
Abstract
Since the inception of the National Mental Health Strategy in 1992, substantial reforms have been made to Australia's mental health service system. Early reforms focused on State/Territory-based, public sector, specialist mental health services, and involved increasing the emphasis on community-based care, decreasing the reliance on stand-alone psychiatric hospitals, and ‘mainstreaming’ acute psychiatric beds into general hospitals. Later reforms have been broader in focus, and have considered a wider range of mental health service providers, most notably those working in a primary care setting. In particular, initiatives such as the Better Outcomes in Mental Health Care (Better Outcomes) programme and the Better Access to Psychiatrists, Psychologists and General Practitioners through the Medicare Benefits Schedule (Better Access) programme have been established to improve access to general practitioners, allied health professionals (particularly psychologists) and psychiatrists. The early reforms focused largely on people with severe and disabling low prevalence disorders such as psychotic disorders, whereas the later reforms have expanded the emphasis to include high prevalence disorders such as affective disorders and anxiety disorders [1, 2].
A number of administrative datasets are available that provide a partial picture of service use for mental health problems in Australia. States/Territories routinely submit data on hospital admissions and community-based contacts through the Admitted Patient Mental Health Care National Minimum Data Set and the Community Mental Health Care National Minimum Dataset, respectively, which are managed by the Australian Institute of Health and Welfare [3]. Data on visits to allied health professionals that occur through the Better Outcomes programme are submitted by Divisions of General Practice to a national minimum dataset, which is held by a team at the University of Melbourne, on behalf of the Commonwealth Department of Health and Ageing [4]. Data on visits to general practitioners, allied health professionals and psychiatrists that occur through the Better Access programme and data on other Medicare-funded services are held by Medicare Australia [5]. It is difficult to accurately gauge overall patterns of service use for mental health problems, however, because each of these data sources has its own system of unique identifiers that cannot be linked. In addition, little information is available from these data sources that provide information on the kinds of mental disorders that are treated.
Data from the 2007 National Survey of Mental Health and Wellbeing (2007 NSMHWB) provide a unique opportunity to examine current service use for mental health problems in Australia in a more comprehensive way, because the survey sought information from individuals about both their use of inpatient services and their contacts with a range of community-based providers. These survey data also enable service use to be examined in the context of mental disorders. This paper provides a snapshot of 12 month rates of service use for mental health problems by the general population and by those with mental disorders.
Method
Sampling and procedure
The NSMHWB was conducted between August and December 2007 by trained interviewers from the Australian Bureau of Statistics (ABS). The ABS identified a stratified random sample of households, and interviewers identified those aged between 16 and 85 years in each through a set of household composition questions. Once the household composition was known, the interviewer selected the specific person to be interviewed, using an algorithm developed by the ABS. If that person declined, no further attempt was made to recruit from that household. The algorithm oversampled younger people (16–24 years) and older people (65–85 years), in order to improve the reliability of estimates for these groups. This sampling process yielded 8841 fully responding households, or a response rate of 60%. Interviews took place in respondents’ homes and took an average of 90 minute. Further detail about the sampling and procedure can be found elsewhere [6, 7].
Survey instrument
The survey instrument was based on the current version of the World Mental Health Composite International Diagnostic Interview (WMH-CIDI 3.0), and relied on the respondent being sufficiently proficient in English to complete it. It sought information on the respondent's mental health status, permitting a judgement to be made about whether they met criteria for an affective disorder, an anxiety disorder and/or a substance use disorder during their lifetime, and had experienced symptoms or an episode during the past 12 months or during the past 30 days. The survey also sought information on respondents’ severity of symptoms, levels of functioning and disability, levels of psychological distress, quality of life, physical health status, social networks and provision of care to family and friends for physical and mental health problems. Further detail about the survey instrument can be found elsewhere [6, 7]. Assessing use of services for mental health problems
In addition to the aforementioned variables, the survey contained a module on service use that was purpose-designed for the Australian context. This focused on respondents’ 12 month use of services for mental health problems. It also sought some information on 12 month use of services for physical health problems, and some information on lifetime service use. It elicited information about hospital admissions and consultations with general practitioners, psychiatrists, psychologists, other mental health professionals (including mental health nurses and other professionals providing specialist mental health services), and other health professionals (including specialist doctors or surgeons, other professionals providing general services, and complementary/alternative therapists).
Data analysis
This paper focuses on 12 month rates of service use for mental health problems. The ABS provided extract tables with weighted population estimates and standard errors from which 95% confidence intervals (95%CIs) were estimated. All data are presented as simple frequencies and percentages with 95%CIs. Differences with non-overlapping 95%CIs were treated as statistically significant. This approach is conservative: when two 95%CIs do not overlap the difference between the two estimates is statistically significant, but when they do overlap this still might reach the nominal 0.05 level of statistical significance.
Results
Use of services by the general population
12 month rates of service use for mental health problems vs sex
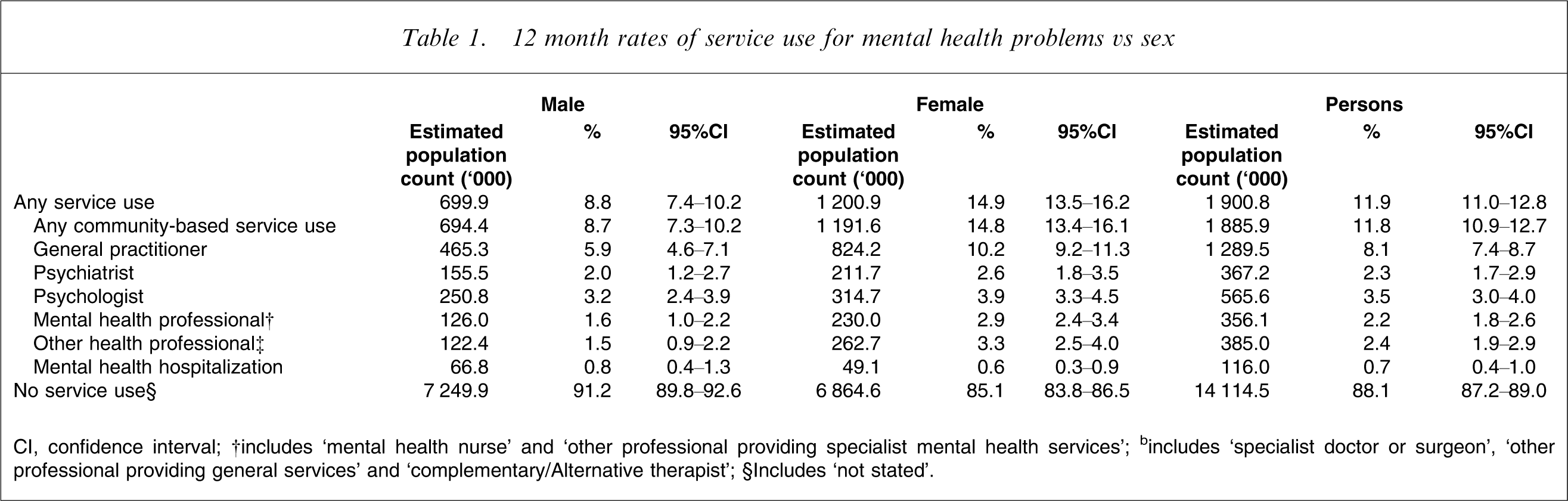
CI, confidence interval; †includes ‘mental health nurse’ and ‘other professional providing specialist mental health services’; bincludes ‘specialist doctor or surgeon’, ‘other professional providing general services’ and ‘complementary/Alternative therapist’; §Includes ‘not stated’.
Use of services by people with mental disorders
12 month rates of service use for mental health problems by people with 12 month mental disorders,† vs age and sex
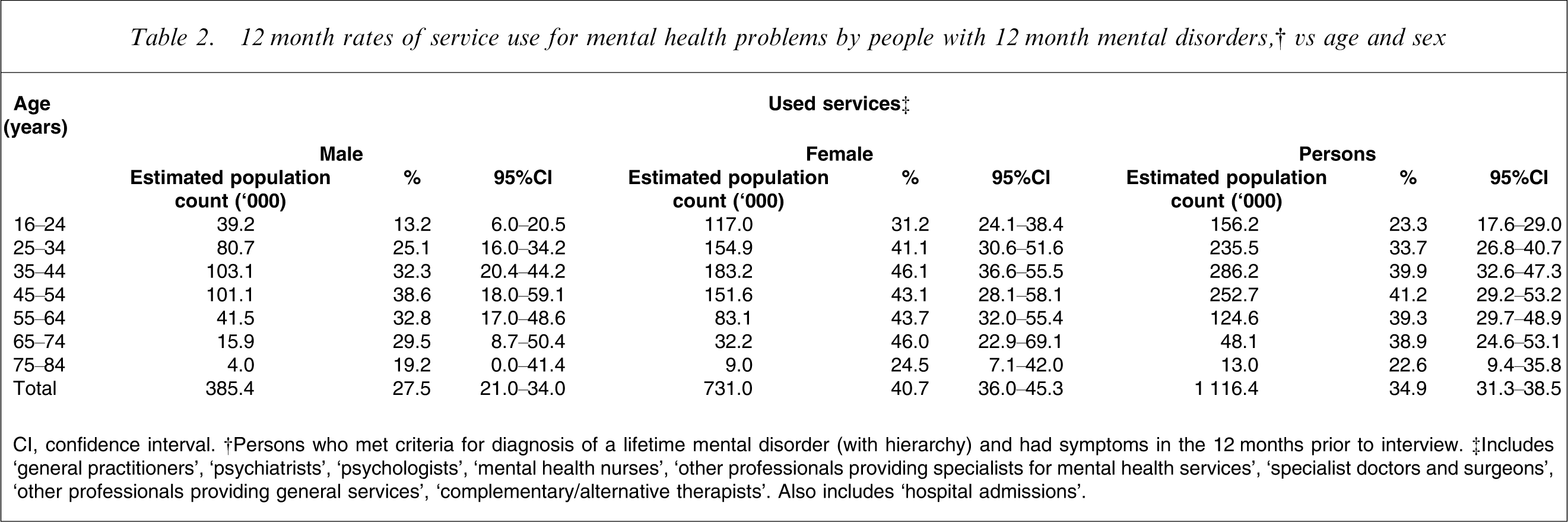
CI, confidence interval. †Persons who met criteria for diagnosis of a lifetime mental disorder (with hierarchy) and had symptoms in the 12 months prior to interview. ‡Includes ‘general practitioners’, ‘psychiatrists’, ‘psychologists’, ‘mental health nurses’, ‘other professionals providing specialists for mental health services’, ‘specialist doctors and surgeons’, ‘other professionals providing general services’, ‘complementary/alternative therapists’. Also includes ‘hospital admissions’.
12 month rates of service use for mental health problems vs mental disorder† class
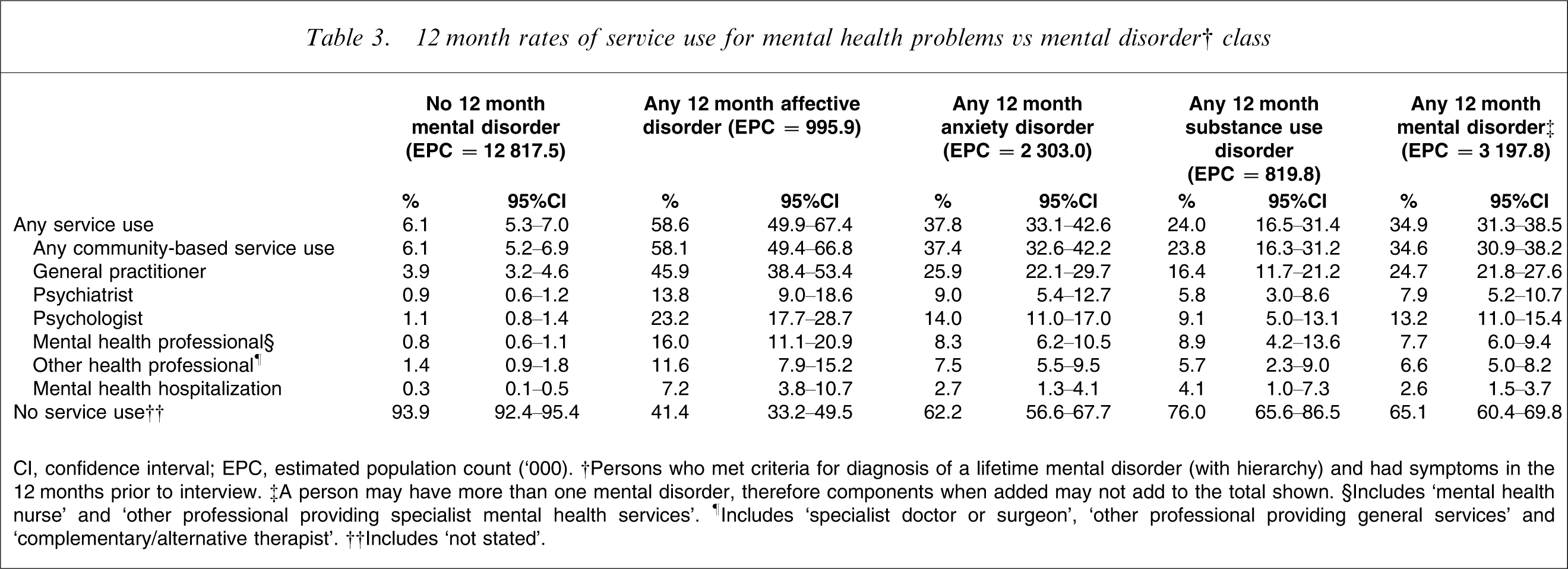
CI, confidence interval; EPC, estimated population count (‘000). †Persons who met criteria for diagnosis of a lifetime mental disorder (with hierarchy) and had symptoms in the 12 months prior to interview. ‡A person may have more than one mental disorder, therefore components when added may not add to the total shown. §Includes ‘mental health nurse’ and ‘other professional providing specialist mental health services’. ¶Includes ‘specialist doctor or surgeon’, ‘other professional providing general services’ and ‘complementary/alternative therapist’. ††Includes ‘not stated’.
Those with affective disorders were most likely to make use of services (58.6%, 95%CI = 49.9–67.4%), followed by those with anxiety disorders (37.8%, 95%CI = 33.1–42.6%) and then those with substance use disorders (24.0%, 95%CI = 16.5–31.4%). Considering the converse of this picture, around two-thirds of those with any mental disorder did not use any services for mental health problems. The same was true for two-fifths of those with affective disorders, three-fifths of those with anxiety disorders, and three-quarters of those with substance use disorders.
Among those with any mental disorder, mental health hospitalizations were relatively uncommon (2.6%, 95%CI = 1.5–3.7%). Most commonly, service use among this group involved visits to community-based providers (34.6%, 95%CI = 30.9–38.2%), particularly general practitioners (24.7%, 95%CI = 21.8–27.6%) and, to a lesser extent, psychologists (13.2%, 95%CI = 11.0–15.4%) and psychiatrists (7.9%, 95%CI = 5.2–10.7%). People with affective disorders tended to make the greatest use of all forms of services, followed by people with anxiety disorders in the case of most community-based providers, and people with substance use disorders in the case of mental health hospitalizations.
The relatively high rate of visits to general practitioners by people with 12 month mental disorders warrants further comment. Often, a general practitioner was the only provider from whom mental health care was sought. Around one-tenth of those with any 12 month mental disorder (9.8%, 95%CI = 8.2–11.4%) visited a general practitioner for mental health problems but did not receive care from any other provider. The equivalent figures for those with any affective disorder, any anxiety disorder and any substance use disorder were 16.8% (95%CI = 12.9–20.7), 10.0% (95%CI = 8.0–12.0%) and 5.2% (95%CI = 4.7–5.7), respectively.
Use of services by people with comorbid mental disorder classes
12 month rates of service use for mental health problems vs comorbidity of mental disorders†
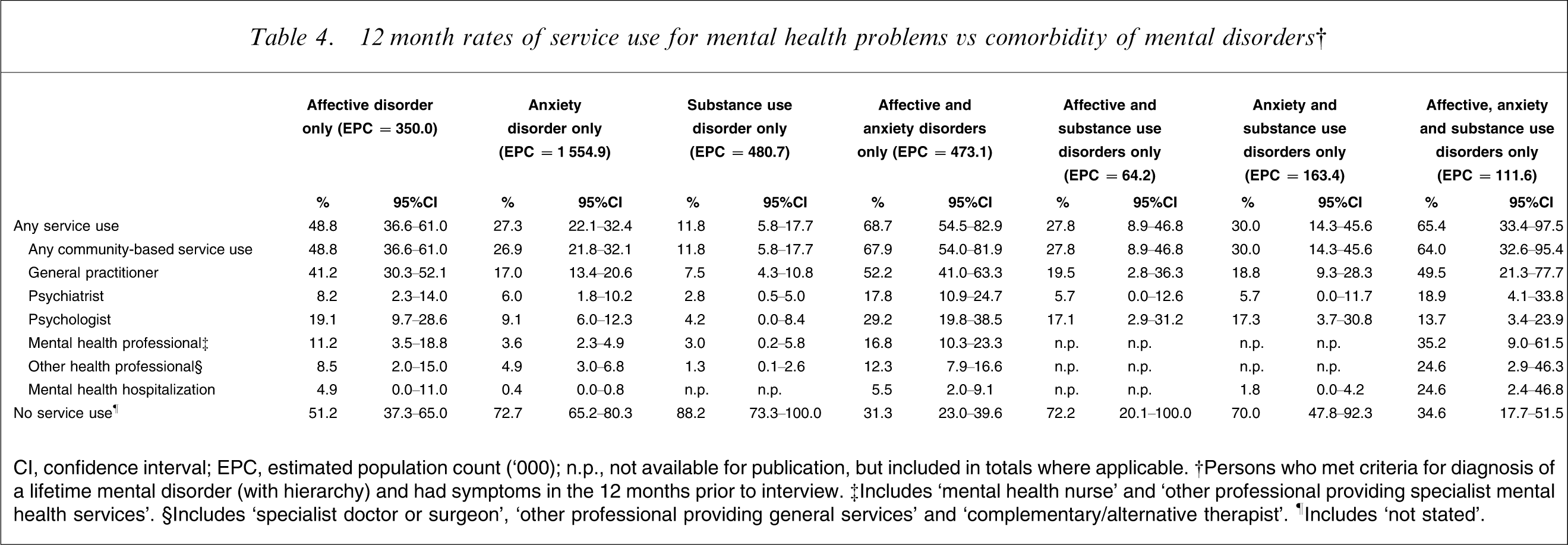
CI, confidence interval; EPC, estimated population count (‘000); n.p., not available for publication, but included in totals where applicable. †Persons who met criteria for diagnosis of a lifetime mental disorder (with hierarchy) and had symptoms in the 12 months prior to interview. ‡Includes ‘mental health nurse’ and ‘other professional providing specialist mental health services’. §Includes ‘specialist doctor or surgeon’, ‘other professional providing general services’ and ‘complementary/alternative therapist’. ¶Includes ‘not stated’.
Use of community-based services by people with mental disorders of varying severity
12 month rates of community-based service use for mental health problems for people with mental disorders,† vs severity of symptoms
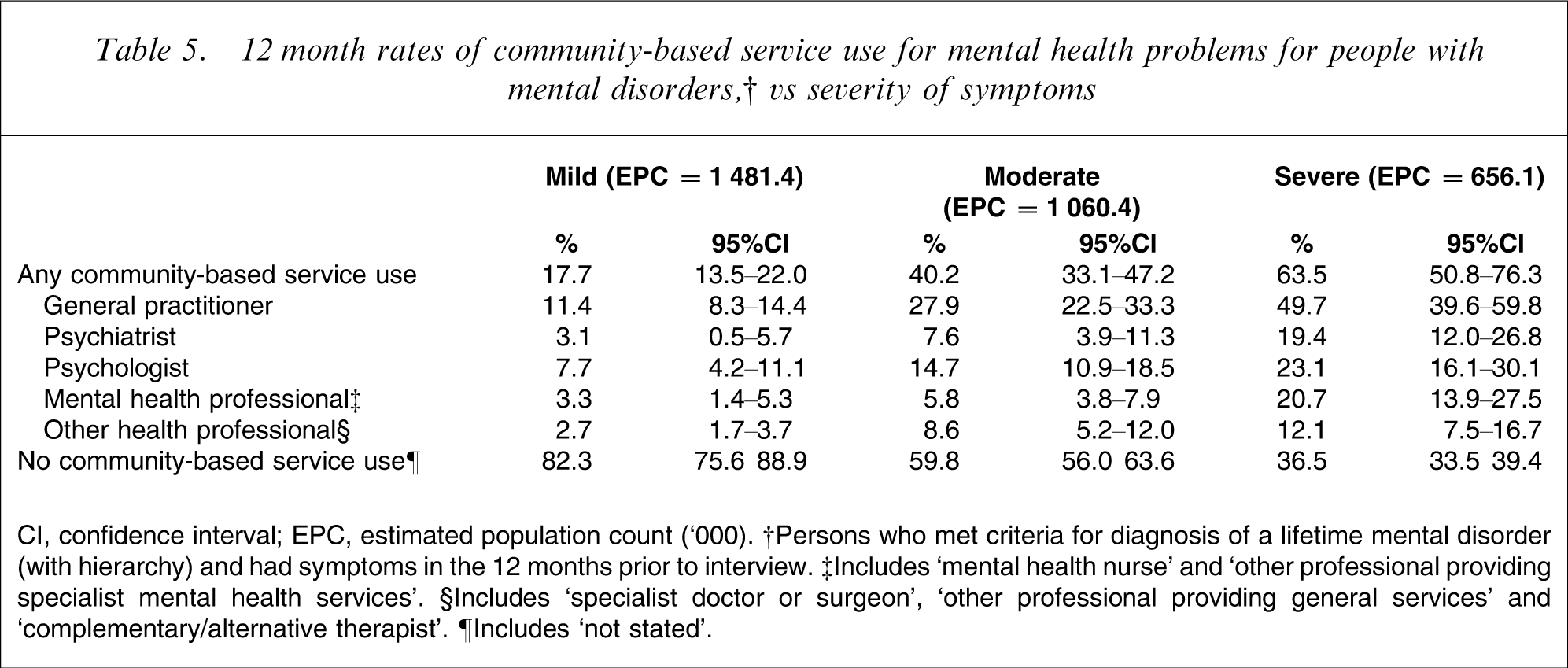
CI, confidence interval; EPC, estimated population count (‘000). †Persons who met criteria for diagnosis of a lifetime mental disorder (with hierarchy) and had symptoms in the 12 months prior to interview. ‡Includes ‘mental health nurse’ and ‘other professional providing specialist mental health services’. §Includes ‘specialist doctor or surgeon’, ‘other professional providing general services’ and ‘complementary/alternative therapist’. ¶Includes ‘not stated’.
Discussion
Summary of findings
The current analysis shows that 11.9% of the general Australian adult population make use of any services for mental health problems in a 12 month period. Only approximately one-third of people (34.9%) meeting criteria for a mental disorder do so. Overall, female subjects with mental disorders were more likely to use services than male subjects with mental disorders (40.7%, 95%CI = 36.0–45.3% vs 27.5%, 21.0–34.0%). People in the youngest age group made relatively lower use of services than older adults, with 23.3% (95%CI = 17.6–29.0%) of 16–24-year-olds doing so compared with 39.9% (95%CI = 32.6–47.3%) of 35–44-year-olds, 41.2% (95%CI = 29.2–53.2%) of 45–54-year-olds, and 39.3% (95%CI = 29.7–48.9%) of 55–64-year-olds. Those with affective disorders are most likely to make use of services (58.6%), followed by those with anxiety disorders (37.8%) and those with substance use disorders (24.0%). A small proportion (6.1%) of people with no mental disorder also makes use of services for mental health problems. Mental health hospitalizations are far less common than consultations with community-based providers: Only 2.6% of those with mental disorders have hospitalizations, whereas 34.6% visit a community-based provider – particularly general practitioners (24.7%) and psychologists (13.2%). Approximately one-tenth (9.8%) of those with mental disorders visit a general practitioner in isolation, and do not receive care from any other mental health professional. There is a clear dose–response effect between severity of disorders and rates of community-based service use: 63.5% of those with severe mental disorders use community-based services, compared with 40.2% of those with moderate mental disorders and 17.7% of those with mild disorders. There is also a relationship between comorbidity of mental disorders and service use, although this relationship is not simple and varies as a function of both the number and the nature of disorders.
Comparisons with recent international surveys
As noted, the survey instrument used in the 2007 NSMHWB was based on the most current version of the WMH-CIDI, which has recently been used in similar exercises in a number of other countries. This facilitates comparisons between Australia and elsewhere regarding rates of service use for mental health problems, although such comparisons should be interpreted with caution because the mental health service systems in different countries vary.
Wang et al. consolidated survey data on 84 850 adults aged ≥18 from 17 countries, and found that rates of service use among respondents from a subset of 10 high-income countries varied from 4.3% in Italy to 17.9% in the USA [8]. They also found that, across all of these high income countries, the most commonly accessed services were those provided in the ‘general medical sector’. The current findings are broadly consistent with this international picture. At 11.9%, Australia's rates sit approximately in the middle, somewhat lower than its closest peer, New Zealand (13.8%). Like their international counterparts, Australians rely most on general practitioners for their mental health care.
Wang et al. did not look at rates of service use for people with mental disorders [8], but other within-country studies have done this. Again, the Australian picture is comparable with that from overseas. Other studies of high-income countries have also generally found that around one-third of those with a mental disorder use mental health services in a 12 month period. For example, Oakley-Browne et al. and Wang et al. found rates of 38.9% and 41.1% in New Zealand and the USA, respectively [9, 10]. These studies also found that rates of service use were highest among those with affective disorders (56.4% in the USA; 55.1% in New Zealand), followed by those with anxiety disorders (42.2% in the USA; 39.4% in New Zealand) and those with substance use disorders (38.1% in the USA; 29.9% in New Zealand) [9, 10]. Supplementary work by Druss et al. in the USA also identified a small proportion of people (8.0%) with no disorder who received services [11].
Using the consolidated international dataset, Wang et al. examined the relationship between severity of mental disorders and service use [8]. As was the case in the current analysis, they consistently found a dose–response effect whereby those with severe disorders were significantly more likely to use services than those with moderate disorders who, in turn, were significantly more likely to use services than those with mild disorders. High proportions of those with severe disorders, however, did not receive services (e.g. 41.3% in New Zealand).
Comparison with the 1997 Australian National Survey of Mental Health and Wellbeing
An earlier NSMHWB was conducted in Australia in 1997, which also made an assessment of service use for mental health problems. Caution must be exercised in comparing the findings from the 2007 NSMHWB with those from the 1997 NSMHWB, given the differences in the two survey instruments [7]. In particular, the criteria for having a mental disorder were stricter in the 1997 survey (e.g. in 1997, to be classified as having a 12 month disorder, all criteria for the disorder had to be met; in 2007, those meeting criteria for a lifetime disorder and having symptoms or an episode during the past 12 months qualified as having a 12 month disorder). With this caveat in mind, it is possible to consider the relative rates of service use for mental health problems in 1997 and 2007, and to consider how policy and practice initiatives implemented in the intervening years may have influenced any changes in service use.
The current overall rate of service use by people with any mental disorder is comparable with that found in 1997 (32.5%) by Andrews et al. [12]. Similarly, the rates of any service use by people with affective disorders (60.4%), anxiety disorders (45.2%) and substance use disorders (27.9%) do not seem to have changed much over time, based on findings published by Parslow and Jorm [13]. What does appear to be the case, however, is that patterns of service use may have changed. In particular, there was a notable increase in the use of psychologists. In 1997, 11.8% of those with an affective disorder saw a psychologist, 8.7% of those with an anxiety disorder did so, and 5.4% of those with a substance use disorder did so [13]. In 2007, the equivalent figures were 23.2%, 14.0% and 9.1%.
Study limitations
The 2007 NSMHWB was a major undertaking, and represents the best available current data on overall patterns of service use for mental health problems in Australia. But certain limitations of the survey should be acknowledged. First, the response rate of 60% was lower than expected and may have introduced some selection biases. Second, the survey relied on self-report with no external validation, and respondents may have underreported or overreported their use of services (in previous studies, the findings have gone in both directions [14, 15]). Third, at the time of analysis, the available data came in the form of extract tables from the ABS, rather than in the form of a de-identified (i.e. confidentialized)
Interpreting the findings within a policy context
From a policy perspective, the current findings can be interpreted in two different ways. On the one hand, they might be viewed negatively. They suggest that, despite significant investment in mental health over the last decade and a half, overall rates of service use for people with mental health problems remain similar to those of 10 years ago, with two-thirds of people with mental health problems not receiving treatment in a given 12 month period. This figure clearly needs unpacking. First, the broader diagnostic criteria in the current survey may have had the effect of shifting the denominator, and if the stricter diagnostic threshold was used rates of service use might have increased. Second, it is clear from these analyses that the likelihood of using services increases with severity, although it is also the case that almost one-third of people with severe conditions do not receive treatment. Finally, some people who have needs for services may not use them because they do not choose to seek care, and others may not use them because they cannot access them for reasons related to the nature, location or cost of the service. Additional analysis of the 2007 NSMHWB data will shed further light on whether the reasons underpinning the current level of service use are consumer-related, service-related or a combination of the two. Consumer-related issues may require further policy efforts in terms of improving mental health literacy and encouraging help-seeking behaviour. Service-related issues may require a redoubling of mental health service reform efforts.
On the other hand, there are some positive messages in the findings. Australia's rates of service use for mental health problems are similar to those in other high income countries, suggesting that we are not alone in our ongoing efforts to improve treatment coverage. More importantly, there are indications that some of the recent policy initiatives designed to improve access to mental health-care providers through the primary mental health care sector have been successful. For example, both the Better Outcomes and Better Access programmes aim to improve access to psychologists, and rates of consultations with these providers have increased substantially.
Conclusions
At present, rates of service use for mental health problems among those with mental disorders in Australia are less than optimal. Little international guidance is available about what an appropriate level of treatment coverage might be and other comparable countries seem to face similar difficulties in improving their levels of service use. It is not realistic, nor desirable, to aim for total coverage because not all those with mental disorders (particularly those with mild disorders) will have a need for services. Few would dispute, however, that the current situation should be improved. Further work is required to determine what an appropriate rate of service use is, and to set targets to reach that rate. Australia has demonstrated that concerted government investment and policy direction can improve rates of service use in particular areas (e.g. increasing access to psychologists), and these efforts should be expanded.
Footnotes
Acknowledgements
The 2007 NSMHWB was funded by the Australian Government Department of Health and Ageing, and conducted by the Australian Bureau of Statistics. The authors would like to thank the 2007 NSMHWB Reference Group for their input into the survey's design. The authors would also like to thank those who participated in the survey.