
Abstract
Objective:
Psychiatric patients have increased rates of comorbid physical illness. There are less data on dental disease, especially decay, despite risk factors including lifestyle and psychotropic side effects such as xerostomia. We therefore undertook an umbrella review of all meta-analyses on the association between mental illness and oral health.
Methods:
We searched PubMed, MEDLINE, PsycINFO, the Cochrane Central Register of Controlled Trials, Embase and CINAHL. Articles were independently assessed. Outcomes were caries, periodontal disease, erosion, and partial or total tooth loss (edentulism), measured where possible with standardised measures such as the mean number of decayed, missing and filled teeth or surfaces. Quality was assessed in line with National Institutes of Health guidelines.
Results:
We identified 11 meta-analyses. The most information and strongest association was between dental decay and severe mental illness or substance use, as well as erosion and eating disorders. Depressive, anxiety and eating disorders were also associated with caries, but the datasets were small. People with severe mental illness had nearly three times the odds of having lost all their teeth than the general community (odds ratio = 2.81, 95% confidence interval = [1.73, 4.57]) and those with depression between 1.17 and 1.32. Findings for periodontal disease were more equivocal, possibly because of study heterogeneity.
Conclusion:
Mental health clinicians should screen for oral diseases when treating those with mental illness and facilitate referral to affordable dental clinics when indicated. Prevention should be a priority, including the promotion of dental care, as well as the management of xerostomia when psychopharmacologic agents are prescribed.
Introduction
There has been a great deal of interest in physical and psychological comorbidity, but until recently, less focus on the impact of mental ill-health on oral health. This is despite the fact that oral health is an important aspect of overall well-being that is linked to many other chronic conditions such as diabetes, cardiovascular disease and cancer (Kisely et al., 2018). Poor oral health can also affect eating, speech, and other social and psychological areas of life (Mirza et al., 2001). The most common diseases that affect oral health are dental erosion, caries (tooth decay) and periodontal (gum) diseases.
Those with mental illness can be particularly vulnerable to dental disease. The potential causes are diverse. These can be difficulties with self-care and access to dental care (due to motivational or financial reasons), lifestyle factors (such as smoking and drinking alcohol and carbonated drinks), a direct result of the illness (such as in the case of eating disorders where vomiting causes erosion due to the acid weakening the enamel), or as a side effect of psychotropic medications (such as xerostomia – dry mouth) (Bardow et al., 2001; Lewis et al., 2001; Ramon et al., 2003).
There have been a number of meta-analyses performed in this area, with most focusing on a specific type of mental illness and one or two key dental outcomes; however, to date, this information has not been drawn together. The purpose of this umbrella review is to summarise this evidence, including a comparison of the magnitude of effect between different types of mental illness. Thus, we aim to provide a complete picture of the effect of mental illness on dental health, informing both clinicians and further research.
Methods
The protocol of this umbrella review was registered on PROSPERO (CRD42020210136). Although work is underway on developing guidelines for the reporting of umbrella reviews, there is currently limited guidance on their conduct (Pollock et al., 2019). This is particularly the case for umbrella reviews of prevalence and risk factors, as opposed to interventions. We therefore followed the recommendations of several sources to include the following steps in our umbrella review: creating a published protocol with predefined inclusion criteria, controls and outcomes; using standardised data extraction techniques; providing a description of any overlap in included meta-analyses; estimating a common effect size; and assessing study quality and heterogeneity (Aromataris et al., 2015; Fusar-Poli and Radua, 2018; Hunt et al., 2018; Pollock et al., 2020).
Dental outcomes
Dental caries, synonymous with dental decay, is tooth damage due to bacteria in dental plaque (Kisely, 2016). These bacteria produce organic acids that cause demineralisation of enamel and the dentin underneath (Kisely, 2016). It is usually measured via the ‘decayed, missing and filled teeth’ – DMFT – index (and the sub-indexes of DT, MT and FT), which has a maximum value of 32 in adults (Kisely, 2016). Another method of measuring dental decay is to look at tooth surfaces instead of the tooth as a single unit. Front teeth have four surfaces, whereas the back teeth have five, the extra one being the occlusal surface for chewing (Kisely, 2016). This adds up to a maximum value of 148 for the DMFS index (‘decayed, missing and filled surfaces’) depending on the teeth included in the count (Kisely, 2016).
By contrast, dental erosion is non-carious wear of dental hard tissue, which can occur due to mechanical wear via tooth-to-tooth contact or chemical wear due to acids (Bretz, 2002; Cormac and Jenkins, 1999).
Periodontal diseases occur due to dental plaque and affect the structures surrounding the teeth, including the gums, periodontal ligaments and alveolar bone (Williams, 1990). The earliest stage is gingivitis, which involves swollen, bleeding gums (Williams, 1990). If the inflammation then spreads to the ligaments and bone, it is called periodontitis, which involves the tissue gradually being destroyed and results in the formation of ‘pockets’ where gums have become detached from teeth (Williams, 1990).
These various diseases can eventually result in tooth loss, termed edentulism or edentulousness, which can be partial or total (Kisely, 2016).
Inclusion/exclusion criteria
We included meta-analyses that assessed the oral health of adults with mental illness. Mental illness was inclusive of substance-use disorders and could be defined clinically, by diagnostic criteria or with standardised instruments. Exclusion criteria were studies with a primary focus on dental phobia and neurodegenerative diseases such as dementia, learning disability, and alcohol and tobacco use. We also excluded studies that used oral health as the exposure variable for mental health or those that lacked quantitative synthesis of data. Finally, self-reported dental outcomes, such as those measured by a questionnaire, were excluded.
Controls were adults without mental illness, either selected for the study or from the general population. The dental outcomes of interest were dental caries, periodontal disease, edentulism and dental erosion as assessed by dental examination.
Search strategy
Systematic searches were conducted on 10 December 2020, in PubMed (inclusive of MEDLINE), Cochrane Central Register of Controlled Trials (CENTRAL), Embase, CINAHL and PsycInfo, with no restriction by language or publication date. A search of grey literature was also performed using Google Scholar by taking the first 10 pages of results (100 articles total). Keywords were searched in titles and abstracts. Index terms relating to the keywords (such as MeSH terms) were also identified and included in the search in their exploded form. A professional librarian was consulted. A detailed search strategy for each database is in Supplemental Figure S1.
After the removal of duplicates, two reviewers (J.P. and J.C.) independently screened the titles and abstracts of the retrieved records. Full-text articles were retrieved for all records identified as potentially relevant by at least one reviewer. The full-text articles were then assessed by two reviewers (S.R. and J.C.), with any conflicts being discussed and resolved with the input of other reviewers (S.K. and D.S.) if necessary.
Data extraction
Two reviewers (J.C. and J.P.) independently extracted data, with any conflict being resolved through discussion. This included authors, publication year, psychiatric population, dental outcomes, number of included articles, effect sizes with 95% confidence intervals for both pooled results and relevant subgroups, p-values, heterogeneity values (I2), results of tests for publication bias and results of key sensitivity analyses. Analyses with only one study were excluded.
We only extracted the results of random effects models where possible, converting continuous data into standardised mean differences and dichotomous variables into odds ratios. A value of greater than 50% for the I2 statistic was interpreted as evidence of heterogeneity. We did not conduct quantitative syntheses of findings across reviews because of variations in method, populations and the consideration of confounding variables.
Quality assessment and credibility of evidence
Two reviewers (J.C. and S.R.) used the National Institutes of Health (NIH) Quality Assessment of Systematic Reviews and Meta-Analyses to independently assess the quality of the included meta-analyses across the following eight domains: a focused question, the use of eligibility criteria, a comprehensive literature search, dual review, quality appraisal for internal validity, an adequate description of included studies, and consideration of both publication bias and heterogeneity. Conflict was resolved through discussion with a third reviewer (S.K.). Each meta-analysis was thus given a score out of eight and categorised as good (7–8), fair (4–6) or poor (0–3), in accordance with previous meta-reviews (Firth et al., 2020).
As the NIH scale does not take into account whether meta-analyses used adjusted or raw data, we also assessed whether the reviews considered or discussed the issue of comparability of cases and controls in terms of sociodemographic or other relevant factors. We also considered whether standardised diagnostic criteria were used for psychiatric diagnoses.
Finally, we assessed for level of evidence using criteria adapted from Fusar-Poli and Radua (2018):
Convincing (class I) when the number of cases > 1000, p < 0.00001, I2 < 50% and there are no small study effects as detected in tests for publication bias.
Highly suggestive (class II) when the number of cases > 1000, p < 0.00001, the largest study in the meta-analysis has a statistically significant effect and class I criteria are not met.
Suggestive (class III) when the number of cases > 1000, p < 0.001 and class I and II criteria not met.
Weak (class IV) when p < 0.05 and class I–III criteria not met.
Results
The initial search identified 1038 references, of which 319 were duplicates. Based on a title–abstract screen using the inclusion/exclusion criteria, 58 potentially relevant records were identified, for which the full-text articles were retrieved and examined. When there were articles with overlapping datasets, articles were excluded if 100% of the dataset was included in another article in similar subgroups. Otherwise, all the articles in question were retained, with the details of the overlap being provided in Tables 1–4. We gave preference to newer over older articles. The full-text screen eliminated 47 articles for reasons outlined in Figure 1, leaving 11 to be included in this umbrella review. Random effects models were used in all but one review, where heterogeneity was low (Table 1). The full list of excluded articles and corresponding exclusion reasons is provided in Supplemental Figure S2.
DMFT/caries.
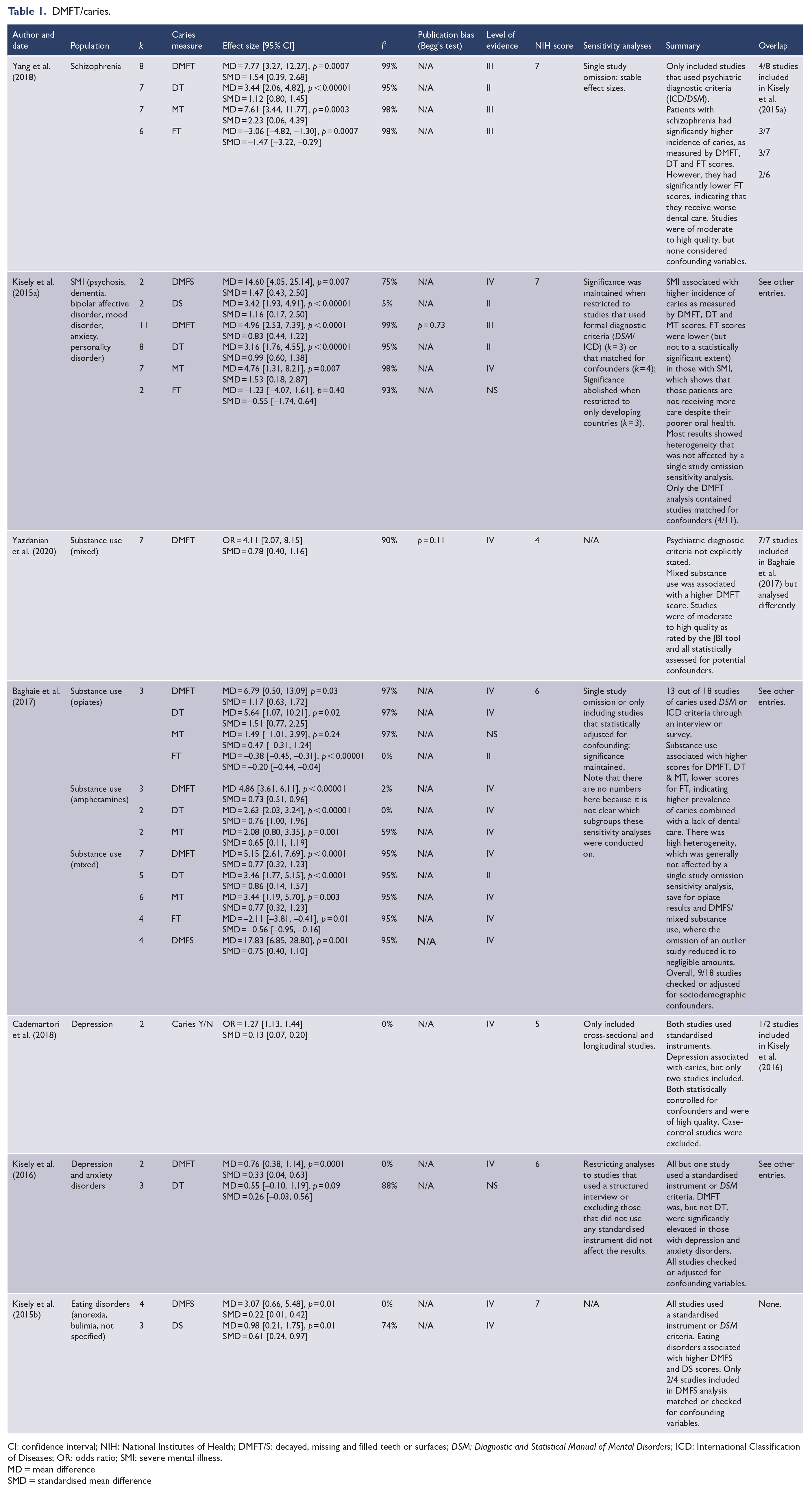
CI: confidence interval; NIH: National Institutes of Health; DMFT/S: decayed, missing and filled teeth or surfaces; DSM: Diagnostic and Statistical Manual of Mental Disorders; ICD: International Classification of Diseases; OR: odds ratio; SMI: severe mental illness.
MD = mean difference
SMD = standardised mean difference
Periodontal disease.
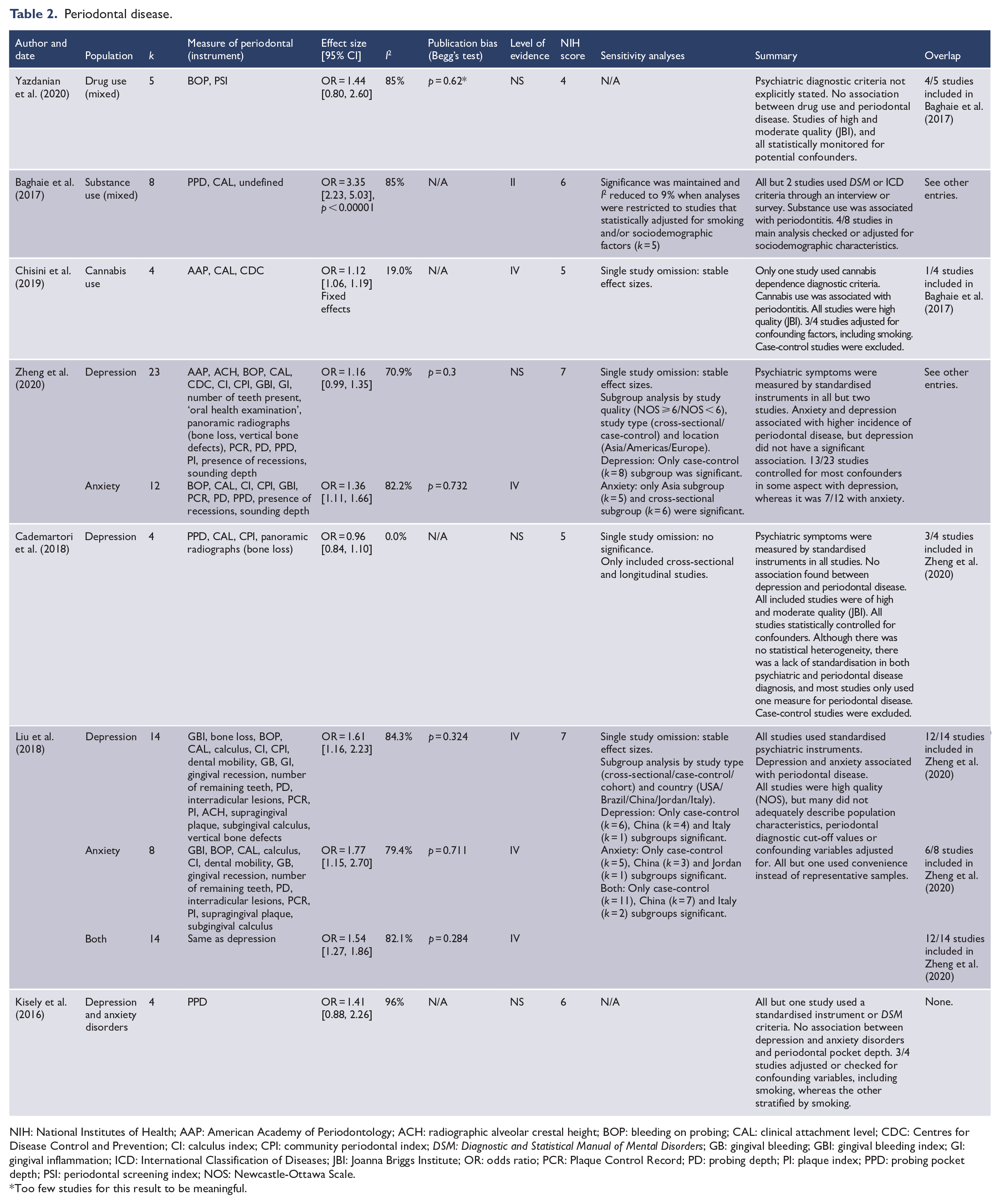
NIH: National Institutes of Health; AAP: American Academy of Periodontology; ACH: radiographic alveolar crestal height; BOP: bleeding on probing; CAL: clinical attachment level; CDC: Centres for Disease Control and Prevention; CI: calculus index; CPI: community periodontal index; DSM: Diagnostic and Statistical Manual of Mental Disorders; GB: gingival bleeding; GBI: gingival bleeding index; GI: gingival inflammation; ICD: International Classification of Diseases; JBI: Joanna Briggs Institute; OR: odds ratio; PCR: Plaque Control Record; PD: probing depth; PI: plaque index; PPD: probing pocket depth; PSI: periodontal screening index; NOS: Newcastle-Ottawa Scale.
Too few studies for this result to be meaningful.
Edentulism (partial/total).
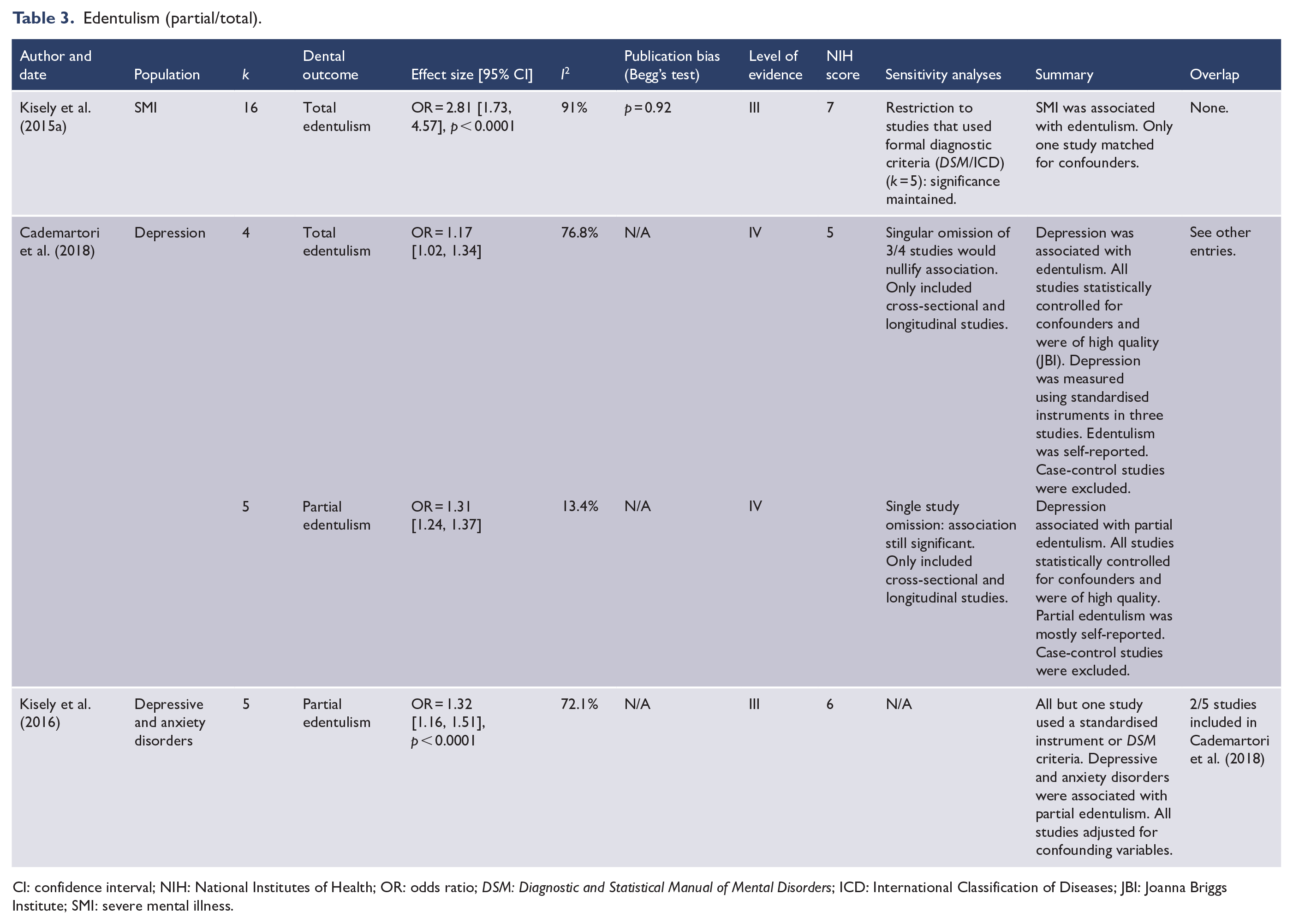
CI: confidence interval; NIH: National Institutes of Health; OR: odds ratio; DSM: Diagnostic and Statistical Manual of Mental Disorders; ICD: International Classification of Diseases; JBI: Joanna Briggs Institute; SMI: severe mental illness.
Dental erosion.
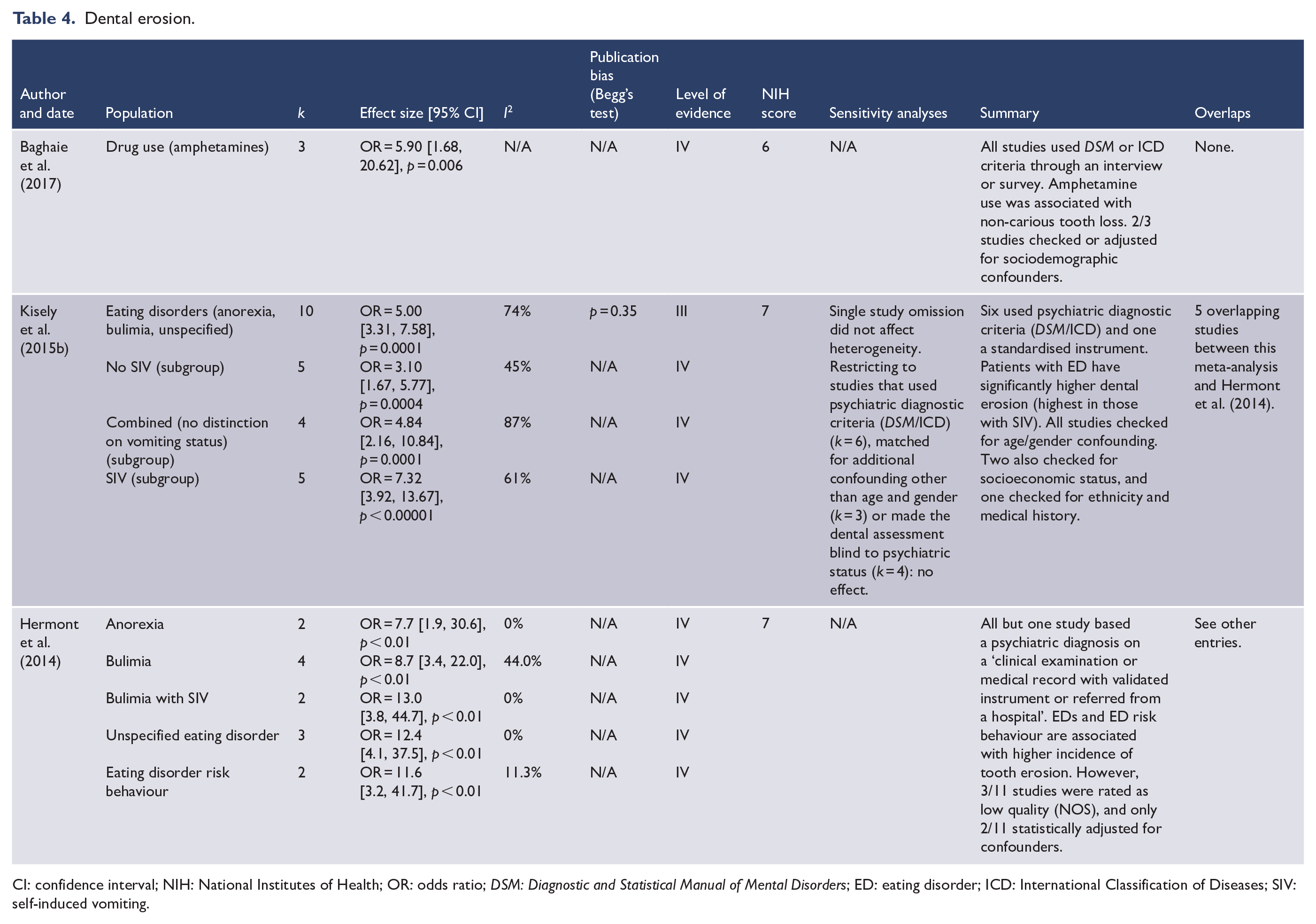
CI: confidence interval; NIH: National Institutes of Health; OR: odds ratio; DSM: Diagnostic and Statistical Manual of Mental Disorders; ED: eating disorder; ICD: International Classification of Diseases; SIV: self-induced vomiting.
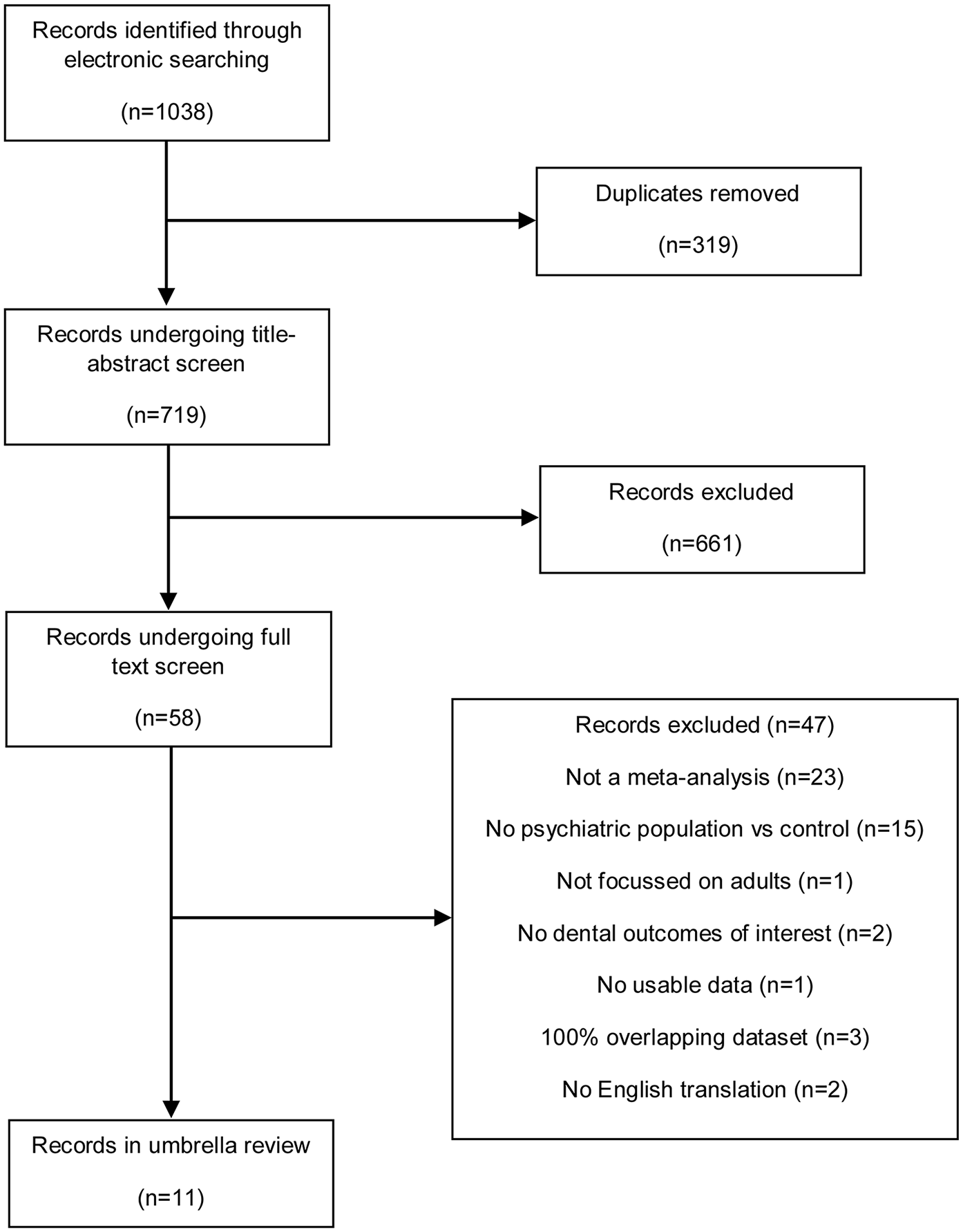
PRISMA diagram.
Quality and credibility of evidence
The meta-analyses ranged from fair to good quality, as per the NIH scale. Common issues were a lack of a manual search to supplement the electronic literature search, insufficient discussion of the possibility of publication bias and inadequate justification for excluding case-control studies. Furthermore, four meta-analyses provided a discussion of the quality of included studies, but individual ratings for each study using a standardised instrument were not provided.
As noted previously, the NIH scale does not take into account whether the meta-analyses used adjusted or raw data. The extent to which studies in a particular meta-analysis accounted for confounders is described in detail in Tables 1–4. Only two meta-analyses explicitly stated that they used adjusted results over raw (Chisini et al., 2019; Yazdanian et al., 2020). All meta-analyses discussed confounding variables, but this was to varying degrees, making it difficult to compare or combine results. Some meta-analyses reported which studies controlled for confounding but did not provide any description of the variables considered (Kisely et al., 2015a; Yazdanian et al., 2020; Zheng et al., 2020). Others reported the specific confounders that were statistically adjusted for, but did not mention other methods of controlling for confounding variables (Cademartori et al., 2018; Hermont et al., 2014). One stated that no included studies accounted for confounders (Yang et al., 2018). Four meta-analyses provided sufficient detail – reporting which studies checked, matched and adjusted for confounders, as well as listing all the variables taken into account for each study (Baghaie et al., 2017; Chisini et al., 2019; Kisely et al., 2015b, 2016). Only one meta-analysis solely reported fixed effects models (Chisini et al., 2019)
Only one meta-analysis did not explicitly comment on how psychiatric diagnoses were derived, and whether these were based on standardised instruments or diagnostic criteria (Yazdanian et al., 2020). However, there was a lack of standardisation in how symptoms were measured, and the use of diagnostic criteria from either the International Classification of Diseases (ICD) or Diagnostic and Statistical Manual of Mental Disorders (DSM). Where ICD or DSM criteria were used, this was usually by a clinical assessment and not by standardised psychiatric interview (Kisely et al., 2015a, 2015b). For substance use, the duration or recency of use was sometimes unclear, as was the distinction between use, use disorder and dependence. Diagnostic criteria for periodontal disease were also highly variable. Even within the same criterion, cut-off values varied. This may explain why the results for periodontitis were more equivocal than other dental outcomes. Finally, blinding or training of the dental assessor to psychiatric status was rarely mentioned, and most meta-analyses did not state the mean age or the proportion of males and females.
The level of evidence was strongest for dental decay and edentulism in severe mental illness (SMI) (Tables 1 and 3). For other psychiatric disorders and dental outcomes, it was only weak to suggestive or not significant (Tables 1–4).
Dental caries
There were seven meta-analyses on caries, all of which reported data derived from DMFS or DMFT indices (Table 1). Statistical heterogeneity was generally high (Table 1). The strongest association was for SMI, where both meta-analyses reported significant findings with relatively large effect sizes – whether this was specifically in schizophrenia (Yang et al., 2018) or for SMI in general (Kisely et al., 2015a). Breaking down the index revealed that DT and MT values were also significantly higher, but FT was lower, with the difference statistically significant for schizophrenia (Table 1). This indicates that despite poorer dental health, people with SMI are not receiving the care that they need. The review on SMI had sufficient studies to reasonably test for publication bias and found no evidence of it via Begg’s test (Kisely et al., 2015a).
Regarding substance use, similar results emerged, with both meta-analyses finding a higher incidence of caries, across the subgroups of opiates, amphetamines and mixed substances (Baghaie et al., 2017; Yazdanian et al., 2020). As in SMI, DMFT, DT and MT scores were generally elevated, whereas FT scores were lower in people who used drugs (Table 1).
There was less information on common mental illnesses such as anxiety and depression, with there being only two reviews, altogether containing five unique studies (Table 1). A review of depressive and anxiety disorders returned equivocal results, with an association found for DMFT but not DT (Kisely et al., 2016). The other review found a small but statistically significant association between depression and caries (Cademartori et al., 2018).
Only one review analysed the association between eating disorders and caries (Kisely et al., 2015b). There was a significant association for both DMFS and DS scores, although to an extent much smaller than that of SMI or substance use (Table 1).
Periodontal disease
As in caries, there were seven included meta-analyses (Table 2). Outcomes were summarised as odds ratios of dichotomous variables (Table 2). Statistical heterogeneity was high in all but two comparisons (Table 2). In addition, and in contrast to the other dental outcomes, there was a wide variation in the included studies as to how periodontal disease was assessed (Table 2). The association with substance use was strongest, where two of the three reviews found a significant result. One was restricted to cannabis (Chisini et al., 2019), while the other included a range of substances (Baghaie et al., 2017). However, a third review of mixed substance use that was restricted to higher quality studies did not find a significant association (Yazdanian et al., 2020).
Two meta-analyses found a significant association with anxiety (Liu et al., 2018; Zheng et al., 2020). However, in the case of one, the association was weak and disappeared when the analysis was restricted to high-quality studies (Zheng et al., 2020).
By contrast, depression was not significantly associated with periodontal disease in three out of four meta-analyses (Table 2), including the largest and most recent one (k = 25) (Zheng et al., 2020). In the one review that reported a significant association, the results were heavily influenced by two studies from China, both of which had noticeably higher odds ratios than the other included studies (Liu et al., 2018). The findings were no longer significant when these were excluded (Liu et al., 2018).
Where applicable, none of the reviews reported statistically significant publication bias (Table 2).
Partial and total edentulism
There were three meta-analyses on edentulism, which were summarised as odds ratios, and all of which showed an association with mental illness (Table 3). The largest meta-analysis (k = 16) found an association with SMI that was robust to publication bias, but had high heterogeneity (Kisely et al., 2015a).
A meta-analysis found that depression was associated with both partial and total edentulism (Cademartori et al., 2018). Statistical heterogeneity was low in partial edentulism, but the total edentulism had high heterogeneity and the association was nullified in a single study omission sensitivity analysis (Table 3). When examined in combination, depression and anxiety disorders were also associated with edentulism (Kisely et al., 2016). Overall, as seen with the results for caries, common mental disorders had a smaller effect size than SMI (Table 3).
Erosion
Similarly, there were three meta-analyses on erosion all summarised as odds ratios: one on substance use and two on eating disorders (Table 4). Amphetamine use was associated with non-carious tooth loss (Baghaie et al., 2017).
Both reviews on eating disorders found an association with tooth erosion across subgroups of anorexia, bulimia, bulimia with self-induced vomiting (SIV), unspecified eating disorders and eating disorder risk behaviour (Table 4). The overall result in one review was robust against publication bias and had moderate heterogeneity (Kisely et al., 2015b). Subgroup analysis based on SIV status showed that those with SIV had worse outcomes (Kisely et al., 2015b). The meta-analyses in the other review had low heterogeneity, but each only contained a small number of studies (Hermont et al., 2014).
Discussion
Disparities in oral ill-health receive less attention than those in other chronic illnesses, even though dental disease is significantly higher in people with psychiatric and substance-use disorders – especially SMI. Explanations include smoking, poverty and reduced access to dental care. In the case of opiate-use disorders, this can be exacerbated by the use of methadone preparations with high sugar content. Similarly, most psychotropic medications can exacerbate dry mouth, as do recreational substances such as opiates, cocaine and amphetamines. Ultimately, dental disease can lead to chronic inflammatory processes such as diabetes and cardiovascular disease that contribute to systemic medical morbidity and ultimately reduced life expectancy. To our knowledge, this is the first umbrella review to comprehensively assess the four main dental outcomes across a range of psychiatric and substance-use disorders.
Table 5 summarises the strength of evidence for the association between each dental outcome and all the psychiatric diagnoses. In general, the most information and strongest association was between dental decay and SMI or substance use. The largest effect size was for people with schizophrenia, who had, on average, eight more DMFT compared to healthy controls. Notably, patients with SMI and those who used substances had more decayed and missing teeth, but less filled teeth, suggesting that there are barriers to dental treatment despite the greater need. This finding was mirrored by an almost threefold likelihood of total edentulism in patients with SMI. Depressive, anxiety and eating disorders were also generally associated with caries, but the datasets were small.
Summary.
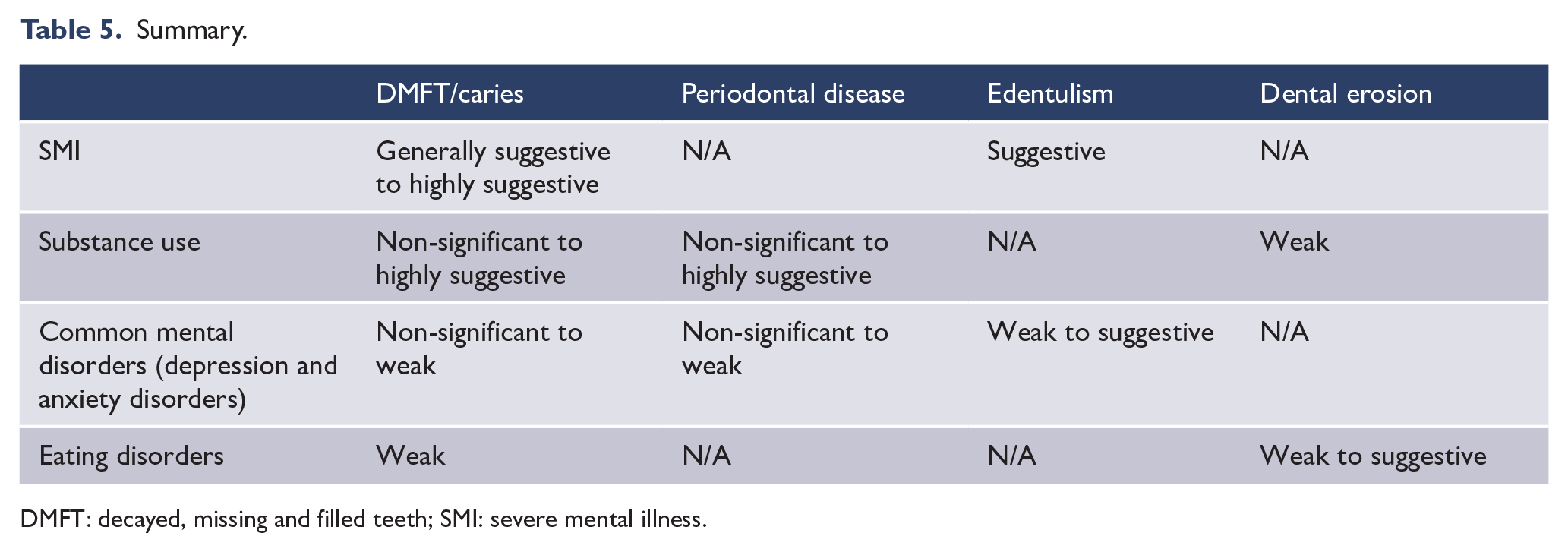
DMFT: decayed, missing and filled teeth; SMI: severe mental illness.
There was less information on other outcomes. For periodontal disease, there were only meta-analyses of either substance use or common mental disorders (depression/anxiety). Two reviews on substance use found a significant association. However, a third that only included higher quality studies did not. Both meta-analyses on anxiety found an association with periodontitis. By contrast, there was a lack of evidence supporting an association between depression and periodontitis. A possible explanation is the wide variability in the diagnostic criteria and thus results of included studies.
Dental erosion was significantly more likely in amphetamine users and patients with eating disorders. In the case of the former, this was due to substances such as amphetamines or cocaine causing bruxism (teeth grinding). However, it is important to note that this was limited to a single meta-analysis of three studies. There was more literature on eating disorders, and this finding is explained by weakened enamel arising from exposure to both carbonated soft drinks and acidic stomach contents following SIV. Consequent tooth brushing causes further mechanical wear of enamel.
The end result of untreated dental disease, such as caries and periodontitis, is edentulism. There were only three reviews of this outcome, but all three found a significant association with mental illness, with the effect size in SMI being markedly higher than that in common mental disorders.
There are several limitations to this umbrella review. First, there were wide variations in both the included reviews and contributing studies in method, populations and the consideration of confounding variables. As noted previously, the results on periodontitis should particularly be interpreted with caution, given variations in the measurement of periodontal disease and, in the case of depression, the consistency of results. There was a low number of contributing studies for some of the associations, such as between substance-use disorders and erosion. Other recurring issues for all outcomes included a lack of dental assessor training and blinding to psychiatric status.
Although the conduct of the meta-analyses was rated as mid to high quality by NIH criteria, many of the results had high heterogeneity, and low numbers of contributing studies limited the assessment of publication bias. All these factors contributed to weak or suggestive levels of evidence for most associations between psychiatric disorders and dental outcomes. The only exception was for dental decay and edentulism in SMI, where scores ranged from suggestive to highly suggestive.
All included meta-analyses had some degree of overlap in their dataset, and three more were excluded because of 100% overlap in datasets (Figure 1). For some of the outcomes, there were as many meta-analyses as contributing studies. This oversaturation highlights the need for the prospective registrations of protocols in an external registry such as PROSPERO that is maintained, monitored and enforced.
Finally, several of the included meta-analyses were authored by authors of this umbrella review (S.K. and D.S.). However, to reduce risk of bias, study selection and quality appraisal were undertaken by three of the other authors (J.C., J.P. and S.R.).
Implications
Our findings highlight the association between mental illness and oral health, in particular areas such as dental decay across a range of psychiatric diagnoses and erosion with eating disorders. This, in turn, can result in partial or total tooth loss.
Problems related to oral heath range from discomfort and impaired function to social withdrawal resulting from painful, unsightly dentition or ill-fitting dentures. Overall, this can have a severe impact on quality of life. For instance, the Global Burden of Disease Study rates severe tooth loss as leading to an equivalent disability as moderate coronary failure (Marcenes et al., 2013). Oral conditions appear frequently among the top 100 causes of disability, with untreated decay being the 10th most prevalent condition, affecting 10% of the world’s population (Marcenes et al., 2013). Dental disease also contributes to systemic medical morbidity. Although some of this is due to common risk factors such as smoking, bacterial colonisation secondary to poor oral hygiene and dry mouth from psychotropic medications are also factors. The rich blood supply to the oral cavity enables the systematic spread of bacteria and associated immune complexes that, in turn, can cause inflammation in organs such as the myocardium, liver and pancreas (Beck and Offenbacher, 2005; Kisely, 2016).
Dental disease is also responsible for a fifth of acute admissions to hospital that could have been avoided with appropriate primary care (Glover et al., 2008). People with mental illness are at greater risk of both these admissions and avoidable Emergency Department presentations for non-traumatic dental problems (Kisely et al., 2015c, 2021).
In terms of clinical implications, mental health clinicians should screen for oral diseases when treating those with mental illness using standard checklists that can be completed by non-dental personnel, as well as facilitate referral to affordable dental clinics when indicated. People should also be advised on the management of xerostomia when prescribed psychotropic drugs, and this side effect should be considered in the choice of agent (Kisely et al., 2018). Management strategies include frequent sips of water throughout the day and the use of artificial salivary products, mouthwashes or topical fluoride applications. Patients should also reduce the consumption of caffeinated, acidic or carbonated drinks, as well as alcohol and tobacco. People with eating disorders should avoid vigorous brushing after SIV.
In the other direction, closer collaboration between dental and mental health professionals is also important. For instance, dental services need to recognise the specialised needs of people with mental illness, including longer appointment times to allow greater time for explanation, counselling and the performance of procedures. Dentists may also be the first clinician to suspect a psychiatric diagnosis such as an eating disorder (Lo Russo et al., 2008).
In terms of research implications, there should be an increased focus on standardising diagnostic criteria for both the exposure (mental illness) and outcome (dental diseases), particularly in the area of periodontal disease, as well as greater uniformity in the reporting of results.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211042239 – Supplemental material for Prevalence of dental disorders among people with mental illness: An umbrella review
Supplemental material, sj-docx-1-anp-10.1177_00048674211042239 for Prevalence of dental disorders among people with mental illness: An umbrella review by Jisu Choi, Josh Price, Samuel Ryder, Dan Siskind, Marco Solmi and Steve Kisely in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-2-anp-10.1177_00048674211042239 – Supplemental material for Prevalence of dental disorders among people with mental illness: An umbrella review
Supplemental material, sj-docx-2-anp-10.1177_00048674211042239 for Prevalence of dental disorders among people with mental illness: An umbrella review by Jisu Choi, Josh Price, Samuel Ryder, Dan Siskind, Marco Solmi and Steve Kisely in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Jisu Choi was partly funded by the University of Queensland Summer Scholar Research Programme and Dan Siskind is funded in part by an NHMRC Emerging Leadership Fellowship (GNT 1194635).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.