
Abstract
Depression is a common condition worldwide and medication has, traditionally, been the mainstay of therapy. Presently, a wide variety of antidepressants are available including the tricyclics (TCAs), monoamine oxidase inhibitors (MAOIs), selective serotonin reuptake inhibitors (SSRIs) and ‘other’ newer antidepressants (mianserin, venlafaxine and mirtazapine).
Drugs employed for the management of depression are frequently toxic in overdose (OD). TCAs have been in use since the second half of the twentieth century and the first adverse effects were reported two years after their clinical usefulness was recognized in 1959 [1]. SSRIs were introduced to Europe in 1983 and have since increased in use worldwide [2].
Antidepressant OD is the fifth greatest cause of mortality by substance in the USA and accounted for 7.6% of all ODs in 2006 [3]. The SSRIs appear to be safer OD. In 2006, there were 42,190 OD exposures to SSRIs with three deaths compared to 10,412 OD exposures to TCAs and 13 deaths. Also, hospital costs for patients with SSRI compared to TCA OD are lower due to shorter hospital stays and fewer ICU admissions [4–5]. This is related to the increased toxicity of TCA compared to SSRIs and MAOIs [6].
There is evidence of increasing antidepressant drug use in Australia [7]. Anecdotally, the nature of emergency department (ED) presentations and poison information centre calls have changed over time. This is particularly evident with regard to the type of antidepressant drug taken and is thought to reflect the prescribing patterns in the community. However, the epidemiology of antidepressant OD in Australia is poorly defined.
This study aimed to determine the epidemiology of antidepressant drug OD in Victoria by examining data on intentional antidepressant OD from both the Victorian Emergency Minimum Dataset (VEMD) and the Victorian Poisons Information Centre (VPIC). The results will inform a better understanding of OD patterns and toxicity related to the various drug classes. It will also help in understanding the use of resources to treat these cases and subsequent impact on the health system.
Methods
This was a retrospective review of VEMD and VPIC data. Ethics approval was obtained from the Monash University and Austin Health Human Research Ethics Committees, respectively.
Victorian Emergency Minimum Dataset
The Victorian Emergency Minimum Dataset (VEMD) contains anonymous demographic, administrative and clinical data that details presentations to Victorian public hospitals with 24-hour EDs. Submission of data to the VEMD from 18 EDs commenced in October 1995. By April 2005 the number of participating EDs had increased to 38. The Victorian Injury Surveillance Unit (VISU) at the Monash University Accident Research Centre (MUARC) administers a subset of the VEMD comprising cases with an external injury cause, including drug OD.
All VEMD cases, regardless of age, that related to an intentional antidepressant OD over a 10-year period (1998–2007, inclusive) were analysed. The VEMD contains a free-text description of the injury event. Potential cases were identified through an electronic free-text search for antidepressant drug trade and generic names, and the keywords of ‘antidepressant’, ‘SSRI’, ‘tricyclic’ and ‘monoamine’. After this initial search, cases identified were sorted by ‘external cause’ and ‘body region’ and were reviewed manually to exclude non-intentional OD, non-OD, non-human OD and other cases where intentional antidepressant OD was not the main factor.
For each VEMD case that met the study entrance criteria, the following data were extracted: year of presentation, age group, gender, nature of main injury, human intent, activity when injured and departure status.
Victorian Poisons Information Centre (VPIC) database
The Victorian Poisons Information Centre (VPIC) receives calls related to poison exposure in Victoria between 0700 and 2100 daily, after which calls are diverted to the Sydney centre. Approximately 40 000 calls are received per annum. It frequently receives calls for advice regarding antidepressant drug OD. VPIC cases, regardless of age, who had taken an intentional antidepressant drug OD during a 3-year and 4-month period (June 2005–September 2008, inclusive) were analysed. Data prior to this period was collected on a different computer system and thought to be incomplete and less accurate.
Electronic screening on key words was undertaken on the VPIC dataset. The narrative description of the call for each case identified was then accessed. Calls not meeting the entrance criteria were excluded. Electronic preformatted case reports were generated for each case identified. From these, data were transferred manually to the study database.
For each VPIC case meeting the entrance criteria, the following data were extracted: date and time of call, gender, age group (adult, child, elderly), designation of the caller (patient, family, carer, etc.), drug taken, dose, time taken, symptomology and Poisoning Severity Score [8], and advice given. The Poisoning Severity Score is an overall evaluation of the patient at the time of the call, taking into account the most severe clinical features. Patients can be classified into ‘none’ (no symptoms), ‘mild’, ‘moderate’ and ‘severe’ severity groups.
Drugs examined
For the purposes of the study the following, commonly prescribed, antidepressant drug classes were examined: SSRIs (citalopram, fluoxetine, paroxetine, escitalopram, fluvoxamine, sertraline), TCAs (amitriptyline, dothiepin, imipramine, trimipramine, clomipramine, doxepin, nortriptyline), MAOIs (phenelzine, tranylcypromine, moclobemide) and ‘other’ specified drugs (mianserin, venlafaxine, mirtazapine).
Census data for Victoria were obtained from the Australian Bureau of Statistics [9] in order to adjust for population increases over the study period. Antidepressant prescriptions data was obtained from Medicare Australia for the antidepressants listed under the Pharmaceutical Benefits Scheme [10]. Both groups were annual data from 1998 to 2007.
Statistical analyses
A sample size calculation was not undertaken as the number of cases identified was expected to number in the thousands. This sample size, accrued over the lengthy study periods, was expected to closely represent the epidemiology of the issue.
Most data are reported descriptively with 95% confidence intervals fitted around point estimates, e.g. proportions. Proportions were compared using the chi-square test. Differences in rates were calculated using the critical ratio (z) test. EpiCalc (version 1.02) and SPSS statistical software (Version 17.0) was used for all statistical analyses. For all calculations, the level of significance was 0.05.
Results
VEMD data
Overall, 6073 cases were identified during screening and 5467 met the inclusion criteria. Most (71.1%) of the ODs occurred at home. Females accounted for 3758 (68.7%, 95%CI 67.5, 70.0) cases and were over-represented in all age groups. The peak age group was 20–24 years with 817 (14.9%, 95%CI 14.0, 15.9) cases (both sexes combined).
The SSRIs and TCAs accounted for more than one half and approximately one fifth of OD, respectively (Table 1). Sertraline and amitriptyline were the most common SSRI and TCA drugs, accounting for 22.9% and 8.2% of all OD, respectively. Notably, rates of OD/100 000 prescriptions were similar for the SSRI, TCA and ‘other’ drugs but lower for the MAOIs. However, there were no significant differences between these rates (p > 0.05).
Antidepressant drugs taken in overdose (1998–2007) (Victorian Emergency Minimum Dataset data)
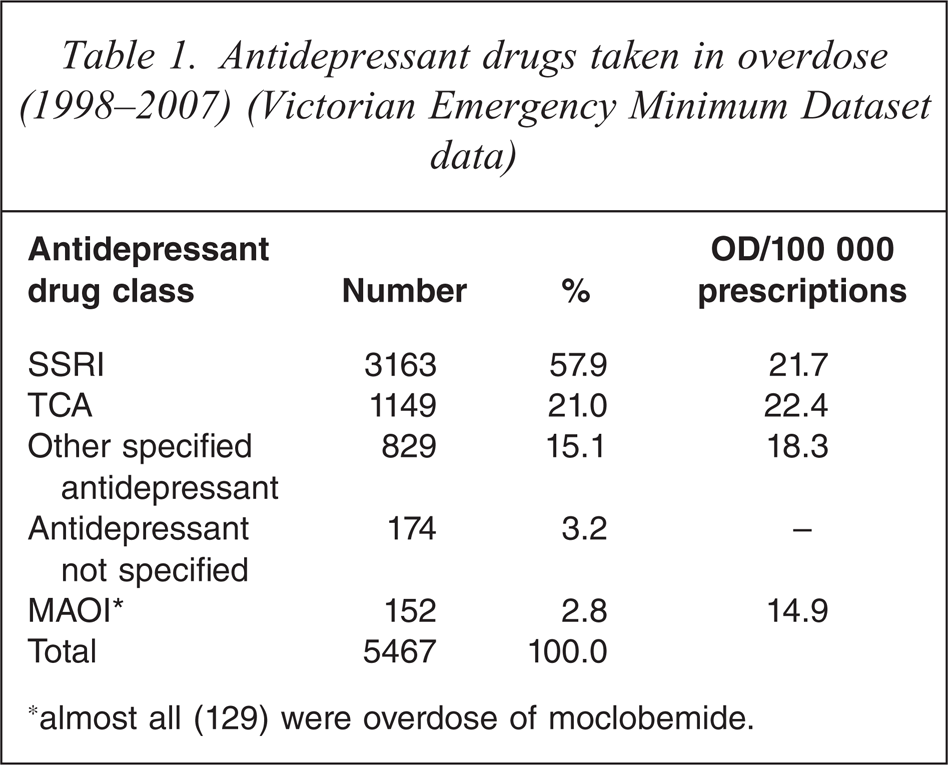
∗almost all (129) were overdose of moclobemide.
OD presentations peaked in 2001 at 759 ODs (14%) (Figure 1). There were 8.8 and 3.8 OD/100 000 population in the SSRI and TCA groups, respectively. Since 2001, OD numbers have trended downwards for all drug groups. In 2007, there were 4.7, 1.5, 1.4 and 0.1 OD/100 000 population in the SSRI, TCA, ‘other’ and MAOI groups, respectively.
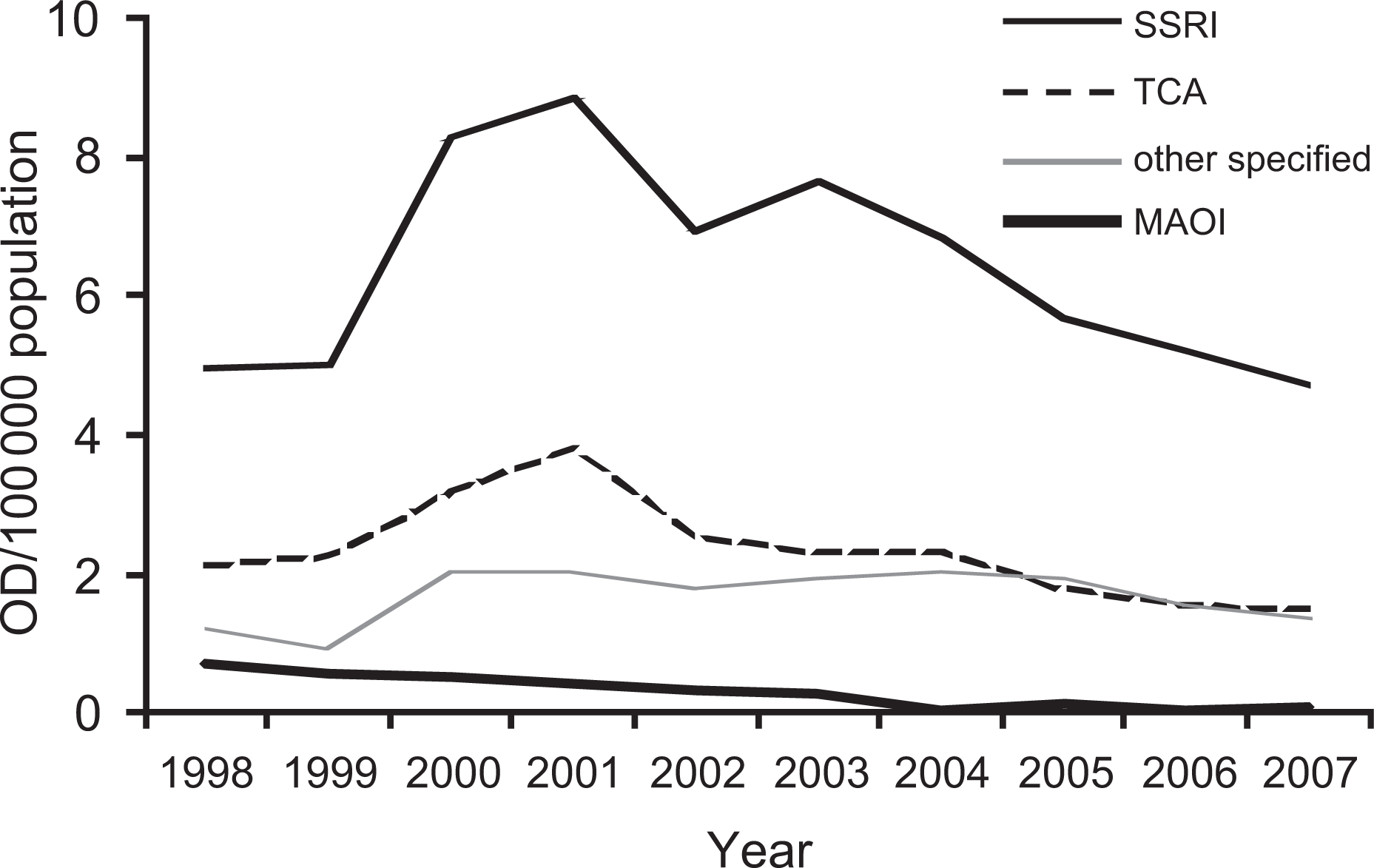
Antidepressant overdose trends with time (Victorian Emergency Minimum Dataset data).
The number of prescriptions filled in Victoria from 1998–2007 rose for the SSRI group (Figure 2) and totalled 14,603,601 scripts over the study period. Prescription rates for the ‘other’ antidepressants also rose. However, rates for TCAs and MAOIs decreased with 5,118,317 and 1,019,101 over the study period, respectively. Overdoses per 100 000 prescriptions trended downwards for all drugs groups over the study period (Figure 3).
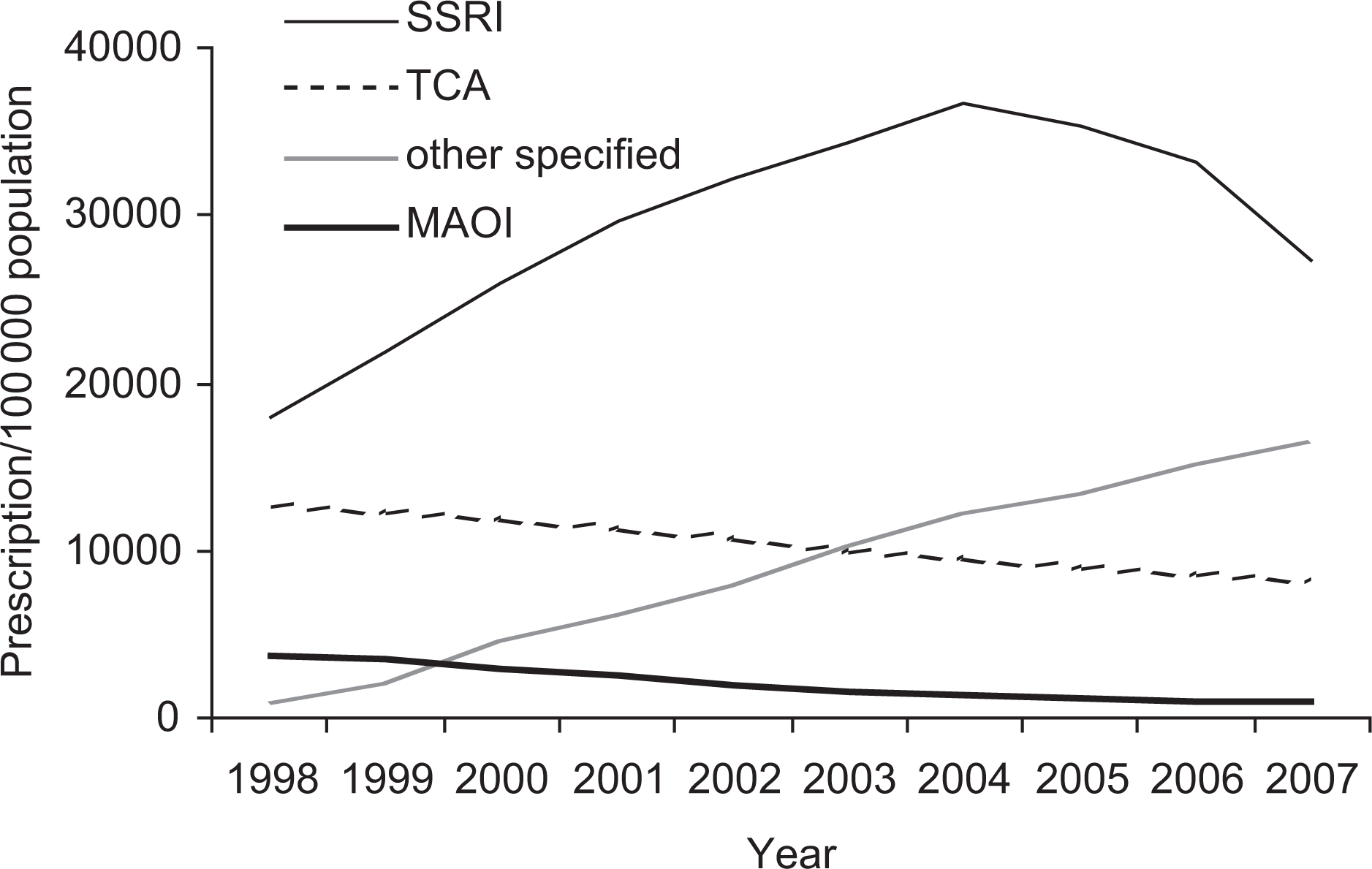
Antidepressant drug prescriptions over time (Pharmaceutical Benefits Scheme data).
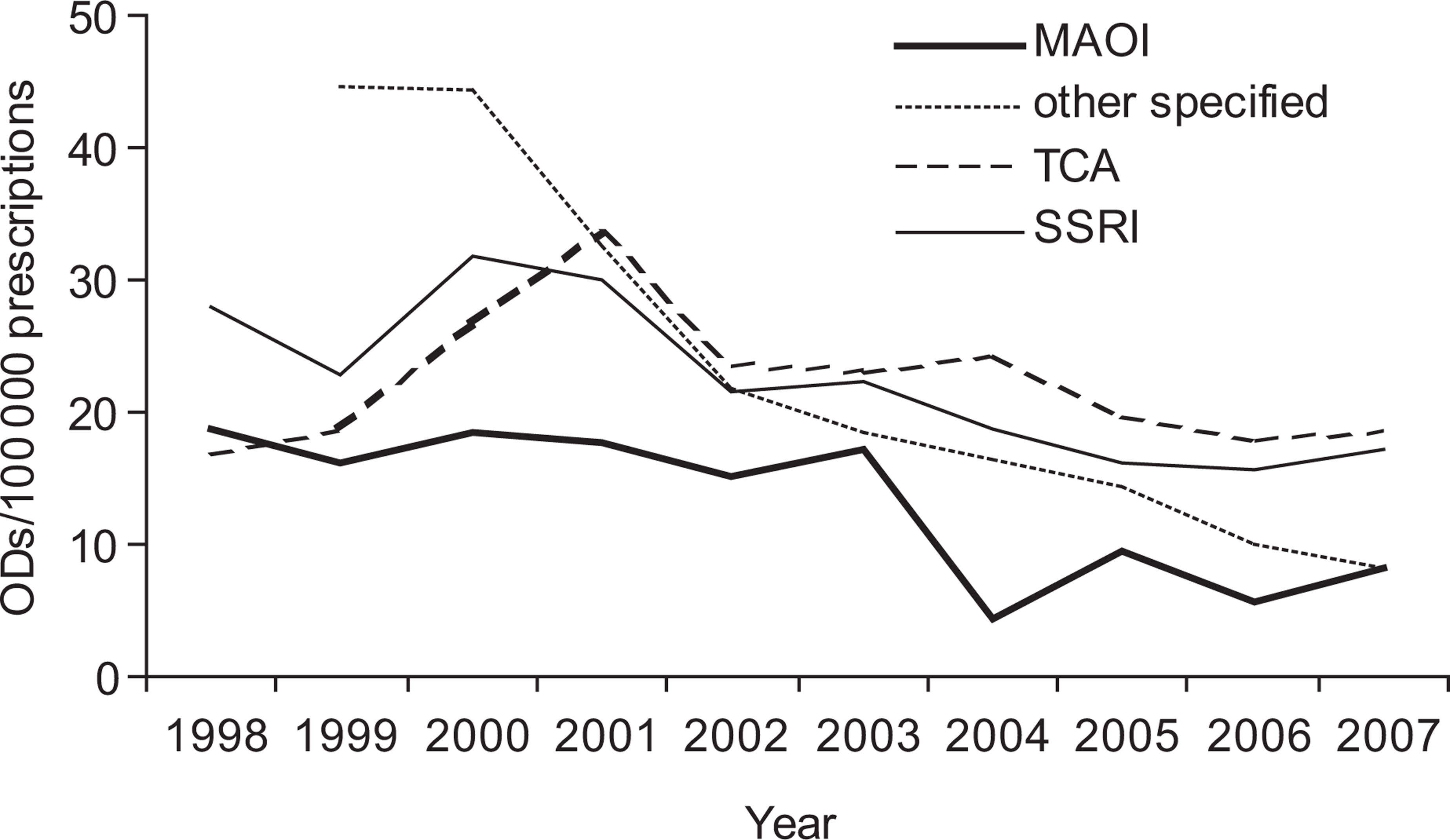
Overdoses per 100 000 prescriptions over time (Victorian Emergency Minimum Dataset and Pharmaceutical Benefits Scheme data).
Approximately two fifths of patients (2252, 41.2%) were admitted to a ward, an ED short stay unit or transferred to a mental health facility. Of those admitted, almost half (47.2%) had a SSRI OD. However, a greater proportion of patients were admitted following TCA OD (690, 60.1%) than after MAOI (67, 44.1%), ‘other’ antidepressants (367, 44.3%) or SSRI (1064, 33.6%) OD, (p < 0.001). There were three deaths, one from an SSRI and two from TCA OD.
VPIC data
Of 2892 antidepressant exposure calls to the VPIC, 1833 met the inclusion criteria of intentional OD, 1118 (61.0%, 95%CI 58.7, 63.2) cases related to females, 1693 (92.7%) calls related to adults, 120 (6.5%) to children (< 16 years) and 20 (0.8%) to the elderly (> 65 years).
The majority of calls were from doctors (553 calls, 30.2%), nurses (254, 13.9%) and family members (433, 23.6%). The remainder were from the patients themselves, friends or carers, counseling services, ambulance staff, other health professionals, the police or the fire brigade.
The majority of calls related to OD with SSRIs (1016, 55.4%) followed by ‘other’ antidepressants (551, 30.1%), TCAs (188, 10.3%), non-specified antidepressants (51, 2.7%) and MAOIs (27, 1.5%). The most frequent calls related to sertraline, venlafaxine, mirtazapine and amitriptyline.
The SSRIs predominated in the child and adult age groups and ‘other’ drugs in the elderly group (Figure 4). All of the 27 calls (1.6%) regarding MAOIs related to adult patients.
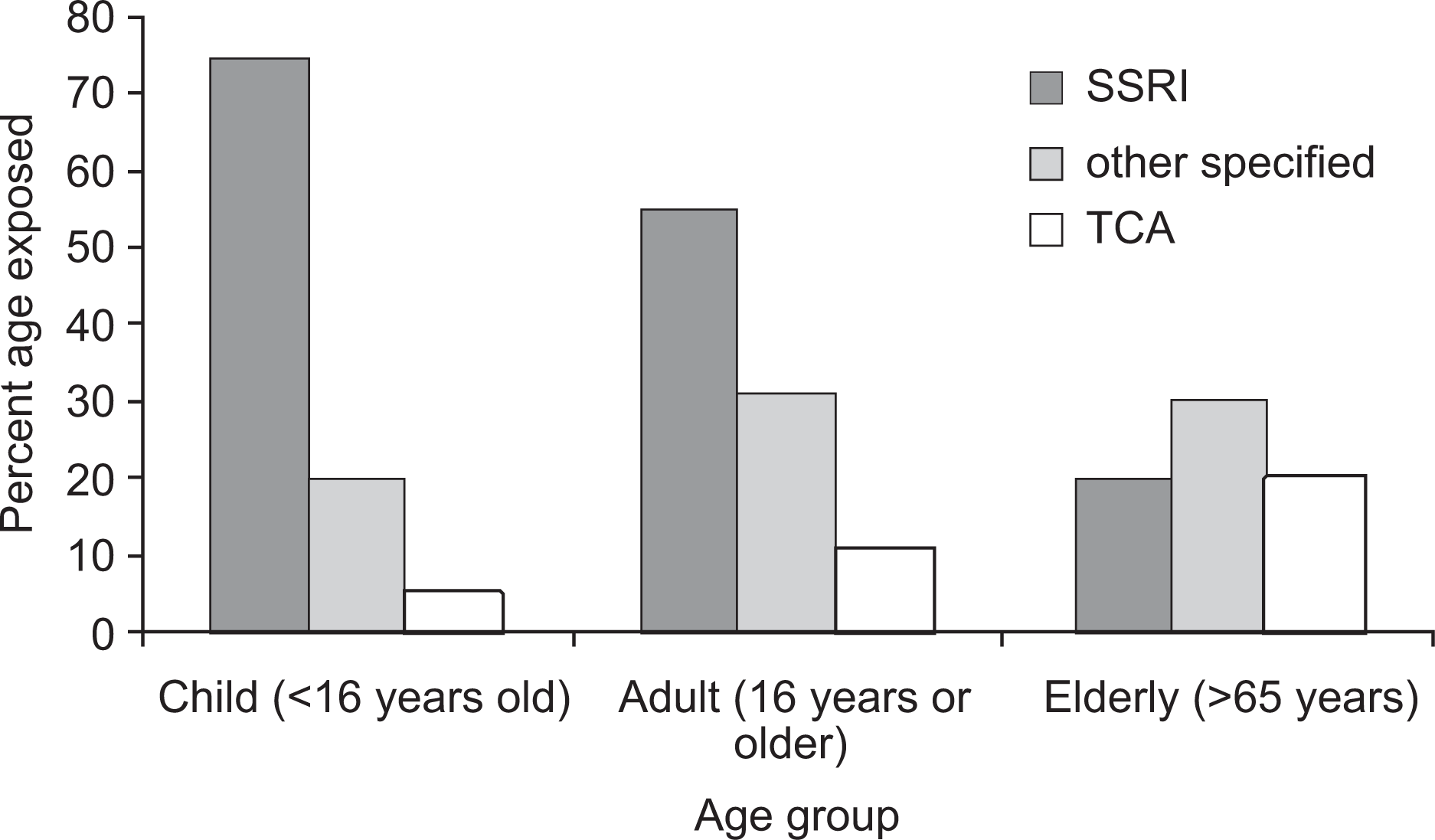
Overdose drug as a function of age group (Victorian Poisons Information Centre).
At the time of the call, 722 (39.4%, 95%CI 37.2, 41.7) cases had symptoms related to their OD. However, there were significant differences between the different drug groups (p < 0.001). Following SSRI OD, 308 (30.3%) patients had related symptoms. However, the MAOI, TAC and ‘other’ antidepressant groups had 13 (51.9%), 94 (50.0%) and 272 (50.6%) symptomatic patients, respectively.
The Poisoning Severity Score classified 118 (6.4%, 95%CI 5.4, 7.7) cases as having moderate or severe symptoms. However, the drug groups differed significantly (p < 0.01). After TCA OD, 30 (15.9%) patients had moderate or severe symptoms compared to 47 (8.6%), 2 (7.4%) and 32 (3.2%) in the ‘other’ antidepressant, MAOI and SSRI groups, respectively.
Overall, 801 (43.7%, 95%CI 41.4, 46.0) calls were from hospital staff asking for advice. For another 853 (46.5%, 95% CI 44.2, 48.9) calls, advice was given to take the patient to a hospital. For the remaining calls, advice was given to general practitioners or to refer the patient to their GP or other personnel. There was only one call where the caller was advised to keep the patient at home.
Discussion
As depression ranks fourth among chronic illnesses managed [11], health professionals must recognize its importance and gain skills in its management. Despite this, a USA-wide study showed that only 21% of patients with depression were adequately treated [12]. This hints at the underutilization of drug therapy, with or without other forms of therapy, and indicates the potential for a substantial increase in antidepressant use.
This study indicates that antidepressant drug OD remains common in Victoria. Females and young people, especially aged 20–24 years are at particular risk. This female predominance is consistent with a study by Grunebaum et al. [13]. In an examination of antidepressants and suicide risk, they reported that females used twice the number of antidepressants and had twice the suicide rate compared with males [13]. The VPIC data also indicate that there is a clear relationship between age and the nature of the antidepressant taken in OD. The frequency of SSRI and TCA OD among young and elderly cases, respectively, likely reflects prescribing patterns.
Over the study period, the population-adjusted incidence of antidepressant OD has been declining since a peak in 2001. However, this overall trend has not been the case for all drug classes. While SSRI, TCA and MAOI OD have been trending down, the incidence of ‘other’ antidepressant OD has remained relatively stable. While this is encouraging, it may not be indicative of trends apparent in OD with drugs other than antidepressants. Analysis of ‘all drug’ OD was beyond the scope of this study. However, our findings are not consistent with large non-ED UK[14] and US[15] studies which have reported decreasing TCA OD and increasing SSRI OD presentations.
Interestingly, as antidepressant drug OD has been trending down, prescription of antidepressants, overall, has been trending up. This has largely resulted from the increased prescription rates for the SSRI and ‘other’ drug classes while TCA and MAOI prescription rates have been slowly declining. Other reports from Australia [7] and New Zealand [16] support these findings. In the early 1990s, TCAs were the most common antidepressant class prescribed in Australia. Not until the mid 1990s did the SSRI prescription rate reach that of the TCAs, and the SSRI rate has continued to rise since [7]. Furthermore, the escalating use of ‘other’ antidepressants is the likely reason why the incidence of OD for this drug class has not been trending downwards.
Of most importance is the data linking OD and prescription rates. Since 2001, OD per 100 000 prescriptions has been trending down for each drug class. This indicates that antidepressant drug OD is becoming less likely for those prescribed these drugs. The reasons for this are not immediately apparent. Although speculation, it may relate to a greater experience with these drugs, newer more efficacious drugs or the increased use of effective non-drug ancillary care. Further investigation of this issue is warranted. Consistent with our findings is a study by Hall et al. where the decreased rate of suicide in Australia correlated with an increase in prescribing of antidepressants [17].
The data suggest an apparent peak in OD rates in 2001, especially for SSRI and TCA, before a trend downwards. This peak is difficult to explain but may represent an under-reporting of OD prior to 2001. Over the study period there were increasing numbers of EDs contributing data. However, all major Victorian EDs were contributing in 1998. One small metropolitan ED joined in 1999 and another in 2000. In 2004 another eight small, mainly regional EDs were also contributing. It is unlikely, therefore, that the 2001 peak can be attributed only to changes in contributing EDs.
Although there were no significant differences between the rates of OD/100 000 prescriptions for each drug class, the absolute magnitudes of the differences are notable. In particular, the MAOI rate was lowest and considerably lower than the SSRI and TCA rates. The reasons for these differences are not clear and further investigation is indicated. Although speculation, it may relate either to the efficacy of the MAOI drugs in managing depression or to differences in the patients prescribed the different agents (selection bias).
The differing safety profiles of the antidepressant drug classes are well known. TCAs can be highly toxic in OD and are associated with higher suicide rates [15]. In contrast, SSRIs are associated with a lower suicide rate [13]. Our data are consistent with these reports. Patients with TCA OD had significantly higher Poisoning Severity Scores and admission rates. In contrast, the patients with SSRI had the lowest symptom rate, Poisoning Severity Scores and admission rate of all the antidepressant classes examined. It is expected that the increasing use of antidepressants with better safety profiles (e.g. SSRIs) will result in more favourable outcomes if they are taken in OD [18]. In addition to suicide rates, the increased costs in managing TCA OD compared with SSRIs is not a new issue [5].
This study has important limitations. Some overlap in the VEMD and VPIC data is evident. Indeed, many VPIC calls related to cases already in an ED and would have appeared in both datasets. Both the VEMD and VPIC data were limited by selection bias. Neither had comprehensive data on patients who had died, patients treated in the non-ED setting nor minor OD. Our findings, therefore, do not reflect the entire OD patient population. The VPIC does not operate 24 h/day and the incidence rates reported will be an under-estimate. Furthermore, it is likely that much of the VPIC data related to patients who were less sick than those already in EDs. Typographical errors in the VEMD narratives will have meant cases were missed in the original search despite some flexibility being built into the search syntax. The VEMD data were incomplete with some triage information unavailable (e.g. drug name). VEMD narratives were recorded at the time of triage or by clerical staff post-patient discharge and are susceptible to measurement bias. As a result of some missed cases, the incidence of OD reported will be an under-estimate of the true incidence. As increasing numbers of EDs contributed to the VEMD data over the study period, data accuracy and, therefore, external validity increased progressively. We grouped all drugs together within their drug class despite there being variability in drug toxicity within each class. This may have limited the comparisons of toxicity across the drug classes. Prescription rates do not account for drug dosage and amounts of drug received. Also, some prescription data will be missing as a result of variability in co-payment thresholds for certain prescriptions and patient populations. Accordingly, they are a crude variable for comparisons across drug classes. They are likely to be more useful for comparison of trends of individual drug classes over time. Only OD rates were examined and, while these are of considerable importance in relation to risk and health care utilization, no meaningful suicide data is reported. Finally, the unit of analysis was presentations of OD rather than presentations of individuals. In many cases, individuals OD and present on numerous occasions.
Conclusion
The epidemiology of antidepressant OD is changing in Victoria. The SSRIs and newer ‘other’ drugs and are now much more widely prescribed than the TCAs and MAOIs. Drug OD patterns follow the prescription trends. Sertraline is now the most frequent antidepressant used in intentional OD. For the SSRI, TCA and MAOI classes, rates of OD/100 000 population are trending down while the rate for ‘other’ antidepressants remains stable. For, each antidepressant drug class, rates of OD/100 000 prescriptions are trending down. Although the most commonly used drug class in OD, the SSRIs cause the fewest symptoms, and have the lowest Poisoning Severity Scores and admission rates.
Footnotes
Acknowledgements