
Abstract
Quality of life (QOL) is used as a valuable outcome measure for evaluating the impact of psychosis on patients' daily lives. Although no consensus exists regarding how to define QOL, most definitions refer to the individual's subjective satisfaction with various aspects of their lives including physical health, psychological state, social functioning and living conditions [1–3]. There is some debate regarding the capacity of people with a psychotic illness to make accurate assessments of QOL because of poor insight or the effect of their symptoms. However, validation studies of a QOL measure such as the World Health Organization Quality of Life (WHOQOL) scale [4] have shown that there is a significant correlation between results obtained from patientrated and clinician-rated QOL [5–7]. In addition, studies have shown that individuals with psychosis can make reasonable judgments about their QOL in the absence of severe psychopathology [3].
Symptomatology not only affects the ability of patients to assess QOL, but also has been assumed to play a substantial role the in the patients' QOL. In reviewing the literature regarding QOL and chronic schizophrenia, Pinikahana et al. [8] concluded that when psychopathology was considered, negative symptoms were usually found to be the most important determinant of QOL among patients with psychotic disorders. In the few published longitudinal first-episode psychosis (FEP) studies, negative symptoms were again observed to be an important determinant of QOL [9] along with depressive symptoms [10].
It is well established that individuals with psychotic disorders have impaired cognitive functioning [11], [12]. However, few studies have investigated the relationship between QOL and cognitive functioning [8], [13]. Early studies [14], [15] reported a positive relation between QOL and psychomotor speed, aspects of both verbal and visual memory and learning and verbal fluency. When the effects of cognitive dysfunction and psychopathology on QOL have been considered together, the results of crosssectional studies (focusing on mainly chronic schizophrenia) have suggested that psychopathology [16], and particularly negative symptoms [11], [17], [18] might be more strongly related to QOL than cognition.
These studies reported at least one significant relationship between QOL and cognitive functioning. Yet no individual cognitive domain was consistently associated with QOL and on balance, it would appear that both cognitive impairment and psychiatric status may be related to QOL. Clarification of these relationships has important implications for management and treatment of individuals with psychosis. Ifwe can determine specific predictors of QOL outcomes in these patients, we identify targets for remediation which might, in turn, improve their QOL.
The purpose of this study was to examine the relative contributions of neuropsychological deficits and psychiatric symptomatology to QOL. To the best of our knowledge, we are the first to report on this issue in a sample of young people who have experienced a first episode of psychosis. The aims and hypotheses of the current study were as follows:
Method
Participants
Participants were drawn from the Western Sydney First-Episode Psychosis Project, which is a longitudinal study [19]. The current paper presents only the cross-sectional results of 51 of these participants who consented to take part in the 2–3-year follow-up phase of the study. Independent sample t-tests revealed no significant differences (at α= 0.05) between the demographic characteristics of those participants who returned for 2–3-year follow-up assessment and those who did not.
Psychiatric status
According to DSM-IV [20] criteria, participants had diagnoses of schizophrenia (n = 29), schizophreniform disorder (n = 2), schizoaffective disorder (n = 6), drug-induced psychosis (n = 3), bipolar disorder (n = 8), brief psychotic disorder (n = 1) and psychotic disorder not otherwise specified (n = 2). Diagnosis was made by the consensus of three psychiatrists on the basis of a longitudinal evaluation of all available data. When assessed, 33 individuals were prescribed atypical antipsychotics with a mean chlorpromazine-equivalent dose of 390 mg day−1 (SD = 248 mg day−1) [21] and 18 were not prescribed any antipsychotic medication.
Psychiatric status was assessed using the Positive and Negative Syndrome Scale (PANSS; [22]). Ratings were performed by psychiatrists trained in the use of this scale and who had reached a satisfactory level of interrater reliability (κ<0.80). The PANSS subscales of Positive (7 items), Negative (7 items) and General Psychopathology (16 items) were used as independent variables. Depression was assessed with the Calgary Depression Scale (CDS; [23]) which is a clinicianrated measure using information provided by the patient and which has been widely used in psychosis research [6], [7]. Independent sample t-tests were performed comparing the clinical characteristics of those participants who returned for 2–3-year follow-up with those who did not. No significant differences were observed at an alpha level of 0.05.
Neuropsychological functioning
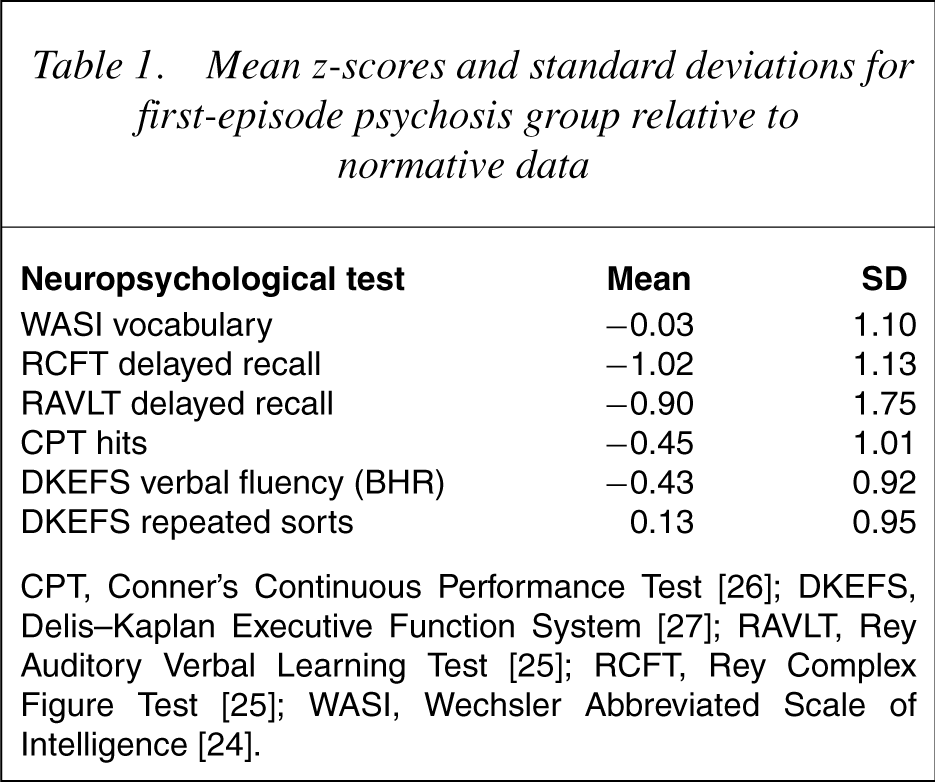
Participants completed a comprehensive battery ofneuropsychological tests at 2–3-year follow-up (see 24]; visual memory with the delayed recall score on the Rey Complex Figure Test (RCFT; [25]); verbal recall with the delayed recall score of the Rey Auditory Verbal Learning Test (RAVLT; [25]); attention with number of hits on the Continuous Performance Test (CPT; [26]); verbal fluency (BHR) from the Delis–Kaplan Executive Functioning System (DKEFS; [27]); and cognitive flexibility was assessed according to the number of repeated sorts on the Sorting Test of the DKEFS [27]. Mean z-scores (according to the published normative data indicated above) for each of these measures appear in Table 1.
Mean z-scores and standard deviations for first-episode psychosis group relative to normative data
Quality of life
The short form of the WHOQOL (WHOQOL-Brèf) [28] is a 26-item self-report questionnaire assessing QOL. It includes four domain scores (physical, psychological, social and environment) and two individually scored items measuring the individual's overall perception of their QOL and satisfaction with their physical health. All items are rated on a fivepoint Likert scale. Domain scores range from 0 to 100, whereas the individual items have a score range of 1–5. In all cases, higher scores reflect better QOL. The internal consistencyof the domain scores is generally good. For example, the Cronbach's coefficient alphas for physical (r = 0.87), psychological (r = 0.81) and environmental (r = 0.81) QOL are acceptable, although somewhat lower for the domain of social QOL (r = 0.68). This latter finding is partly because of scale length (the social domain includes only three items), but may also be attributable to the poor correlation between items [28]. Test–retest reliabilities for the domains are all excellent (r = 0.83–0.86). The four domains of QOL were used in analyses because of a lack of variability in the distributions of the two global measures (overall QOL and satisfaction with physical health).
Statistical analyses
Tests of normality revealed the dependent variables (i.e. QOL domains) to be normally distributed. In order to examine the ability of neuropsychological variables alone to predict scores on each of the four QOL domains (physical, psychological, social and environmental), separate multiple regression analyses using the backward stepwise elimination method were performed. Subsequently, the ability of psychiatric status and neuropsychological variables together to predict QOL was examined with a further four multiple regression analyses. All analyses were conducted using the Statistical Package for Social Sciences (SPSS)V 11.0 [29].
Results
At the time of testing, subjects had a mean age of 21.5 (SD = 2.9) and education of 12.1 years (SD = 1.9). Sixty-seven per cent were male. All participants were outpatients, 38 of whom lived with their family of origin. The clinical characteristics of our study sample are as follows: mean PANSS Positive subscale score 13.41 (SD = 6.03); mean PANSS Negative score 14.04 (SD = 6.48); mean PANSS General Psychopathology score 29.84 (SD = 10.08); and mean CDS score 3.06 (SD = 2.90).
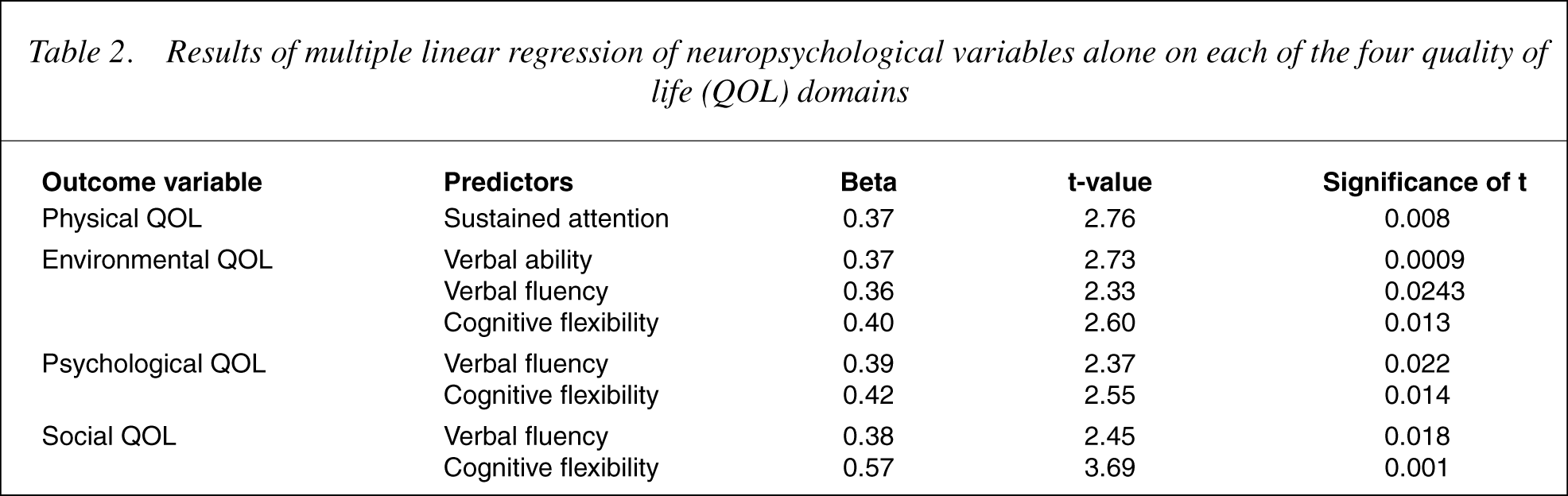
The results of multiple regression analyses using the backwardstepwise elimination method to predict the four QOL domain scores from the six neuropsychological variables are presented in Table 2. In each case QOL was entered as the dependent variable and the six neuropsychological variables were entered as independent variables. The criterion for entry into an equation was set at 0.03 to provide reasonable protection against Type 1 error. Excluded variables are not reported. All domains of QOL were significantly predicted by one or more neuropsychological variables. Specifically, physical QOL was significantly predicted by performance on a test of sustained attention (F(1,48) = 7.63, p= 0.008), which accounted for 13.7% of the variance in this outcome measure. Environmental QOL was significantly predicted by performance on tests of verbal ability, verbal fluency and cognitive flexibility (F(3,46) = 5.91, p= 0.002), which accounted for 27.8% of the variance in this outcome measure. Social QOL was significantly predicted by performance on tests of verbal fluencyand cognitive flexibility (F(2,47) = 6.93, p= 0.002), which accounted for 22.8% of the variance. Psychological QOL was significantly predicted by performance on tests of verbal fluency and cognitive flexibility (F(2,47) = 3.88, p= 0.027), accounting for 14.2% of the variance.
Results of multiple linear regression of neuropsychological variables alone on eachofthe four quality of life (QOL) domains
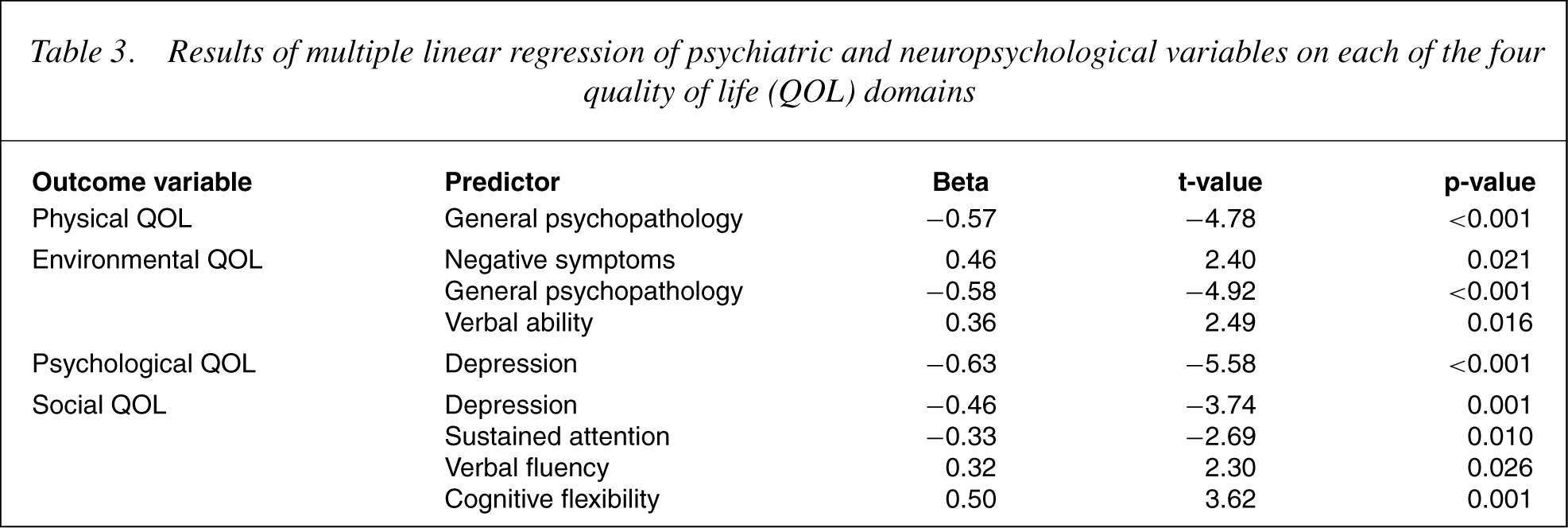
The results of further multiple regression analyses when psychiatric status variables were also entered are presented in Table 3. In these analyses, QOL was entered as the dependent variable, whereas the four psychiatric status variables and six neuropsychological variables were entered as two families of independent variables. Psychiatric variables were entered into the model first because previous research has uniformly supported the role of these variables in QOL, and neuropsychological variables were entered second as there is relatively less support for the unique contribution of these variables to QOL. The criterion for entry into an equation remained at 0.03. Psychiatric status variables were significant predictors of all four domains of QOL. The environmental and social QOL were also significantly predicted by neuropsychological variables. Physical QOL was significantly predicted by General Psychopathology (F(1,48) = 22.80, p< 0.001), which accounted for 32.2% of the variance. Environmental QOL was significantly predicted by General Psychopathology, Negative Symptoms and performance on a measure of verbal ability (F(3,46) = 11.34, p< 0.001), accounting for 42.5% of the variance. Psychological QOL was significantly predicted by the Depression score (F(1,48) = 31.09, p< 0.001), which accounted for 39.3% of the variance. Social QOL was significantly predicted by Depression and performance on tests of sustained attention, verbal fluency and cognitive flexibility (F(4,45) = 8.47, p< 0.001), which accounted for 43.0% of the variance in this outcome measure.
Results of multiple linear regression of psychiatric and neuropsychological variables on each of the four quality of life (QOL) domains
Discussion
In general, the hypothesis that neuropsychological deficits would predict diminished QOL when considered alone was confirmed. Neuropsychological variables produced small-effect sizes (variance ranging from 14% to 28%), which is broadly consistent with previous reports of significant but fairly modest associations between QOL and cognitive functioning [11],[16–18]. Verbal fluency and cognitive flexibility were found to be significantly associated with poorer ‘subjective’ QOL in three out of the four domains. This is particularly interesting in light of the common perception that executive deficits are associated with poorer insight [30].
The finding that neuropsychological functioning was unrelated to physical and psychological QOL in the presence of psychiatric status variables supported our second hypothesis and was consistent with previous reports suggesting that the relationship between neuropsychological functioning and these aspects of QOL is largely mediated by the degree of patients' psychiatric distress [11], [18].
Contrary to our expectations, however, social QOL was significantly predicted by performance on neuropsychological tests of sustained attention, verbal fluency and cognitive flexibility, and environmental QOL being predicted by verbal ability. This represents the first evidence that cognitive functioning provides a sizeable additional explanation of any aspect of QOL over and above the contribution of psychiatric symptoms. Despite this, it is important not to overinterpret the specific relationships in the absence of replication. However, an interaction of verbal fluency and cognitive flexibility with social QOL is appealing, given the need for adequate communication abilities for reasonable social interaction.
Interestingly, higher negative symptoms were also associated with higher environmental QOL, which goes against the published works that report a negative correlation between QOL and overall negative symptomatology [8]. Again this finding requires replication.
In line with our third hypothesis, psychiatric status predicted QOL (when entered with the neuropsychological variables). Lower General Psychopathology scores predicted higher physical and environmental QOL, whereas lower depression predicted higher psychological and social QOL. It is important to remember that the PANSS General Psychopathology scale includes items that rate depression, so the agreement of both measures of psychopathology may well represent the overwhelming importance of depression to QOL.
The relationship between social and psychological QOL was specifically with depression as measured by the CDS, supporting the primary role of mood over positive and negative symptoms. This finding is certainly consistent with several previous reports in chronic schizophrenia [16], [31], [32]. Moreover, Priebe et al. [10] found changes in depression and anxiety over time to correlate with changes in QOL reports in their sample of FEP patients. However, given that the bulk of prior research has suggested a primary role for negative symptoms in QOL, it may have been expected that they would emerge as a significant predictor in the current study. This was not observed.
Our results inevitably reflect our choice of instrument. Unlike the Quality of Life Scale [33], which was developed assuming that primary enduring negative symptoms of schizophrenia would impact upon patients' life satisfaction [34], [35], the WHOQOL-Brèf was not. This may make our findings more difficult to compare with other studies, and until a ‘gold-standard’ measure of QOL is established, will be a continued source of confusion in published works.
It is possible that the failure to identify a consistent relationship between negative symptoms and QOL may have resulted from the youth and lack of chronicity in our sample. Subjects had relatively low levels of negative symptoms and had mostly recovered from their initial psychotic episode. The dependence on chronic and institutionalized samples in other studies may at least partly account for their findings of an association between negative symptomatology and QOL. However, the average degree of depressive symptomatology in our sample was also quite low, but still emerged as being highly predictive of two aspects of QOL (psychological and social). In addition to low levels of depression, our sample showed low overall levels of positive symptomatology and cognitive impairment. Thus, by Katschnig's [3] reasoning, it would follow that the assessment of QOL in our sample was valid.
The issue of cross-sectional versus longitudinal studies in this area is important. The present study, although cross-sectional, has identified variables that will be examined over time. The next step will be to track the longitudinal relationships of symptoms and cognitive function to QOL.
This study underlines important treatment issues. If the aim of treatment is to improve our patient's overall wellbeing and not just to reduce psychotic phenomena in this cohort of young people, more attention is required in the management of their depressive symptoms. Further treatment targeting specific cognitive disabilities is also likely to materially improve their QOL. The inclusion of a QOL measure would appear to be a valuable additional assessment in the evaluation of treatment outcome.