
Abstract
Objective:
To describe the rates and trends of emergency department presentations and calls to a state poisons centre for antidepressant overdose.
Methods:
A retrospective cohort study utilising the Victorian Emergency Minimum Dataset and Victorian Poisons Information Centre call registry between January 2009 and December 2018 was conducted. This captured all presentations to Victorian emergency departments and calls to the Victorian Poisons Information Centre. Any intentional overdose involving an antidepressant was included. Annual rates of emergency department presentations and calls per 100,000 persons and 100,000 prescriptions for antidepressants overall and individual antidepressant classes, in addition to age-group-specific rates, were reported.
Results:
A total of 3650 presentations to emergency department and 7096 calls to the poisons centre were included. No changes were seen in overall emergency department presentation rates when controlled for population or prescription numbers, but large and significant increases were seen for younger age groups. The 10–14- and 15–19-year age groups had average annual increases of 13.1% (95% CI = [6.5%, 19.7%], p < 0.001) and 7.2% (95% CI = [2.8%, 11.5%], p < 0.001) per 100,000 persons, respectively. Increases were seen in overall annual call rates of 6.7% (95% CI = [5.2%, 8.1%], p < 0.001) per 100,000 persons and 7.5% (95% CI = [4.9%, 10.1%], p < 0.001) per 100,000 prescriptions.
Conclusion:
Overall, emergency department presentation rates remained stable during the study period. Overall poisons centre call rates increased moderately. However, when examining younger persons, large increases were seen in both emergency department presentations and poison centre call rates. These findings highlight the need for future interventions to mitigate against intentional overdose in younger populations.
Introduction
Mental and behavioural conditions are an increasing problem for Australians with self-reported rates of illness doubling from 10% in 2001 to 20% in 2018 (Australian Bureau of Statistics [ABS], 2019). Of note, just over half report depression as their primary issue. A variety of treatments can be employed to manage depression, ranging from lifestyle change, psychotherapy to pharmacological therapies. Unfortunately, these pharmacological therapies can be used as a means of self-harm and some low-level evidence suggests their use can itself increase rates of self-harm (Hetrick et al., 2021). With increasing numbers of Australians diagnosed with depression, it is unknown if this has been associated with an increase in intentional overdose with antidepressant medications.
Presentations to an emergency department (ED) for intentional overdose represent a significant proportion of the visits related to a mental health issue, constituting 12% of the total (Alarcon Manchego et al., 2015). In addition, these presentations often result in admission to hospital and long lengths of stay (Perera et al., 2018). A previous study described antidepressant overdose in Australia between 1998 and 2008 (Wong et al., 2010). Overall, rates of presentations to ED and calls to a state poisons centre were shown to be decreasing when controlling for population and prescription numbers. No subsequent studies have examined this topic and considering the increase in rates of depression it is unclear if rates of overdose have continued to decrease in the past decade.
Describing these trends will inform prescribers as to how changes in prescription rates may impact overdose rates. In addition, it can provide regulators with insight as to whether changes to prescribing guidelines may be needed to decrease intentional overdoses. This study aimed to describe the rates and trends of intentional overdose involving antidepressants in Victoria, Australia over a 10-year period between 2009 and 2018.
Methods
Study design
We conducted a retrospective cohort study using two clinical registries, the Victorian Emergency Minimum Dataset (VEMD) and the Victorian Poisons Information Centre (VPIC) dataset, including data from the 2009 to 2018 calendar years. Ethics approval was granted by the Austin Health Human Research Ethics Committee.
Setting
The study was conducted in Victoria, Australia. Victoria has a population of 5.9 million and all 39 hospitals with a 24-hour ED contribute to the VEMD. The state referral centre for poisonings (VPIC) is located at The Austin Hospital in Melbourne. The VPIC provides a phone consultation service for any poisonings in the state (Victorian Poisons Information Centre, 2018).
Data sources
Victorian Emergency Minimum Dataset
The VEMD is an administrative dataset for presentations to EDs in Victoria, of which 39 contributed throughout the study period. Data collected included the date/time of the ED presentation, basic patient demographics, as well as the presentation diagnosis and outcome. All presentations due to an injury or poisoning have a free-text narrative section providing further details of the event. Data are entered by trained coders or clinical staff at each study hospital, with the Victorian Department of Health undertaking regular quality control. There were no major changes in the data reporting methods during the study period. Data were provided by the Victorian Injury Surveillance Unit at Monash University.
VPIC dataset
The VPIC dataset is a registry of all phone calls made to the VPIC. This is the only phone consultation service for poisoning in Victoria. Data collected included the date/time of the phone call, the demographics of the patient the call is regarding, as well as the agents involved in the poisoning and the outcome of the call. Data are entered by the call-takers who are predominantly pharmacists with expertise in toxicology. As with the VEMD, there were no major changes in data reporting methods during the study period.
State prescription numbers and population
Data for the estimated annual population of Victoria (2009–2018) were obtained from the Australian Bureau of Statistics (ABS, 2020). Data for the number of dispensed prescriptions for antidepressants each year in Victoria were obtained from the Pharmaceutical Benefits Scheme section of the Australian Government Department of Health website (Services Australia, 2022). This resource provides the number of Pharmaceutical Benefits Scheme (PBS) items processed by Services Australia by date of processing (year), state and item. Both data sources are publicly available.
Antidepressant drugs
The list of antidepressant drugs used for this study were obtained by searching for agents approved for the treatment of depression in Australia on the Australian Pharmaceutical Benefits Scheme website (Services Australia, 2022). The included classes were: selective serotonin reuptake inhibitors (SSRIs), serotonin noradrenaline reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), mono-amine oxidase inhibitors (MAOIs), noradrenaline reuptake inhibitors (NARI) and atypical antidepressants. Supplement 1 includes a full list of all included drugs.
Inclusion criteria
To derive the cohort of phone calls to the VPIC all calls between 1 January 2009 and 31 December 2018 were eligible for inclusion. Only phone calls pertaining to an intentional overdose aimed at causing self-harm that involved at least one antidepressant were included. Recalls regarding the same incident were excluded. Any calls made from outside Victoria were excluded.
To derive the cohort for presentation to ED all presentations between 1 January 2009 and 31 December 2018 were eligible for inclusion. Presentations for antidepressant overdose were selected in the VEMD using the free-text field, International Classification of Diseases, 10th revision, Australian modification (ICD-10-AM) diagnosis codes, and the cause of injury field. Only overdoses that were both intentional and done as a means of self-harm were included. Each included case was manually examined to confirm the presentation was related to antidepressant overdose. A description of the selection method and terms searched for is provided in Supplement 2. Manual text search is required as ICD10-AM diagnosis codes relating to antidepressant poisoning are limited within the VEMD. The only code available for use is T43.0 (poisoning by tricyclic and tetracyclic antidepressants). Other ICD10-AM codes related to antidepressant poisoning are used in admissions data but not available in the VEMD. The method used has been shown to be successful when identifying terms relating to other drugs, such as opioids in the VEMD (Lam et al., 2020, 2022).
Outcomes
The two primary outcomes were the number of calls to the VPIC and number of presentations to Victorian EDs for intentional overdose involving an antidepressant during the study period controlled for population or prescription numbers. Each outcome was further reported for specific drug classes and age groups where possible. Due to differences in reporting the age groups differed between the datasets.
Statistical analysis
Baseline characteristics of each cohort are all reported as frequencies with percentages. Rates per 100,000 population and 100,000 prescriptions were calculated by dividing the number of calls or presentations in a year by the population at the time or total prescriptions dispensed in the same year. For the VEMD cohort, the MAOI class data were not provided to the researchers due to low annual numbers. Trends in calls and presentations were assessed using negative binomial regression. Poisson regression was initially used but the data were over dispersed, making this method inappropriate. The outcome was the count of presentations or calls, the predictor used was year as a continuous outcome, the offset used was population or prescriptions for the relevant year.
A p-value of < 0.05 was considered significant. All analysis was conducted using the R Project for Statistical Computing Software Version 1.3.959.
Results
Cohort derivation
During the study period, VPIC received 396,899 calls, of these 15,720 (4.0%) were related to antidepressants. Over a half (n = 9910, 63.0%) of these were intentional overdoses. After recalls regarding the same overdose and calls from outside of Victoria were excluded, the final VPIC cohort included 7096 calls. During the study period, there were 3,795,453 presentations to Victorian EDs for injuries, including poisonings. Of these 5415 involved an antidepressant poisoning and in 3650 (67.4%) of these cases the poisoning was an intentional overdose. Figure 1 describes both inclusion processes.
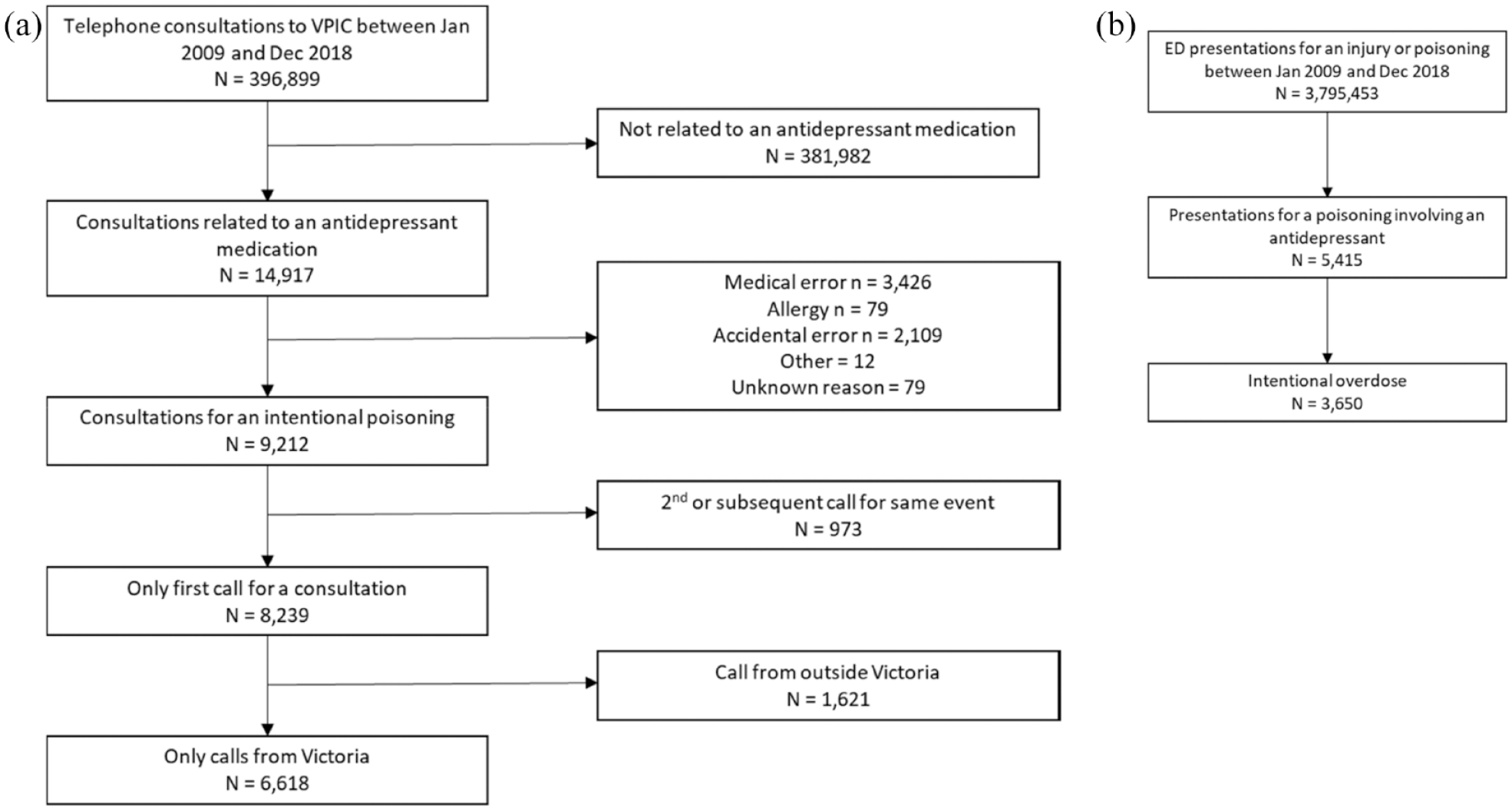
Inclusion and exclusion process for (a) VPIC dataset and (b) VEMD dataset.
Cohort characteristics
Patients in the VPIC cohort were predominantly adults (⩾ 18 years) (4347, 61.3%) and female (4936, 69.6%). The person making the call was most commonly a doctor (4169, 59.0%) followed by any other health care worker (1481, 20.7%). Calls were primarily made from hospitals (4697, 66.2%). More than half (3805, 54.0%) of the calls were for an overdose that involved an SSRI and approximately one in four calls involved an SNRI (1858, 26%).
Similar to the VPIC cohort, most patients presenting to ED were adults (2634, 72.1%) and females (2668, 73.1%). Over half of the ED presentations resulted in an admission to hospital (1896, 51.9%). Presentations most frequently involved an SSRI (1865, 51.1%), followed by SNRIs (908, 24.9%). Table 1 describes the characteristics of both cohorts.
Characteristics of the VPIC and VEMD cohorts.
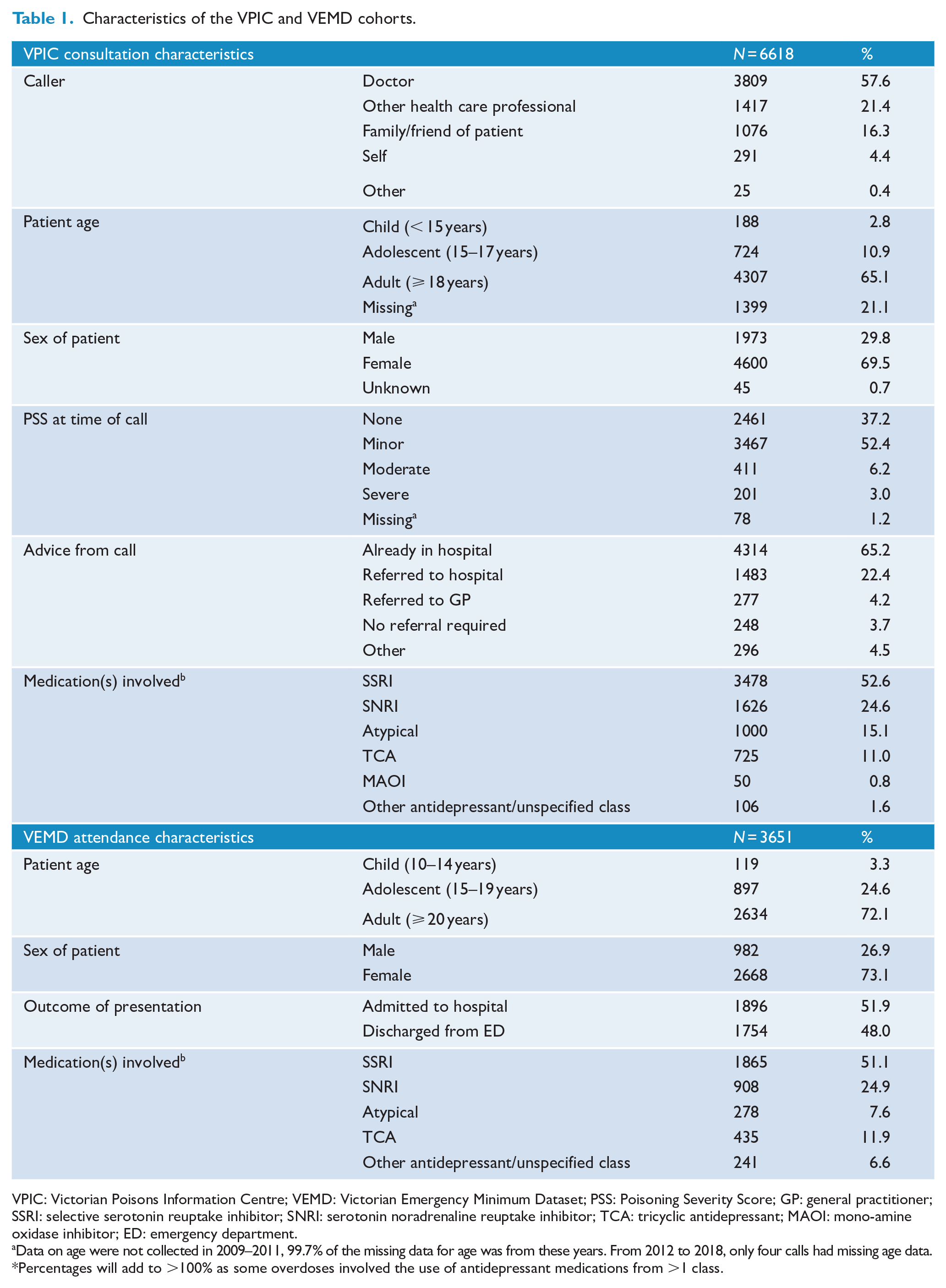
VPIC: Victorian Poisons Information Centre; VEMD: Victorian Emergency Minimum Dataset; PSS: Poisoning Severity Score; GP: general practitioner; SSRI: selective serotonin reuptake inhibitor; SNRI: serotonin noradrenaline reuptake inhibitor; TCA: tricyclic antidepressant; MAOI: mono-amine oxidase inhibitor; ED: emergency department.
Data on age were not collected in 2009–2011, 99.7% of the missing data for age was from these years. From 2012 to 2018, only four calls had missing age data.
Percentages will add to >100% as some overdoses involved the use of antidepressant medications from >1 class.
Trends in calls to VPIC and presentations to ED
Overall, the annual rate of calls per 100,000 population for antidepressant overdose increased significantly during the study period from 8.2 in 2009 to 15.2 in 2018, with an average annual increase of 6.7% (95% CI = [5.2%, 8.1%], p < 0.001). When rates were calculated per 100,000 prescriptions there was an increase from 13.7 in 2009 to 27.3 in 2018, with a higher average annual increase of 7.5% (95% CI = [4.9%, 10.1%], p < 0.001). Significant increases in call rates for all antidepressant classes when controlling for either population or total prescription numbers were observed. The largest increase was seen for SNRIs, with an average annual increase of 10.3% (p = 0.004) per 100,000 people and 12.8% (p < 0.001) per 100,000 prescriptions. Figures 2 and 4 describe these results further. Overall, the proportion of overdoses that resulted in an admission to hospital was lower form SSRIs than TCAs (62% vs 44%, p < 0.001).
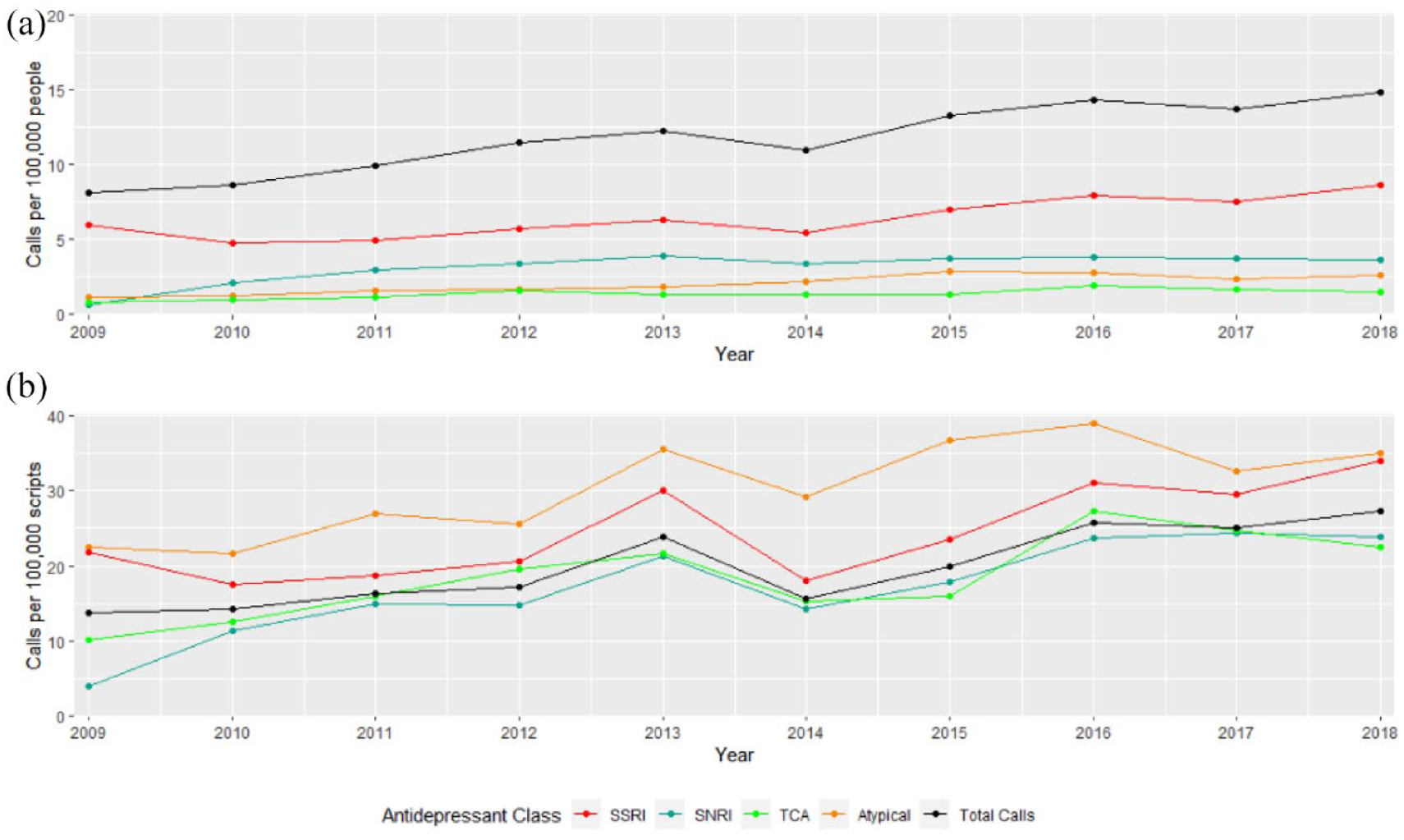
Annual telephone consultation rates to VPIC (2009–2018) (a) per 100,000 people and (b) per 100,000 dispensed prescriptions.
There was no significant change in ED presentations per 100,000 people or per 100,000 prescriptions for antidepressants overall during the study period. An average annual increase in presentations per 100,000 population for SSRIs was seen of 2.3% (p = 0.004). A decrease was seen for TCAs by population and prescription numbers with average annual decreases of 5.8% (p = 0.001) and 5.1%, respectively (p = 0.003). Figures 3 and 4 describe these results further.
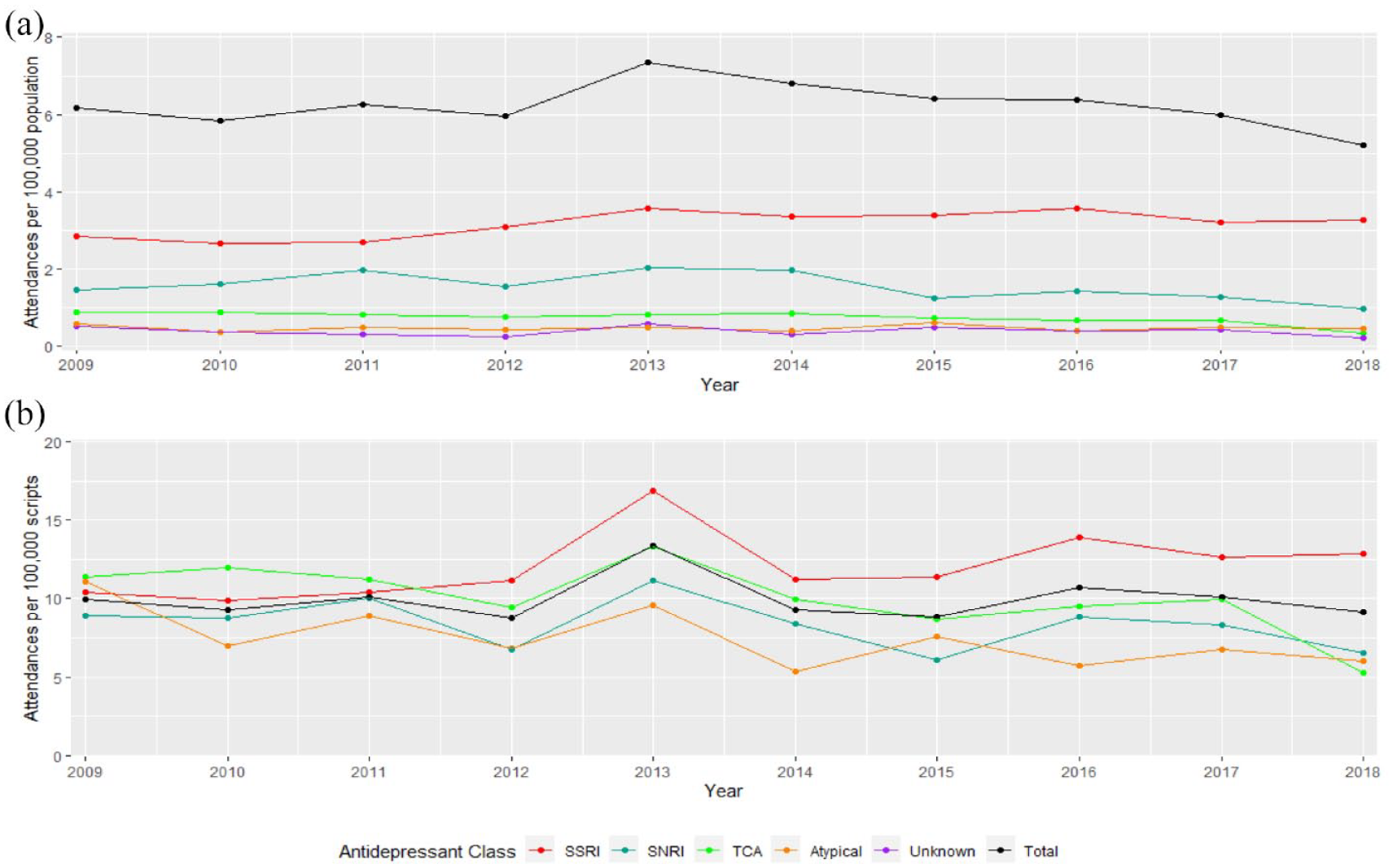
Annual rates of presentation to a Victorian ED (2009–2018) (a) per 100,000 population and (b) per 100,000 dispensed prescriptions.
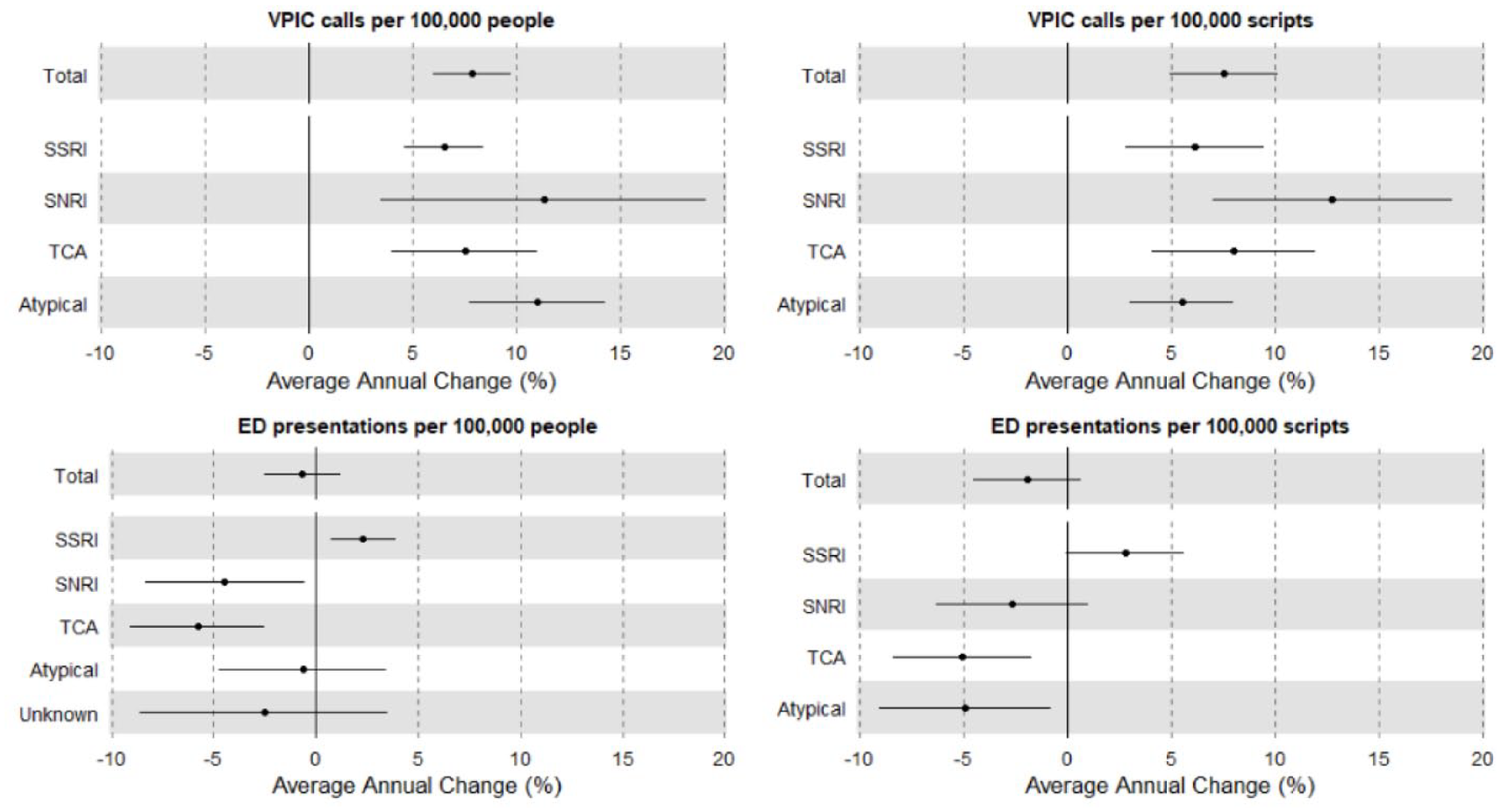
Average annual change in VPIC telephone consultations and ED presentations.
Trends in calls to VPIC and presentations to ED by age groups
There were significant increases seen in annual call rates across all age groups. The largest increase was seen for the 0–14-year group with an average annual increase per 100,000 persons of 18.1% (p < 0.001). It should be noted that this age group had relatively low annual call numbers (range = 13–52). The 15–19- and > 19-year groups had lower average annual increases per 100,000 persons of 5.1% and 3.9%, respectively (p < 0.001 and p = 0.008). Figure 5 describes these results further.
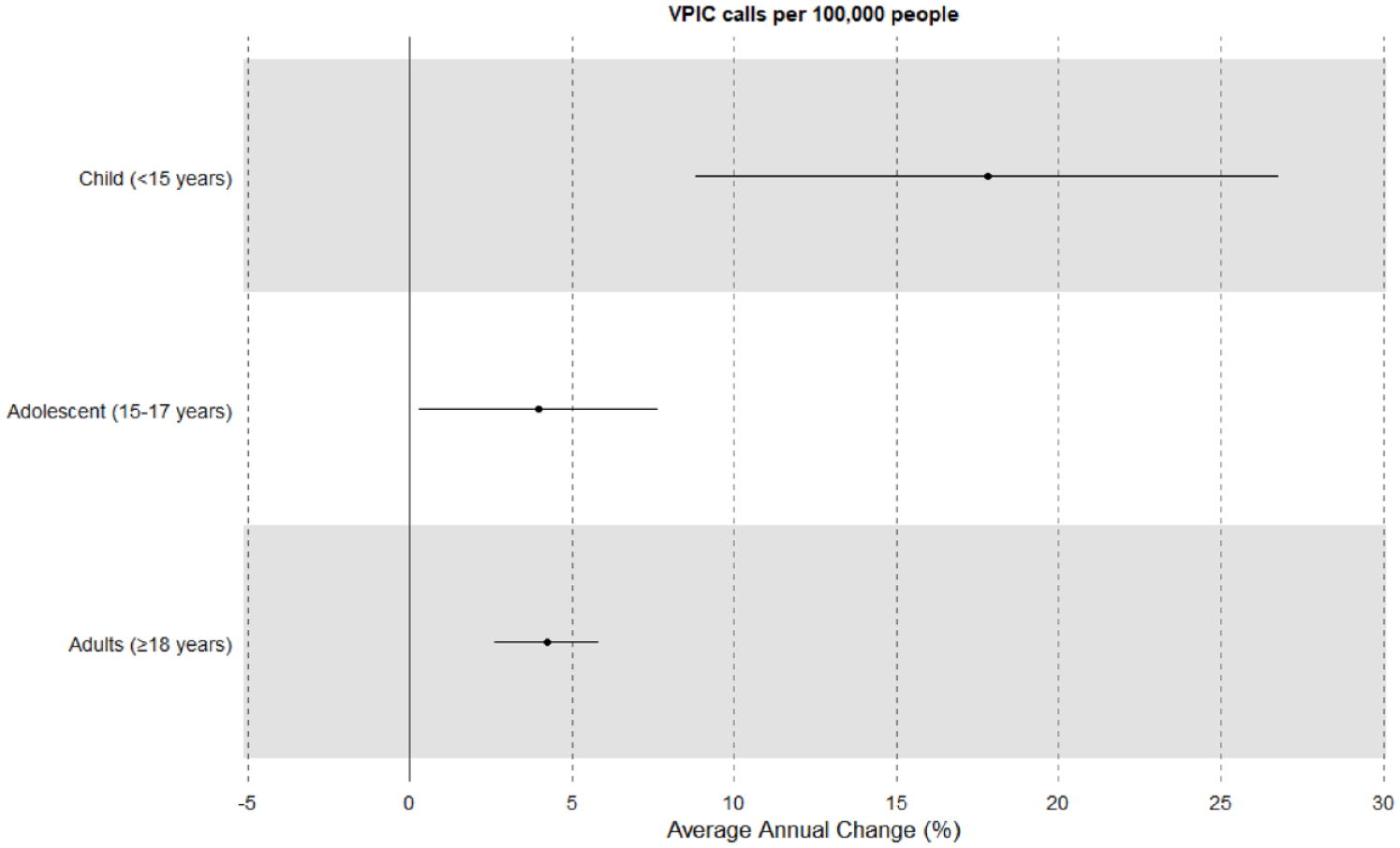
Average annual change in VPIC telephone consultations per 100,000 people by age group.
There were large and significant changes in the age distribution of those presenting to ED. In 2009, the 10–14- and 15–19-year age groups together represented 10.6% of presentations, in 2018, this had approximately tripled to 29.7%. The two groups had average annual increases in presentations per 100,000 population of 13.1% (p < 0.001) and 7.2% (p = 0.001), respectively. Decreases in call rates over the study period were seen for adult patients, particularly the middle age groups. Figure 6 describes these results further.
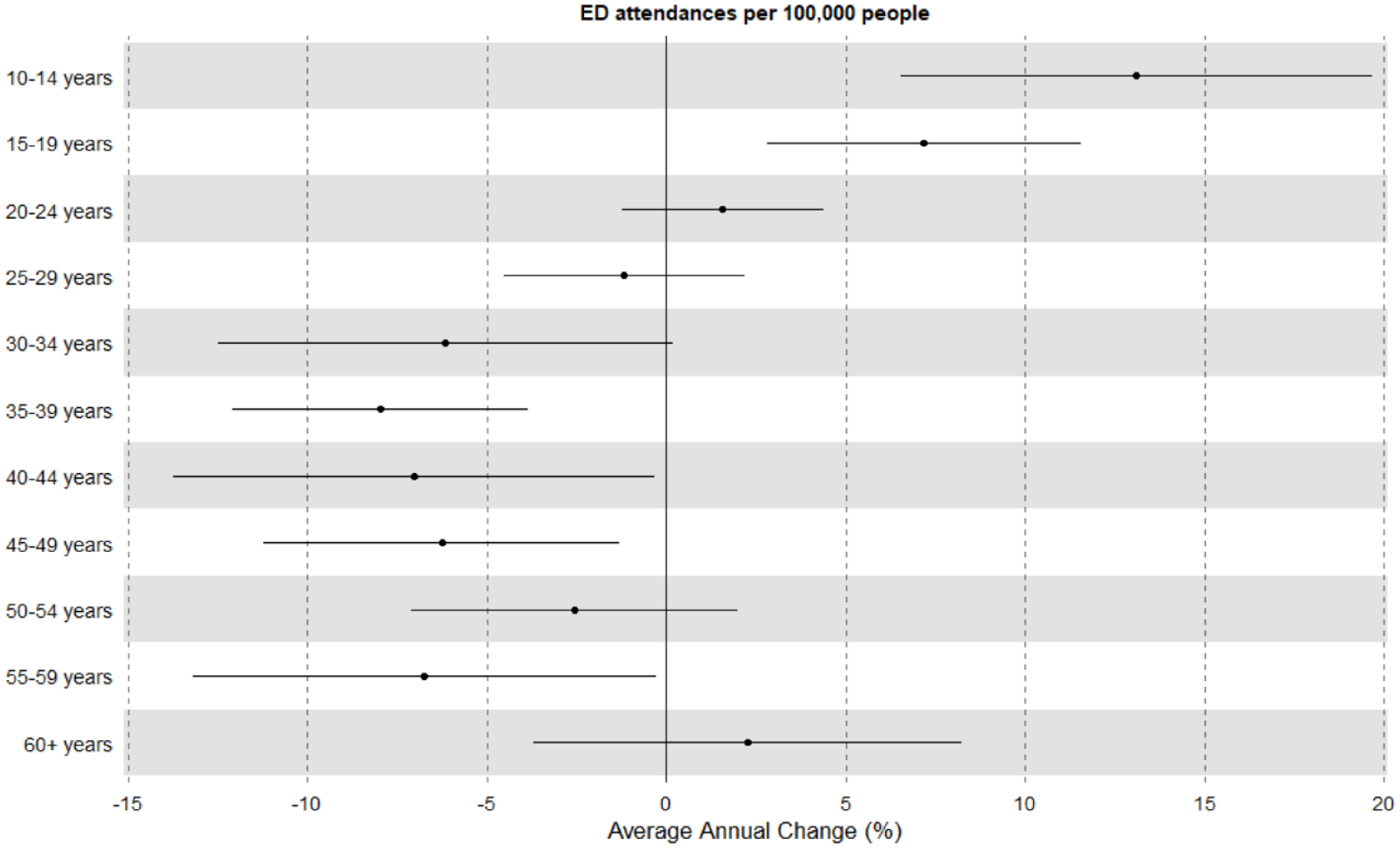
Average annual change in ED presentations per 100,000 people by age group.
Discussion
Overview
In this study, we identified an increase in the overall rate of calls to a state poisons centre and no change in the overall rate of presentations to EDs for intentional antidepressant overdose from 2009 to 2018. However, large increases were seen in ED presentation rates for antidepressant poisoning in persons aged 10–19 years, and in calls to the state poisons centre for intentional self-poisonings using antidepressants in this cohort. Such increases are concerning, and further research is required to understand the underlying drivers of these changes.
Increases in the rate of ED presentation for mental health issues and specifically, intentional overdose, have been described in Australia and worldwide in recent years, particularly in young persons (Hawton et al., 2010; Hiscock et al., 2018; Perera et al., 2018). A study of presentations to all EDs in New South Wales, Australia from 2010 to 2014 found the number of presentations for intentional overdose more than doubled in the 10–19-year age group, findings consistent with our study (Perera et al., 2018). Such increases may be secondary to an overall increase in the total number of individuals in the 10–19-year age group prescribed an antidepressant medication. Alternatively, increases in the number of overdoses as a fraction of total prescriptions may have contributed. Previous work examining antidepressant prescribing trends in young Australians have identified increases, particularly for SSRIs, from 1990 to 2001 in the 15–24-year age group and from 2012 to 2016 in the 5–19-year age group (Cairns et al., 2019; Hall et al., 2003). In addition, large increases in prescribing rates in English and Scottish youth have been reported in recent years (Henderson et al., 2021; Jack et al., 2020). Whether these results can be directly extrapolated to the current Australian context is unknown, however, it is clear that increases were noted in Australia and similar Western nations in recent years.
Changes in the classes of antidepressant used in overdoses were also identified, namely, decreases in TCA involvement and an increase in SSRI involvement for the overall cohort, independent of population change and prescription number changes. Similar changes have been noted elsewhere in Australia (Buckley et al., 2015). Fortunately, these changes may result in a decrease in mortality and need for hospitalisation due to the lower toxicity of SSRI relative to TCAs (Hawton et al., 2010; White et al., 2008). To support this, a further analysis of ED presentation data in our study found a lower rate of hospital admission for overdoses involving SSRIs than TCAs. Increases in the frequency of reported SSRIs overdose necessitate appropriate training of health care workers in managing these presentations. In addition, clinicians must maintain expertise in managing TCA overdose presentations, despite such presentations becoming less frequent.
Beyond a clear need to investigate the driving factors behind these changes, there are some immediate implications worth consideration. First, any strategies to lessen observed increases in total numbers of overdoses must been done with care as deprescribing of antidepressants in the younger cohort may lead to unintended increased mental health morbidity (Hosenbocus and Chahal, 2011). With that said, equal care must be taken with the initial decision to prescribe antidepressants to young persons due to possible adverse effects. Education regarding appropriate prescribing may help to mitigate against the trends observed in this study (Bondar et al., 2020). Second, education should be directed to front-line clinicians regarding the identification and management of toxidromes secondary to antidepressant overdose in line with current use patterns, while considering the possibility for decreased familiarity with less frequently used drug classes.
A large unknown is what impact controlling for any change in the number of prescriptions made to young people will have on the rate of ED presentation. It may be that the increase is concordant with an increase in prescriptions made to young persons, but examining this hypothesis was beyond the scope of this study. This presents an important opportunity for future research that will allow more targeted measures to be made to prevent further increases. In addition to this further exploration of sub-group specific trends (e.g.: gender, rural/remote/metropolitan status), analysis of data from more recent years and from other Australian states will show if the increases extend to other groups, is representative nationally, and has continued beyond the timeframe utilised in this study. Finally, ICD10-AM codes for newer classes of antidepressant are lacking, updates should look to include these as specific codes to facilitate future research.
The results of this study must be considered in the context of its strengths and weaknesses. We were able to capture all ED presentations in Victoria using a state-wide registry. This ensured our sample was less prone to selection bias. Limiting this was the method used to identify ED presentations for inclusion. We required the narrative field to mention an antidepressant and the intent field to state the overdose was intentional self-harm. It is unclear what number of presentations were unintentionally excluded because of incorrect completion of narrative field free text or intent field. However, previous work has found the VEMD to have a relatively high rate of accuracy when compared to patient interviews, particularly for overdoses (Stokes et al., 2000). It must also be considered that the VEMD only reports on ED presentations. It is unknown what number of patients attend their General Practitioner or are reviewed by paramedics without transport to an ED. The use of two datasets added depth to the study, but it should be noted that an ED presentation could have also been associated with a poisons centre call, resulting in dataset duplication. In addition, calls to VPIC are not a reflection of overdose incidence. To appear in the dataset, a phone call to the centre must be made, the threshold for which may vary based on patient age, overdose severity and caller characteristics. Further to this, all poison’s centres across Australia participate in an after-hours on-call roster. Therefore, if Victoria is not the elected after-hours centre a caller from Victoria will not appear in the VPIC dataset. Another strength of the study was the length of the inclusion period, which facilitated the identification of any temporal trends. However, due to the timing of data release from the VEMD, we were unable to report on data from more recent years, therefore it is unknown if the trends have continued since 2018, particularly in the context of the COVID-19 pandemic. Furthermore, it could not be determined whether the patient obtained the medication via a personal prescription or through other means. It is also possible that patients from outside of Victoria travelled to a Victorian ED to receive care. Furthermore, prescription data for specific age groups were not publicly available for the study period, preventing any analysis of age-group-specific trends that controlled for a change in the number of prescriptions. Finally, the data source used to collect prescription numbers only includes instances where the PBS assisted with the cost of a medication. When this was not the case (i.e. cost of drug less than the PBS benefit) the dispensing would not appear in the dataset. Therefore, prescription numbers reported were likely an underestimate.
Conclusion
In this study of intentional antidepressant overdose in the state of Victoria, Australia, we identified an increase in the rate of calls to the state poisons centre between 2009 and 2018, particularly in younger age groups. While there was no change in overall presentation rates to EDs for antidepressant overdose, significant increases were seen in presentations by young persons. These findings suggest future interventions should particularly target young persons to mitigate associated harms.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221098636 – Supplemental material for Trends in calls to a state poisons centre and presentation to emergency departments for intentional antidepressant overdose in Victoria, Australia
Supplemental material, sj-docx-1-anp-10.1177_00048674221098636 for Trends in calls to a state poisons centre and presentation to emergency departments for intentional antidepressant overdose in Victoria, Australia by Zakary Doherty, Anselm Wong, Jane Hayman and Shaun Greene in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to acknowledge the Victorian Department of Health as the source of VEMD data for this study. Furthermore, they wish to acknowledge the Victorian Poisons Information Centre for the VPIC data used.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.