
Abstract
Objectives:
There is limited evidence on the impact of parental mental health problems on offspring’s educational outcomes. We investigated the impact of maternal anxiety and depressive symptoms, as well as paternal emotional problems on the educational outcomes of their adolescent and young adult offspring.
Methods:
We used data from a longitudinal birth cohort recruited between 1989 and 1991 in Australia (the Raine Study). The Depression, Anxiety and Stress Scale was used to assess maternal depressive and anxiety symptoms, and a self-reported question was used to measure paternal mental health problems. Both were assessed when the offspring was aged 10 years. Outcomes included offspring’s self-reported education attainment—not completing year 10 at age 17, not attending tertiary education at ages 17 and 22 and primary caregiver’s reports of offspring’s academic performance at age 17.
Results:
A total of 1033, 1307 and 1364 parent–offspring pairs were included in the final analysis exploring the association between parental mental health problems and offspring’s academic performance at school, completing year 10 and attending tertiary education, respectively. After adjusting for potential confounders, the offspring of mothers with anxiety symptoms were 3.42 times more likely than the offspring of mothers without anxiety symptoms to have poor or below-average academic performance (odds ratio = 3.42; 95% confidence interval = [1.31, 8.92]) and more than 2 times more likely to not attend tertiary education (odds ratio = 2.55; 95% confidence interval = [1.10, 5.5.88]) and not to have completed year 10 (odds ratio = 2.13; 95% confidence interval = [1.04, 4.33]). We found no significant associations between maternal depressive symptoms or paternal emotional problems and offspring educational attainment.
Conclusion:
Maternal anxiety symptoms, but not depression and paternal emotional problems, are associated with poor educational attainment and achievement in adolescent offspring. The findings highlight that efforts to improve the outcomes of offspring of mothers with anxiety could focus on educational attainment.
Background
Evidence from the World Health Organization (WHO, 2001) on global mental health shows that roughly one in four people globally experience at least one mental health problem in their lifetime, commonly anxiety and depression. The prevalence estimates approach 50% in some countries (Wittchen and Jacobi, 2005). For example, a national health survey of 4181 participants in Germany found that about 43% of the adult population had experienced at least one mental disorder in their lifetime (Jacobi et al., 2004). In Australia, a national survey of mental health and wellbeing of Australians aged 16–85 years revealed that nearly half of the population (45%) had experienced at least one mental disorder in their lifetime (Australian Bureau of Statistics [ABS], 2008).
Notably, evidence suggests that roughly 68% of women and 57% of men with mental health problems are parents (Royal College of Psychiatrists, 2014). The presence of mental health problems in parents is associated with increased risk of poor cognitive functioning (Byrne et al., 1999; Erlenmeyer-Kimling et al., 2000) and considerable delays in neuromotor (Erlenmeyer-Kimling et al., 2000; Niemi et al., 2003), behavioral and social-emotional developments in the offspring (Niemi et al., 2003). These problems in turn are linked with poor academic achievements in those affected (Comes et al., 2019). Thus, early identification of and interventions for parental mental health problems may be critical to reduce and possibly prevent adverse educational outcomes in their offspring. Findings from observational studies show that the offspring of parents with mental health difficulties, including depressive and anxiety symptoms, are found to have lower classroom engagement, lower grades, higher school absenteeism and greater special education needs (Billings and Moos, 1983; Hay et al., 2001; Paget et al., 2018; Ranning et al., 2018; Shen et al., 2016). They are also more likely to drop out of school and not engage in tertiary education (Paget et al., 2018).
There are many potential explanations for the association between parental mental health problems and offspring poor academic attainment. Mental health problems in parents may interfere with optimal parenting and the ability to provide care and emotional supports to children across the developmental years (Coleman and Karraker, 1998; Oyserman et al., 2000, 2005). Environmental influences, such as exposure to parental psychological distress and growing up in a family environment with social challenges, are other possible explanations (McLoyd et al., 1994). Parental mental health problems can also have a negative impact on social, cognitive, emotional and behavioral development, which are in turn linked to poor educational attainment (Barnes and Stein, 2000; Manning and Gregoire, 2009; Murray and Cooper, 2003). Furthermore, the association could also be due to parental mental health problems impacting offspring’s physical health such as low birth weight and malnutrition, which in turn lead to poor educational performance at schools (Islam, 2015; Pierce et al., 2019).
Most evidence on this subject has focused on maternal mental health problems during the perinatal period, while there is a paucity of data regarding exposure into late childhood. Very little is also known about the role of paternal mental health status in the association. The few studies on the subject are mostly cross-sectional and case–control in design, characterized by small sample sizes and poor adjustment for potential confounders. Most studies reporting on the impacts of maternal and paternal mental health problems on the educational outcomes of the offspring focus on the associated effects during the perinatal period (Billings and Moos, 1983; Hay et al., 2001; Paget et al., 2018; Ranning et al., 2018; Shen et al., 2016), with one study reporting the impact on offspring exposed to parental mental illness at any time (Laurens et al., 2020). To the best of our knowledge, there are no prior studies that have investigated the association between parental mental health problems during child development and offspring’s educational outcomes in late adolescence and early adulthood involving a wide range of educational attainment parameters. Furthermore, unlike the aforementioned studies that considered paternal and maternal mental health exposure during pregnancy and postpartum periods, this study investigated exposures in late childhood. Understanding whether or not there exists an increased risk of lower educational attainment following exposure to parental mental health problems in late childhood is critical to better understand the impact of those problems and target prevention and intervention strategies. The overall objective of this study is, therefore, to fill the gaps in the literature by examining the risk of poor academic attainment (including completing year 10, attending tertiary education and overall academic performance) in adolescents (generation 2) of parents with mental health symptoms, including paternal emotional problems (generation 1), using robust data from a population-based prospective cohort study in Australia (the Raine Study).
Methods
Study population and data sources
Data were drawn from the Raine Study, a multigenerational population-based prospective birth cohort study, which contains measures of sociodemographic, clinical and environmental factors influencing the health of parents and their children. A total of 2900 pregnant women attending public antenatal care at the King Edward Memorial Hospital and a nearby private clinic in Perth, Western Australia, between May 1989 and November 1991 were enrolled in the study and resulted in 2868 live births. Detailed descriptions of the Raine Study have been published previously (Newnham et al., 1993; Straker et al., 2017) and can be found on the study website (https://rainestudy.org.au/). The study was approved by the University of Western Australia Human Research Ethics Committee, and all participants gave written informed consent.
Of the 2868 cohort participants enrolled at baseline, 1033, 1307 and 1364 parent–offspring pairs were included in the analysis of the association between maternal mental health problems (anxiety and depressive symptoms in late childhood) as well as paternal lifetime mental health problems and academic attainment in the offspring such as academic performance at school, attending tertiary education and completing year 10, respectively.
Outcomes
Educational attainment of children (attending tertiary education) was assessed using data from the tertiary institute service center (TISC) at year 22 follow-up (when the child was aged 22 years). TISC provides a platform for students who had completed year 12 to apply to selected universities in Western Australia for admission to undergraduate courses (post-secondary education). Detailed information about TISC can be found on the website (www.tisc.edu.au). In addition, self-reported educational attainment of the offspring such as completing year 10 (yes/no) and attending university (yes/no) was included as outcome variables, which were assessed at year 17 follow-up (when the child was aged 17 and 22 years). Primary caregiver–reported academic performance of adolescent offspring (at age 17 years or year 12) at school in the last g months (poor, below average, average, very good and excellent) is also included as an outcome variable.
Exposure
Maternal anxiety and depressive symptoms were assessed using Depression, Anxiety and Stress Scale (DASS-42) when the child was aged 10 (Lovibond and Lovibond, 1995). The DASS-42 contains 42 questions about anxiety, depression and stress (14 items for each symptom) with a four-level response scale (Lovibond and Lovibond, 1995). It is validated to use in adults and has shown high internal consistency for both depression and anxiety symptoms (Lovibond and Lovibond, 1995). In accordance with the recommended cut-off points of the instrument (DASS-42), we defined mothers who score 10 and above as having significant depression symptoms (normal ⩽9; mild-severe depressive symptoms ⩾10) and those mothers who score 8 and above as having significant anxiety symptoms (normal ⩽7; mild-severe anxiety symptoms ⩾8) (Lovibond and Lovibond, 1995).
A self-reported question (yes/no) was used to measure the lifetime history of emotional problems in fathers assessed when the child was aged 10. Several previous epidemiological studies have used a self-reported history of mental health problems in parents to measure the association between parental mental health difficulties and mental health difficulties and suicidality in their offspring (Bramness et al., 2010; Low et al., 2012).
Confounding variables
A range of paternal, maternal and child-related variables that have been consistently associated with both parental mental health problems and poor educational attainment in offspring were adjusted in our final multivariable logistic regression analysis. These variables included parental sociodemographic characteristics such as family income (AUD <24,000, AUD24,000–AUD35,000, AUD⩾36,000), maternal age at delivery (<20, 20–25, 25–29, 30–34, ⩾35 years), marital status (never married/de facto, married, divorced/separated or widowed), race (Caucasian and non-Caucasian) and maternal educational level (no schooling/up to year 12 or equivalent, trade or apprenticeship, certificate/diploma, university/higher degree) (Chudal et al., 2015; Ong et al., 2010); behavioral factors (current maternal smoking [0, 1–5, 6–10, 10–15, 16–20, ⩾20 years] or alcohol consumption during pregnancy [yes/no] and paternal lifetime smoking [0, 1–5, 6–10, 10–15, 16–20, ⩾20 years]) (Boksa, 2017; Rogers and Reese, 1964); and child-related factors, including child’s gender, attention deficit hyperactivity disorder (ADHD) symptoms, offspring asthma and birth weight (Islam, 2015; Ong et al., 2010). ADHD symptoms were assessed using Diagnostic Statistical Manual of Mental Disorders oriented scales of the Child Behavior Checklist (Achenbach et al., 2003).
Statistical analysis
Comparisons of the frequency and distribution of key covariates were made across all three educational attainment–related outcomes (self-reported academic performance, tertiary education attendance and grade 10 completion) using analysis of variance (ANOVA) and chi-square tests. We modeled the outcome (academic attainment) as a binary categorical variable and compared the proportion of parental- and offspring-related key covariates across the categories before conducting our main regression analysis models for the relationship between the exposure and outcome variables.
We used logistic regression analysis to examine the association between parental mental health problems and the risk of poor educational attainment, computing odds ratio (OR) as a measure of effect. We conducted the analysis in two models: model 1 (unadjusted model) and model 2 (adjusted model). Model 2 was adjusted for the following potential confounders: sociodemographic factors including parental age, race, maternal educational attainment, marital status and income; maternal substance use (smoking and alcohol use before and during pregnancy); paternal smoking (lifetime smoking); and offspring-related variables such as ADHD symptoms, gender and birth weight.
To account for the missing data in our analysis, we employed multiple imputation by chained equation (Tan et al., 2018). To predict the missing data, all independent variables used in the final regression model analysis were included in the imputation model along with additional auxiliary variables, and the analysis was repeated. We imputed 100 datasets. The imputation was conducted in Stata using the ‘ice’ command. The p-value for statistical significance was set at <0.05, and all tests of significance were two-sided. All analyses were conducted in Stata/SE (version 16).
Results
Sample characteristics
Table 1 shows the comparison of the principal characteristics of the participants (both parents and offspring) according to offspring educational attainments, that is, self-reported academic performance, attending tertiary education and completing year 10. Mothers of offspring with low educational attainment (across all of the indices of educational attainment) were more likely to report low educational status, low income, anxiety symptoms, tobacco smoking during pregnancy and alcohol consumptions during pregnancy compared with mothers of offspring with good educational attainment. Moreover, mothers of offspring with poor educational attainment (across all of our indices) were more likely to be younger, never married or divorced/separated/widowed when compared with offspring with good educational attainment. The fathers of offspring with poor educational attainment (across all of our indices) were more likely to be smokers when compared with their counterparts.
Characteristics of parents and children included in the analysis according to offspring educational attainment, specifically self-reported academic performance, attending tertiary education and completing year 10.
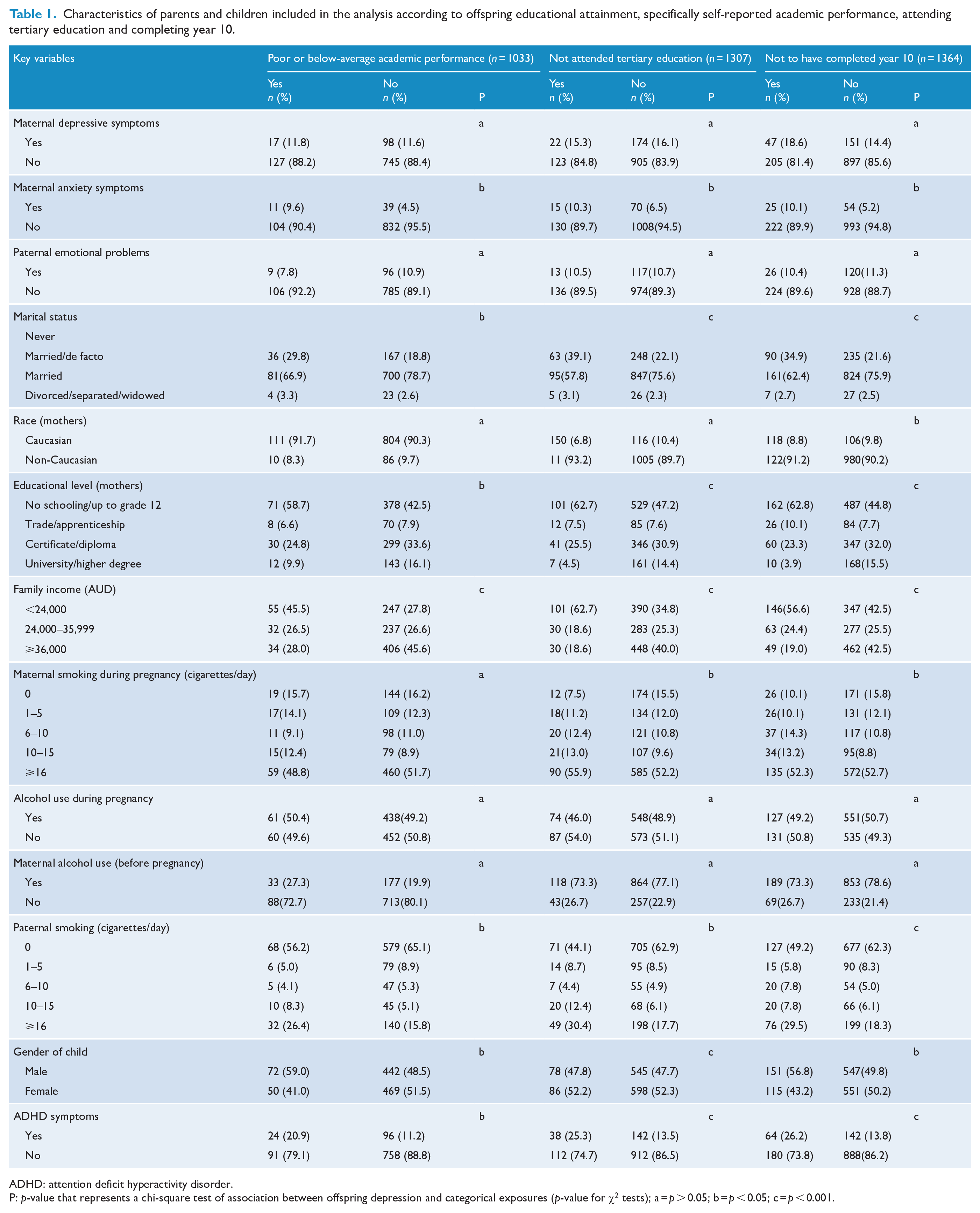
ADHD: attention deficit hyperactivity disorder.
P: p-value that represents a chi-square test of association between offspring depression and categorical exposures (p-value for χ2 tests); a = p > 0.05; b = p < 0.05; c = p < 0.001.
When we compare offspring who had poor educational attainment (across all of our indices) with their counterparts with good educational attainment, offspring with poor educational attainment were more likely to report ADHD symptoms, low birth weight and male sex compared with those offspring with good educational attainment. However, we observed no significant difference in the educational attainments of the offspring according to maternal depressive symptoms or paternal emotional problems.
We also compared the key characteristics of parents and children with data on all indices of educational attainment with those lost to follow up. In comparison with mothers included in the analysis, those lost to follow-up were more likely to be younger at baseline, non-Caucasians, unmarried, divorced, and with low educational levels and low income. They were also more likely to smoke and drink during pregnancy and to have increased rates of depressive and anxiety symptoms in late childhood. Similarly, the fathers of offspring who were excluded due to missed data were more likely to be smokers and report lifetime mental health problems when compared with fathers of offspring who were retained. Children lost to follow-up or excluded due to missing data were more likely to be males and have increased symptoms of ADHD (see Table 2).
Comparisons between offspring with completed data on educational outcomes and offspring lost to follow-up.
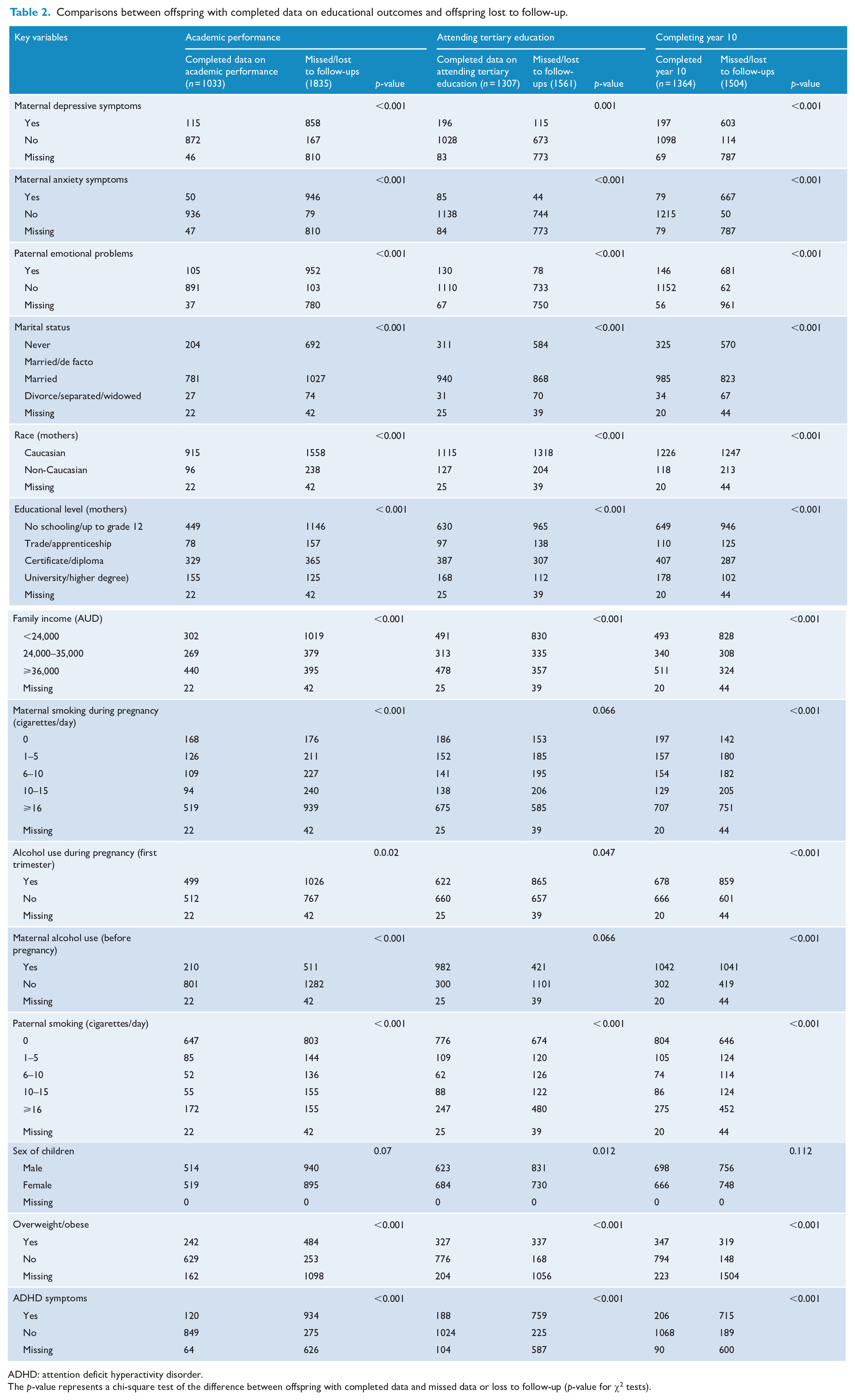
ADHD: attention deficit hyperactivity disorder.
The p-value represents a chi-square test of the difference between offspring with completed data and missed data or loss to follow-up (p-value for χ2 tests).
Associations of parental mental health problems with offspring educational attainment
As shown in Table 3, in the unadjusted analysis, we found that the offspring of mothers with anxiety symptoms were 3.60 times more likely than the offspring of mothers without anxiety symptoms to have poor or below-average academic performance (OR = 3.60; 95% confidence interval [CI] = [1.50, 8.60]), more than 2 times more likely not to attend tertiary education (OR = 2.78; 95% CI = [1.39, 5.56]) and not to have completed year 10 (OR = 2.13; 95% CI = [1.10, 4.33]). After adjusting for relevant covariates, the evidence of association remained but was attenuated for all outcomes: poor or below-average academic performance(OR = 3.42; 95% CI = [1.31, 8.92]), not attending tertiary education (OR = 2.55; 95% CI = [1.10, 5.88]) and not completing year 10 (OR = 2.13; 95% CI = [1.10, 4.33]).
Association between parental mental health problems with offspring educational attainment, specifically self-reported academic performance, attending tertiary education and completing year 10.
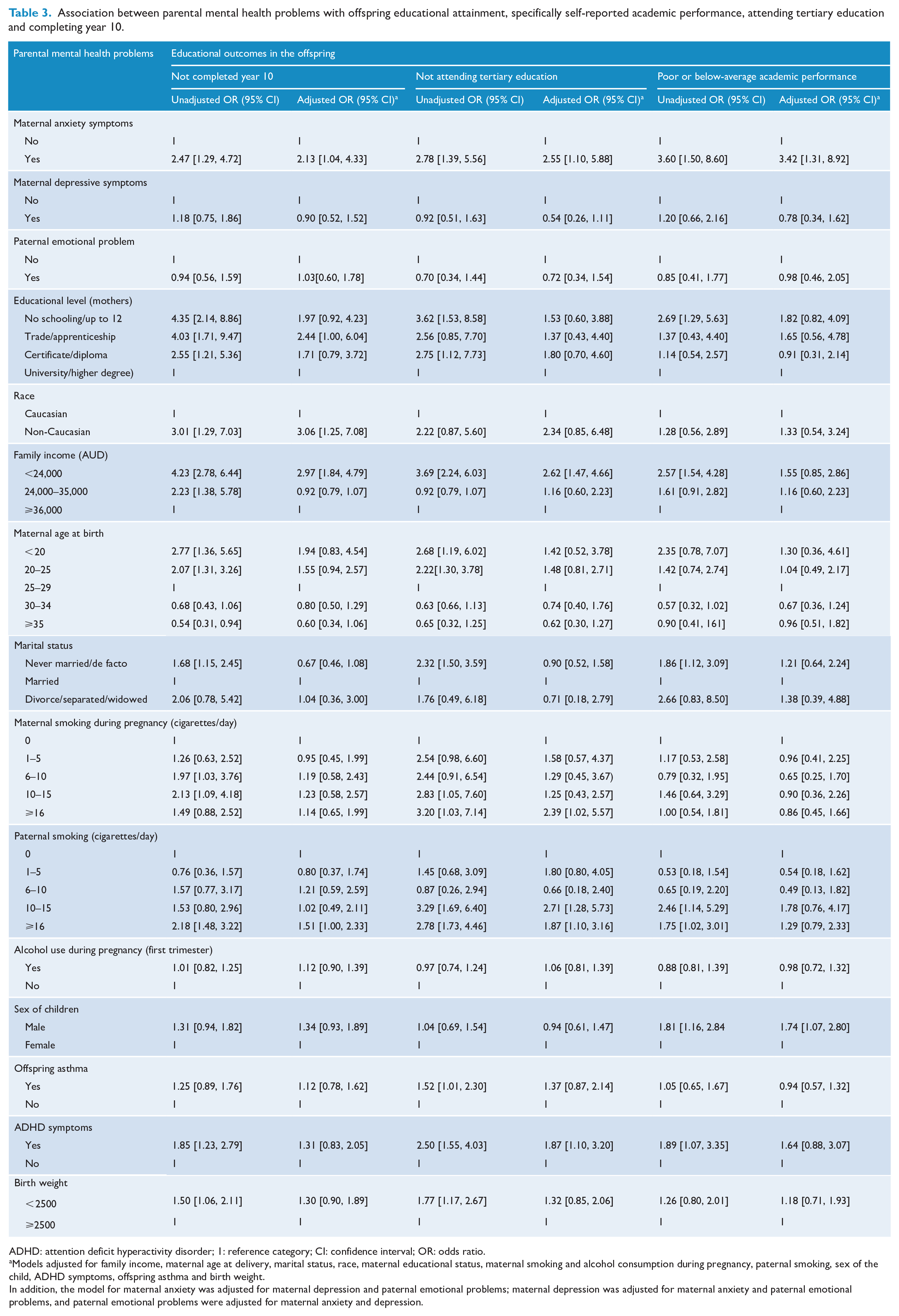
ADHD: attention deficit hyperactivity disorder; 1: reference category; CI: confidence interval; OR: odds ratio.
Models adjusted for family income, maternal age at delivery, marital status, race, maternal educational status, maternal smoking and alcohol consumption during pregnancy, paternal smoking, sex of the child, ADHD symptoms, offspring asthma and birth weight.
In addition, the model for maternal anxiety was adjusted for maternal depression and paternal emotional problems; maternal depression was adjusted for maternal anxiety and paternal emotional problems, and paternal emotional problems were adjusted for maternal anxiety and depression.
Conversely, we observed no significant associations between maternal depressive symptoms or paternal emotional problems with offspring with any poor educational achievements (poor or below-average academic performance, not attending tertiary education and completing year 10) in both the unadjusted and adjusted analyses (Table 3). When we repeated the analysis based on the imputed datasets, the association remained broadly consistent with the complete case analysis (Supplementary Table 1).
Discussion
Summary of the main findings
In this study, we investigated the association between maternal anxiety and depressive symptoms as well as paternal emotional problems and the risk of offspring’s poor educational attainment. This was assessed as self-reported poor academic performance, not attending tertiary education and not completed year 10 schooling, using data from a prospective multigenerational birth cohort study in Western Australia (the Raine Study). To the best of our knowledge, this is the first study to examine maternal or paternal mental health problems measured during a child’s educational outcomes in late adolescence and young adulthood. Our results suggest that after controlling for a range of potential confounders, exposure to maternal anxiety symptoms at age 10 was associated with 3.42-, 2.13- and 2.55-fold increased odds of reporting poor academic performance, not completing year 10 and not attending tertiary education, respectively. This suggests the potential that interventions for academic performance in the adolescent offspring could address maternal anxiety symptoms during the early childhood years. We found no evidence of significant associations between maternal depressive symptoms as well as paternal mental health problems and increased odds of low educational attainment in the adolescent offspring.
Possible mechanisms and comparison to previous studies
Our results, based on population-based prospective birth cohort data, extend findings from a prior study which found a significant association between maternal prenatal anxiety symptoms and an increased risk of poor academic performance, specifically poor mathematics in adolescent offspring at age 16 years (Pearson et al., 2016). Our study adds to this evidence as it suggests that exposure to maternal anxiety during childhood is also associated with offspring’s academic difficulties later in adolescence.
Several plausible mechanisms have been proposed to explain the link between maternal anxiety and offspring poor academic performance. One of the possible explanations is that maternal mental health problems, including significant anxiety symptoms, may lead to neurodevelopmental impairments in children, specifically by causing problems in working memory (short-term memory) (Entringer et al., 2009), a memory system that is important for conscious storage and recall of information (Cowan and Sciences, 2001; Morey, 2011). Complementing the above, a 2011 study by Buss and colleagues found that maternal anxiety symptoms were linked to impairment in children’s working memory (Buss et al., 2011), which in turn was associated with problems in reading and academic achievements in school (Engel de Abreu et al., 2014). The other putative mechanisms linking maternal anxiety symptoms and problems in academic achievement in the offspring include poor relationships between the mother and their children due to maternal anxiety, leading to poor parental stimulation and reduced involvement in learning (El Nokali et al., 2010; Mattejat and Remschmidt, 2008). Evidence suggests that parental involvement in schools is often considered as a pathway through which schools enhance achievements and address the underperformance of students (Berger, 1991; Hill and Tyson, 2009) and was also positively associated with offspring academic performance (Topor et al., 2010). Furthermore, maternal anxiety has been linked to reduced family functioning or dysfunctional family structure, possibly leading to separation, divorce, economic distress and hardships, as well as a conflict between the parents, consequently leading to problems or decreases in academic performance in the offspring (Behere et al., 2017). However, in this study, we have adjusted the final model for many of those factors, and therefore this is an unlikely interpretation.
In this study, maternal depressive symptoms were not linked to poor academic performance in offspring, which is consistent with one previous study (Augustine and Crosnoe, 2010) but not other studies (Lin et al., 2017; Netsi et al., 2018). For example, a 2017 study conducted by Lin and colleagues found that offspring of mothers with major depression were more likely to perform below the benchmark in numeracy (OR = 1.22; 95% CI = [1.07, 1.39]), spelling (OR = 1.30; 95% CI = [1.15, 1.46]) and writing skills (OR = 1.40; 95% CI = [1.21, 1.62]) at age 12 (grade 7) when compared with the offspring of those mothers with no known mental health disorders (Lin et al., 2017). The discrepant findings could be due to the instrument used to ascertain both the exposure and outcome. We used screening instruments for mental health symptoms and self-reported performance, whereas Lin et al. used diagnostic measures of mental health disorders consistent with International Classification of Diseases (ICD) codes and standard cut-offs scores for educational outcomes. The other possible reason for the observed discrepancy might be the differences in the severity and persistence of symptoms of depression in mothers included in the studies. Lin et al. used linked data of mothers who had an inpatient hospital admission or outpatient contact recorded on the Hospital Morbidity Data System and Mental Health Information System. Mothers recorded in these systems are likely to have relatively severe depression, while the self-reported measures we used would also have picked up mothers with milder and intermittent symptoms of depression in our study. Complementing this interpretation, a recent longitudinal study found that the offspring of mothers with severe and persistent postnatal depression were more likely to get lower mathematics grades at 16 years of age when compared with their counterparts (OR 2.65; 95% CI = [1.26, 5.57]) (Netsi et al., 2018).
Concerning paternal mental health exposure, we found no evidence that paternal emotional problems were associated with increased risks of poor educational attainment in the offspring. This finding is consistent with the results of a prior longitudinal birth cohort study that found no association between paternal mental health problems and poor academic performance in English and mathematics in adolescent offspring aged 16 years (Pearson et al., 2016).
Strength and limitations
Our study has several strengths, including the use of population-based longitudinal study design, reliable measures to assess exposure variables (maternal mental health) and large sample size. Extensive adjustment of the relevant confounding variables and conducting multiple imputation to account for the effects of missing data on the reported findings were the other strengths of the study.
A number of limitations of the study have to be acknowledged: First, we observed high attrition rates or missing follow-up data in our final complete case analysis. Compared with mothers included in the analysis, mothers of children who were lost to follow-up were more likely to be younger at baseline, non-Caucasians, unmarried, divorced and report lower levels of education and low income. Offspring’s fathers lost to follow-up were more likely to be smokers and have mental health problems. Children lost to follow-up were more likely to have increased symptoms of ADHD. These factors have been associated with increased risks of poor educational outcomes in previous studies (Chudal et al., 2015; Ong et al., 2010). Thus, had these participants remained in the study, it is conceivable that we would have observed a stronger effect in the association between maternal mental health problems and offspring’s educational attainments. When we further explored the impact of attrition on our findings, we used multiple imputation for missing data and reran all analyses using the imputed dataset values and showed that our findings were robust. In addition, a 2017 study conducted by White et al. (2017) to assess the potential bias from attrition in the Raine Study suggests no evidence of selection bias. Educational performance or attainment of the offspring was based on a self-rated questionnaire (no standard instrument was used), which might underestimate the true effects of the associations. Moreover, one of the exposure variables (a mental health problem in fathers) was a self-report of lifetime mental health problems, and thus there are possibilities of recall bias as well as undiagnosed bias, which might underestimate the true magnitude and associated effects of paternal mental health problems on child outcome. Another limitation is that some important variables such as psychiatric problems during pregnancy were not available.
Not using the actual grade as a measure of academic performance is the other limitation of this study. In fact, epidemiological data suggest that self-reported or parent-reported academic performance was found to be strongly correlated with the actual grades, which confirms the robustness of our findings (Gilger, 1992; Sticca et al., 2017). In addition, in this study, we have used parent-reported academic performance instead of self-reported performance, and the existing scientific evidence suggests that parent-reported associations (results) were stronger than self-reported associations (Gilger, 1992). Nevertheless, Gilger et al. (1992) found that the association was significant in both parent-reported and self-reported academic performance with a strong correlation between the two reports. Further studies using the actual grades as the measures of academic performance are needed to strengthen and confirm our findings. The reliance on self-reports of tertiary education as an indicator of good educational attainment is another limitation of the study and should be interpreted with caution. Young people with entry scores above the minimum standard but no aspirations for higher education or unable to engage in tertiary education due to family or personal issues may have been missed. Therefore, future studies using objective measures of academic achievement are required to strengthen and confirm our findings.
Conclusion
This population-based prospective birth cohort study demonstrates that after adjusting for maternal, paternal and offspring-related potential confounders, exposure to maternal anxiety symptoms at the age of 10 (grade 5) was associated with an increased odds of having poor or below-average academic performance, not attending tertiary education and not completing year 10 in the adolescent offspring at age 17. No significant associations were found between maternal depressive symptoms or paternal emotional problems with offspring’s poor educational achievement. The findings highlight that efforts to improve the educational attainment of children might need to support kids with maternal anxiety symptoms. In addition, future studies investigating better strategies to improve the educational performance of children with maternal anxiety symptoms are warranted.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211025633 – Supplemental material for The impact of parental mental health problems on the educational outcomes of their offspring: Findings from the Raine Study
Supplemental material, sj-docx-1-anp-10.1177_00048674211025633 for The impact of parental mental health problems on the educational outcomes of their offspring: Findings from the Raine Study by Getinet Ayano, Ashleigh Lin, Berihun Assefa Dachew, Robert Tait, Kim Betts and Rosa Alati in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We are sincerely thankful to all the families who took part in this study, as well as the whole Raine Study team including data collectors, cohort managers, data managers, data officers, clerical staff, research scientists and volunteers.
Author Contributions
G.A. was involved in study design, conceptualization, data analysis, interpretation of data and drafting the manuscript. K.B., R.T., A.L., B.A.D. and R.A were involved in data analyses, interpretation of data and critical revisions of the manuscript for important intellectual content. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The National Health and Medical Research Council (NHMRC) for long-term contribution to funding the Raine study since inception, The Raine Medical Research Foundation, Curtin University, The University of Western Australia, Telethon Kids Institute, Women and Infants Research Foundation, Edith Cowan University, Murdoch University and The University of Notre Dame Australia are acknowledged for their support and funding of the core management of the Raine Study. The 17-year follow-up of the Raine Cohort was supported by the National Health and Medical Research Council Program Grant Nos 353514, 1099655 and 1173991. The 22-year Raine Study follow-up was funded by NHMRC project grants 1027449, 1044840 and 1021855. Funding was also generously provided by SafeWork Australia. A.L. is funded by an NHMRC Career Development Fellowship (No. 1148793). G.A. is funded by Curtin University through Curtin International Postgraduate Research Scholarship (CIPRS). The funders had no further role in the study design, data collection, and analysis and interpretation of the results. In addition, the funders have no role in writing the reports and the decision to submit the paper for possible publication.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.