
Abstract
Background:
The obsession of turning into another person (transformation obsessions [TO]), and its related compulsions have been initially conceptualised as a form of mental contamination. Nevertheless, it has remained understudied in the current obsessive-compulsive disorder (OCD) literature. In parallel, disturbances of the self have been identified as markers of prodromal psychosis in patients with schizophrenia. Based on the later association, this study aimed to investigate the sociodemographic and clinical correlates of TO.
Methods:
In all, 1001 OCD outpatients from the Brazilian OCD Research Consortium were included in this study. Several semi-structured and structured instruments were used to compare 48 OCD patients with TO with 953 OCD patients without TO. A repression model investigated the relationships between the presence of current TO and statistically significant univariate test outcomes.
Results:
Participants with TO presented an overall younger age, a longer period of time between the onset of the OCD symptoms and an OCD diagnosis, greater severity of the sexual/religious dimension and increased suicidality symptoms.
Conclusions:
These results indicate that TO may be better conceptualised as a form of forbidden/taboo thoughts rather than contamination. While no significant associations with psychotic features (e.g. decreased insight) were observed, TO patients displayed increased suicidality, overall younger age and a significantly larger disparity between seeking treatment and OCD diagnosis. This demonstrates that further clinical awareness and research into TO as an OCD symptom is most needed.
Introduction
In clinical practice, thought-disabling concerns regarding one’s identity are not only pervasive, but also characteristic of several standalone mental disorders, such as Obsessive-Compulsive Disorder (OCD), dissociative disorders, and schizophrenia (Rachman, 2006; Sass and Parnas, 2003; Schäflein et al., 2018). However, given the growth of a dimensional approach in psychiatry, it is possible to understand preoccupations regarding one’s personal identity as lying within a spectrum ranging from the fear of being someone else (as in OCD associated with the specified ‘transformation obsessions’ [TO]) (Rachman, 2006), the ‘feeling’ that one has somehow changed (as in depersonalization disorder or prodromal phases of schizophrenia) (Schäflein et al., 2018), to the certainty that one is not the same person anymore (as in schizophrenia or other psychotic disorders) (Sass and Parnas, 2003).
Transformation obsessions, first referred to as the ‘Fear of Morphing’, are a subset of symptoms in patients with OCD that involve the presence of obsessions and/or compulsions about turning into another person or acquiring another’s undesirable physical, moral or behavioural characteristics (Rachman, 2006; Volz and Heyman, 2007). Initially suggested as, and often still considered, a form of ‘mental contamination’; morphing fears may be triggered by physical proximity or contact with the undesired person and are frequently accompanied by the person’s attempt to avoid any contact with that person. Morphing fears are typically associated with ‘undesirable’ traits of the feared person, often reflecting prejudices, such as people from marginalised cultural or racial groups, have particular physical features/deformities or are considered unpopular or immoral (Coughtrey et al., 2013; Rachman, 2006).
The term ‘transformation obsessions’ was devised and implemented in Volz and Heyman’s (2007) early study to highlight the unique persistent preoccupation with a metamorphosis of the self and to differentiate it from the generalised concept of mental contamination; defined as feelings of contamination that are derived without physical contact with an ‘infected’ article (Rachman, 2006). Case examples of OCD patients with observed transformation obsessions have included a 16-year-old female whose main fear was concerned with turning into Hitler through growing a moustache and male genitalia (Monzani at al., 2015), a 13-year-old male worried about becoming a person that he accidentally breathes on or touches (Volz and Heyman, 2007), and a man in his 20s who feared being transformed into an immoral and unintelligent person through proximity with an undesirable individual (Zysk et al., 2018). At present, there is only one OCD assessment scale that includes specific items to identify transformation obsession symptoms, the Dimensional Yale-Brown Obsessive-Compulsive Scale (Rosario-Campos et al., 2006).
Past studies with substantial sample sizes in patients under the age of 18 have found the prevalence of transformation obsessions in OCD youth assessed to range from 3.5% to 10% (Monzani et al., 2015; Volz and Heyman, 2007). The more recent and significantly larger prevalence rate presented by Monzani et al. (2015) raises the hypothesis that transformation obsessions may not be as uncommon as initially conceptualised. These studies have also suggested that transformation obsessions may be associated with an early age of obsessive-compulsive symptom (OCS) onset and higher proportions of males than females (Monzani et al., 2015; Volz and Heyman, 2007). Importantly, we are not aware of any systematic assessment of transformation obsessions in adult samples.
The association between OCD and psychotic disorders (including schizophrenia) is not uncommon (Kokurcan and Şafak, 2020). Furthermore, while OCD is sometimes associated with poor or absent insight/delusional beliefs (de Avila et al., 2019), sensory symptoms (known as ‘sensory phenomena’) may be present in 40% to 65% of patients (Ferrão et al., 2012; Prado et al., 2008). Although sensory phenomena are conceptually distinct from hallucinations, they may occasionally be difficult to differentiate (Fontenelle et al., 2008). These ‘grey diagnostic zones’ may result in delayed identification of OCD and greater duration of untreated (or mistreated, wrongly treated) illness (Dell’Osso et al., 2019). The observed presence of vivid sensory symptoms in OCD patients supports the position of a dimensional co-expression of symptoms with psychotic disorders that is upheld by a shared dysfunction in dopaminergic circuits (Fontenelle et al., 2008).
Accordingly, the presentation of transformation obsession symptoms in young people has also been conceptualised as an expression of a psychotic disorder or ‘quasi-psychotic’ in nature (Monzani et al., 2015; Volz and Heyman, 2007). Transformation obsessions can be described as having a particular conceptual overlap with a basic self (ipseity) disorder, that is, a disturbance often reported in people with schizophrenia, who may feel that they have a different identity or do not exist (Sass and Parnas, 2003). Studies in self-disorders have suggested that an instability or disruption of the basic sense of self can elicit the onset of psychosis (Daneault, 2013), as self-disorder symptoms have had a higher prevalence in prodromal, active and residual phases of psychosis (Haug et al., 2015).
Given the potential relationship between transformation obsessions and psychosis, we feel it is relevant to investigate whether this symptom is associated with other phenotypical aspects of OCD, such as greater overall symptoms severity (Dell’Osso et al., 2017), progressive course (Kichuk et al., 2013), positive family history of psychosis (Owashi et al., 2010), lower insight (de Avila et al., 2019), sensory disturbances (Ferrão et al., 2012; Fontenelle et al., 2008) and comorbid body image disorders (Conceição Costa et al., 2012).
The fact that transformation obsessions often involve bodily experiences (from feeling as though one’s face or other parts of the body have changed to identity confusion) suggests that this association may also be related to a series of OCD comorbid psychiatric disorders involving fears about body changes, such as body dysmorphic disorder (BDD), hypochondriasis, and eating disorders (particularly anorexia nervosa [AN] and bulimia nervosa [BN]). In fact, when investigated in conjunction with OCD, patients with these comorbidities often display more severe OCD symptoms (Borda et al., 2017), decreased insight levels (Toh et al., 2017) and more self-focused perceptual distortions (Buchanan et al., 2011). Patients with OCD comorbid with BDD or hypochondriasis typically display more self-focused perceptual distortions (e.g. coming to believe that one’s nose is severely crooked when it would be commonly be perceived as straight) than OCD patients without these conditions (Buchanan et al., 2011).
Although transformation obsessions have been conceptualised as a form of ‘mental’ contamination (Rachman, 2006), due to associated descriptions of a fear of physical contact and the invisible transmission of something undesirable (Radomsky et al., 2018) more recent studies have suggested that transformation symptoms are better understood as part of the ‘forbidden/taboo thoughts’ OCS dimension (Monzani et al., 2015; Volz and Heyman, 2007). The ‘forbidden/taboo thoughts’ OCS dimension encompasses obsessions and/or compulsions about the ‘aggression’ and the sexual/religious/moral OCS dimensions (Rosario-Campos et al., 2006), which are often accompanied by feelings of shame, guilt, humiliation or supernatural fears (Hale and Clark, 2013).
Given the potential association between transformation obsessions and other comorbid disorders, it is very relevant to investigate whether the presence of these obsessions are associated with specific phenotypical characteristics of OCD, such as a higher symptom severity (Dell’Osso et al., 2017), a progressive course (Kichuk et al., 2013), positive family history of psychosis (Owashi et al., 2010), lower insight level (de Avila et al., 2019), higher frequency and/or severity of sensory phenomena (Ferrão et al., 2012; Fontenelle et al., 2008) and comorbid body image disorders (Conceição Costa et al., 2012; Sallet et al., 2010).
Therefore, the current study analysed data from a large sample of adult OCD patients to investigate whether transformation obsessions and/or compulsions are associated with specific clinical characteristics. Based on the literature, it was hypothesised that OCD patients with transformation obsessions would be characterised by an earlier age at onset of the OCS, higher frequency of males (Monzani et al., 2015; Volz and Heyman, 2007), higher severity of OCS (Catapano et al., 2010), poorer insight (Catapano et al., 2010), a progressive course (Van Oudheusden et al., 2018), increased suicidality reports (Massons et al., 2017; Torres et al., 2011), higher severity of ‘sensory phenomena’ (Fontenelle et al., 2008), higher frequencies of family history of psychosis and/or disorders associated with bodily distortions (Buchanan et al., 2011; Catapano et al., 2010) and a later age at final OCD diagnosis (Volz and Heyman, 2007). Finally, based on the findings by Monzani et al. (2015), it was hypothesised that OCD patients and transformation obsessions would report an increased severity of fear of harm/taboo thoughts when compared with OCD patients without transformation obsessions.
Methods
Participants
The sample of this study was composed of 1001 OCD patients (mean age = 35, SD = 13, 56.8% female). Patients were recruited from 2003 until 2009 as part of the Brazilian Research Consortium on Obsessive-Compulsive Spectrum Disorders (C-TOC), a research initiative funded by Brazilian Government Grants. Participants required a primary diagnosis of OCD according to the Structured Clinical Interview for the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), Axis I disorders (SCID-I) (American Psychological Association [APA], 1994). Participants were excluded if they had comorbid diagnoses of schizophrenia, intellectual disability or another condition that would have impacted their understanding of the procedures involved in the study. All adult participants signed individual informed consent forms following a comprehensive explanation of the study and the guarantee that participation would not impact their opportunity to access clinical treatment. Participants under the age of 18 instead signed written informed assent, in addition to written informed consent signed by a parent/legal guardian.
Measures
The study protocol included a series of semi-structured clinical interviews conducted by trained psychiatrists or clinical psychologists with expertise in OCD as well as self-report instruments. More specifically, assessments comprised the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS; Goodman, 1989, Brazilian Portuguese version by Fontenelle et al., 1998), the Dimensional Yale-Brown Obsessive-Compulsive Scale (DY-BOCS; Rosario-Campos et al., 2006), the University of São Paulo Sensory Phenomena Scale (USP-SPS; Rosário et al., 2009), the Brown Assessment of Beliefs Scale (BABS; Eisen et al., 1998, Portuguese translation by Ferrão and Hounie, 2002, as cited in Miguel et al., 2008), the Beck Depression Inventory (BDI; Beck et al., 1961, Brazilian Portuguese version by Cunha, 2001), the Beck Anxiety Inventory (BAI: Beck et al., 1988, Brazilian Portuguese version by Cunha, 2001), the Yale OCD Natural History Questionnaire (Leckman and Cohen, 1999, Portuguese translation by Rosário et al., 2002, as cited in Miguel et al., 2008), the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I; First et al., 1997, Brazilian Portuguese version by Del-Ben et al., 2001) and a Medical and Risk Factors Questionnaire that was specifically designed for the C-TOC studies to gather data pertaining to patient sociodemographic, socioeconomic, suicidality and medical/psychiatric history data.
The DY-BOCS was used to identify OCD patients with transformation obsessions through ‘currently experiencing’ answers of items 78 and/or 79. Item 78 refers to the experience of intrusive thoughts about turning into another person and item 79 involves the experience of active compulsions to relieve feelings or fears of turning into another person (Rosario-Campos et al., 2006).
Procedure
The C-TOC research studies were approved by the local Ethics Committee of the involved universities. An ethical amendment was approved by the Monash University and the Monash Health Human Research Ethics Committees. All the subjects were interviewed by experienced clinicians. Detailed information about the C-TOC procedures is described elsewhere (Miguel et al., 2008).
Data analysis
Data analyses included initial univariate analyses that were then used in a single multivariate regression to identify independent predictors of transformation obsessions. Independent Samples t tests or Mann–Whitney U tests were used to compare the sociodemographic and clinical OCS severity of OCD patients with and without current transformation obsessions, according to whether the variables were normally distributed or not. Categorical variables were described by absolute (n) and relative (%) values and compared between groups with Yates or Pearson Chi-Square tests and Fisher’s Exact tests.
Nominal data (gender, suicidality, family history of psychosis, spending over 3 hours a day thinking about appearance, progressive OCD course and prevalence of BDD, hypochondriasis, AN and BN); was analysed through a Chi-Square Test of Contingencies. However, if the expected frequency assumption was violated then Fisher’s Exact Test was used instead. The Mann–Whitney U Test was implemented when analysing ordinal data or scale data between the groups if the normality assumption from an independent sample t test was violated (i.e. current age, age at onset of OCD symptoms, age when symptoms became bothering, age when treatment sought, age diagnosed with OCD, severity of aggression, sex/religion, contamination/cleaning and symmetry/order and hoarding dimensions: BDI, BAI, BABS and USP-SPS scores, and level of insight in BDD symptomology).
A binomial logistic regression was used to observe the relationships between the presence of current transformation obsessions and the statistically significant (alpha = .05) univariate test outcomes. Missing values were excluded list-wise, resulting in 81 missing cases and the total sample size decreasing to 920 OCD patients. The number of cases of OCD patients without transformation obsessions was 876 (95.2%) and the sample of OCD patients with transformation obsessions was 44 (4.8%). The impact of collinearity was determined through obtaining the Variance Inflation Factor (VIF) of each independent predictor. There was an instance of high collinearity between two age-related variables (age when treatment sought [VIF = 7.79] and age diagnosed with OCD [VIF = 11.79]). This was resolved by removing the variable with the highest VIF value (age diagnosed with OCD), which levelled all VIF values to acceptable levels of below 2.9 (Hair et al., 2010).
Results
Descriptive statistics and univariate analyses
At the baseline interview there were 48 (4.8%) OCD patients that experienced current transformation obsessions and/or compulsions and 953 (95.2%) OCD patients that did not experience transformation obsessions and/or compulsions.
Tables 1 and 2, compare sociodemographic and clinical features between the groups, respectively. OCD patients currently experiencing transformation obsessions were found to have higher total scores on the aggression, sex/religion/moral, symmetry/ordering and hoarding dimension scales of the DY-BOCS. Compared to OCD patients without current transformation obsessions, OCD patients with transformation obsessions also had significantly lower current age, age at which treatment was first sought, and age at which the patient was first diagnosed with OCD.
Sociodemographic variable descriptive statistics with Mann–Whitney U tests and Pearson Chi-Square Test of Contingencies grouped by current transformation obsessions (TO).
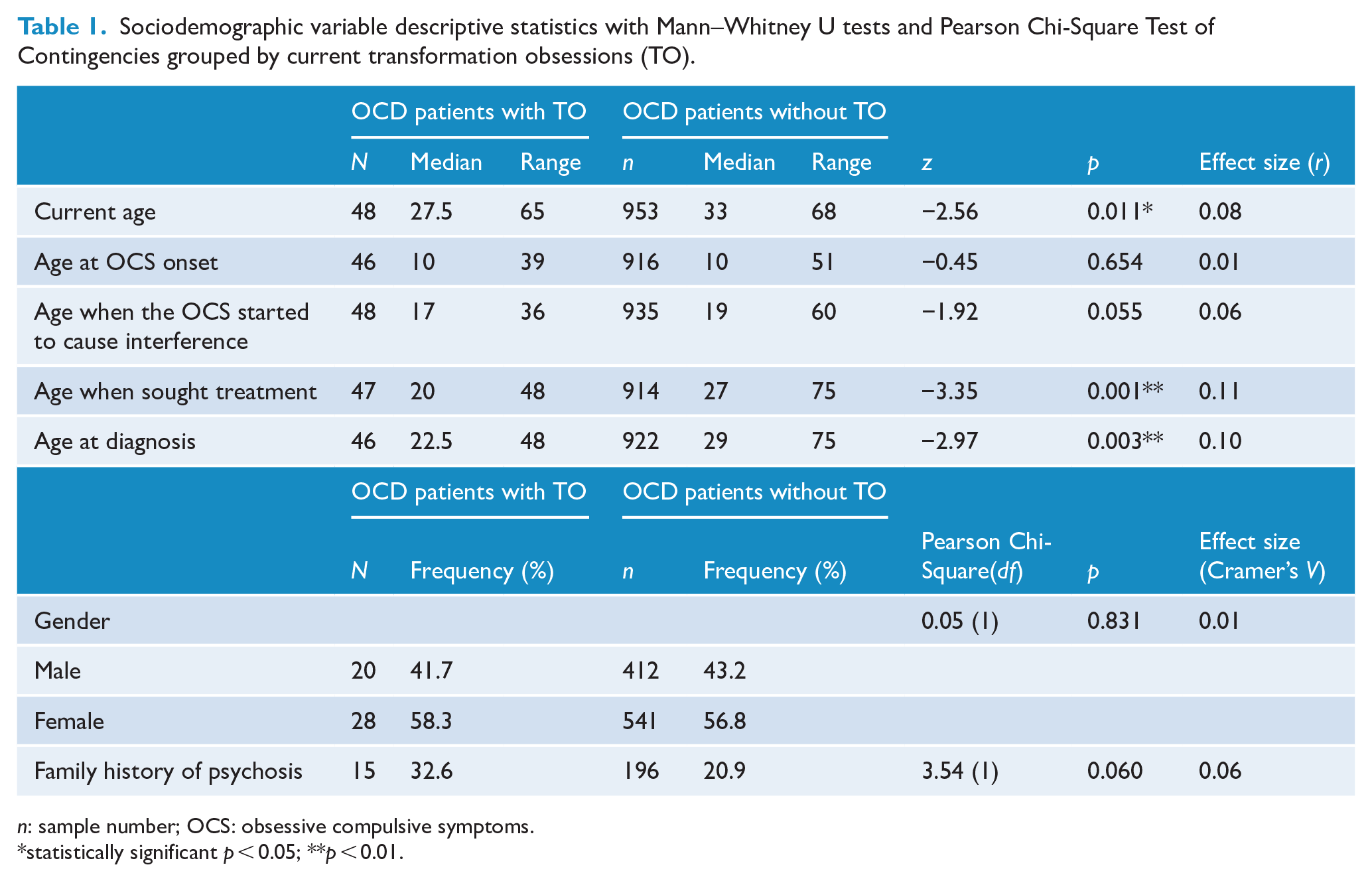
n: sample number; OCS: obsessive compulsive symptoms.
statistically significant p < 0.05; **p < 0.01.
Clinical variable descriptive statistics with Mann–Whitney U tests and Pearson Chi-Square Test of Contingencies grouped by current transformation obsessions (TO).
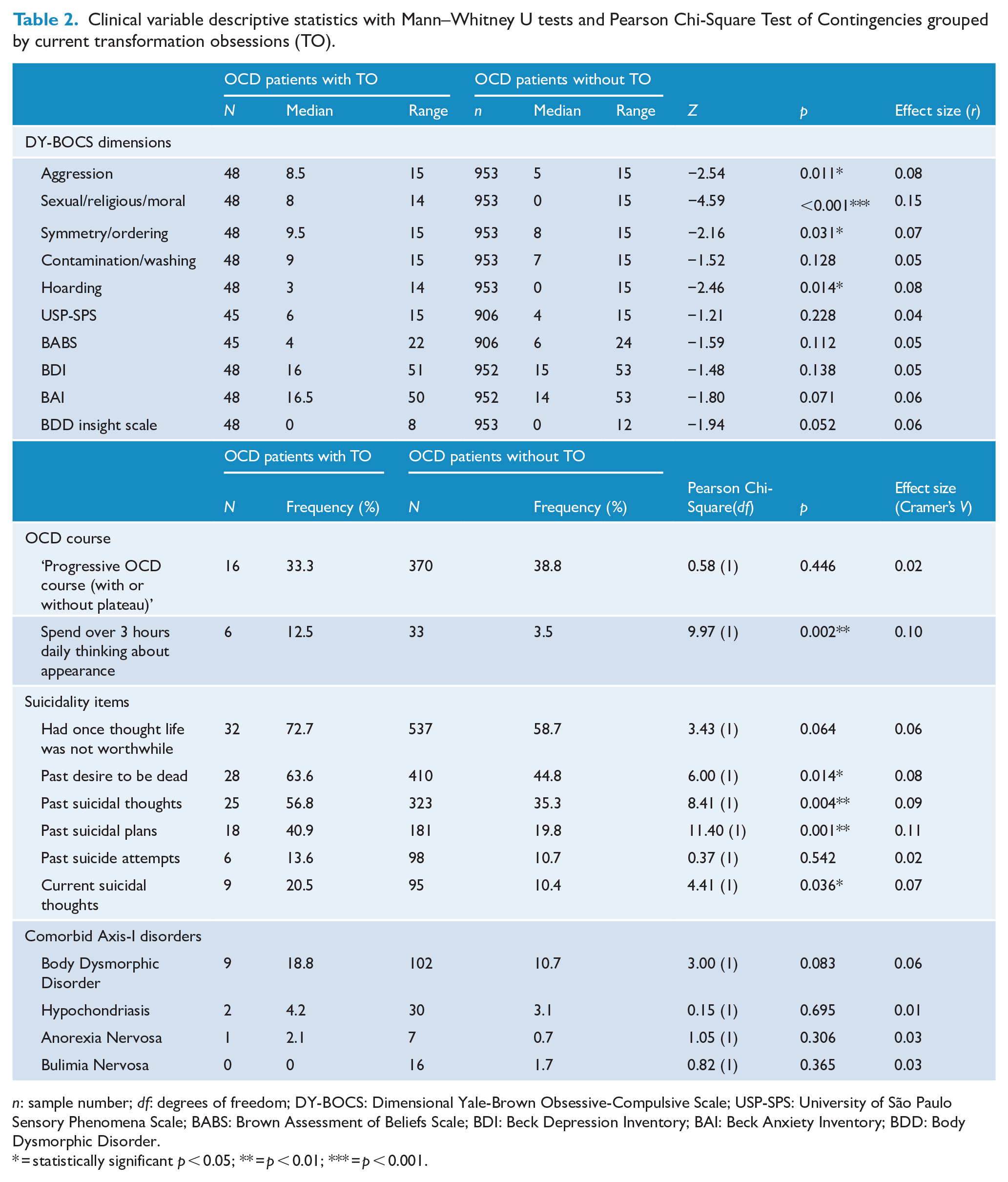
n: sample number; df: degrees of freedom; DY-BOCS: Dimensional Yale-Brown Obsessive-Compulsive Scale; USP-SPS: University of São Paulo Sensory Phenomena Scale; BABS: Brown Assessment of Beliefs Scale; BDI: Beck Depression Inventory; BAI: Beck Anxiety Inventory; BDD: Body Dysmorphic Disorder.
= statistically significant p < 0.05; ** = p < 0.01; *** = p < 0.001.
Positive answers to four of the six suicidality items also had a statistically significant higher frequency in patients with transformation obsessions than without. This included items describing past thoughts about wanting to be dead, past thoughts of suicide, past suicide plans and current suicidal thoughts. Patients with transformation obsessions also displayed a statistically significant higher frequency of spending over 3 hours thinking about their appearance. However, all of the statistically significant variables had effects that are considered quite small (Cohen, 1988).
Independent samples t tests were used to compare the severity of obsessive-compulsive symptoms, measured by the Y-BOCS, between OCD patients with transformation obsessions and those without transformation obsessions (see Table 3). Independent t tests did not indicate a statistical significant difference between groups in obsessive, t(957) = 0.87, p = 0.383, two-tailed, d = 0.13, and compulsive, t(982) = 0.38, p = 0.704, two-tailed, d = 0.06, symptoms. In addition, the t tests revealed that there was no statistically significant difference between the groups in terms of global severity of OCD (total YBOCS scores), t(999) = 1.16, p = 0.248, two-tailed, d = 0.18.
Y-BOCS descriptive statistics and t test confidence intervals grouped by current transformation obsessions (TO).
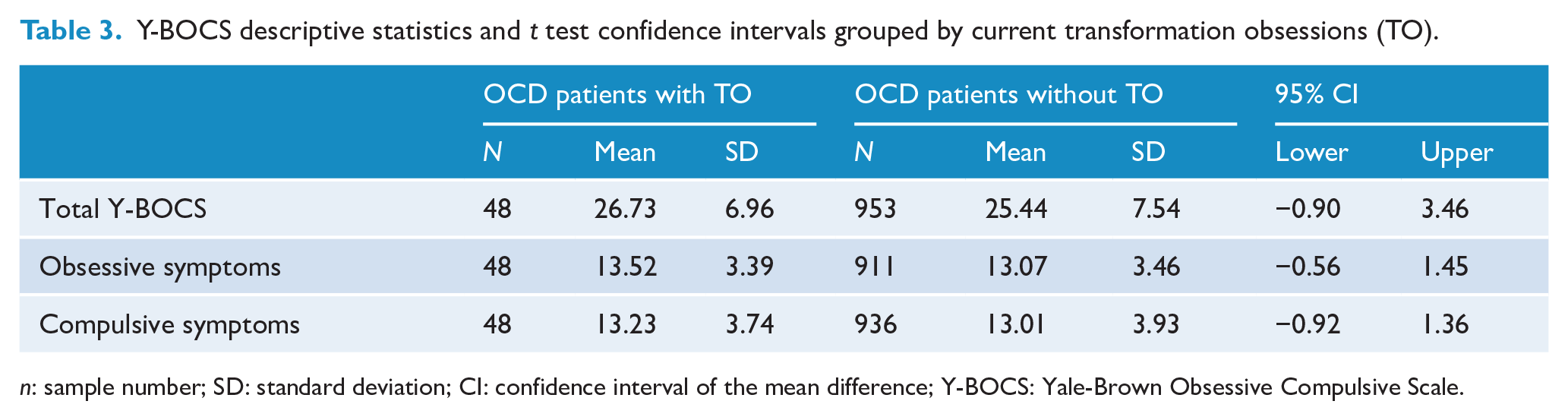
n: sample number; SD: standard deviation; CI: confidence interval of the mean difference; Y-BOCS: Yale-Brown Obsessive Compulsive Scale.
Regression analysis
The following variables were included in the binomial logistic regression model: current age, age at treatment sought, whether patients spend over 3 hours thinking about their appearance, the severity of four OCD dimensions (aggression, sex/religion/moral, symmetry/order and hoarding) and the levels of suicidality features.
As seen in Table 4, only two variables were identified as significant independent predictors that improved the model’s predictive capability. The model found that a lower age for seeking treatment was associated with an increased likelihood of exhibiting current transformation obsessions and increasing scores on the Sex/Religion/Moral dimension was associated with an increased likelihood of exhibiting current transformation obsessions
Binomial logistic regression model with OCD patients experiencing current transformation obsessions as the dependent variable.
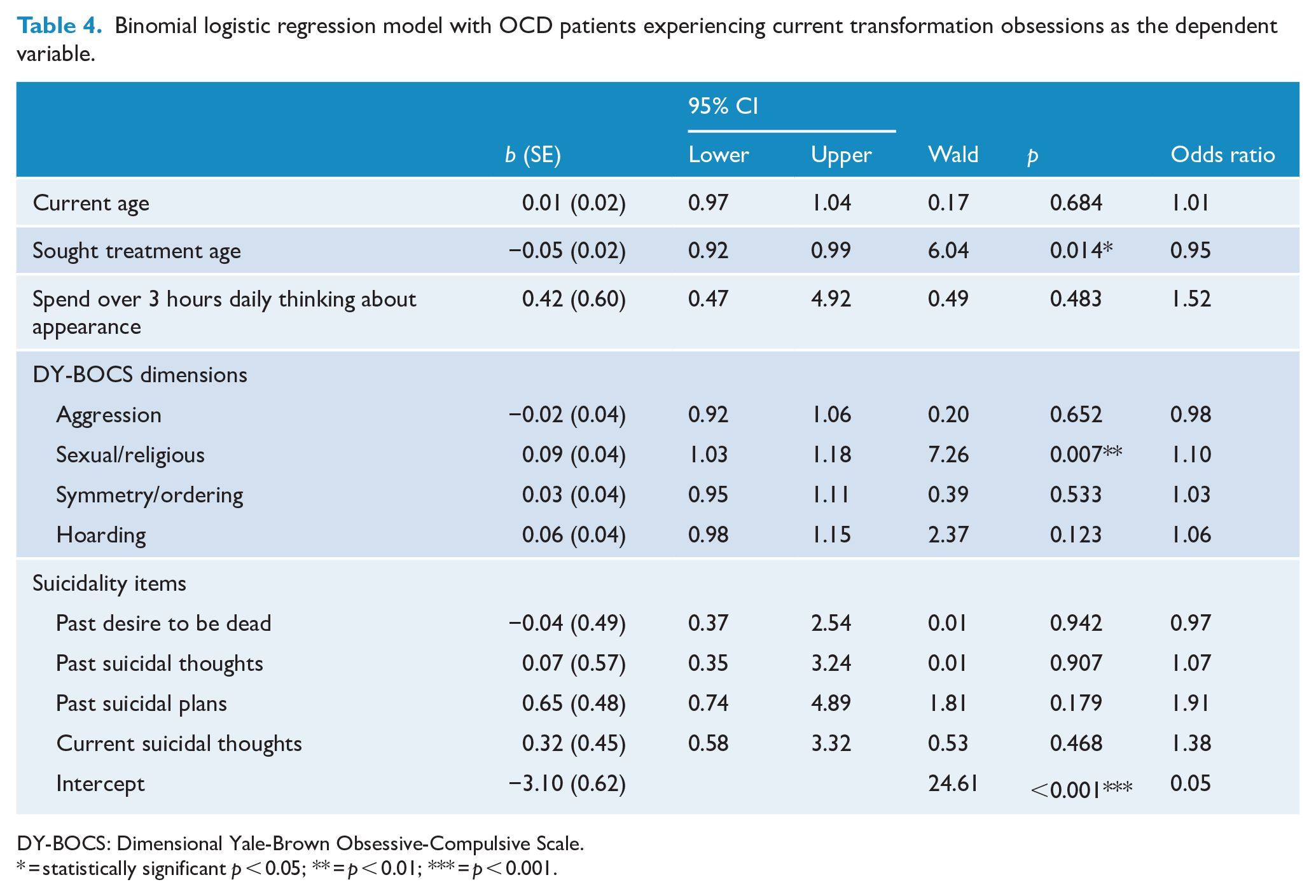
DY-BOCS: Dimensional Yale-Brown Obsessive-Compulsive Scale.
= statistically significant p < 0.05; ** = p < 0.01; *** = p < 0.001.
Post-hoc analysis
Due to the high multicollinearity between the significant variables ‘age at diagnosis’ and ‘age when sought treatment’, ‘age at diagnosis’ was removed from the regression model. However, further analysis was taken to explore the nature of its close association with the variable ‘age when sought treatment’. A new variable was created by subtracting the difference between the two variables to determine the length of time (measured in years) between the age at which treatment was sought for the first time and the age at which a diagnosis of OCD was made.
A Mann–Whitney U test found that the difference in age between seeking treatment and diagnosis in OCD patients with transformation obsessions (mean rank = 552.57, Mdn = 0, range = 25) was statistically significantly higher than OCD patients who do not experience transformation obsessions (mean rank = 474.76, Mdn = 0, range = 61), z = -2.46, p = 0.014. However, this can be indicated as a small effect, with r = 0.08 (Cohen, 1988). On mean average, OCD patients with transformation obsessions (M = 2.43, SD = 5.11) experienced around a year delay in diagnosis longer than OCD patients without transformation obsessions (M = 1.46, SD = 5.06).
Discussion
While there have been steps made in developing and analysing effective treatments for adult patients with morphing fears through single-subject case studies (Coughtrey et al., 2013; Shafran et al., 2019; Zysk et al., 2018), at present, this is the first study to have centred on developing an understanding of the frequency, phenomenology and clinical correlates of transformation obsessions within a substantial adult OCD sample.
The frequency of transformation obsessions in the total sample of OCD patients within the current study was 4.8%, a figure in-between the two previous paediatric rates of 3.5% and 10% (Monzani et al., 2015; Volz and Heyman, 2007), and indicates that transformation obsessions are not rare symptoms and that some form of transformation obsessions may be present within one in every twenty OCD patients.
In congruence with the first hypothesis, OCD patients with transformation obsessions were found to be significantly younger at the time of the interview. Despite the evidence of younger age and younger treatment seeking, there was no significant difference in age at OCS onset between the groups. This indicates that while patients experiencing transformation obsessions develop their symptoms around the same time as other OCD patients, the unusual and distressing nature of these symptoms may prompt an earlier decision by concerned patients or parents to seek professional help.
The expression of transformation obsessions is thought to be maintained by an insecurity in self-identity (Rachman, 2006; Zysk et al., 2018), a prominent feature of psychosocial development during adolescence and young adulthood (Arnett, 2000). Numerous studies have observed rising rates and severity of identity distress and dysfunction in adolescents and young adults, particularly within young clinical populations (Palmeroni et al., 2020). These findings support the current study’s significant association between transformation obsessions and younger age at seeking treatment and imply that being in a developmental period where self-stability is naturally low may be a predictor of developing obsessive-compulsive fears of morphing.
In contrast with the hypothesis that males would be more likely to express obsessions/compulsions about fears of transformation, the results found no significant difference between groups in gender frequency. In fact, there was a higher frequency of women than men in the current study’s transformation obsessions group, which is the first deviation from the male trend observed in the limited previous literature with sufficient sample sizes (Monzani et al., 2015; Volz and Heyman, 2007).
OCD patients with transformation obsessions were not found to be associated with a higher severity of obsessions, compulsive behaviours, overall OCD symptoms, or depression and anxiety symptoms; indicating that the experience of transformation obsessions does not correlate to a more severe expressions of symptoms.
The second hypothesis was not supported, as ‘psychotic features’ (e.g. increased delusionality) did not exhibit any significant group differences. It should be noted that a comorbid diagnosis of schizophrenia was a part of the exclusion criteria for the study sample, while other comorbid diagnoses were not controlled for, and this may have impacted results from psychosis-related variables, including family history of psychosis.
Significant results in univariate analyses proposed that elements of suicidality may be elevated in patients with current transformation obsessions; however, their role did not emerge as significant in the regression analyses.
It was found that OCD patients with transformation obsessions were diagnosed at a significantly younger age than those without transformation obsessions, which contrasted with the hypothesis that suggested a later age at diagnosis for individuals with transformation obsessions. However, a post hoc test that considered the difference between age at diagnosis and age at treatment seeking discovered a significant discrepancy between the two groups, whereby on mean average, the patients with transformation obsessions experienced a year longer between seeking treatment and diagnosis than the patients without transformation obsessions. This supports the concerns raised by previous studies (Monzani et al., 2015; Volz and Heyman, 2007), and suggests that clinicians treating these patients may have experienced difficulty in classifying transformation obsessions as forms of OCD symptomatology sufficient for a swift, accurate diagnosis. However, this conclusion is impacted by the detail that it was not able to be accurately determined whether transformation obsessions were the predominant symptoms for which consultation was sought for the participants with current transformation obsession symptoms as identified by the DY-BOCS.
The lack of discrepancy in clinical correlates between OCD patients with and without transformation obsessions solidify transformation obsessions as symptoms of OCD; therefore, it is important that they are identified and diagnosed as such. Ultimately, more clinical awareness and insight into this OCD subtype is required in order for the observed disparity in gaining efficient treatment to minimise or disappear.
The sexual/religious dimension was the only dimension identified as a significant independent predictor of transformation obsessions. This supports the initial findings of Monzani et al. (2015), whereby transformation obsessions were found to load onto a ‘forbidden thoughts’ factor that included obsessions that were sexual or religious in nature. Notably, the sexual/religious dimension has been identified as being associated with several concerning outcomes in OCD patients, including higher suicidality, greater severity of OCD symptoms, and lower responses to general Cognitive Behavioural Therapy (CBT) treatment methods (Thorsen et al., 2018; Torres et al., 2011). Transformation obsessions can be speculatively linked to religious obsessions through the shared elevated involvement of thought-action fusion, magical ideation and a preoccupation with the occurrence of supernatural/impossible events (Coughtrey et al., 2013; Zysk et al., 2015). There has been evidence to suggest that fears of transformation can be maintained by a diminished sense of self and low self-esteem, and that targeting these deficiencies in CBT treatment may reduce the presence of transformation obsessions (Zysk et al., 2018). This previous finding provides another possible connection between religious obsessions and transformation obsessions, as greater positive religiosity (i.e. a loving perception of God) has been found correlated with increased self-esteem across different age groups (Smith and Crosby, 2016). Further research into transformation obsessions and sexual/religious dimensional symptoms of OCD with measures of religiosity and self-esteem is required in order to explore these proposed implications.
The current study’s results did not support the fourth hypothesis, as rates of comorbidity in BDD, hypochondriasis, AN, and BN were not significantly different between the two groups, indicating that transformation obsession related bodily fears are distinct from symptoms of body-focused disorders that are of a diagnostic threshold. However, according to the self-report screening measure for BDD used in the SCID-I, it was established that OCD patients with transformation obsessions spent ‘over 3 hours a day thinking about their appearance’ with a frequency that was significantly (3.5 times) higher than patients without transformation obsessions. In addition, the finding that OCD patients with transformation obsessions experienced a 3.5 times higher rate of spending over 3 hours a day thinking or worrying about their appearance expresses implications about effective daily functioning. Although these data could indicate that preoccupations with physical appearance and personal identity are actually part of the same ‘self-awareness’ spectrum, time spent thinking about appearance was not identified as a significant independent predictor in the regression model.
There are several limitations of the study’s methodology that should be considered when interpreting the results. For instance, the study used a cross-sectional design which meant that we were unable to discover the duration of transformation obsessions across a participant’s life or whether symptoms fluctuated in severity over time. Further, despite a large overall sample size, the study sample of participants with current transformation obsessions was very disproportionate to the sample of participants without transformation obsessions. This may have led to an increased margin of error, which therefore, may have decreased the power of the results from the transformation obsessions group.
Future studies should focus on longitudinal outcomes in OCD patients with transformation obsessions, as no studies have yet done this with a sufficiently sized adult sample. They could also include patients with schizophrenia or other psychotic disorders and utilise instruments used to measure symptoms of psychosis, such as the Bonn Scale for the Assessment of Basic Symptoms (Gross et al., 1987) or the Examination of Anomalous Self-Experience scale (Parnas et al., 2005), in order to determine if scores from OCD patients with transformation obsessions align closer to scores from individuals with schizophrenia or to OCD without transformation obsessions. In addition, future studies would benefit from implementing severity measures (e.g. the Morphing Fear Questionnaire) (Zysk et al., 2015) to provide a robust method of discerning both the presence and severity of transformation obsessions in OCD patients.
In conclusion, out of the variables tested, it was found that younger age at first seeking treatment and a higher severity of sexual/religious dimension symptoms predicted transformation obsessions in OCD patients. Thus, the unusual nature of transformation obsessions may spur a quicker reaction to seek professional help. There were no significantly raised rates of comorbid body-focused disorders, including BDD, AN, BN and hypochondriasis, in OCD patients with transformation obsessions. The lack of findings to support an association between transformation obsessions and OCD psychotic features highlights the importance accurately describing transformation obsessions as relatively typical. Achieving this will hopefully coincide with a reduction of the observed disparity between seeking treatment and gaining an accurate OCD diagnosis in individuals with transformation obsessions. This can be accomplished by further research to gain increased understanding and awareness of its expression and treatment.
Footnotes
Consent to Participate/Publish
Informed consent was obtained from all individual participants included in the study. Study conducted at: Brain & Mental Health Research Hub (BrainPark). Turner Institute for Brain and Mental Health, Monash University, 770 Blackburn Rd, Clayton, VIC 3168 Australia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
C-TOC research studies were given in to and approved by the local Ethics Committee of the connected university treatment centres. Ethical amendment approval was sought in Melbourne to gain access to the Brazilian database and was approved by Monash University and the Monash Health Human Research Ethics Committees (Date 05/09/2019, No. 21842).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Prof. Fontenelle was supported by Consdelho Nacional de Desenvolvimento Científico e Tecnológico (CNPq; grant # 302526/2018-8, Rio de Janeiro, RJ, Brazil), Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ; grant # CNE E-26/203.052/2017, Rio de Janeiro, RJ, Brazil), the David Winston Turner Endowment Fund (Melbourne, VIC, Australia), and intramural grants from D’Or Institute for Research and Education (IDOR, Rio de Janeiro, RJ, Brazil).