
Abstract
Objectives:
Functional disruption is a main feature of schizophrenia and still represents a major treatment challenge. A more in-depth identification of functional predictors is crucial for the creation of individualized rehabilitation treatments, which can translate into better functional outcomes. In this study, we aimed at pinpointing specific domains that affect different functional profiles, using a data-driven approach.
Methods:
We included a comprehensive evaluation of functional predictors, namely demographic, cognitive, sociocognitive and clinical variables, with a focus on constituent subdomains of autistic symptoms that have been associated with functioning in the recent literature.
Results:
In 123 schizophrenia patients, a two-step cluster analysis identified two groups of patients with different functional profiles (low vs high functioning). A backward stepwise logistic regression analysis showed that the odds of being a member of the high functioning group are significantly higher for individuals with (1) more years of education, (2) better Theory of Mind abilities, (3) higher levels of stereotypies/narrowed interests, (4) lower difficulties in social interaction, (5) lower communication difficulties and with (6) being male.
Conclusion:
Findings raise the intriguing possibility that stereotypic behaviors may have a beneficial effect on functioning in schizophrenia. While the underlying mechanism is currently unknown, we hypothesize that patients may benefit from contexts in which more predictive relationships between environmental entities can systematically be established. This study underscores the potential utility of routinely assessing autistic symptomatology in schizophrenia, which can be instrumental in identifying novel therapeutic targets that can be utilized to improve daily functioning.
Introduction
Ranked among the top 25 principal causes of disability worldwide, schizophrenia is one of the most burdensome and costly illnesses worldwide (World Health Organization [WHO], 2001). Disruption in daily functioning is a main feature of schizophrenia that manifests in considerable deterioration in social, personal and occupational areas of life (Bechi et al., 2017). With 57–74% of patients showing a significant and persistent functional disability—even after achieving psychopathological stabilization (González-Blanch et al., 2010)—the recovery of daily functioning represents a priority target of treatment in schizophrenia (Buonocore et al., 2017). While the sizable literature on functioning in schizophrenia has been instrumental in identifying important predictors of functioning, it has often focused on only a specific or a subset of the functional domains affected in schizophrenia, or influencing factors. With the aim of pinpointing specific factors that can be targeted to improve functioning, the present study reports on a comprehensive analysis examining the influence of demographic, clinical, cognitive and sociocognitive variables on both functional capacity and everyday functioning of patients with schizophrenia.
With the purpose of creating individualized rehabilitation treatment tailored to the patient’s profile of impairment, previous studies have identified several important functional predictors (Bechi et al., 2017). First, demographic (e.g. age) and clinical variables (e.g. negative symptoms) have been associated with poor levels of functioning, although their predictive value is relatively low (Olsson et al., 2016). Second, cognitive abilities, and especially attention and executive functions (Kurtz et al., 2016), and sociocognitive skills, and especially Theory of Mind and empathic abilities (Mucci et al., 2021), are considered major predictors of daily functioning in patients with schizophrenia, accounting for 20–30% of the variance (Best et al., 2014). Third, and in light of accumulating evidence suggesting that autistic symptoms can co-occur in individuals with schizophrenia, a number of studies have shown that co-occurring autistic symptoms in schizophrenia are significantly associated with lower quality of life and functioning (Bechi et al., 2019, 2020b), although this seems to be specific to symptomatically severe patients (Bechi et al., 2021).
However, our current knowledge of functional dysfunction and associated factors in schizophrenia remains incomplete, which may be attributed to four main reasons. The first pertains to considerations concerning the concept of ‘daily functioning’. Daily functioning is a multi-faceted construct, which is susceptible to internal (i.e. satisfaction, motivation, intimacy) and external cues (i.e. social activities, job role). Studies have distinguished between two different facets of functioning: functional capacity and real-world functioning (Bechi et al., 2017). Functional capacity refers to the ability to perform everyday tasks in a neutral environment, for instance, in a laboratory or a hospital setting, and real-world functioning refers to what the patient actually does in real life, such as occupational role functioning, verified by a third party. In a previous study by our research group (Bechi et al., 2017), we observed that functional capacity and real-world functioning were influenced by different factors: functional capacity was influenced by overall cognitive abilities (i.e. IQ), while real-world functioning was influenced by sociocognitive abilities (i.e. empathy and emotion recognition abilities) as well as overall symptomatology. The second is heterogeneity of the illness outcomes. While the majority of patients present significant functional dysfunction (González-Blanch et al., 2010), research has reported considerable heterogeneity among patients, ranging from severe impairments (as seen in chronic patients) to viable levels of functioning (i.e. having satisfying job role and significant relationships; Bosia et al., 2019). The third pertains to the breadth of the possible contributing factors to functional dysfunction. Previous studies have mostly assessed functioning by considering a subset of possible contributing factors (Mucci et al., 2021), which prohibits reaching conclusive conclusions about the most relevant targets of treatment. Fourth, studies that examined the effect of co-occurring autistic symptoms on functioning in schizophrenia have estimated the effect of overall autism symptom severity, rather than the contribution of specific subdomains, which include social interaction and communication difficulties, as well as narrowed interests and stereotypic behavior. Accounting for this subdomains may be necessary, given evidence suggesting that these subdomains are dissociable in terms of their genetic and neural mechanisms (Szatmari et al., 2012).
Delineating functional heterogeneity and determinants in schizophrenia can be meaningfully clarified by assessing functioning using multi-faceted measures and by considering a wide array of potentially contributing factors. Accordingly, we extend previous research in three important respects: (1) we evaluate functioning with a comprehensive assessment that covers both functional capacity and real-world functioning; (2) based on the literature, we adopt an all-embracing evaluation of demographic, clinical, cognitive and sociocognitive predictors that have been shown to contribute to functional heterogeneity; and (3) to examine the specific interplay between functioning and autistic symptoms, we also include as predictors the constituent subdomains of autistic symptoms, namely, social interaction and communication difficulties, as well as narrowed interests and stereotypic behavior. To our knowledge, the association of specific autistic subdomains with daily functioning in schizophrenia has not been systematically investigated in previous studies.
In line with previous literature, and given the well-known heterogeneity that characterizes schizophrenia, we expect to identify different functional profiles within our sample, where we expect higher functioning patients to exhibit better cognitive and sociocognitive abilities and lower expression of clinical symptomatology (Bechi et al., 2019; Bosia et al., 2019). In addition, previous research has linked communication abnormalities and active social avoidance in schizophrenia with socially disruptive behavior, and withdrawal from social contact and impaired social functioning (Harvey et al., 2019), and more recently communicative-pragmatic disruption with functional outcome (Agostoni et al., 2021). We, therefore, predict a negative association between autistic social interaction and communication difficulties and social functioning in schizophrenia. As for narrow interests and stereotypic behaviors domain, previous literature does not permit us to make specific predictions about their impact on daily functioning in schizophrenia, although, in the autism spectrum disorder (ASD) literature, these behaviors have been viewed as both a source of disruption in everyday living and a coping mechanism to reduce high levels of arousal and distress (Scahill et al., 2015).
Materials and methods
Participants
A total of 123 patients, 52 female; mean age (SD) = 44.20 (11.31) years; mean illness duration (SD) = 20.29 (10.14) years, were recruited at the IRCCS San Raffaele Hospital, Department of Clinical Neurosciences, Milan, Italy. They all met Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria for schizophrenia, as determined by trained psychiatrists through a clinical interview. All patients were clinically stabilized and treated with a stable dose of the same antipsychotic therapy for at least 3 months. Exclusion criteria included having severe traumatic brain injury or neurological disorders, alcohol or substance abuse in the past 6 months, or severe psychotic acutization in the past 3 months.
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human subjects/patients were approved by the local Ethical Committee (approval number: 318/06). All enrolled subjects provided written informed consent.
Assessment
All patients were assessed for psychopathology, intellectual level, daily functioning, and neurocognitive and sociocognitive abilities.
Psychopathology
Psychopathology was assessed by means of the Positive and Negative Syndrome Scale (PANSS) (Kay et al., 1987), a standardized measurement for typological and dimensional symptoms evaluation in schizophrenia. PANSS evaluates the severity of positive, negative and general psychopathology. The PANSS shows good internal consistency for the positive (Cronbach’s α = 0.80), negative (Cronbach’s α = 0.82) and general psychopathology (Cronbach’s α = 0.82) scales. The measure of interest in this study was PANSS Positive score.
Autistic symptoms were evaluated with the PANSS Autism Severity Score (PAUSS) (Kästner et al., 2015). The PAUSS is the only validated measure for the assessment of autistic symptoms in schizophrenia and has high internal consistency (Cronbach’s α = 0.85) and good convergent validity (r = 0.76) (Kästner et al., 2015). Importantly, the PAUSS, which was originally validated with the Autism Diagnostic Observation Schedule (ADOS) (Lord et al., 2000), has been shown to also reflect autistic severity of individuals with Schizophrenia Spectrum Disorder SSD who were assessed with the Autism Diagnostic Interview–Revised (ADI-R; Lord et al., 1994)—a measure that is based on the individual’s early developmental history through a parent/caregiver interview. This suggests that the PAUSS is capturing childhood-onset autistic features rather than current autistic-like features (Deste et al., 2018). Three scores, representing the three symptom domains of autism, are derived from eight PANSS items: (1) ‘Difficulties in Social Interaction’ Score, generated by summing items 1, 3 and 4 from the Negative Scale; (2) ‘Difficulties in Communication’ Score generated by summing items 5 and 6 from the Negative Scale; and (3) ‘Stereotypies/Narrowed Interests’ Score generated by summing items 5 and 15 from the General Scale and item 7 from the Negative Scale. The PAUSS Total Score is the sum of the subscales and ranges from 0 to 56. A PAUSS cut-off score of ⩾30 identifies patients with significant levels of autistic symptoms (Kästner et al., 2015). The measures of interest in this study were PAUSS Difficulties in Social Interaction, Difficulties in Communication Score and Stereotypies/Narrowed Interests scores.
Cognitive abilities
Intellectual level was assessed by means of the Wechsler Adult Intelligence Scale–Revised (WAIS-R, Italian Version) (Wechsler, 1997), which is a well-known battery of 11 tests estimating the intelligence quotient and both verbal and performance IQ. The measure of interest in this study was the IQ Total Score.
Neurocognitive abilities were evaluated with the Italian version of the Brief Assessment of Cognition in Schizophrenia (BACS) (Anselmetti et al., 2008), a broad neuropsychological battery evaluating core cognitive domains that are typically impaired in schizophrenia, namely verbal memory, working memory, psychomotor speed and coordination, attention, verbal fluency and executive functions. Cognitive Index, as a measure of overall cognitive functioning, is derived from BACS mean equivalent scores. The BACS shows a good internal consistency (Cronbach’s α = 0.85) (Zhou and Li, 2020). The variables of interest in this study were the BACS Attention, Executive functions and Cognitive Index scores.
Sociocognitive abilities were evaluated with the Theory of Mind Picture Sequencing Task (PST) (Brüne, 2003) and the Interpersonal Reactivity Index (IRI) (Davis, 1983). In the Sequencing task, six cartoon picture stories were presented, and the participants were asked to order the cards of the stories in a logical sequence of events. In addition, a Theory of Mind (ToM) questionnaire was administered to the participants to test their ability to appreciate the mental states, motivations or beliefs of the characters involved in the cartoon stories. The PST shows a good internal consistency (Cronbach’s α = 0.86) (Bechi et al., 2012). The variables of interest of this study were the PST Questionnaire and the PST Sequencing scores. The IRI is a validated multi-dimensional self-report questionnaire assessing cognitive and affective empathy and consists of the following four subscales: Perspective Taking (Cronbach’s α = 0.54), Empathic Concern (Cronbach’s α = 0.69), Personal Distress (Cronbach’s α = 0.50) and Fantasy (Cronbach’s α = 0.77). The variables of interest in this study were the four IRI subscores.
Functional outcomes
Real-world behavior was assessed with the Quality of Life Scale (QLS) (Heinrichs et al., 1984), a semi-structured interview made up of 21 items, balancing subjective questions regarding life satisfaction and objective indicators of social and occupational role functioning. As in previous studies (Buonocore et al., 2017), three domains of functioning were analyzed: (1) Interpersonal Relations, (2) Instrumental Role and (3) Personal Autonomy. The QLS global score has good internal consistency (Cronbach’s α = 0.8–0.9) (Simon-Abbadi et al., 1999). The measures of interest in this study were the QLS Interpersonal Relations, Instrumental Role and Personal Autonomy scores.
Functional capacity was assessed with the UCSD Performance based Skills Assessment–Brief (UPSA-B) (Mausbach et al., 2010). The UPSA-B is a measure of functional capacity in which patients are asked to perform everyday tasks in communication and finances areas. The UPSA-B has good internal consistency for both the communication (Cronbach’s α = 0.59) and finances (Cronbach’s α = 0.59–0.77) areas of functioning (Olsson et al., 2012). The measures of interest in this study were the UPSA-B Communication and Finances scores.
All assessments, except for the PANSS, were administered by trained psychologists who demonstrated adequate reliability at routine reliability checks. The PANSS was administered by trained psychiatrists.
Data analysis
A two-step cluster analysis, with Schwarz’s Bayesian Criterion as an estimate of cluster stability, was conducted to identify the potential presence of groups of patients with different functional profiles. In this data-driven approach, the clustering variables consisted of all the patients’ individual subscale scores on the QLS (i.e. Interpersonal Relations, Instrumental Role and Personal Autonomy scores) and UPSA (i.e. Finances and Communication). Based on these scores, the two-step cluster analysis identifies clusters by categorizing subjects into groups with small within-cluster variation relative to the between-cluster variation (Dillon and Goldstein, 1984). This clustering technique is commonly used in the literature (Bechi et al., 2019, 2020b), and we adopted this procedure to characterize potential functional heterogeneity within our patient sample.
Differences between clusters in demographic (age, education and sex), clinical (duration of illness, PAUSS subscores and PANSS Positive score), cognitive (BACS Attention, Executive functions, and Cognitive Index scores, and IQ), sociocognitive (PST Questionnaire and Sequencing scores and IRI subscores of Perspective Taking, Empathic Concern, Personal Distress and Fantasy) and functional scores (QLS and UPSA subscores) were evaluated using analyses of variance (ANOVAs), with Bonferroni correction (p < 0.0025) to account for multiple testing. Additionally, Bonferroni’s corrected Pearson correlation analysis (p < 0.0002) was performed to explore the relationship between demographic, clinical, cognitive, sociocognitive and functional variables in the whole sample as well as in each cluster (see Supplemental Figures S1–S3).
Next, in order to identify significant predictors of functional outcome, a backward stepwise logistic regression analysis was performed, which takes as its starting point the full saturated model and finds, through a backward elimination process, the most parsimonious set of variables that best explain the data. In this model, demographic (age, education and sex), clinical (duration of illness, PANSS Positive score, and the three PAUSS subscores of Difficulties in Social Interaction, Difficulties in Communication, and Stereotypies/Narrowed Interests), cognitive (BACS Attention, Executive functions, and Cognitive Index scores, and IQ), sociocognitive (PST Questionnaire, PST Sequencing and IRI subscores) were entered as predictors, and Cluster was entered as the dependent variable.
Analyses were performed using the Statistical Package for the Social Sciences (IBM-SPSS for MAC, Version 25). Effect sizes are reported, as appropriate, in terms of Cohen’s d and Nagelkerke R2.
Results
Sample description
Demographic, clinical, cognitive, sociocognitive and functional characteristics of the study sample are presented in Table 1.
Characteristics and functional measures of the patients overall and by cluster.
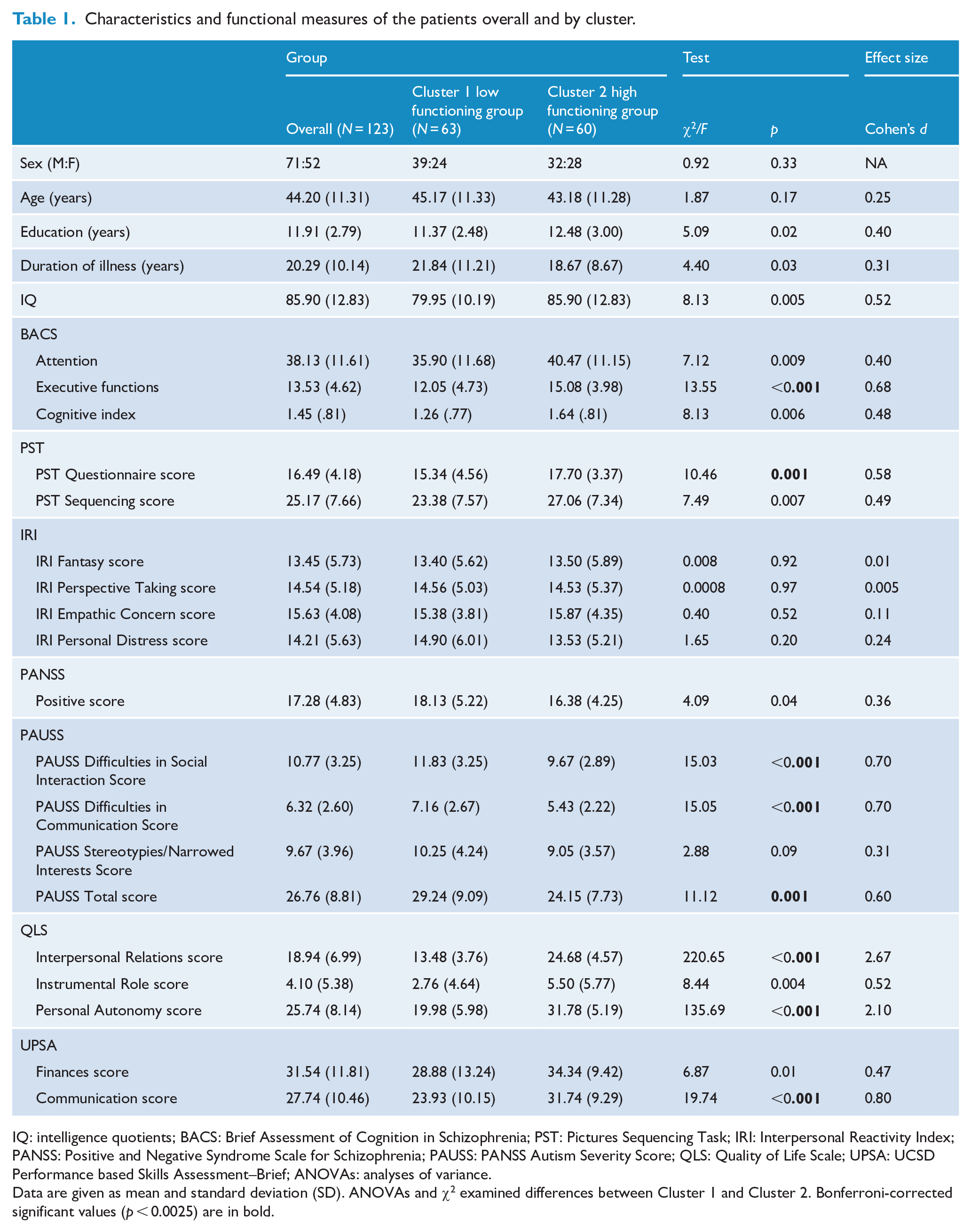
IQ: intelligence quotients; BACS: Brief Assessment of Cognition in Schizophrenia; PST: Pictures Sequencing Task; IRI: Interpersonal Reactivity Index; PANSS: Positive and Negative Syndrome Scale for Schizophrenia; PAUSS: PANSS Autism Severity Score; QLS: Quality of Life Scale; UPSA: UCSD Performance based Skills Assessment–Brief; ANOVAs: analyses of variance.
Data are given as mean and standard deviation (SD). ANOVAs and χ2 examined differences between Cluster 1 and Cluster 2. Bonferroni-corrected significant values (p < 0.0025) are in bold.
Cluster analysis
The two-step cluster analysis, using QLS subscores (i.e. Interpersonal Relations, Instrumental Role and Personal Autonomy scores) and UPSA subscores (i.e. Finances and Communication scores) as clustering variables, yielded two clusters, with 63 and 60 members (see Table 1 for Clusters characteristics; see Figure 1 for the Clusters’ functional profiles). Bayesian information criterion (BIC) value showed a maximum of 427.96, and a silhouette score of 0.3 (a measure of ‘cohesion and separation’ of clusters), suggesting a stable cluster structure.
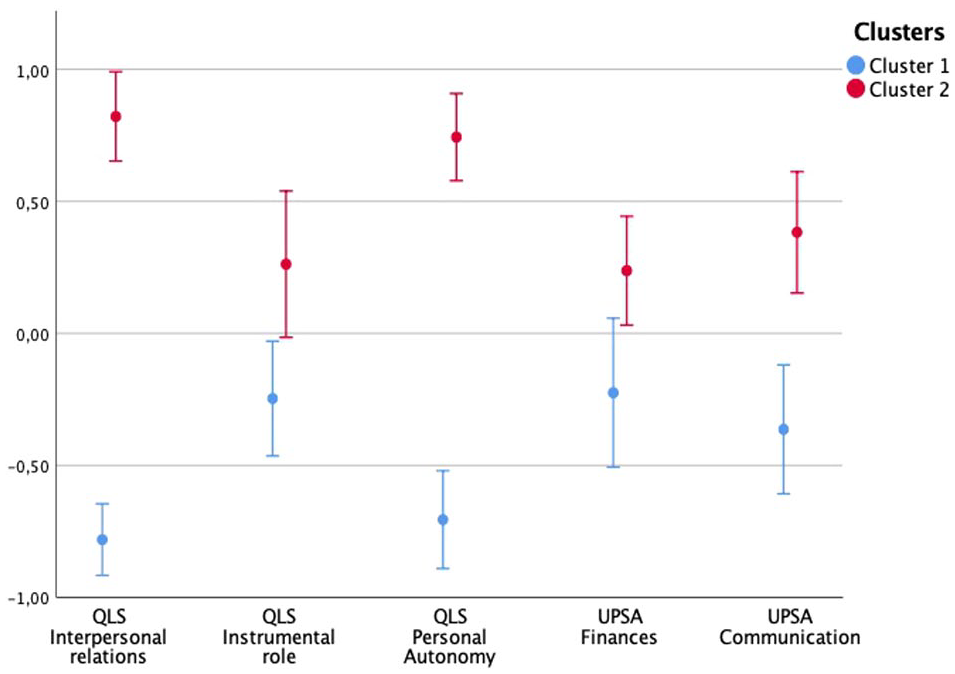
Mean functional profiles and 95% confidence intervals stratified by cluster. Data are given as standardized values.
Clusters presented significantly different demographic, clinical, cognitive, sociocognitive and functional profiles, as confirmed by the ANOVAs (see Table 1). Compared to the high functioning cluster (Cluster 2; N = 60), the low functioning cluster (Cluster 1; N = 63) showed significantly more compromised executive functioning and ToM abilities, a more severe clinical symptomatology (higher levels of overall autistic symptoms and specifically more severe difficulties in social interaction and communication), as well as a more disrupted functional outcome (lower QLS interpersonal relations and instrumental role scores and lower UPSA communication score) (Bonferroni-corrected ps < 0.0025).
Correlation analysis
Results of the Pearson correlations between demographic (age and education), clinical (duration of illness, PAUSS subscores and PANSS Positive score), cognitive (BACS Attention, Executive functions, and Cognitive Index scores, and IQ), sociocognitive (PST and IRI Total scores) and functional scores (QLS and UPSA subscores) for the whole sample and for each of the cluster are presented in Supplemental Figures S1–S3. After Bonferroni correction for multiple testing, functioning was overall moderately and negatively associated with the PAUSS difficulties in social interaction and communication and positively with IQ (all ps < 0.0002). Specifically, the PAUSS difficulties in social interaction were negatively associated with the QLS Interpersonal Relations score (r = −0.38) and the QLS Personal Autonomy score (r = −0.47). The PAUSS difficulties in communication were negatively associated with the QLS Personal Autonomy score (r = −0.40). IQ was positively associated with the QLS Personal Autonomy score (r = 0.34), the UPSA Finances score (r = 0.45) and the UPSA Communication score (r = 0.47).
Backward stepwise logistic regression
The logistic regression had a good model fit (χ2 = 38.55, p < 0.001, Nagelkerke R2 = 0.39), explaining 39% of the variance and correctly classifying 76.6% of the cases. As can be seen from Table 2, the odds of being a member of the high functioning group are significantly higher for individuals with (1) more years of education (odds ratio [OR] = 1.21, 95% confidence interval [CI] = [1.02, 1.44]); (2) higher Theory of Mind scores (PST Questionnaire; OR = 1.17, 95% CI = [1.03, 1.33]); (3) higher PAUSS Stereotypies/Narrowed Interests score (OR = 1.33, 95% CI = [1.09, 1.66]); (4) lower PAUSS Difficulties in Social Interaction score (OR = 0.79, 95% CI = [0.64, 0.97); (5) lower PAUSS Difficulties in Communication score (OR = 0.62, 95% CI = [0.45, 0.84]) and (6) being male (OR = 3.79, 95% CI = [1.35, 10.61]).
Backward stepwise logistic regression analyses.
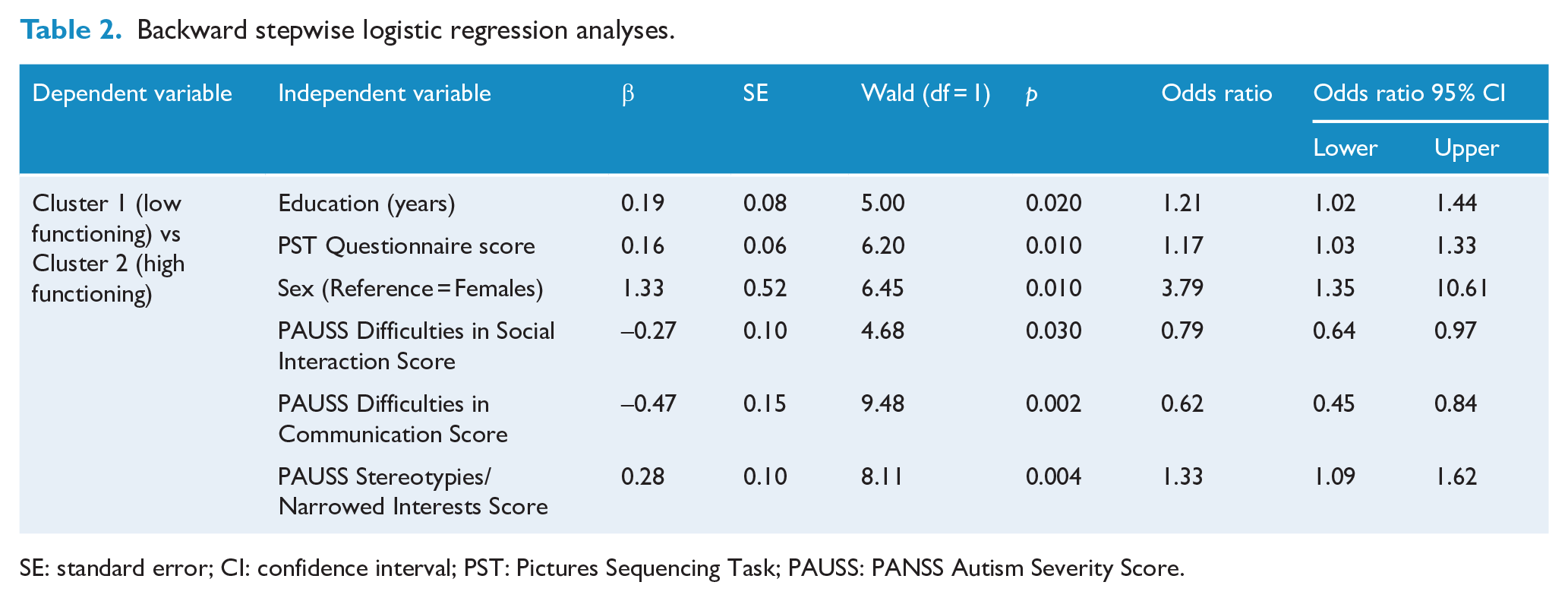
SE: standard error; CI: confidence interval; PST: Pictures Sequencing Task; PAUSS: PANSS Autism Severity Score.
Given the novelty of our findings regarding the positive association of the PAUSS Stereotypies/Narrowed Interests scores with the probability of being in the higher functioning cluster, and in order to gain a more nuanced insight into this relationship, we visualized this association in both male and female patients at three different levels of severity, defined in terms of 1 SD above the mean, at the mean and 1 SD below the mean of predictive variables of the logistic regression (see legend of Figure 2 for details). As can be seen in Figure 2, the association of the PAUSS Stereotypies/Narrowed Interests scores with high functioning is more consequential in females than males (i.e. higher scores are needed on average to pass a 0.50 probability threshold), and that increasing scores are particularly augmentative of high functioning in patients presenting average and severe profiles, but not in those with an enhanced profile.
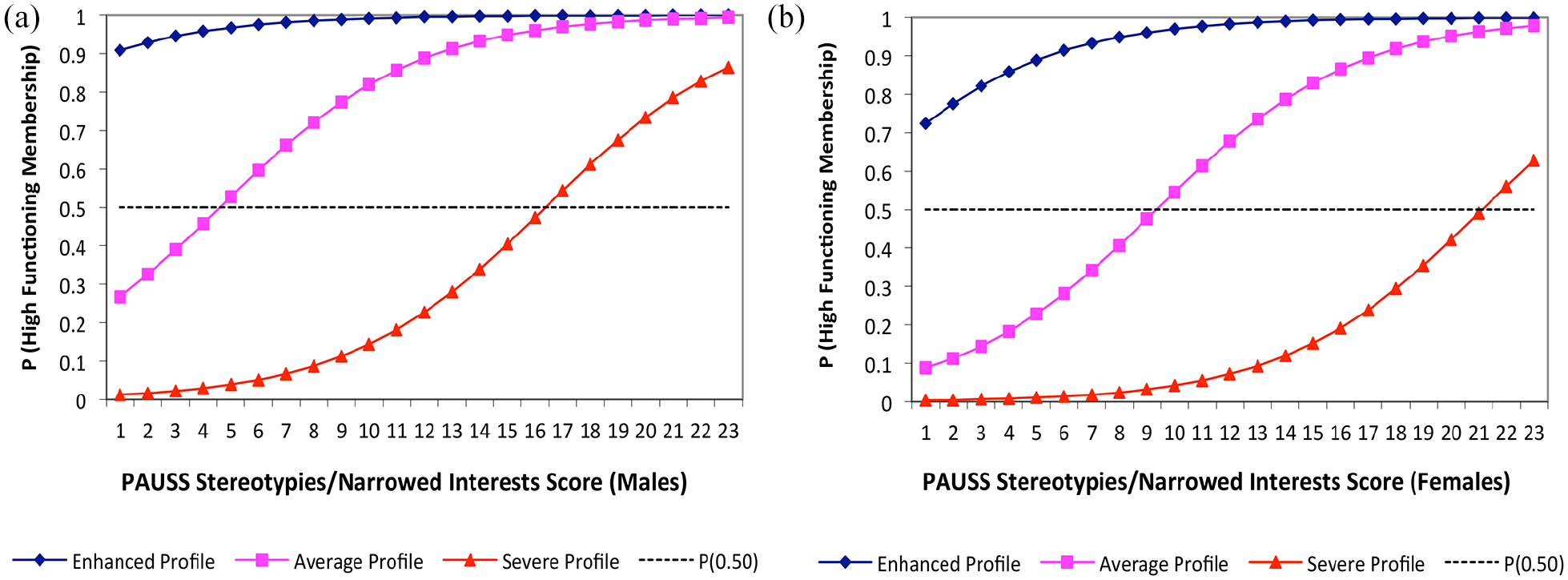
Visualization of the logistic regression showing the association of the PAUSS Stereotypies/Narrowed Interests (PAUSS-SNI) scores with the probability of being in the high functioning cluster for both male (A) and female (B) patients. In both panels, the association is depicted for three patient profiles based on the predictor variables of the logistic regression: (1) an enhanced profile defined as having scores that are 1 SD above the mean of the whole sample in education and Theory of Mind (ToM) abilities, and 1 SD below the mean in PAUSS social interaction and PAUSS communication; (2) an average profile defined as having scores that are at the mean of the whole sample in education, ToM abilities, PAUSS social interaction and PAUSS communication; (3) a severe profile defined as having scores that are 1 SD below the mean of the whole sample in education and ToM abilities, and 1 SD above the mean in PAUSS social interaction and PAUSS communication. Higher PAUSS-SNI scores are more consequential for female than male patients, and increasing PAUSS-SNI scores are particularly augmentative of the probability of high functioning in patients presenting average and severe profiles.
Discussion
The present study aimed to disentangle the influence of demographic, clinical, autistic, cognitive and sociocognitive variables on daily functioning of patients with schizophrenia, whose heterogeneity was characterized using a data-driven approach. Taking into account the heterogeneity of functional outcome in schizophrenia, we accounted for both functional capacity, assessed with QLS, and real-world functioning, assessed with UPSA, in order to create a realistic model of daily functioning. We identified two groups of patients, a low functioning group and a high functioning group, which were different in terms of functional capacity and real-world functioning (see Figure 1). The backward stepwise logistic regression revealed that demographic (i.e. sex and education), sociocognitive (i.e. ToM) and clinical (i.e. autistic symptoms) variables discriminated between the low and high functioning patient groups. Specifically, the odds for being in the high functioning group was associated with being male, having more years of education, better ToM, higher manifestation of stereotypic behaviors and narrowed interests, and more attenuated difficulties in social interaction and communication skills.
Our results are in line with previous findings showing an association between ToM and functioning (Mucci et al., 2021; Thibaudeau et al., 2021), including vocational functioning and personal life satisfaction (Thibaudeau et al., 2021). ToM impairment is considered a trait marker of the illness and has been the target of several rehabilitation programs (d’Arma et al., 2021). Studies have shown that improvement in ToM abilities results in better functioning (Bechi et al., 2013), an effect that seems to be sustained over time (Bechi et al., 2020a; Vaskinn et al., 2019). Moreover, we also observed a significant role for education, which could be considered as a measure of premorbid IQ and functioning, affecting post-onset functional outcome (Bechi et al., 2019).
Our results also confirm the significant role of autistic symptoms in affecting functional outcome in patients with schizophrenia (Ziermans et al., 2020). However, unlike previous research, which has examined the role of overall severity of autistic symptoms, we explored the differential associations of the autistic subdomains with functioning. We found that while social and communication difficulties were associated with impaired functioning, higher levels of stereotypic behavior and narrowed interests were associated with better functioning. While the association of poor daily functioning with autistic social and communication symptoms and with ToM difficulties is not surprising, it underscores the importance of targeting social components to improve daily functioning in schizophrenia.
In contrast, the association of stereotypic behavior with better functioning suggests that this autistic subdomain, or associated mechanisms, may have a positive effect on functional outcome in schizophrenia. Stereotypic behavior is a domain that is scarcely explored in schizophrenia. However, stereotyped and ritualistic behaviors, which enforce a more predictive and thus controllable environment, have been conceptualized as an adaptive response to stressors induced under conditions of unpredictability (Eilam et al., 2011). This has in fact been argued to be the case for people with ASD who putatively engage in stereotypic behaviors in order to reduce the unpredictable and often stressful nature of social and environmental demands (García-Villamisar and Rojahn, 2015). Difficulties of patients with schizophrenia to navigate the social world, and particularly in those with higher level of disorganization (Rocca et al., 2018), have been linked to deficits in prediction and planning abilities, discriminating relevant from nonessential environmental cues (Uhlhaas et al., 2006), updating and integrating new stimuli (Giersch et al., 2015) and interacting with the environment in a goal-direct manner (Rinaldi and Lefebvre, 2016). As such, we hypothesize that stereotypic behaviors in schizophrenia may be an adaptive response to their otherwise chaotic and disorganized world. While future research is needed to confirm this hypothesis, there is preliminary supportive evidence showing that compared to individuals with only obsessive-compulsive disorder—characterized by fixation on routine and ritualized patterns—or only delusional disorder, individuals with co-occurring obsessive-compulsive and delusional disorders present typical probabilistic reasoning (Fear and Healy, 1997).
Taken together, our results thus raise the intriguing possibility that daily functioning in schizophrenia can benefit from contexts in which more predictive relationships between environmental entities can systematically be established. This would be consistent with rehabilitative interventions in schizophrenia in which sociocognitive and neurocognitive remediation appear to benefit from top-down regulation aimed at systematizing the selection of relevant information and environmental cues (Bechi et al., 2013). Intriguingly, the association of higher functioning with stereotypic behavior and being male dovetails with the notion that males, compared to females, typically present higher levels of systemizing—a cognitive style characterized by proclivity to navigate rule-based systems (Baron-Cohen, 2002). In considering our results (see Figure 2), we see that while the presence of higher stereotypic behavior is particularly beneficial in promoting better functioning in those with average and severe profiles, increasing stereotypic behavior appears relatively more consequential for the female patients.
The results of this study should be considered in light of some limitations. First, patients have been followed for a long time by psychiatric services, and thus, they may not be fully representative of all patients with schizophrenia. Second, the study would have benefited from the inclusion of data concerning treatment history, such as current antipsychotic therapy and the duration of the treatment. Third, the differentiation between autistic and negative symptoms is a controversial issue, and can be clinically challenging, particularly with respect to symptoms related to social and communicative behaviors (Trevisan et al., 2020). However, genomic evidence suggests that both autistic and negative symptoms are of common origin (Taylor et al., 2015) and thus may be transdiagnostic. In addition, the convergent validity of the PAUSS with both the ADOS (Lord et al., 2000) and the ADI-R (Lord et al., 1994) gives further support to the idea that the overlap between autistic and negative symptoms may not reflect superficial similarities but rather genuine etiological commonalities (Stone and Iguchi, 2011).
Notwithstanding these limitations, our findings can have important clinical and translational implications. First, our findings underscore the potential utility of implementing routine assessments of autistic symptoms in schizophrenia (Deste et al., 2018; Kästner et al., 2015). Second, the differential effect of sex on functioning suggests that rehabilitation programs should be tailored with this difference in mind. Third, the discovery of the differential contribution of autistic subdomains on functioning in schizophrenia could help the revision of rehabilitative strategies, and particularly those concerned with mitigating the influence of autistic symptoms. One potential implication of this discovery is to explore the potential beneficial effect of stereotypic behaviors on functioning, by incorporating techniques that promote systemized thinking and/or implementing rehabilitation programs in systemized and structured environments.
Only a minority of individuals diagnosed with schizophrenia achieves recovery and a satisfactory independent living. As such, there is a need to identify predictors of functional outcome to improve treatment and services for these individuals. In addition to previously identified roles for education, theory of mind skills and psychopathological severity, we found that stereotypic behavior may be associated with improved adaptive behaviors and functioning in individuals with schizophrenia. Understanding the potential functional properties of stereotypic behavior and the nature of its mechanism could be instrumental in the identification of novel therapeutic targets and strategies of daily functioning in individuals with schizophrenia.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211038513 – Supplemental material for Theory of mind and stereotypic behavior promote daily functioning in patients with schizophrenia
Supplemental material, sj-docx-1-anp-10.1177_00048674211038513 for Theory of mind and stereotypic behavior promote daily functioning in patients with schizophrenia by Margherita Bechi, Ahmad Abu-Akel, Giulia Agostoni, Mariachiara Buonocore, Marta Bosia, Francesca Martini and Roberto Cavallaro in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.