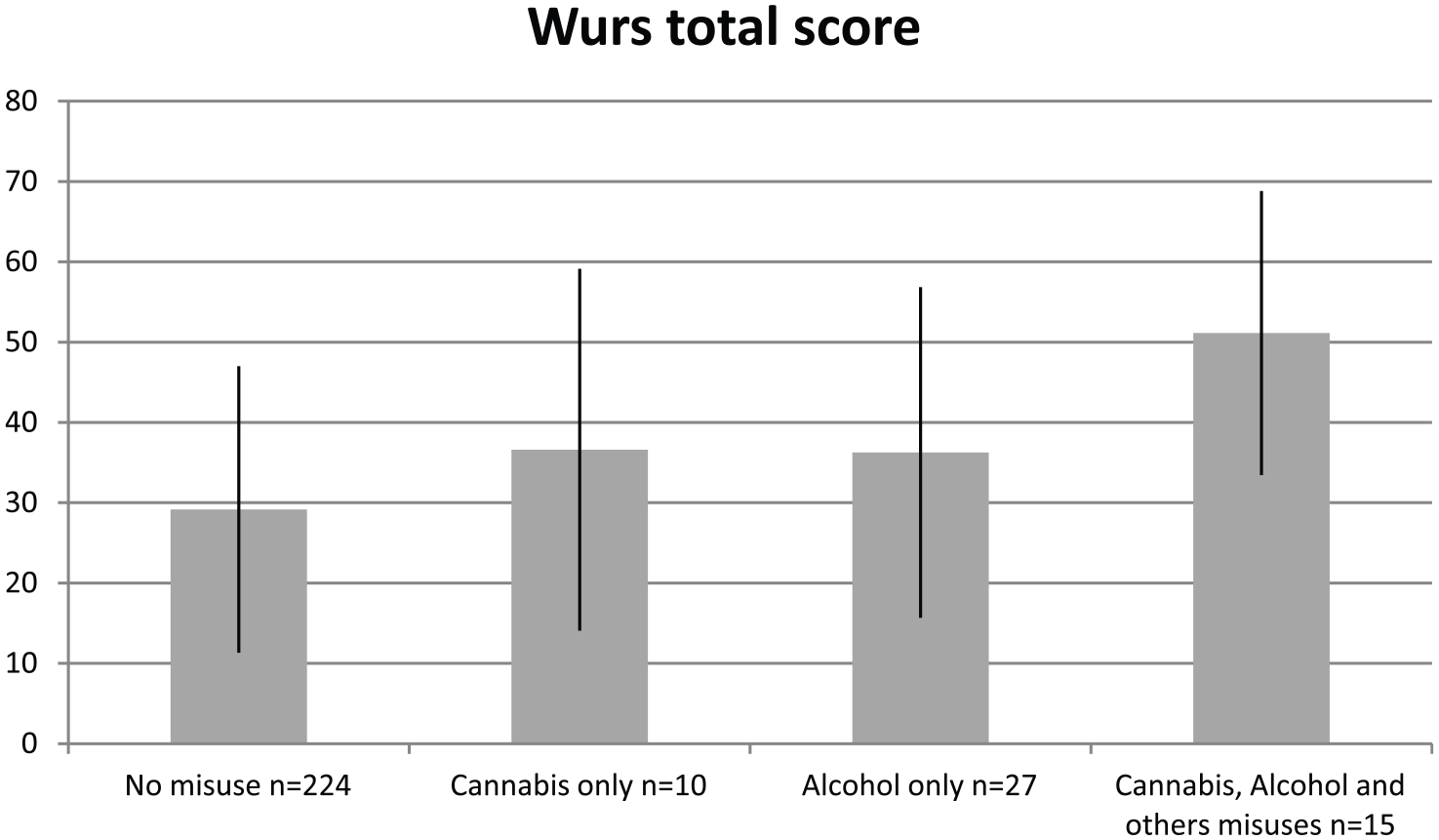
WURS total score as a function of substance misuses.
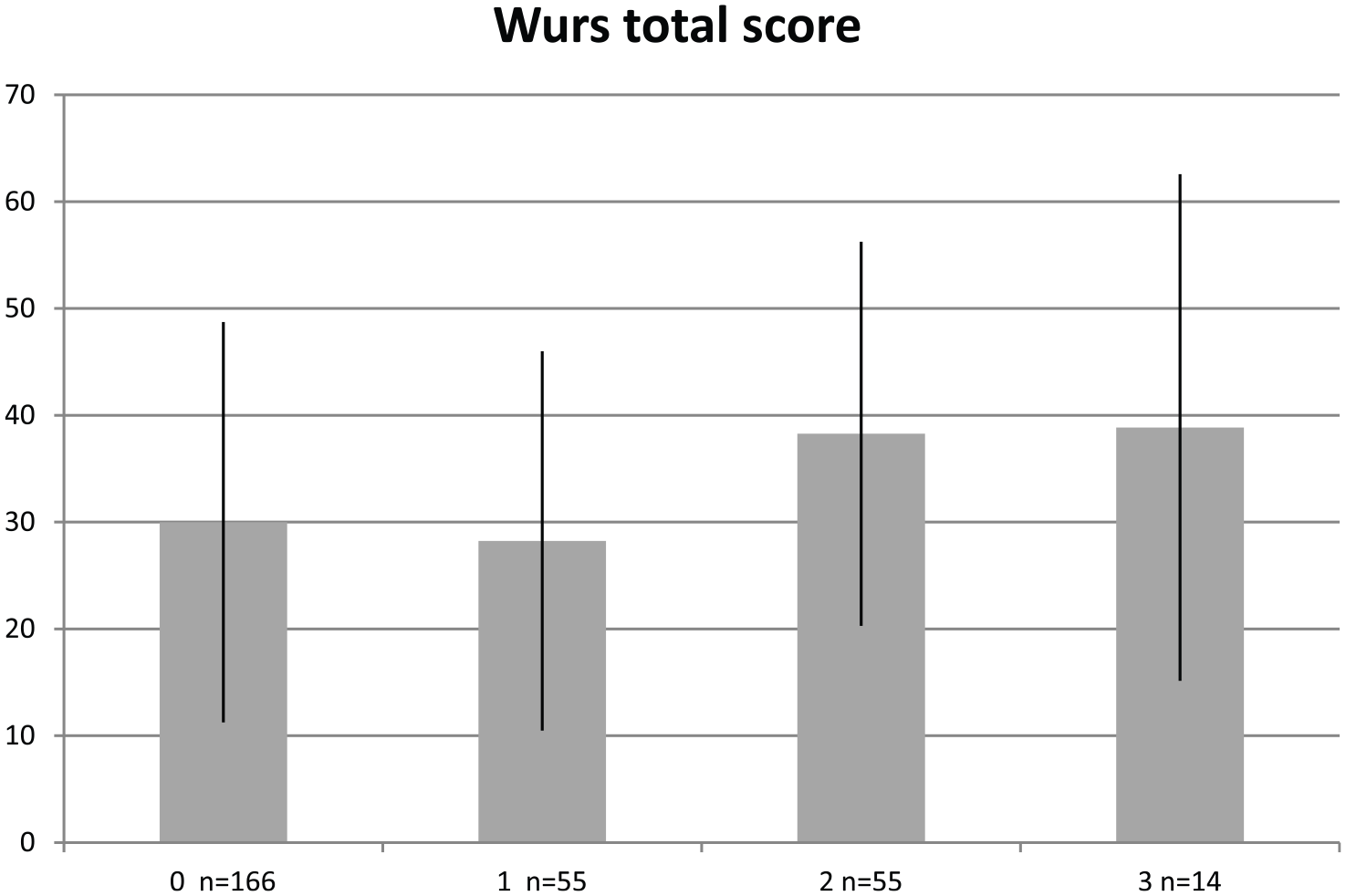
WURS total score as a function of severity of suicidal behaviors.
No differences for WURS total score were observed for cases classified according to BD subtype (p = 0.65), polarity at onset (p = 0.46), lifetime history of psychotic symptoms during mood episodes (p = 0.77) or rapid cycling (p = 0.99).
Multivariate analysis
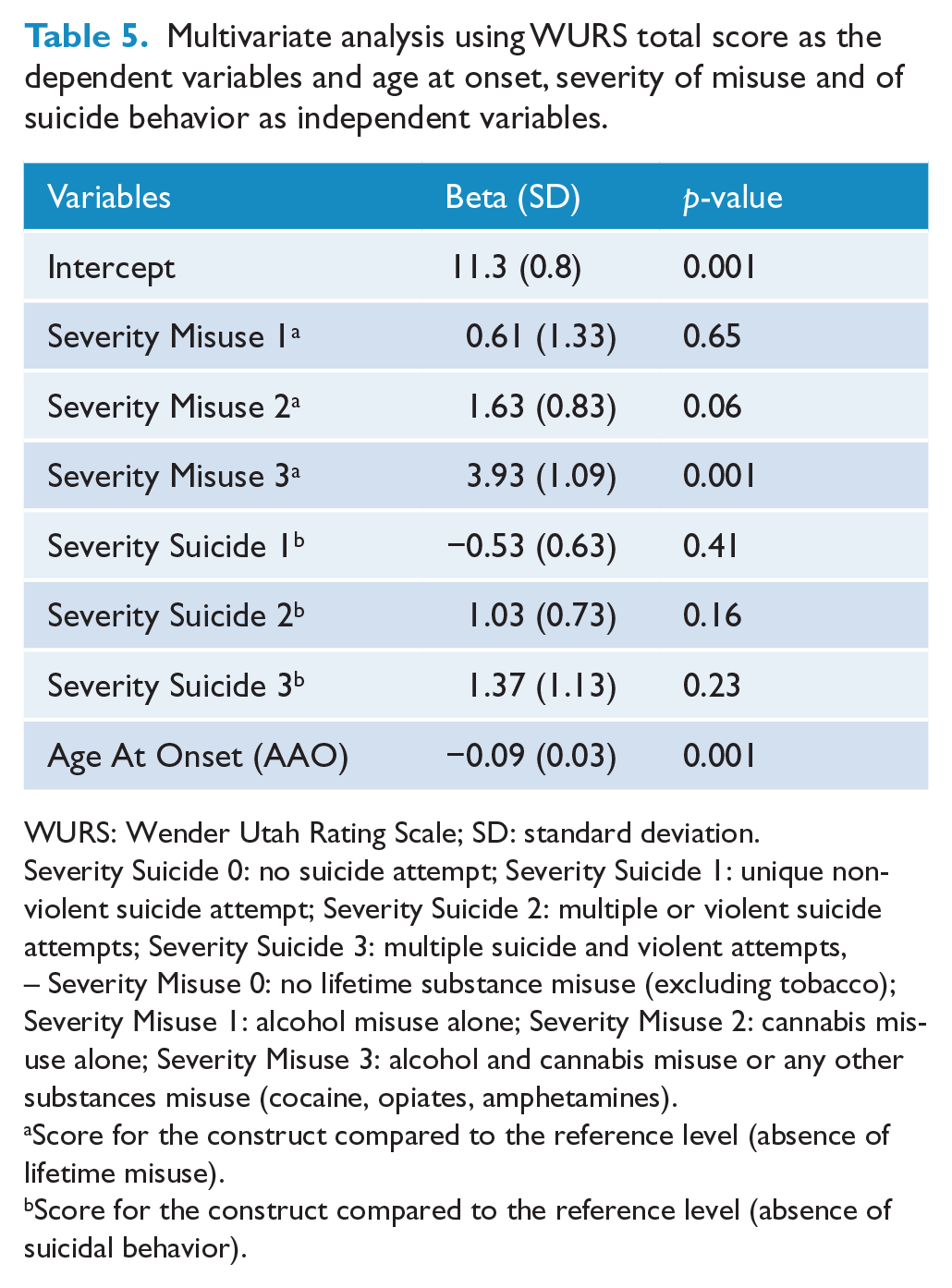
As shown in Table 5, linear regression analysis (controlling for potential confounders) confirmed significant associations between WURS total score, earlier age at onset of BD and higher severity of alcohol and substance misuse, but did not find a significant association with severity of suicidal behaviors.
Multivariate analysis using WURS total score as the dependent variables and age at onset, severity of misuse and of suicide behavior as independent variables.
WURS: Wender Utah Rating Scale; SD: standard deviation.
Severity Suicide 0: no suicide attempt; Severity Suicide 1: unique non-violent suicide attempt; Severity Suicide 2: multiple or violent suicide attempts; Severity Suicide 3: multiple suicide and violent attempts, – Severity Misuse 0: no lifetime substance misuse (excluding tobacco); Severity Misuse 1: alcohol misuse alone; Severity Misuse 2: cannabis misuse alone; Severity Misuse 3: alcohol and cannabis misuse or any other substances misuse (cocaine, opiates, amphetamines).
Score for the construct compared to the reference level (absence of lifetime misuse).
Score for the construct compared to the reference level (absence of suicidal behavior).
Scores for the three factors (derived from the PCA) identified significant associations between age at onset, severity of misuse and the Impulsivity/Temper, Inattentiveness and Mood/Self-esteem sub-scales (all p-values ⩽ 0.003), but again there was no association between any of these factors and the composite measure of suicidal behaviors (data not shown).
Discussion
We confirmed the factorial structure of the French version of the 25-item WURS in a sample of euthymic BD cases and healthy controls. The three factors identified (Impulsivity/Temper, Inattentiveness and Mood/Self-esteem) replicated the structure previously described in a French validation study (Caci et al., 2010) and that reported in studies of patients with other mood disorders (Greenwood et al., 2013; Joo et al., 2012). Adult BD cases differed significantly from healthy controls for the WURS total score and the three factor scores. A greater magnitude of childhood ADHD features was associated with more evidence of clinical severity and complexity of BD including an earlier age at onset and comorbid alcohol and substance misuse (mainly cannabis), but only a trend for a greater array of suicidal behaviors. In addition to discussing these findings, it is worthwhile highlighting some of the issues that complicate the measurement of ADHD symptoms in BD (and vice versa).
First, it is notable that the design of our study does not allow us to determine the sensitivity or specificity of the WURS as a tool to detect ADHD caseness in our BD sample or the healthy controls. We did not include a structured interview to ascertain a formal diagnosis of ADHD. This limitation arose mainly because the version of the DIGS that is validated for use in French does not include a section of the diagnosis of ADHD (unlike later versions of the DIGS). We note that about 20% of WURS scores exceeded the arbitrary cut-off score (total >46) used to identify probable caseness, so some or all of these individuals may have true ADHD comorbidity. Having said that, screening tools such as the WURS can generate a substantial rate of false positives in clinical samples (as high as 75% in some studies) (Suhr et al., 2009), and the positive predictive values of the WURS are only around 45% among alcohol dependent patients (Daigre et al., 2015), around 35% in individuals seeking treatment for substance use disorders (Dakwar et al., 2012) and about the same in patients with BD (Oncu et al., 2005). Screening for adult ADHD in BD samples gives rise to similar issues, and about 40% of the individuals who score positively on the adult self-rating scale (ASRS-v1.1) do not meet ADHD caseness criteria (Edebol et al., 2012; McCann and Roy-Byrne, 2004; Perroud et al., 2014; Torres et al., 2015). However, we were primarily interested in considering dimensions of ADHD and potential symptom clusters, not simply studying presentations that exceeded diagnostic thresholds. To this end, several authors have thus proposed that the WURS rather is actually measuring clinical manifestations of externalizing behaviors or other symptoms that are far from specific to ADHD (Suhr et al., 2009).
An alternative view of our approach is that we have used the WURS as a multi-dimensional measure to capture aspects of the complex clinical phenomenology and overlapping features of BD and ADHD. This overlap typically includes impulsivity and inattention and also emotional lability, and all these dimensions are represented in the factorial structure of the WURS scale. It has been highlighted that ADHD manifestations in childhood also include an emotional component (mood swings and emotional lability), and Shaw et al. (2014) report that emotion dysregulation is found in up to 50% of children with ADHD. The clinical overlap between ADHD and bipolar mania includes irritable mood, poor concentration, increased motor activity and features that can also be observed in certain subtypes of bipolar depression. Indeed, the clinical manifestations assessed in the WURS belong to different psychological domains such as impulsivity, temper, inattention, unstable mood, low self-esteem and anxiety. As such, the conclusion in favor of any one position over another (i.e. the WURS demonstrates the co-occurrence of BD and ADHD phenomena and represents true comorbidity or it highlights early manifestations of BD or indicates non-specific psychopathological manifestations of several putative disease trajectories) is far from easy. Our own review of the literature indicated that more than half of individuals who developed BD presented a putative prodrome prior to 14 years of age and that this frequently included a mixture of precursors such as mood lability, depressive episodes, anxiety, sleep disorders, conduct problems, attention and concentration impairments, altered energy patterns and/or a family history of mania or depression (Geoffroy et al., 2015; Leopold et al., 2012).
The validation study of the WURS (Ward et al., 1993) selected the 25 items that showed the greatest mean difference between subjects with ADHD and healthy controls. However, in addition to externalizing behaviors, the items included (anxiety, worry, inattention, daydreaming, sleep problems, stubborn behavior, poor concentration) bear a striking resemblance to the prodromal signs identified in longitudinal studies of high-risk offspring of BD parents (Duffy, 2010; Duffy et al., 2010; Egeland et al., 2012) and other risk syndromes (Scott et al., 2013). A review of prospective studies exploring clinical risk factors for BD found evidence for at least two heterotypic trajectories, one characterized by prodromal anxiety symptoms and the other by high impulsivity, aggression, externalizing behaviors and mixed dysphoric features (Faedda et al., 2014). As such, high WURS scores may simply reflect heterotypia in the developmental trajectory of BD and such findings should encourage clinicians to explore not only problems related to ‘early mood deregulation’ but also a larger range of (non-)specific precursors that may be markers of future morbidity independent of the specific late-stage syndrome (Hickie et al., 2013).
The utility of the research assessment we have undertaken is that it demonstrates an association between high scores on the WURS and specific aspects of a more severe, complex, BD phenotype characterized by an earlier age at onset and an increased lifetime severity of suicidal attempts and substance misuse. The association between higher WURS and earlier onset of BD could represent higher levels of true ADHD comorbidity in the early-onset BD sub-group (since 32% of those with early onset vs 15% of those with later onset have a positive WURS), and there is corroborating evidence for such a finding in the literature. For example, Greenwood et al. (2013) reported a negative correlation between age of onset and all WURS scores except for inattention. The bidirectional and robust comorbidity between pediatric BD type I and ADHD has been well documented in pediatric and adult studies in both clinical and epidemiological samples (Biederman et al., 2013). In the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) cohort of adults, the overall lifetime prevalence of ADHD was about 10% and patients with BD and comorbid ADHD reported the onset of their mood disorder about 5 years earlier than other cases (Nierenberg et al., 2005). Also, the bidirectional association between pediatric BD and ADHD has been documented in clinical and epidemiological samples (Biederman et al., 2013) and ADHD is reported to be a significant risk factor for switching from unipolar to BD in youth (Biederman et al., 2009; Chen et al., 2015). However, the evidence does not suggest the association between the WURS ratings, and an earlier age is due to misdiagnosis of ADHD and juvenile mania in our sample. It is notable that the earliest age at onset in our sample is 14 years old, corresponding to the often-noted lack of pre-pubertal mania in European clinical populations (Douglas and Scott, 2014; James et al., 2014). Furthermore, it is unlikely that mood swings or emotion lability dramatically accounts for the differences observed between groups in our study (as this factor accounts for only 7% variance in the WURS total score). The largest proportion of the variance was explained by the impulsivity/temper factor.
We have previously reported evidence linking impulsivity to alcohol and substance misuse in BD (Etain et al., 2013) and to dimensions of hostility/impulsivity to suicidal behaviors (Parmentier et al., 2012). Two meta-analyses have demonstrated that children with ADHD were more likely to develop disorders of abuse/dependence for nicotine, alcohol, marijuana, cocaine and other substances (Charach et al., 2011; Lee et al., 2011). The use of the WURS might shed light on how trans-diagnostic symptoms may accelerate or exaggerate disorder-related phenomena such as age at onset or patterns of risky or self-harming behaviors. The clinical implication is to systematically screen patients with BD for this early component to identify those who might be at risk for such high-risk behaviors.
This study has several methodological limitations. As noted, using the WURS to retrospectively measure childhood ADHD features is the main weakness, and recall biases and cognitive deficits may further confound the assessment. Responses could also be biased by residual mood symptoms although our sample has been assessed during a period of euthymia. We used no external validation of the self-assessment made by individuals. We used the WURS as an indicator of ADHD during childhood but provided no formal diagnosis for childhood or adulthood persistent ADHD. Therefore, our study was not an attempt to assess a retrospective diagnosis of ADHD. Finally, the cut-off of 46 that we used to define WURS-positive cases is not universally accepted as the optimal cut-off score (Suhr et al., 2009). We also did not provide any adult ADHD assessment to study the continuity between ADHD symptoms from childhood to adulthood. Although this is one of the larger studies on this topic, false negative findings could have emerged such as the reduced magnitude in association with suicidal behaviors (after controlling for other variables).
Conclusion
We found that ADHD features were common in adults with BD, with 22% of cases versus 5% of controls having a positive WURS score. The presence of ADHD features in childhood was associated with early onset, suicidal behavior and substance misuse. Both the total WURS score and scores on the three factor sub-scales (Impulsivity/Temper, Inattentiveness and Mood/Self-esteem) were linked with early onset and substance misuse. Further clinical studies of BD cases and individuals at high risk of developing BD will enable better understanding of how ADHD features fit into a neurodevelopmental model of BD and whether the features predict a specific illness trajectory or represent an epiphenomena (such as overlapping clinical features). Additional research would also be useful to delineate how the WURS can be integrated into assessment packages of ‘risk constellations’ for adults with complex BD presentations (Leopold et al., 2012). The systematic investigation of ADHD features (and a possible diagnosis of childhood ADHD) especially in those with an early-onset BD and evidence of substance misuse or suicidal behaviors could help treatment planning and modify outcomes. Indeed, some recommendations have been proposed for the management of patients with mood disorders and comorbid ADHD in national clinical guidelines (Bond et al., 2012).
Footnotes
Acknowledgements
We thank the patients and controls for participating in this study. We thank E Abadie, and JR Richard for their assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Institut National de la Santé et de la Recherche Médicale (INSERM), Assistance Publique des Hôpitaux de Paris and Fondation FondaMental.