
Abstract
Objective:
Increased point prevalence rates of oppositional defiant disorder and conduct disorder have been reported in American Indian and Canadian First Nations children and adolescents. To date, in Australia, there has been no published examination of standardized Diagnostic and Statistical Manual mental disorder diagnoses in First Nations children and adolescents, determined after addressing key cultural methodological issues.
Methods:
In all, 113 First Nations children and adolescents and 217 non-First Nations young people, aged 6–16 years, age, gender, mental disorder symptom severity, symptom-linked distress and impairment matched were recruited in a case control study. Also, 112 typically developing non-First Nations participants, age and gender matched to the other two clinical groups as a second comparison group were recruited. Diagnostic and Statistical Manual mental disorder diagnoses via semi-structured clinical interview, social adversity status and full scale IQ were determined in all participants with cultural validity and reliability of the impairing patterns of symptoms in First Nations young people determined by First Nations mental health staff and Aboriginal Health Liaison Officers. Full scale IQ and social adversity status were appropriately controlled in the Logistic Regression analyses of Diagnostic and Statistical Manual mental disorder diagnoses between the two clinical groups.
Results:
Oppositional defiant disorder was the only diagnostic and statistical manual mental disorder diagnosis that differed between the First Nations and non-First Nations clinical groups, adjusting for confounding by social adversity status and full scale IQ in the multivariable model. The point prevalence of oppositional defiant disorder was 2.94 times higher (95% confidence interval: 1.14–7.69) among the First Nations compared to the non-First Nations clinical group.
Conclusion:
Key known risk factors for oppositional defiant disorder can be identified early and holistically managed in First Nations young people. This will prevent oppositional defiant disorder decreasing their access to mental health services and increasing their involvement in the criminal justice system. In addition, the resilience building aspects of oppositional defiant disorder that may enhance self-respect need to be nurtured.
Keywords
Introduction
First Nations (Aboriginal and Torres Strait Islander) children and adolescents in Australia continue to suffer from significant economic, social and physical health disadvantage compared to their non-First Nations peers, regardless of the region where they live (Australian Institute of Health and Welfare (AIHW), 2018). Their mental health is similarly significantly worse. Despite experiencing much higher levels of mental health stress, mental disorder and self-harm, First Nations young people do not differ from non-First Nations youth in their use of existing mental health services (First Nations 20%—non- First Nations 18%) (AIHW, 2018). Importantly, these comparisons are consistent across a variety of national and international databases (Anderson et al., 2016; Azzopardi et al., 2018). Azzopardi et al. (2018) also notes that First Nations young people report higher levels of depression but have lower rates of admission for comparable levels of depression than their non-First Nations peers, suggesting that there are existing barriers for First Nations children and adolescents and their families accessing mental health care.
The large-scale epidemiological survey of Aboriginal children aged 4–17 years in Western Australia (De Maio et al., 2005), used a questionnaire to interview carers face to face in discrete households about the mental health status of their child. The authors first confirmed the cultural psychometric validity and reliability of their ascertainment process and then reported that 24% of the First Nations children were at high risk of clinically significant emotional and behavioral difficulties. This was significantly higher than the 15% figure reported in non-First Nations children. Internationally, the Great Smoky Mountain Study in the United States (USA; Costello et al., 1997), using non-First Nations trained interviewers administering a semi-structured clinical interview, reported a point prevalence of 17% for one or more carer-reported mental disorder diagnoses in the First Nations children, compared to 19% in the non-First Nations children. A similar figure of 15% was reported in 109 First Nations (American Indian) children aged 13–17 years using a similar methodology (Beals et al., 1997). In contrast, Whitbeck et al. (2008) investigated 651 American Indian and Canadian First Nations children and adolescents aged 10–12 years at base line and 13–15 years at follow-up. They found a 12 month prevalence of 15.2% in the 10- to 12-year-old group and 41.2% in the 13- to 15-year-old group of one or more carer-reported Diagnostic and Statistical Manual (DSM) mental disorder diagnoses. These figures were significantly higher than those found in non- First Nations age-matched peers. In their study, trained First Nations interviewers who were members of the First Nations community administered the semi-structured clinical interviews. The authors also reported that three mental disorders’ 12 month prevalence increased from baseline to follow up: major depressive disorder (MDD) 1.7% to 7.8%; oppositional defiant disorder (ODD) 5.6% to 14.3%; and conduct disorder (CD) 4.4% to 15.5%. generalized anxiety disorder (GAD), attention deficit hyperactivity disorder (ADHD) (combined presentation) and dysthymic disorder (DD—DSM 5 persistent depressive disorder equivalent) did not change significantly from base line to follow up. The MDD figure was consistent with non-First Nations peers (1.6%—8.9%) while the ODD and CD figures were significantly higher than non-First Nations peers (5%—10%). This same group subsequently completed an 8 year follow up study of the ODD and CD groups and determined that those with no ODD or CD symptoms over the 8-year follow-up period had greater caregiver warmth, positive school adjustment, less social discrimination, less peers with ODD or CD symptoms and were less likely to have a caregiver with major depressive disorder at baseline (Greenfield et al., 2017). To date, in Australia, there has been no published examination of standardized DSM mental disorder diagnoses in First Nations children and adolescents.
There are a number of methodological issues specifically linked to defining mental disorders in a cultural context: For example, a wide range of point prevalences for ADHD have been reported in Canadian First People (Baydala et al., 2006) (22.7%) and Brazilian First Nations (Azevedo et al., 2020) (1.1%) community samples, with comorbid ODD, CD and anxiety symptoms in the latter sample, using gold standard ADHD psychometric measures in non- First Nations populations, but without validity and reliability data for the respective First Nations young people. Other authors have noted that the variability of mental disorders point prevalence rates is reduced when the cultural variation of the countries sampled are limited (Canino et al., 2010) and First Nations specific understandings of Western constructs of ADHD, ODD, CD and anxiety/depressive disorders are ascertained (Betancourt et al., 2009). Finally, the advantages of First Nations people and mental health professionals working collaboratively and as co-investigators in a mutually beneficial dialogue with shared understandings of symptoms and their associated impairment in a variety of domains, have been outlined internationally (Storck et al., 2009) and in Australia (Loh et al., 2016). An additional important issue in determining the point prevalence of mental disorders in First Nations young people is community versus clinic referred case ascertainment. Clinic referred samples have limited generalizability due to referral biases and grossly inflated point prevalence diagnostic estimates (Verhulst, 2001). Yet, their clear advantage is the potential for culturally valid and reliable mental disorder diagnoses to be made in a culturally safe and appropriate way (Fleischmann and Dabbah, 2019).
It is crucial to control social adversity status (SAS) in any assessment of the point prevalence of mental disorders in First Nations children and adolescents. Lower SAS is known to have a greater than chance association with a range of mental disorders including ADHD and ODD/CD (Counts et al., 2005). Lower SAS is also known to have a greater than chance association with First Nations children and adolescents in Australia (AIHW, 2018). Moreover, lower SAS is known to have a greater than chance association with lower Intelligence Quotient (IQ) attainment (Turkheimer et al., 2003).
Accordingly, in this study, the First Nations authors aim to carefully assess for DSM mental disorder diagnoses in First Nations children and adolescents. The cultural validity and reliability of the impairing patterns of symptoms will be carefully and systematically determined by First Nations mental health staff and Aboriginal Health Liaison Officers. Given the First Nations group examined is clinic referred, an age, gender, mental disorder symptom severity, symptom-linked distress and impairment matched clinic referred group of non-First Nations young people will be used as a clinical comparison group. A typically developing participant group from the same 50 local primary and secondary schools as the non-First Nations clinical group will be used to determine if full scale IQ and SAS status of the First Nations and non-First Nations clinical groups differ so they can be appropriately controlled in the analyses. The authors hypothesize that ODD and CD will be significantly increased in the First Nations young people compared to the non-First Nations children and adolescents.
Methods
Participants
In all, 113 First Nations children and adolescents, aged 6-16 years, were recruited from consecutive referrals to the Wadja Aboriginal Family Place and their tertiary hospital based First Nations mental health team over a 3-year period. The First Nations young people, their families and community were cared for by the Victorian Aboriginal Health Service or Victorian Aboriginal Community Controlled Health Organizations and/or the Victorian Aboriginal Child Care Agency. They were referred for a range of difficulties that overlapped but can be grouped as follows: oppositional defiant rule breaking behaviors (61%), impulse control problems (19%), depression and anxiety difficulties (15%) and other (namely learning problems (5%). Sixty seven percent of these children were medicated with stimulant medication being most common (81%).
An age, gender, mental disorder symptom severity, symptom-linked distress and impairment (Rutter et al., 1975) matched clinic referred group of non-First Nations young people (N = 217), aged 6–16 years, from 50 local primary and secondary schools was recruited as a clinical comparison group over a 5-year period. These 217 children and adolescents were screened from a total sample of 574 children and adolescents identified by teachers and/or school support staff as having coping difficulties who then referred them to specialized university clinics in metropolitan Melbourne (Australia), over a 5-year period. All 574 young people were assessed but only 217 were age, gender, mental disorder symptom severity, symptom-linked distress and impairment matched to the First Nations group. They were referred for a range of difficulties that overlapped but can be grouped as follows: oppositional defiant rule breaking behaviors (60%), impulse control problems (21%), depression and anxiety difficulties (12%) and other (namely learning problems (7%). 63% of these children were medicated with stimulant medication being most common (83%). The two groups did not differ with respect to their referring problems, their medication status or the community-based psychosocial interventions that had been trialed. All the children and adolescents met the inclusion criteria of living in a family home (and not in an institution) and attending normal primary and secondary schools. All had non-age corrected Intelligence Quotients of 70 or above (Wechsler, 2003) and none had neurological disease, endocrine disease, substance abuse/dependence disorders, personality disorders, bipolar or psychotic disorders. There was no refusal to participate. The clinical research protocol was Hospital Ethics Committee approved (2019.207/56941). All participants and their caregivers were given verbal and written information and written informed consent was obtained from each participant’s caregiver before entering the study. DSM-IV mental disorders were determined from semi-structured clinical interview with each child’s caregiver using the Schedule for Affective Disorders and Schizophrenia for school age children-present and lifetime version (K-SADS-PL) (Kaufman et al., 2000). The cultural validity and reliability of the impairing patterns of symptoms in the First Nations group were carefully and systematically determined by First Nations mental health staff or Aboriginal Health Liaison Officers ensuring that each carer-identified pattern of symptoms and associated functional impairment was correctly interpreted. Trained interviewers (mental health staff) interviewed all the remaining caregivers of the non-First Nations young people.
An age and gender matched typically developing non-First Nations participant comparison group (N = 112) was recruited from the same 50 local primary and secondary schools to determine if full scale IQ and SAS (Taylor et al., 1986) status of the First Nations and non-First Nations clinical groups differ so they can be appropriately controlled in the analyses. This group manifested no DSM mental disorders.
Measures
The K-SADS-PL (Kaufman et al., 2000) is a structured diagnostic interview schedule based on DSM-IV criteria (0 = no information, 3 = threshold), with a parent version. It has proven clinical utility, reliability (inter-rater reliability kappa > 0.75 [kappa = 0.88 current sample]) and validity.
The Rutter and Graham Interview Schedule (Rutter et al., 1975) is a semi-structured clinical interview originally developed to ascertain mental disorders presence or absence from a parent perspective. It ascertains overall mental disorder symptom severity, symptom-linked distress and impairment rated on a 0-absent, 1-mild and 2-severe Likert-type scale. The Rutter and Graham Interview Schedule has good test–retest reliability (κ = .85), consistency (Cronbach’s α= 0.92) and concurrent validity.
The Parental Account of Childhood Symptoms (PACS) (Taylor et al., 1986) is a semi-structured clinical interview which was originally developed as an instrument for the measurement of children’s behavior problems as experienced at home. A trained interviewer administered the demographic section of the interview. A SAS scale (range 3-) was formed from a total of family income level (1–2), mother’s educational level (1–2), single parent status (0–1), sibling size (0-) and broken home status (1–2). The PACS has been demonstrated to have adequate inter-rater reliability (κ = 0.69–0.96) and Cronbach’s coefficient alphas ranged from 0.87 to 0.89.
The fourth edition of the Wechsler Intelligence Scale for Children (WISC-4) (Wechsler, 2003) was used. This provides verbal comprehension, perceptual reasoning, working memory, processing speed and full-scale scores of measured intelligence via ten core subtests. The WISC-4 is well established with valid and reliable (Cronbach’s α > 0.80) normative data.
Procedure
Testing occurred over one session (90 minutes maximum duration) with breaks as needed. Each parent and their child were assessed in separate rooms by different trained clinical researchers (a child and adolescent psychiatry Fellow; a probationary psychologist—both under approved supervision; an Aboriginal child and adolescent psychiatrist; an Aboriginal clinical psychologist; and Aboriginal Health Liaison Officers). During the session, the parent was interviewed using the PACS demographic section, Rutter and Graham Interview Schedule overall mental disorder symptom severity, symptom-linked distress and impairment scales and K-SADS-PL while his or her child completed the WISC-IV. The WISC-IV (10 core subtests) was administered by a probationary psychologist under the supervision of a registered psychologist. Paper versions of the psychometric measures were used.
Statistical analysis
Data analysis was performed using the Statistical Package for the Social Sciences (SPSS). All dimensional variables analyzed were normally distributed. Missing data were filled by contacting the participants in question. Participant demographic and key clinical characteristics were compared across the three groups using one-way analysis of variance (ANOVA). Where the omnibus F was significant, the post hoc Studentized Newman-Keuls (SNK) procedure was conducted (p < 0.05) to determine the source of this significance. Separate logistic regression analyses comparing each of the three groups to each other were conducted to determine variables that significantly predicted group membership, adjusting for SAS and FSIQ. Independent sample t-tests were used to compare the First Nations and non-First Nations clinical groups on mental disorder symptom severity, symptom-linked distress and impairment. DSM mental disorder diagnoses were compared between these two clinical groups using separate logistic regression analyses to determine diagnoses that significantly predicted group membership, adjusting for confounding by SAS and FSIQ in the multivariable model.
Results
The First Nations and non-First Nations clinical and typically developing groups did not differ for age or gender. The two clinical groups had lower full-scale IQ compared to the typically developing participants after adjusting for SAS. Similarly, the two clinical groups had higher levels of social adversity than the typically developing group after adjusting for full-scale IQ. Moreover, the First Nations group had a greater SAS than the non-First Nations clinical group. The two clinical groups did not differ on parent-reported mental disorder symptom severity, symptom-linked distress and/or impairment (see Table 1).
Key demographic and clinical factors in the (1) First Nations clinical (I), (2) non-First Nations clinical (NI) and (3) non-First Nations typically developing participant (TDP) groups.
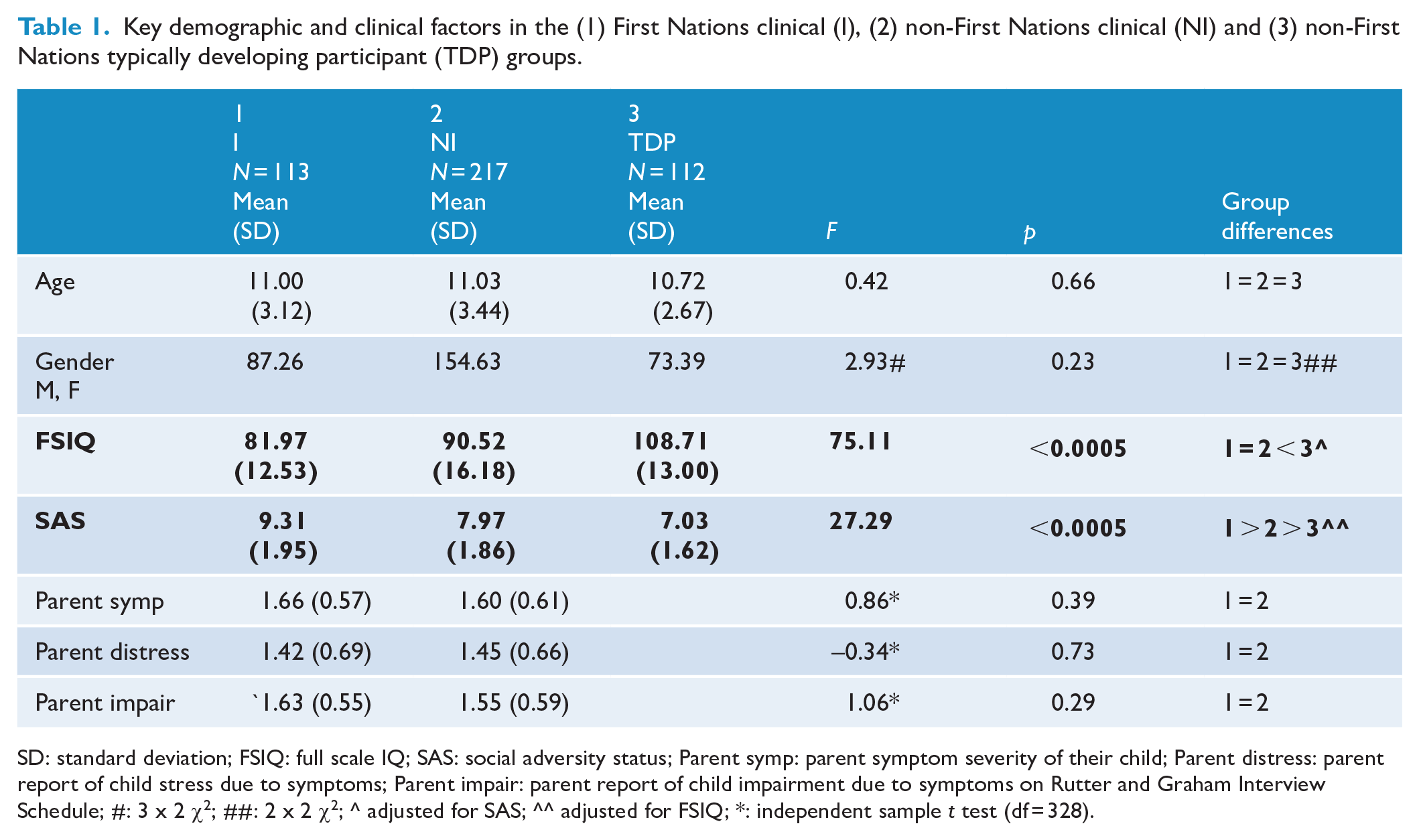
SD: standard deviation; FSIQ: full scale IQ; SAS: social adversity status; Parent symp: parent symptom severity of their child; Parent distress: parent report of child stress due to symptoms; Parent impair: parent report of child impairment due to symptoms on Rutter and Graham Interview Schedule; #: 3 x 2 χ2; ##: 2 x 2 χ2; ^ adjusted for SAS; ^^ adjusted for FSIQ; *: independent sample t test (df = 328).
ODD was the only DSM mental disorder diagnosis that differed between the two clinical groups, adjusting for confounding by SAS and FSIQ in the multivariable model. The point prevalence of ODD was 2.94 times higher (95% CI: 1.14-7.69) among the First Nations compared to the non-First Nations clinical group (see Table 2). Chen et al. (2010) suggest this is a small magnitude clinical effect. Conduct disorder approached clinical significance (p = 0.07) with odds 1.82 (95% CI: 0.95–3.45) times higher to predict group membership of the First Nations compared to the non-First Nations clinical group (see Table 2). However, there was considerable uncertainty in this estimate, reflected in wide confidence intervals, due to lower sampling precision from a smaller sample size. However, most of the confidence interval suggested that the odds were higher. All other DSM mental disorder diagnoses 95% CIs crossed unity confirming no difference between the two clinical groups. Odds ratios ranged from 1.69 (95% CI: 0.64-4.56) to 1.79 (95% CI: 0.42-7.56).
DSM Mental disorder diagnoses in the in the (1) First Nations clinical (I) and (2) non-First Nations clinical (NI) groups.
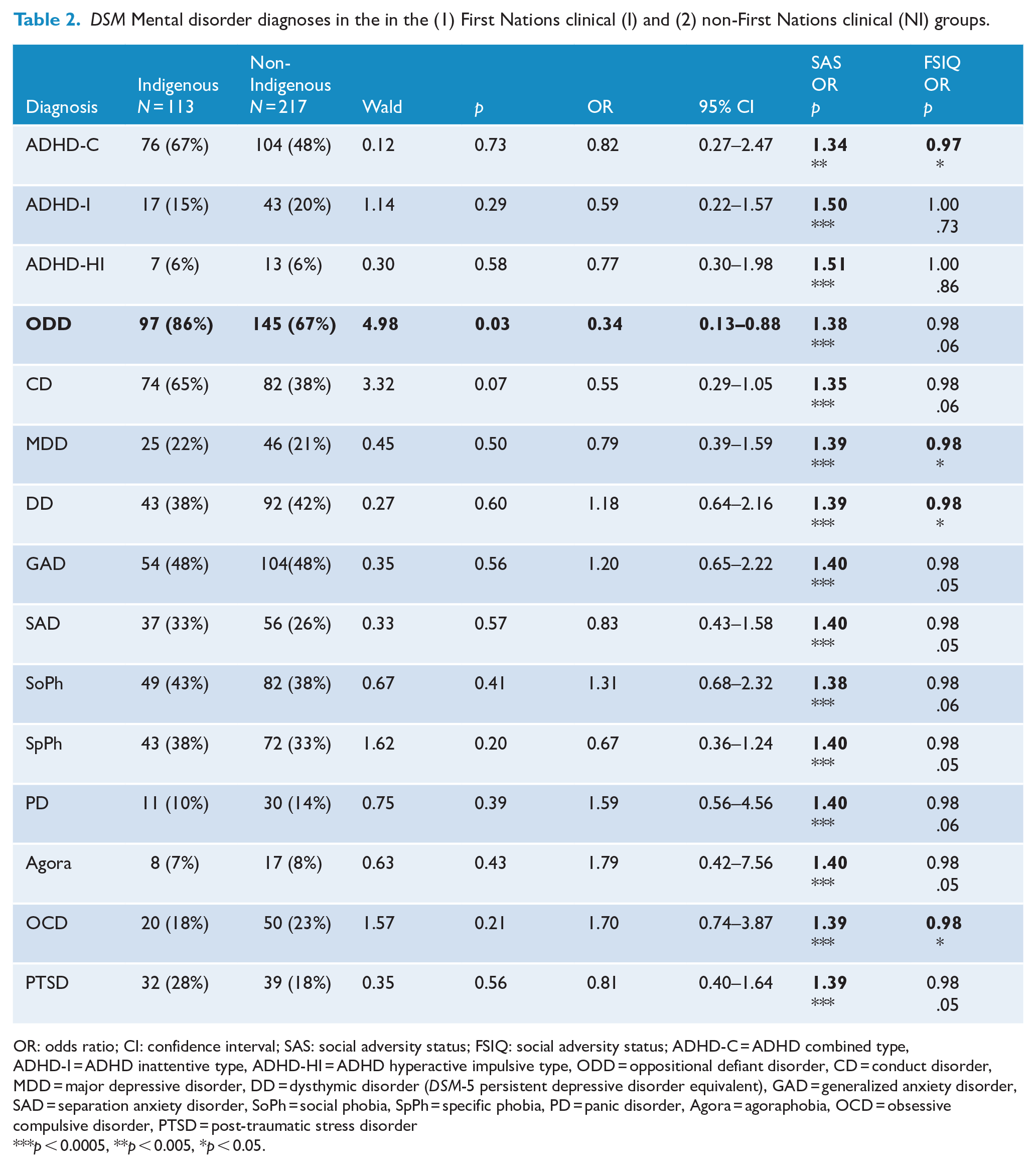
OR: odds ratio; CI: confidence interval; SAS: social adversity status; FSIQ: social adversity status; ADHD-C = ADHD combined type, ADHD-I = ADHD inattentive type, ADHD-HI = ADHD hyperactive impulsive type, ODD = oppositional defiant disorder, CD = conduct disorder, MDD = major depressive disorder, DD = dysthymic disorder (DSM-5 persistent depressive disorder equivalent), GAD = generalized anxiety disorder, SAD = separation anxiety disorder, SoPh = social phobia, SpPh = specific phobia, PD = panic disorder, Agora = agoraphobia, OCD = obsessive compulsive disorder, PTSD = post-traumatic stress disorder
p < 0.0005, **p < 0.005, *p < 0.05.
Discussion
The key demographic and clinical features of the First Nations group are consistent with the extant literature (AIHW, 2018; Turkheimer et al., 2003): higher SAS than both the non-First Nations clinical and typically developing participant groups. Also, as expected, the two clinical groups had lower full-scale IQs than the typically developing non-Indigenous comparison group, when SAS was controlled. Accordingly, both SAS and full-scale IQ were included as independent variables in all logistic regression analyses of DSM mental disorder diagnoses in the First Nations and non-First Nations clinical groups. Importantly, the two clinical groups were matched for parent-reported mental disorder symptom severity, symptom-linked distress and the degree of impairment due to the mental disorder symptoms. Their clinical homogeneity was further evident given they did not differ in the main types of clinical problems leading to their referral to mental health services, the psychological management and/or the medications trialed at the time of their referral.
Broadly speaking, the point prevalence rates of the ADHD presentations, disruptive behavior disorders, anxiety and depressive disorders in the two clinical groups were grossly elevated compared to epidemiological samples but consistent with clinic-derived samples (MacLeod et al., 1999; Verhulst, 2001). The finding of increased ODD in the First Nations young people investigated compared to the non-First Nations clinical group is consistent with Whitbeck et al.’s (2008) prior findings in American Indian and Canadian First Nations children and adolescents aged 10–12 years at base line and 13–15 years at follow-up. Importantly, in our findings, SAS and full-scale IQ were controlled to remove the effects of these confounding factors. In addition, we used First Nations mental health staff or Aboriginal Health Liaison Officers to administer the semi-structured clinical interviews, to ensure that each carer-identified pattern of symptoms and associated functional impairment was correctly interpreted and culturally valid and reliable. In contrast, Whitbeck et al. (2008) used trained First Nations interviewers who were members of the First Nations community to administer the semi-structured clinical interviews. Nevertheless, the standardized scales used in our study are not culturally valid and reliable even if delivered by First Nations staff. This is especially true for determining the different domains of Intelligence via instruments such as the Wechsler scales. Accordingly, an important future clinical research direction is undertaking this psychometric work in First Nations populations.
The extant literature is clear about identifying and managing clinically certain key risk factors for ODD, regardless of Indigeneity. Tragically, for First Nations young people, these risk factors are further intensified by the effects of intergenerational trauma linked to social policies such as the ‘Stolen Generation’ and inequitable socioeconomic status, especially in education, employment and income (AIHW, 2018): temperament (Lavigne et al., 2012), especially high negative emotionality and activity, high novelty seeking, low task persistence and effortful control, usually moderated by increased parental psychopathology (Lavigne et al., 2012) (mainly depression, ADHD, substance use disorders and antisocial personality disorder) and parenting practices (Lavigne et al., 2012) (primarily harsh parenting, increased parental control and decreased parental positive guiding and effective monitoring). Also, unstable family structures, including disruptive divorce and re-forming of family units, and family functioning deficits in behavioral, cognitive and emotional domains have been outlined (Burke et al., 2002). Importantly, ODD and parental psychopathology, ODD and parenting practices and ODD and family functioning have been shown to be bidirectional in nature (Lavigne et al., 2012). Accordingly, interactive longitudinal models of factors across these domains are being developed (Lavigne et al., 2012). Additional variables such as decreased verbal memory, increased negative emotion and poor emotional regulation and decreased social information processing and poor social relationships have been noted (Burke et al., 2002). In future studies, these variables can be examined in carefully defined and culturally valid First Nations samples of young people. Moreover, in clinical practice these variables can be identified early and become the focus of holistic cultural and psychosocial management that includes whole-of-extended family system skills training in Aboriginal Community-Controlled Health settings along with societal initiatives to correct inequities in education, employment and income. This may aid First Nations young people accessing mental health services and prevent ODD progressing to become a risk factor for them becoming involved in the criminal justice system (Greenfield et al., 2017). It is known that in children and adolescents with ODD, there is an odds ratio of 7.9 for developing CD (Rowe et al., 2010). In turn, CD in children and adolescents has an odds ratio of 2.9 for developing antisocial personality disorder in young adulthood, the most common personality disorder in criminal justice settings, regardless of Indigeneity (Rowe et al., 2010).
However, increased ODD in First Nations young people can also be understood using a variety of different lenses that focus on the sociocultural context of the clinical interviewer: Potter (2011) presents a cogent philosophical argument that ODD behaviors must be understood from the perspective of which particular group in society the interviewer and interviewee are members of. Specifically, Potter contends that there are substantial ‘hegemonic power differences’ between elite groups (e.g. educated and economically powerful settler Western groups such as health professionals) and ‘subjugated’ ‘disenfranchised’ groups (e.g. colonized First Nations groups) in our society. ODD behaviors may provide self-respect for the latter (First Nations) groups, aid them affecting change in society and also allow them to create a safe place and decolonized space in society where that can practice their Culture entirely separate from the colonizers. Indeed, in Australia, ODD behaviors could be seen as a valid part of ongoing resistance to colonization in Australia. Future qualitative work with young people with ODD might be useful to explore whether this is the case. Certainly, for Potter, ODD behaviors may indeed be virtuous, in an Aristotelian sense, for the First Nations young people. Grimmett et al. (2016) focus on interviewer bias as a key factor ‘beyond the health needs of the client’ for the diagnosis of ODD in African American males. They contend that ODD as a diagnosis creates stigma for the label itself contains a ‘negative social weight and judgment within and beyond the mental health clinical field’. They conclude that the ‘personal and professional worldview’ of health professionals needs to be reviewed as part of the diagnostic process so African American males can be diagnosed with ODD accurately and tailored psychosocial management implemented. Priest et al.’s (2018) findings concur with their view: They found in a US sample of white clinicians working with children, negative racial stereotypes were most pronounced for African American adolescents and least evident for Asian children compared to white children and adolescents. This line of evidence on sociocultural context has been incorporated into the prison Abolitionist movement (Gilmore, 2021).
The critique proffered by Potter (2011), Grimmett et al. (2016) and Priest et al. (2018) is somewhat mitigated by our First Nations young people being assessed carefully and systematically in a culturally valid and reliable manner: impairing patterns of symptoms in the Indigenous group were determined by First Nations mental health staff or Aboriginal Health Liaison Officers ensuring that each carer-identified pattern of symptoms and associated functional impairment was correctly interpreted. Nevertheless, all of our First Nations young people remain immersed in a colonized settler-dominated place, including the school and wider social spaces and places where they live their lives in their family and kinship networks. And their ODD patterns of behavior limit their access to educational opportunities and services.
In future, it would be advantageous to assess such ODD features in families and kinship networks before and after they moved from these settler-colonized contexts to First Nations self-determined places and spaces. It would be also crucial to address the disenfranchisement of the First Nations community, and the subtle biases of health professionals that may affect their clinical assessment and formulation of First Nations young people. The ‘Closing the Gap in Indigenous Disadvantage’ policy is a politically bipartisan state and federal Australian Government initiative to address the pervasive social, economic, health, welfare and criminal justice system disadvantage experienced by First Nations people (Lowitja Institute, 2021). Perhaps this policy initiative may lead to such Indigenous self-determined places and spaces being created. This may benefit and enrich Australian society as a whole.
Footnotes
Acknowledgements
We thanks our Elder’s board, especially Uncle Herb Patten and Aunty Esther Kirby for the counsel and leadership, Karen Dally for her administrative support and Janice Dally for her data entry. The reviewers aided the preparation of this manuscript greatly.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This project was funded by the Medical Research Future Fund Million Minds Program Grant (1179461). The funder of this study had no role in the study design, data collection, data analysis, data interpretation and writing of the manuscript.
Data Sharing
All Indigenous data are under the control of our governing Victorian Traditional Custodian Elder’s board. Reasonable requests made to the corresponding author will be presented to the Elder’s board and if approved data will be made available.