
Abstract
Background and Objectives:
Evidence indicates that mood disorders often co-occur with substance-related disorders. However, pooling comorbidity estimates can be challenging due to heterogeneity in diagnostic criteria and in the overall study design. The aim of this study was to systematically review and, where appropriate, meta-analyse estimates related to the pairwise comorbidity between mood disorders and substance-related disorders, after sorting these estimates by various study designs.
Methods:
We searched PubMed (MEDLINE), Embase, CINAHL and Web of Science for publications between 1980 and 2017 regardless of geographical location and language. We meta-analysed estimates from original articles in 4 broadly defined mood and 35 substance-related disorders.
Results:
After multiple eligibility steps, we included 120 studies for quantitative analysis. In general, regardless of variations in diagnosis type, temporal order or use of adjustments, there was substantial comorbidity between mood and substance-related disorders. We found a sixfold elevated risk between broadly defined mood disorder and drug dependence (odds ratio = 5.7) and fivefold risk between depression and cannabis dependence (odds ratio = 4.9) while the highest pooled estimate, based on period prevalence risk, was found between broadly defined dysthymic disorder and drug dependence (odds ratio = 11.3). Based on 56 separate meta-analyses, all pooled odds ratios were above 1, and 46 were significantly greater than 1 (i.e. the 95% confidence intervals did not include 1).
Conclusion:
This review found robust and consistent evidence of an increased risk of comorbidity between many combinations of mood and substance-related disorders. We also identified a number of under-researched mood and substance-related disorders, suitable for future scrutiny. This review reinforces the need for clinicians to remain vigilant in order to promptly identify and treat these common types of comorbidity.
Introduction
Comorbidity between different types of mental disorders is common and more pervasive than previously thought (i.e. each type of mental disorder is associated with an increased risk of subsequently developing most other types of mental disorders; McGrath et al., 2020; Plana-Ripoll et al., 2019; Saha et al., 2021). Evidence from a series of community surveys based on World Health Organization International Consortium in Psychiatric Epidemiology showed significant comorbidity between various mental disorders (e.g. mood disorders) and substance-related disorders (Kessler, 2004). In a trans-national study based on 27 countries, McGrath et al. (2020) found substantial pairwise comorbidity between depression and alcohol dependence (ALD), regardless of whether depression was the prior disorder (hazard ratio [HR] = 15.8; 95% confidence interval [CI] = [14.4, 17.4]) or the later disorder (HR = 12.0; 95% CI = [11.1, 13.0]). A Danish register-based study (n = 5,940,778) (Plana-Ripoll et al., 2019) found that the associations between broadly defined mood disorder and substance abuse (SA) were bidirectional; those with a prior diagnosis of mood disorder had eightfold risk of subsequently developing SA within 5–10 years (HR = 8.4; 95% CI = [8.0, 8.7]) while those with prior SA had sixfold risk of subsequently developing mood disorder (HR = 6.6; 95% CI = [6.3, 6.9]). Recent systematic reviews based on prospective studies also found temporally ordered association between mood and substance-related disorders (Esmaeelzadeh et al., 2018; Li et al., 2020). While the evidence supports substantial comorbidity between mood and substance-related disorders, the risk estimates can vary depending on study types as well as various study design features (e.g. diagnostic criteria).
In recent years, several systematic reviews have focused on comorbid mood and substance-related disorders. Most of these studies were based on cross-sectional studies (Hunt et al., 2016b; Lai et al., 2015; McKetin et al., 2019; Mathew et al., 2017; Messer et al., 2017; Pinto et al., 2019); however, only a few used temporally ordered longitudinal data (Esmaeelzadeh et al., 2018; Fluharty et al., 2017; Li et al., 2020; Mammen et al., 2018). While these reviews showed substantial comorbidity, most were focused on selected comorbid pairs and/or a limited number of studies, used symptom-based (Hussong et al., 2017; Kingston et al., 2017) or estimates based on studies with a mix of symptom-based and diagnostic criteria. The pooling of comorbidity estimates can be challenging because of heterogeneity in study design and between-site variations in the prevalence of the underlying disorders. There is a need for a more comprehensive systematic review and meta-analysis that (a) takes into account a comprehensive range of mood- and substance use disorders, broad or narrow diagnostic criteria (e.g. any type of broad depression-related disorder, specific depression-related disorder); (b) provides pooled estimates based on period of observation (e.g. lifetime or period prevalence that does not take temporal order into account, or temporally ordered estimates) and (c) adjustments of covariates (unadjusted risk estimates, or estimates adjusted for a range of covariates; e.g. sex, age). The aims of the current systematic review are to provide an up-to-date list of studies that have examined comorbidity between broadly defined mood- and substance-related disorders and to meta-analyse the risk estimates according to various key design features.
Method
Search strategy and identification of studies
This systematic review is based on protocol registered with PROSPERO (PROSPERO 2019 CRD42019080516) (Saha et al., 2021) following the search strategy of our recently published meta-analysis of mood and anxiety disorders (Saha et al., 2021). We followed PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) (Moher et al., 2015; Shamseer et al., 2015) guidelines as shown in Supplemental PRISMA Checklist. To ensure a comprehensive search, two researchers (J.J.M., S.S.) independently validated and revised search algorithms for identifying research publications on comorbidity of mood and substance-related disorders across four electronic databases: PubMed-Medline, Embase, CINAHL and Web of Science, between 1 January 1980 and 30 December 2017 (Methods S1). No restrictions were made regarding geographical location or language of publications.
Screening, snowball searching and data extraction
Based on inclusion and exclusion criteria, studies extracted from four database searches were uploaded into a commercial software, Covidence (www.covidence.org/) for Title and Abstract (TIAB) screening. The inclusion criteria include (1) studies based on general human population, (2) studies that report an association in the form of risk ratio or equivalent (i.e. HR, relative risk, odds ratio [OR]) and corresponding variance or provide data for calculating the estimates, (3) peer-reviewed articles using case-control, cohort or cross-sectional studies, and (4) studies with clear diagnostic criteria (International Classification of Diseases [ICD]/Diagnostic and Statistical Manual of Mental Disorders [DSM], etc.). We did not include studies with sub- or ‘special’ populations (e.g. prison, homeless, veterans, any illness group or experimental groups), genetic studies or reviews (e.g. narrative, scoping or systematic reviews). We conducted a snowball search for additional articles (details are in Methods S2.1).
We collected information on (1) study characteristics (author, year, site, etc.), (2) methodology (sample size used, diagnostic criteria, type of mood and anxiety disorder, etc.) and (3) risk estimates (ORs, HRs). In general, we extracted data from studies that provided (1) both cross-sectional and temporally ordered risk estimates (e.g. OR, HR, risk ratio) and (2) both unadjusted and adjusted estimates. We also extracted data from cohort studies that provided sufficient information (i.e. numbers of people with an index disorder and those without) to allow the calculation of crude ORs. These estimates were considered as unadjusted estimates.
Data were extracted into an Excel spreadsheet based on various aspects of study characteristics (author, year, site, diagnostic criteria, type of mood and substance-related disorders, risk estimates, etc.). In general, we extracted data from studies that provided (1) both cross-sectional and temporally ordered risk estimates (e.g. OR, risk ratio) and (2) both unadjusted and adjusted estimates. We also extracted data from studies that provided enough information to allow the calculation of ORs, which were considered as unadjusted estimates. For uniform presentation, we used pooled OR as our primary risk measure, as more than 95% studies reported ORs.
Operationalized features: diagnostic criteria, sequential filters and quality reporting scale
Several operationalized features were used in keeping with our previous systematic reviews (McGrath et al., 2004; Saha et al., 2005, 2007, 2021) and followed standard systematic review guidelines (von Elm et al., 2007). The first operationalized feature was to use studies with defined diagnostic criteria (e.g. ICD, DSM or other published criteria) for case definitions for both mood and substance-related disorders. Details of diagnostic instruments are in Methods S3. Second, to identify discrete data from overlapping studies, we used two types of filters, a ‘study-level filter’ and an ‘estimate-level filter’. The former delineated overlapping studies, while the latter parsed overlapping estimates between studies (Methods S2.4). Using the study-level filter, we excluded 43 papers that completely overlapped in time and place. In keeping with our previous meta-analysis (Saha et al., 2021) and our published protocol (Saha et al., 2021), we developed a ‘Quality Reporting Scale’ (QRS) to assess overall quality of the study estimates using 14 criteria (see Methods S4) (McGrath et al., 2004; Saha et al., 2021).
As expected, we found a wide variety of disorder labels in mood and substance-related disorders. In order to make the meta-analysis tractable, we combined similar disorder terms into ‘broad’ categories. For example, we used ‘broadly defined mood disorder’ (henceforth ‘MOOD’) for studies that included a mix of any mood disorders. Similarly, we used ‘broadly defined depressive disorder’ (henceforth ‘DEP’) for any depressive disorders, ‘broadly defined dysthymic disorder’ (henceforth ‘DYS’) for any dysthymic disorders, and ‘broadly defined bipolar disorder’ (henceforth ‘BIPOLAR’) for any bipolar disorders. We also used abbreviations for 35 different types of substance-related disorders (details are in Methods S5).
Data analysis and presentation
We reported meta-analysed risk estimates (i.e. pooled ORs) using random-effect models based on the inverse-variance method. We also summarized the findings in a narrative fashion for disorder pairs that were below our threshold for meta-analysis (less than three estimates). In keeping with our registered protocol (Saha et al., 2019) for assessing publication bias, we inspected funnel plots with Egger’s test (Egger et al., 1997) for disorder pairs with a sufficient number of studies (>10) (Methods S2.5). In addition, we assessed the heterogeneity of the studies by using Q-statistic and I2 (DerSimonian and Laird, 1986, 2015). Details are available in Methods S3.5. To avoid bias, pooled estimates were divided into three different groups (based on timing): (1) lifetime prevalence (i.e. the presence of the two disorders at any time across the lifespan), (2) period prevalence (i.e. the presence of the two disorders within a period of 1, 3, 6 and 12 months) that did not take into account temporal ordering (i.e. which of the two disorders came first) and (3) temporally ordered estimates related to cross-sectional, case-control or cohort studies (i.e. the ages of onset for the two disorders are known). We also divided pooled estimates based on adjusted or unadjusted estimates to reduce heterogeneity (Peters and Mengersen, 2008). Thus, we presented separate pooled estimates based on these 5 categories for the main 4 mood disorders (MOOD, DEP, DYS and BIPOLAR) together with 35 different types of substance-related disorders.
We used the ‘metafor’ (package=‘metafor’) in R (R Core Team, 2017) to derive the pooled estimates, forest and funnel plots. ORs from each study were transformed using natural logarithm, and standard errors (SEs) were calculated from the reported CIs. In studies with missing CIs, reported p-values were used to calculate SEs. Comorbidity between pairwise disorders was presented as pooled risk estimates using unadjusted OR or adjusted odds ratio (aOR) for disorder pairs with three or more studies. All data underlying meta-analyses codes can be found at: https://github.com/uqssaha3/Saha2021. We present meta-analysed pooled estimates in tables and forest plots, while individual pairwise association data are presented in Supplementary Tables S2–S10.
Results
Search results
The PRISMA flow diagram is shown in Figure 1, and additional details are presented in Methods S1–S2. After the removal of duplicates and excluding 37,393 through TIAB screening, 187 studies were included for full-text reviews. After further exclusion of 67 studies for various reasons (Figure 1), 120 studies were included in the quantitative synthesis. From these, we were able to generate 56 pooled estimates including 52 unidirectional lifetime and period prevalence risk estimates and 4 temporally ordered estimates.
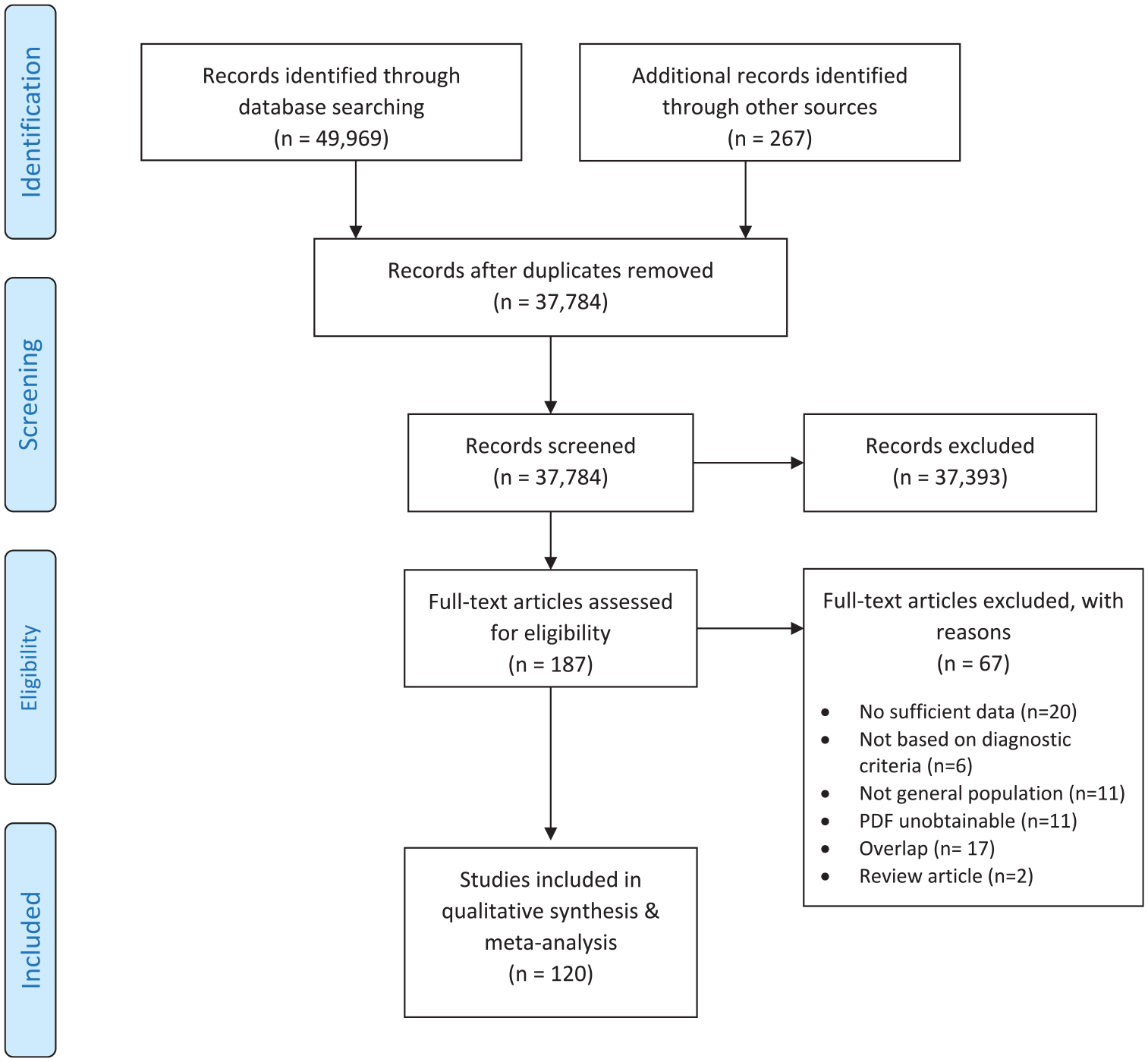
PRISMA flow diagram (selection strategy) of included studies.
Study characteristics of the 120 studies that provided lifetime, period prevalence and temporally ordered estimates are shown in Supplementary Table S1.
Pooled estimates for pairwise associations
Pooled estimates based on separate pairwise meta-analysis of mood- and substance-related disorders are presented in Tables 1–4. In these tables, we show estimates for pairs with pooled meta-analytic data and leave blank the combinations where data were not available (to guide future research). By way of example, we present three informative forest plots (Figures 2–4) in the main text, while other forest plots (n = 53) and funnel plots (n = 5) are presented in Supplementary Figures S2–S59. For disorder pairs that had insufficient information for meta-analyses (i.e. less than 3 estimates), we summarized the findings in Supplementary Tables S2–S10. Full details of the studies contributing to each of the broad group meta-analyses can be found in Supplementary References (S1–S27).
Pooled estimates for broadly defined mood disorder (MOOD) and substance-related disorders.
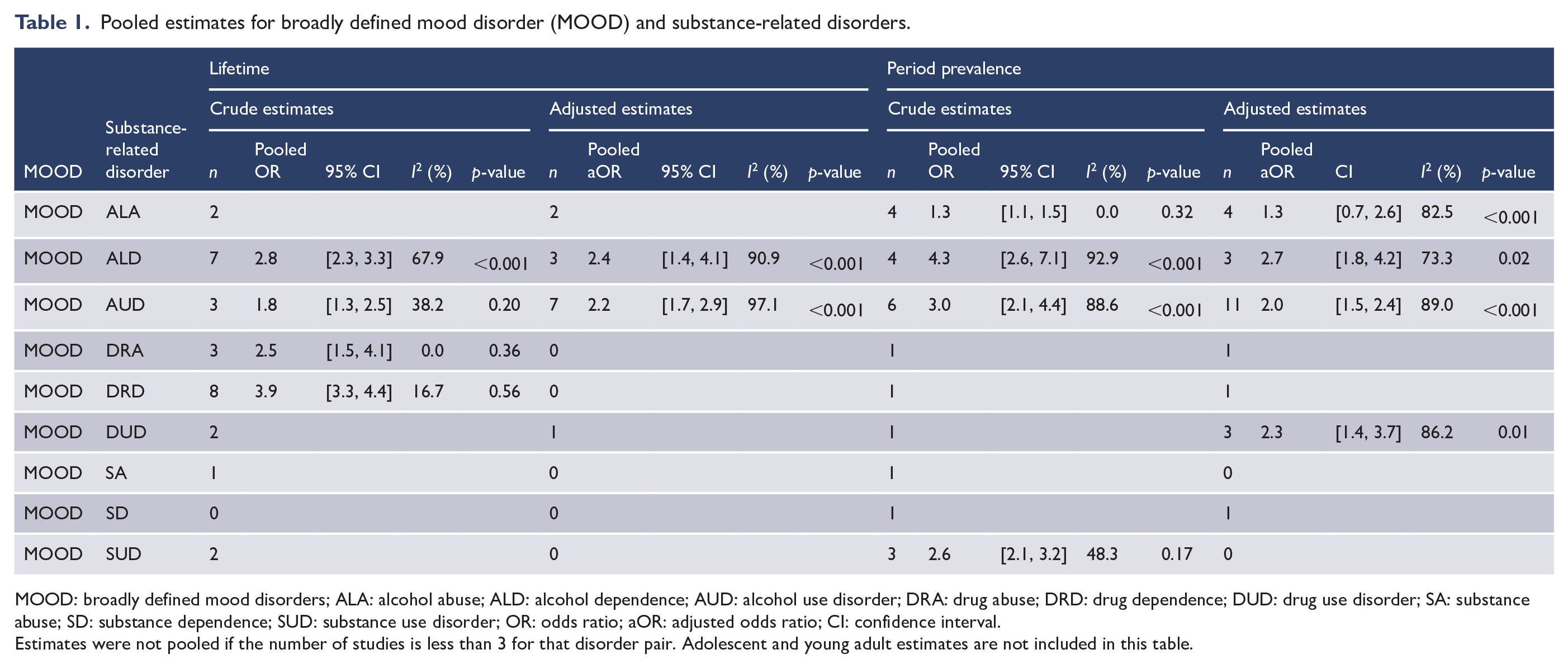
MOOD: broadly defined mood disorders; ALA: alcohol abuse; ALD: alcohol dependence; AUD: alcohol use disorder; DRA: drug abuse; DRD: drug dependence; DUD: drug use disorder; SA: substance abuse; SD: substance dependence; SUD: substance use disorder; OR: odds ratio; aOR: adjusted odds ratio; CI: confidence interval.
Estimates were not pooled if the number of studies is less than 3 for that disorder pair. Adolescent and young adult estimates are not included in this table.
Pooled estimates for broadly defined depression (DEP) and substance-related disorders.
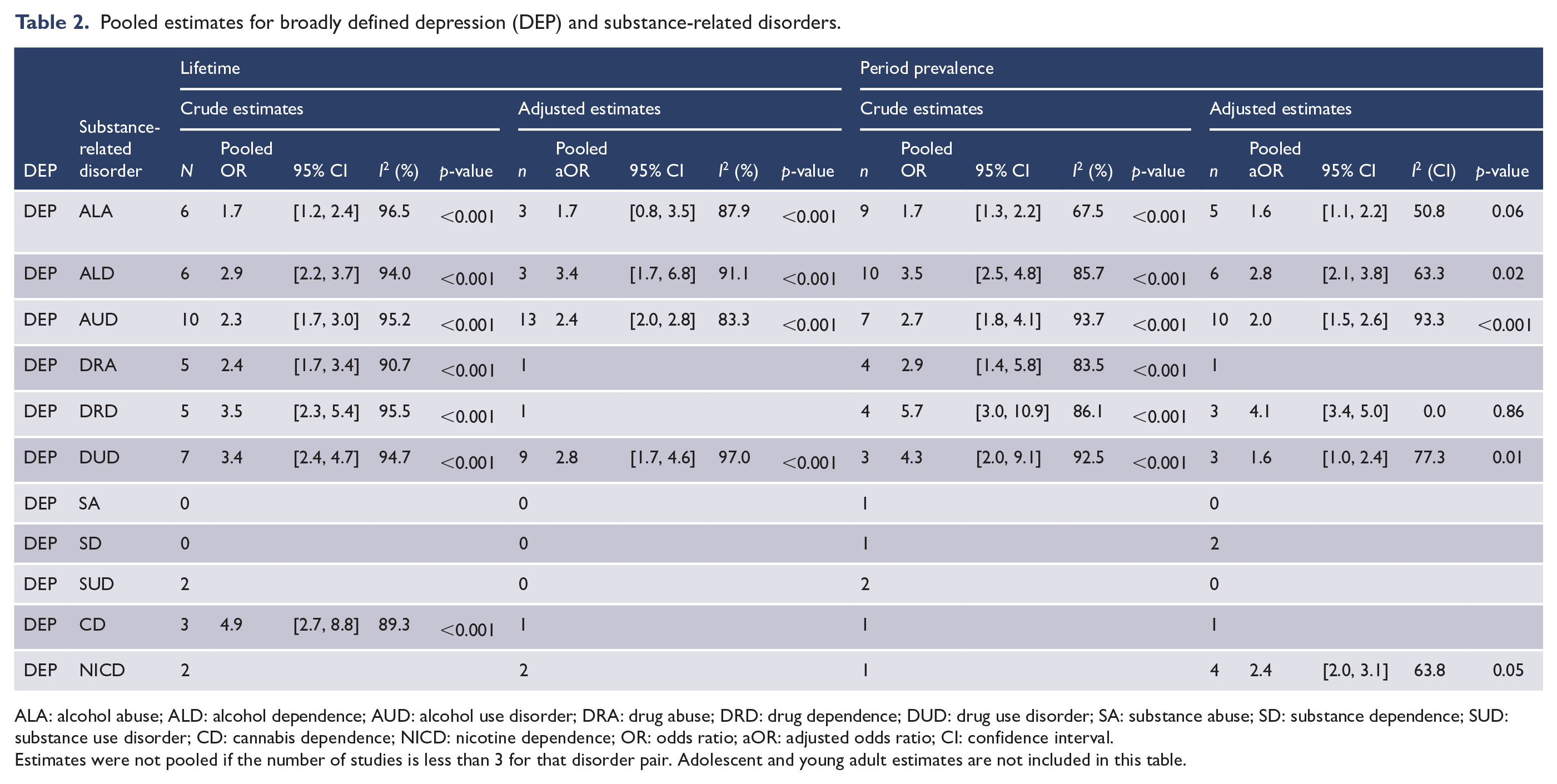
ALA: alcohol abuse; ALD: alcohol dependence; AUD: alcohol use disorder; DRA: drug abuse; DRD: drug dependence; DUD: drug use disorder; SA: substance abuse; SD: substance dependence; SUD: substance use disorder; CD: cannabis dependence; NICD: nicotine dependence; OR: odds ratio; aOR: adjusted odds ratio; CI: confidence interval.
Estimates were not pooled if the number of studies is less than 3 for that disorder pair. Adolescent and young adult estimates are not included in this table.
Pooled estimates for broadly defined dysthymic disorder (DYS) and substance-related disorders.
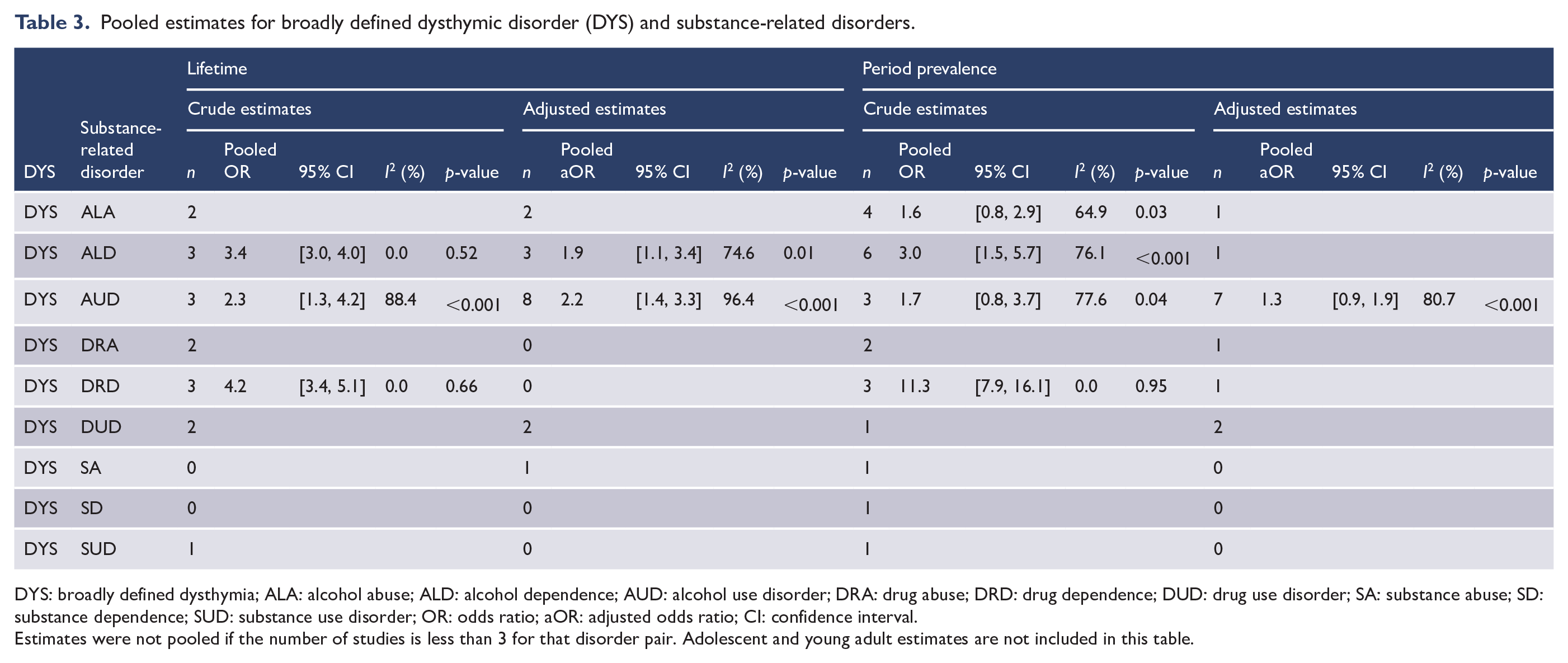
DYS: broadly defined dysthymia; ALA: alcohol abuse; ALD: alcohol dependence; AUD: alcohol use disorder; DRA: drug abuse; DRD: drug dependence; DUD: drug use disorder; SA: substance abuse; SD: substance dependence; SUD: substance use disorder; OR: odds ratio; aOR: adjusted odds ratio; CI: confidence interval.
Estimates were not pooled if the number of studies is less than 3 for that disorder pair. Adolescent and young adult estimates are not included in this table.
Pooled estimates for broadly defined bipolar disorder and substance-related disorders.
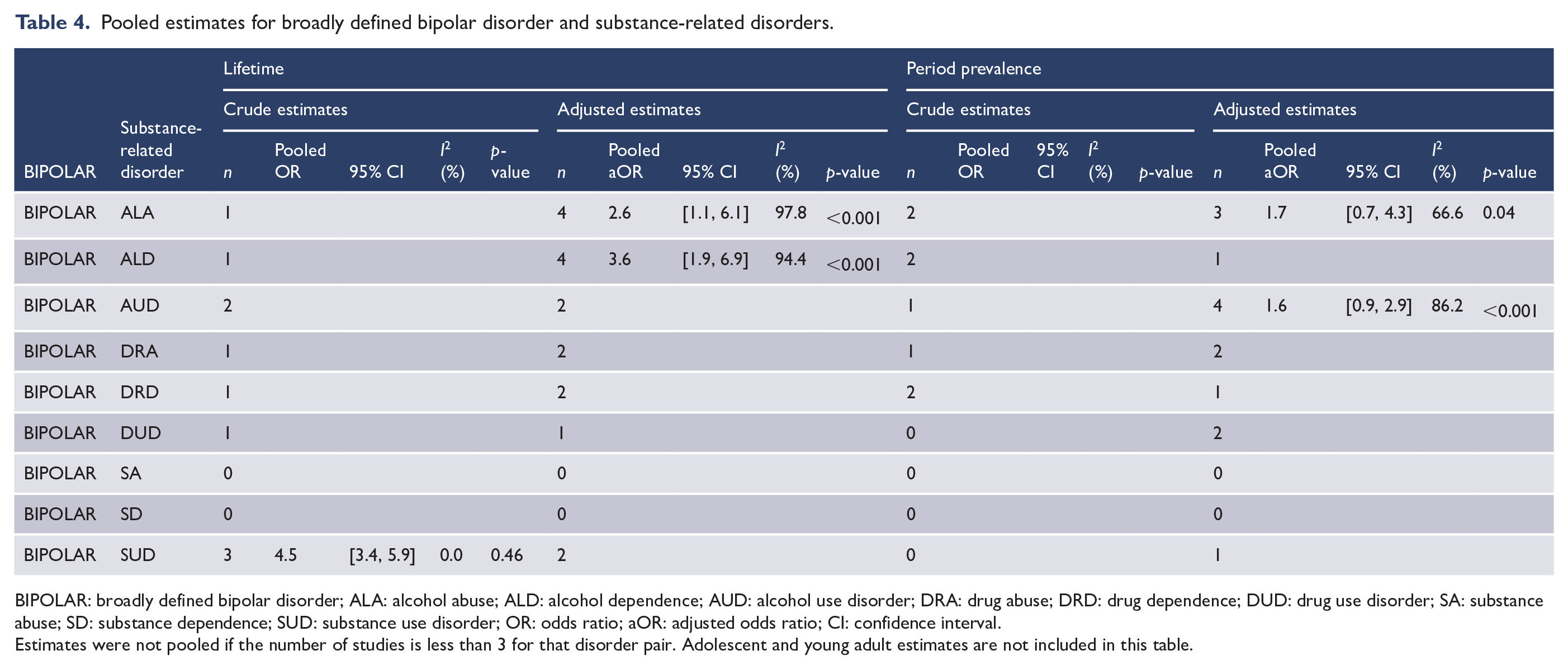
BIPOLAR: broadly defined bipolar disorder; ALA: alcohol abuse; ALD: alcohol dependence; AUD: alcohol use disorder; DRA: drug abuse; DRD: drug dependence; DUD: drug use disorder; SA: substance abuse; SD: substance dependence; SUD: substance use disorder; OR: odds ratio; aOR: adjusted odds ratio; CI: confidence interval.
Estimates were not pooled if the number of studies is less than 3 for that disorder pair. Adolescent and young adult estimates are not included in this table.
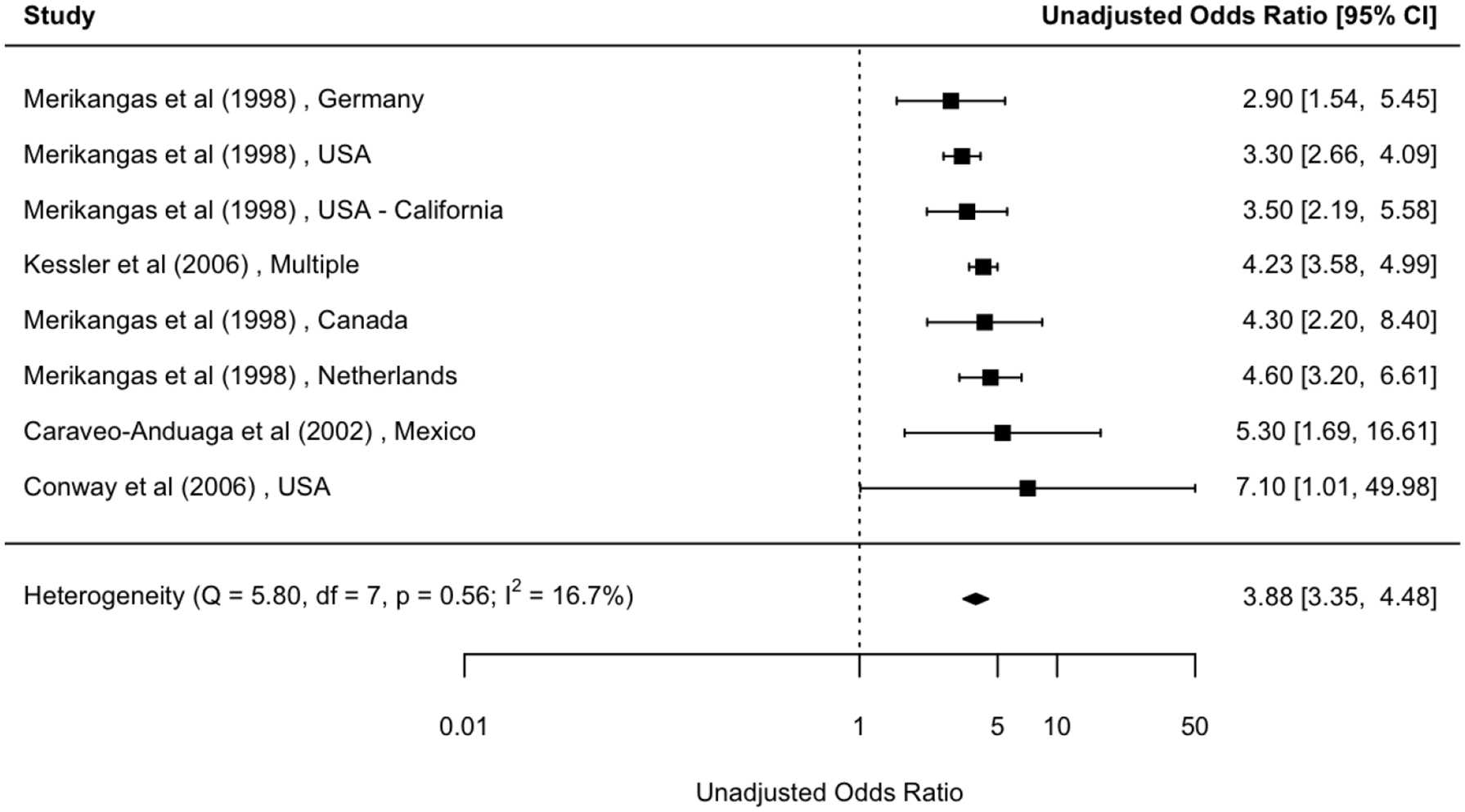
Forest plot: lifetime comorbidity between broadly defined mood disorder and drug dependence (unadjusted).
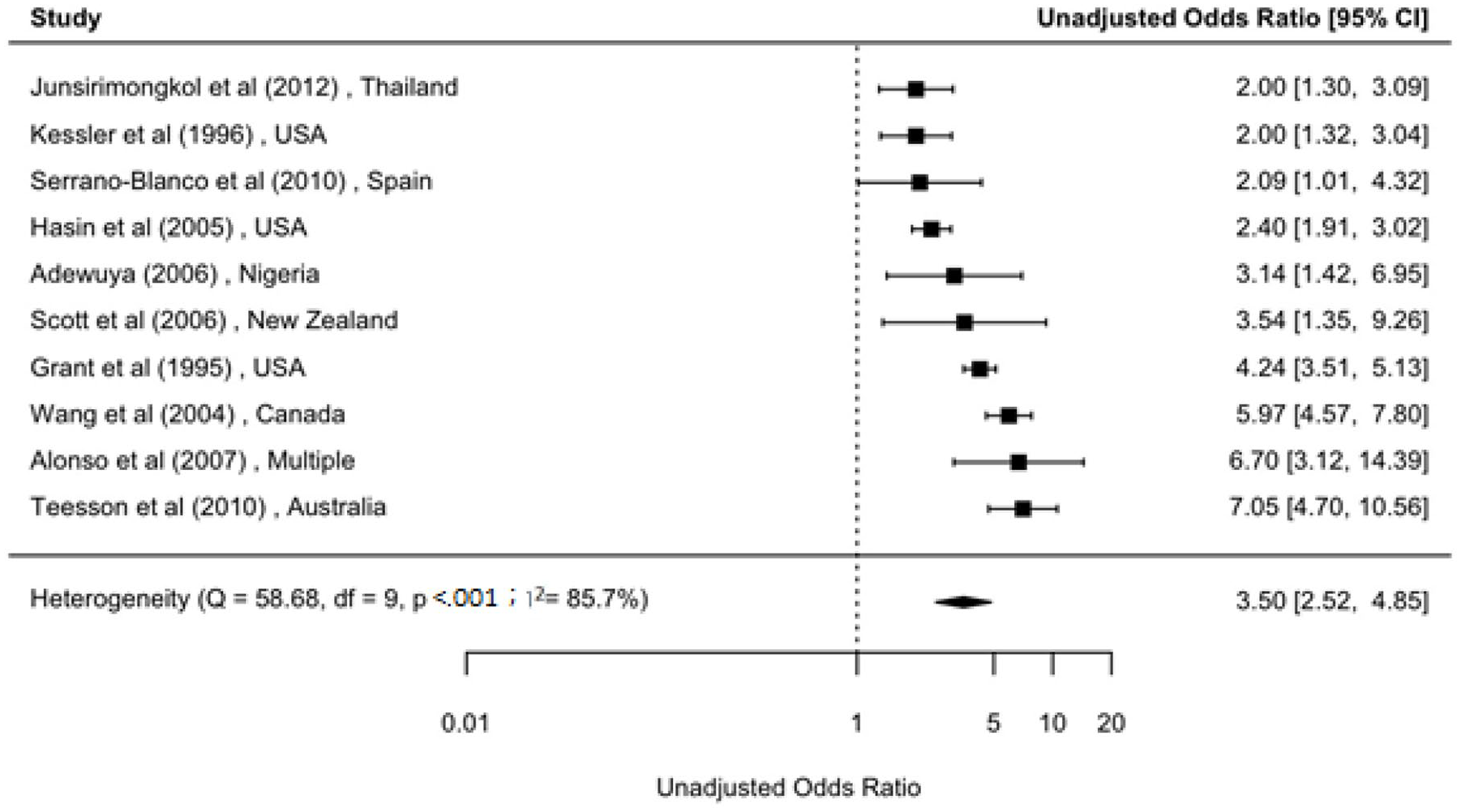
Forest plot: period prevalence comorbidity between broadly defined depression and alcohol dependence (unadjusted).
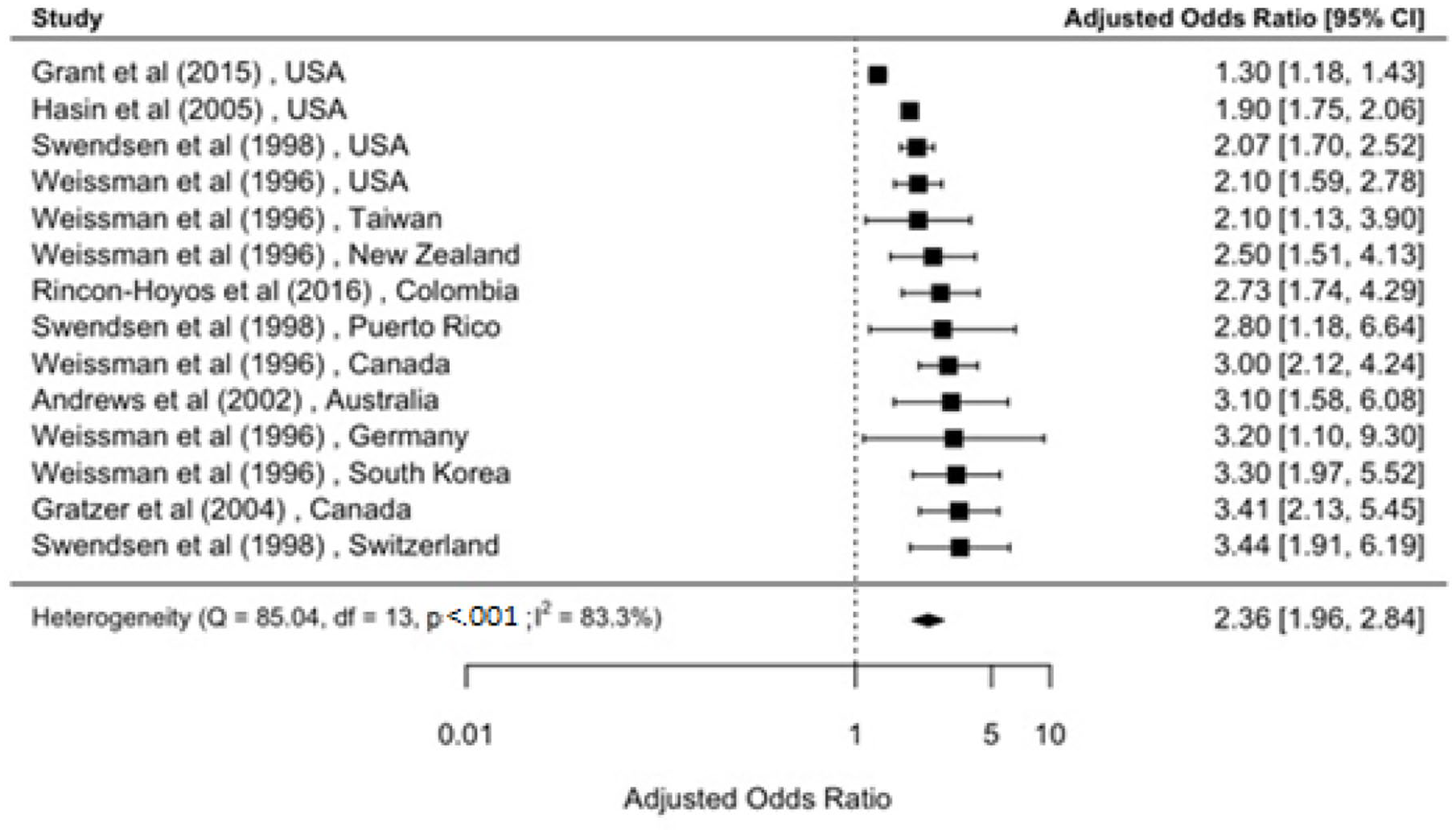
Forest plot: lifetime comorbidity between broadly defined depression and alcohol use disorder (adjusted).
Overall, there was a substantial comorbidity between mood- and substance-related disorders. For example, those with lifetime MOOD had a fourfold elevated risk of drug dependence (OR = 3.9; 95% CI = [3.4, 4.5]). Similar comorbidity was found between DEP and ALD (OR = 3.5; 95% CI = [2.5, 4.9]), while we found slightly lower risk of comorbidity between DEP and alcohol use disorder (AUD; aOR = 2.4; 95% CI = [2.0, 2.8]; Figures 2–4). In those with lifetime MOOD had three times elevated risk of ALD (Supplementary Figure S4).
MOOD and alcohol-related disorder: lifetime/period prevalence comorbidity
We identified 10 estimates based on 5 studies (Reference S1) for unadjusted lifetime comorbidity between MOOD and alcohol-related disorders (Table 1). The unadjusted ORs [95% CI] were significant and ranged between 1.8 [1.3, 2.5] for MOOD and AUD, and 2.8 [2.3, 3.3] for MOOD and ALD. In the adjusted models, we found twofold association between these two disorder groups (Reference S2). The aOR [95% CI] ranged between 2.2 [1.7, 2.9] for MOOD and AUD based on seven estimates, and 2.4 [1.4, 4.1] for MOOD and ALD.
We identified 14 estimates based on 7 studies (Reference S3) for unadjusted period prevalence comorbidity between MOOD and alcohol-related disorders (Table 1). The unadjusted ORs [95% CI] were significant, and ranged between 1.3 [1.1, 1.5] for MOOD and alcohol abuse (ALA), and 4.3 [2.6, 7.1] for MOOD and ALD. Adjusted models were derived from 18 estimates based on 10 studies (Reference S4). The aOR [95% CI] ranged between 1.3 [0.7, 2.6] for MOOD and ALA based on four estimates, and 4.2 [2.0, 8.8] between MOOD and ALD.
MOOD and other substance-related disorder (drug, substance): lifetime/period comorbidity
We identified 11 estimates based on 5 studies (Reference S5) for lifetime comorbidity between MOOD and drug-related disorders (Table 1). The unadjusted ORs [95% CI] were significant for MOOD and drug abuse (DRA) and drug dependence (DRD). The pooled estimates were 2.5 [1.5, 4.1] and 3.9 [3.3, 4.4], respectively. There were no adjusted pooled estimates for any MOOD and drug-related disorders.
We generated only two pooled estimates for period prevalence comorbidity between MOOD and substance-related disorders (MOOD vs substance use disorder [SUD], and MOOD vs drug use disorder [DUD]) based on six estimates/studies (Reference S6). The unadjusted OR [95% CI] between MOOD vs SUD was 2.6 [2.1, 3.2] and the adjusted aOR [95% CI] between MOOD vs DUD was 2.3 [1.4, 3.7].
Depression (DEP) and alcohol-related disorder: lifetime/period prevalence comorbidity
We identified 22 estimates based on 12 studies (Reference S7) for unadjusted lifetime comorbidity between DEP and alcohol-related disorders (Table 2). The unadjusted ORs [95% CI] were significant and ranged between 1.7 [1.2, 2.4] for DEP and ALA based on six estimates/studies, and 2.9 [2.3, 3.8] for DEP and ALD. Adjusted estimates were also significant that were derived from 19 estimates based on 9 studies (Reference S8). The aOR [95% CI] ranged between 1.7 [0.8, 3.5] for DEP and ALA and 3.4 [1.7, 6.8] for DEP and ALD.
We identified 26 estimates based on 14 studies (Reference S9) for unadjusted period prevalence comorbidity between DEP and alcohol-related disorders (Table 2). The unadjusted ORs [95% CI] were significant and ranged between 1.7 [1.3, 2.2] for DEP and ALA and 3.5 [2.5, 4.9] for DEP and ALD. Adjusted aORs were derived from 21 estimates based on 11 studies (Reference S10). The aORs [95% CI] were significant and ranged between 1.6 [1.1, 2.2] for DEP and ALA and 2.8 [2.1, 3.8] for DEP and ALD.
Depression (DEP) and other substance-related disorders (drug, cannabis, nicotine): lifetime/period prevalence comorbidity
We identified 17 estimates based on 9 studies (Reference S11) for unadjusted lifetime comorbidity between DEP and drug-related disorders (Table 2). The unadjusted ORs [95% CI] were significant and ranged between 2.4 [1.7, 3.4] for DEP and DRA and 3.5 [2.3, 5.4] for DEP and DRD. The only aOR [95% CI] for DEP and DUD was 2.8 [1.7, 4.6] based on nine estimates (four studies: Reference S12).
We identified 11 estimates based on 5 studies (Reference S13) for unadjusted period prevalence comorbidity between DEP and drug-related disorders (Table 2). The unadjusted ORs [95% CI] were significant and ranged between 2.9 [1.4, 5.8] for DEP and DRA and 5.7 [3.0, 10.9] for DEP and DRD. The adjusted aORs were significant that derived from six estimates (five studies: Reference S14). The aOR [95% CI] for DEP, and DRD and DUD were 4.1 [3.4, 5.0] and 1.6 [1.0, 2.4], respectively.
We generated significant lifetime comorbidity between DEP and cannabis dependence (OR = 4.9, 95% CI = [2.7, 8.8]) based on three studies (Reference S15), and period prevalence comorbidity between DEP and nicotine dependence (aOR = 2.4, 95% CI = [2.0, 3.0]) based on four studies (Reference S16) (Table 2).
Dysthymia (DYS) and alcohol-related disorders: lifetime/period prevalence comorbidity
We identified six estimates based on five studies (Reference S17) for unadjusted lifetime comorbidity between DYS and alcohol-related disorders (Table 3). The unadjusted ORs were significant for DYS and AUD (OR = 2.3; 95% CI = [1.3, 4.2]), and DYS and ALD (OR = 3.4: 95% CI = [3.0, 4.0]). The adjusted lifetime estimates derived from 11 estimates based on 6 studies (Reference S18). The aORs were also significant between DYS and AUD (OR = 2.2: 95% CI = [1.4, 3.3]), and between DYS and ALD (OR = 1.9: 95% CI = [1.1, 3.4]).
We identified 13 estimates based on 7 studies (Reference S19) for unadjusted period prevalence comorbidity between DYS and alcohol-related disorders (Table 3). The only significant association was between DYS and ALD (OR = 2.9; 95% CI = [1.5, 5.7]). The only adjusted aOR between DYS and AUD that derived from seven estimates (four studies; Reference S20) was not significant.
Dysthymia (DYS) and other substance-related disorders: lifetime/period prevalence comorbidity
We generated only one unadjusted lifetime estimate based on three studies (Reference S21), and one period prevalence comorbidity estimate based on three studies (Reference S22) between DYS and DRD (Table 3). The respective ORs [95% CI] were 4.2 [3.4, 5.1] and 11.3 [7.9, 16.2]. No adjusted estimates were available.
BIPOLAR and alcohol-related disorders: lifetime/period prevalence comorbidity
We generated only two pooled estimates for lifetime comorbidity (adjusted) between BIPOLAR and alcohol-related disorders (Table 4) based on eight estimates (four studies: Reference S23). The aORs [95% CI] were 2.6 [1.1, 6.1] for DEP and ALA, and 3.6 [1.9, 6.9] for DEP and ALD. Similarly, we found only two pooled estimates for period prevalence comorbidity (adjusted) between BIPOLAR and alcohol-related disorders (Table 4) based on seven estimates (four studies: Reference S24). Both the aORs [95% CI] were not significant.
We found a significant lifetime comorbidity between BIPOLAR and SUD in the unadjusted model (OR = 4.5, 95% CI = [3.4, 5.9]) based on three studies (Reference S25).
Pooled estimates for temporally ordered associations
There were two unadjusted and two adjusted temporally ordered pooled estimates between DEP and alcohol-related disorders (Supplementary Tables S2). Unadjusted pooled estimates between DEP, and ALA and ALD were derived from seven estimates (four studies: Reference S26). Those with DEP (as a prior disorder) had twofold elevated risk of later ALD (OR = 2.1; 95% CI = [1.3, 3.7]), while the estimate between DEP and ALA was not significant. Adjusted pooled estimates between DEP, and ALD and AUD were derived from seven estimates (seven studies: Supplementary Reference S27. Those with DEP (as a prior disorder) had about 70% elevated risk of later ALD (aOR = 1.7; 95% CI = [1.1, 2.8]), while those with AUD as a prior disorder, the risk of subsequently developing DEP was about 40% (aOR = 1.4; 95% CI = [1.2, 1.6]).
Individual estimates not meta-analysed
As stated, we present individual pairwise association data for lifetime and period prevalence comorbidity estimates in Supplementary Tables S2–S5, while temporally ordered comorbidity estimates are presented in Supplementary Tables S6–S10. Overall, we found 502 individual estimates of comorbidity between MOOD and various substance-related disorders that were not included in the 56 meta-analyses presented above. Consistent with the meta-analytic findings, the majority of estimates from these studies showed elevated risk of comorbidity (estimates above 1 with 95% CI not including 1) between mood and substance-related disorders.
Publication bias, quality scores and heterogeneity
Because most of the meta-analyses were based on small numbers of contributing studies, we were able to produce only five funnel plots (with studies > 10) (Supplementary Figures S55–S59). Overall, the funnel plots did not suggest substantial publication bias. Q-statistics and I2 tests showed signs of heterogeneity within most pooled estimates (44 out of 56 plots). For the included studies, the median quality score was 14 and the interquartile range was 13–15 (Supplementary Table S1). Because of the lack of variation in the quality scores, no additional investigation of the impact of this score on the findings was undertaken.
Discussion
Based on 120 studies from 24 countries, this systematic review generated 56 separate meta-analyses that included 52 lifetime and period prevalence, and 4 temporally ordered pooled estimates. To the best of our knowledge, this is the most comprehensive systematic review and meta-analysis of comorbidity between mood and substance-related disorders. We found consistent evidence of comorbidity between broadly defined mood and various substance-related disorders. The pooled risk estimates for all 56 meta-analyses were above 1, of which 47 were significant (i.e. the 95% CI did not include 1). Additionally, this review sheds light on three key issues. First, we found significant comorbidity between mood and substance-related disorders regardless of the period of observation, and regardless of the study design (e.g. diagnostic criteria) or covariate estimates. Second, we report temporal ordering of the pooled estimates showing significant associations between certain disorder pairs. Finally, we found a lack of data for some mood and substance-related disorder pairs, which can guide future research. We discuss each of these in turn.
With respect to the period of observation (period, lifetime, temporal order, etc.) and covariate estimates (unadjusted vs adjusted), we found substantial comorbidity between mood and substance-related disorders. The majority of the pooled estimates were significant (i.e. the 95% CI did not include 1), broadly consistent with previously conducted systematic reviews (Hunt et al., 2016a, 2020; Lai et al., 2015; Messer et al., 2017). For example, Lai et al. (2015) reported an elevated lifetime comorbidity between depression, and both AUD (OR = 2.4; 95% CI = 2.2, 2.6) and drug use disorder (OR = 3.8; 95% CI = [3.0, 4.8]), which is comparable to our pooled estimates (aORs: 2.4 between DEP and AUD, and 2.8 between DEP and DUD). Our estimates were also broadly consistent with two recently published studies (published after completion of our data extraction) (McGrath et al., 2020; Plana-Ripoll et al., 2019). We note that the pooled OR varies between disorder pairs. For example, we found a sixfold elevated risk between MOOD and drug dependence (OR = 5.7) and fivefold risk between depression and cannabis dependence (OR = 4.9) while the highest pooled estimate, based on period prevalence risk, was found between DYS and drug dependence (OR = 11.3). Overall, the consistent patterns identified by our systematic review, and the findings from earlier systematic reviews and two recent studies, provide strong convergent evidence of comorbidity between these disorders.
While most of the pooled estimates showed elevated comorbidity risk, we note that we did not find significant increased risks for some disorder pairs. For example, ALA did not show any significant associations with period prevalence mood, dysthymia or bipolar disorders. Similarly, there were no significant associations between AUD, and dysthymia or bipolar disorders in the adjusted models. However, while pooled point estimates for these disorder pairs were above 1, the CIs were imprecise (i.e. they included 1). As additional primary studies on these disorder pairs become available, these CIs may become more precise and meet conventional criteria for statistical significance.
With respect to the temporal ordering of comorbidity between mood- and substance-related disorders, there was a twofold association between lifetime DEP and ALD in those with DEP as a prior disorder. The risk was found in both unadjusted and adjusted models. Additionally, we found a 40% elevated risk of subsequently developing depression in those with AUDs, a finding consistent with recently conducted meta-analysis of cohort studies. For example, Li et al. (2020) meta-analysed 42 studies and found about 60% risk of subsequently developing DEP those with AUD. However, our estimates were based on a limited number of studies. More prospective epidemiological studies are needed for bidirectional comorbidity data in this field of research. For example, while the findings may be bidirectional, it would be interesting to explore in future studies if the absolute effect sizes vary according to temporal order (i.e. within bidirectional comorbidity, the risks are asymmetrical).
In addition, we wish to draw attention to the gaps in the literature. For example, we were not able to find enough estimates to pool any drug-related disorders for bipolar disorders, and there was also limited data for mood or dysthymic disorders. There were no pooled estimates for cannabis or nicotine-related pooled estimates for mood, dysthymia or bipolar disorders. Overall, we were able to meta-analyse only 269 estimates in 56 models (where we found 3 or more estimates per model). However, within non-meta-analysed estimates (n = 502), the vast majority also reported an increased risk of comorbidity between mood- and substance-related disorders.
Strengths and limitations
In this systematic review, we used a range of methodological features for pooled estimates. First, we applied rigorous criteria for selecting studies. Second, we used a range of design features for pooled estimates and presented separate estimates for period of observation (period, lifetime prevalence, etc.), temporal order and the use of adjustments for covariates. With respect to key limitations, we note that despite parsing estimates into these meaningful groups, Q-statistics and I2 tests indicated heterogeneity in the estimates underlying most of the pooled estimates. This is not uncommon in studies of comorbidity, because the prevalence of the individual disorders can vary between sites (McGrath et al., 2020). This is particularly the case for the prevalence of different types of substance use, which can vary according to cultural practices and legal frameworks. Despite these issues, we note that most individual estimates were above 1, and the heterogeneity relates to the precise effect size, rather than (a) the direction of the association (i.e. the sign of the estimate) or (b) the significance of the estimates (e.g. the exclusion of individual estimates were unlikely to result in CIs that included 1).
Conclusion
This comprehensive systematic review confirms the substantial comorbidity between various mood- and substance-related disorders. The consistency of comorbidity of pairs of these two groups of common mental disorders emphasizes the possibility of a shared risk architecture which could underpin their pathogenesis (Grotzinger, 2021; Johnson et al., 2020; Kessler, 2004; Zhou et al., 2020). Understanding the risk of comorbidity between mood and substance-related disorders is important from a public health perspective, given that this type of comorbidity is associated with poorer clinical outcomes, increased risk of suicidality and higher service use (Jørgensen et al., 2018; Østergaard et al., 2017; Prior et al., 2017). Clinical practice guidelines for the treatment of mood disorders emphasize the need to take into account comorbid substance use disorders (Malhi et al., 2015). Services can be designed to streamline the management of individuals with this common type of comorbidity (Substance Abuse Mental Health Services Administration (SAMHSA), 2020). Reviews of the evidence surrounding these services highlight the importance of features such as (a) universal screening of substance use and common mental disorders in mental health services, (b) supportive therapies (e.g. motivational interviewing and related counselling, withdrawal management, psychoeducation) in mental health setting and (c) assertive follow-up and integration between different treatment services (NSW Ministry of Health, 2015). We hope that the findings of our systematic review can alert clinicians to the increased risk of shared comorbidity between mood and substance use disorders in clinical settings and also guide future research.
Supplemental Material
sj-pdf-1-anp-10.1177_00048674211054740 – Supplemental material for Comorbidity between mood and substance-related disorders: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-anp-10.1177_00048674211054740 for Comorbidity between mood and substance-related disorders: A systematic review and meta-analysis by Sukanta Saha, Carmen CW Lim, Louisa Degenhardt, Danielle L Cannon, Monique Bremner, Finley Prentis, Zoe Lawrence, Ed Heffernan, Carla Meurk, John Reilly and John J McGrath in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We wish to thank Ann Cude for logistic support.
Author contributions
S.S. and J.J.M. conceived the study. C.C.W.L., S.S. and J.J.M. conducted the analysis, drafted and edited the manuscript. D.L.C., M.B., F.P. and Z.L. were involved in data entry and consistency checking. L.D., C.C.W.L., J.R., C.M. and E.H. critically reviewed the manuscript. All authors contributed to refinement of the manuscript and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The project is supported by the Danish National Research Foundation (Niels Bohr Professorship to J.J.M.) as well as John Cade Fellowship APP1056929 (awarded to J.J.M.) from the National Health and Medical Research Council, Australia.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.