
Abstract
Although gambling has traditionally been considered an adult activity, there is now evidence to suggest that a significant proportion of adolescents are also involved, and from an increasingly younger age. Across a number of studies conducted in Canada [1–3], the US [4, 5], the UK [6, 7] Australia [8, 9] and New Zealand [10], it has been found that between 60% and 80% of young people aged 13–17 years gamble at least once per year, and that between 3% and 5% display many of the behaviours indicative of adult problem gambling [3]. Such behaviours include an excessive preoccupation with gambling, chasing losses, lying to friends and family about the extent of gambling, as well as ongoing neglect of important commitments (e.g. school or friendships) to provide opportunities for gambling. While adolescent problem gambling is thought to differ from adult problem gambling in that it is generally less likely to give rise to significant personal and financial harm to others because adolescents are generally unmarried and are less likely to own significant assets [9], there is clear evidence to suggest that an early involvement with gambling is a precursor to more significant problems later in life [6, 11]. Recent studies in both New Zealand [12] and Australia [13] has shown that adult problem gamblers report having gambled at significantly younger age than those without problems, and indicate that their gambling problems were well established before they turned 18 and could gamble legally. For this reason, adolescent gambling has been identified as an important public health issue which may have implications for preventing and reducing the incidence of problem gambling in the adult population [14].
Another important finding from this emerging body of research is that problem gambling also appears to be a corollary of significant difficulties in social and psychological adjustment during adolescence. Adolescent problem gamblers, for example, have been found to be more depressed and apprehensive and to have poorer coping skills than non-problem gamblers [15]. One common explanation for this association is that gambling may, at least for a substantial percentage of young people, serve as a form of emotion-based copying that allows young people to escape from unhappy home lives, difficulties at school, or painful memories of previous trauma or abuse [6, 11]. Gambling is thought to fulfil this function because gambling venues provide a milieu that isolates people from the outside world, and which provides excitement and social interactions not available elsewhere.
Furthermore, because gambling often involves peers with similar motivations and interests, there is also evidence to suggest that gambling is a correlate of involvement in other high-risk or self-harming behaviours [15–20]. Barnes, Welte, Hoffman and Dintcheff, in the US, showed that 62% of young people who drank heavily gambled on a weekly basis compared with only 43% of moderate drinkers [19]. Similar findings were obtained by Gupta and Derevensky in Canada, who found that adolescents classified as problem or pathological gamblers were three to four times more likely to drink alcohol on a weekly basis, take drugs or smoke compared with those who gambled very little, or not at all [3]. Similarly, an American study by Volberg and Moore showed that over 50% of at-risk or adolescent problem gamblers in Washington State smoked or used alcohol compared with only a quarter of non-problem gamblers [5].
Other studies have shown that adolescent problem gambling also frequently coincides with other negative life outcomes [6, 7]. Studies in Canada [18] and the US [20–22], for example, have found that problem gamblers are significantly more likely to have been suspended or excluded from school than non-problem gamblers or display the symptoms of general conduct disorder, whereas studies in the UK [7] have found that almost a quarter of problem gamblers have truanted to gamble, or turned to turned to petty crime or other delinquency behaviours to support their gambling [18].
The present study
Despite the existence of international research demonstrating a relationship between adolescent problem gambling and various forms of psychosocial maladjustment, only one Australian study has so far sought to investigate whether a similar link exists in Australia [23]. In Jackson's study, 2700 first-year high school students (Year 8) in the State of Victoria were surveyed about their gambling habits and administered a variety of questions relating to their social, educational and psychological adjustment. The study found that those who were more involved in gambling (as measured by the number of activities preferred) were more likely to engage in risky behaviours (alcohol, smoking, drug use), to be less satisfied with school, and more likely to engage in selfharming behaviours. However, the age of the students, the low rate of gambling, as well as the absence of a validated problem gambling screen precluded any opportunity to determine the relationship between problem gambling and adolescent functioning.
Aims and hypotheses
Accordingly, the aim of the present study was to extend existing Australian adolescent gambling research by formally assessing the prevalence of problem gambling using a validated diagnostic measure and administering well-established measures of psychosocial adjustment. The principal hypothesis was that adolescent problem gamblers would score significantly more poorly on measures of psychological adjustment or general mental health, be more disillusioned and alienated, and also be more likely to be engaged in other high-risk activities than peers without gambling problems. The underlying practical and policy imperative governing this research was to provide educators and clinicians with insights into the psychological and social profile of adolescents experiencing difficulties with gambling. It was hoped that this would enhance knowledge of how to detect the early stages of this often hidden disorder, as well as encourage awareness of its short-term and longerterm developmental consequences for young adults.
Method
Respondents
The sample comprised 926 (473 boys, 448 girls, five gender missing) students in grades 7–12 drawn from 18 schools in the Australian Capital Territory (ACT) in 2003–04. The ACT is one of the principal territories of Australia surrounding Australia's capital city, Canberra (population: approximately 330 000). Eleven of these schools were government high schools, and the remaining seven were Catholic or independent. This ratio was similar to that for the ACT area as a whole (approximately 60% government and 40% Catholic/independent). Survey respondents comprised 346 students (37.4%) in years 7–8, 406 (43.9%) in years 9–10 and 174 (18.8%) in Years 11 and 12. The mean age of the sample was 14.46 years (SD = 1.64) with an age range of 11–19 years (only 39 or 4.2% were 18 years or older). Thirty-two (3.5%) identified themselves as Aboriginal or Torres Strait Islanders and 24.3% indicated that a language other than English was spoken at home. Most students lived with their parents (73.2%), 8.9% lived independently and the rest lived in other arrangements.
Cross-tabulation analyses revealed no significant association between school type (Catholic/independent
Measures
Gambling habits
Respondents were asked how often during the previous 12 months they had gambled on all the major forms of gambling available in the ACT, including: cards (private
DSM-IV-J
The 12-item adolescent version of the DSM-IV, the DSM-IV-J [24, 25] was used. The scale includes such behaviours as: being preoccupied with gambling, being restless and irritable if unable to gamble, ‘chasing’ behaviour, spending lunch money, stealing money, and social conflict. Each of the items was scored Yes/No, with scores being based upon the total number of ‘Yes’ responses. As with the adult scale, scores of 4 or more on the DSM-IV-J are indicative of problem gambling. In the present sample, the internal reliability was found to be very high, α = 0.91. It is important to note that there have been concerns raised in the literature regarding the scoring of the DSM-IV-J, particularly due to researchers' use of two possible scoring methods [26]. In Fisher's original formulation [24], scoring was based on nine items, but most studies have used all 12 items. Derevensky
Victorian Gambling Screen (VGS)
Respondents were also administered the VGS recently developed and validated in Australia by Ben-Tovim, Esterman, Tolchard, Battersby & Flinders Technologies [27]. The VGS Harm to Self Scale comprises 15 statements. Respondents were scored according to their responses on a five-point scale where ‘never’ = 0, ‘rarely’ = 1, ‘sometimes’ = 2, ‘often’ = 3 and ‘always’ = 4. The scoring range for this scale is from 0 to 60. Validation of this scale against gold-standard clinical interviews with problem gamblers and ROC analysis indicates that a cut-off score of 21 or higher identifies a person as a problem gambler [27]. Concurrent validity indicates that this scale correlates very highly with the South Oaks Gambling Screen (SOGS) (
Negative mood scale
Negative mood was measured using a six-item negative mood checklist previously used in a 10-year longitudinal adolescent school-leaver study by Tiggemann and Winefield [28]. For each of the five words (bored, lonely, angry with self, happy (reversed scored), helpless and depressed), participants indicated how often they felt that way, 1 = almost never, 2 = sometimes, 3 = quite often and 4 = almost always. The minimum score of 6 indicated almost no negative symptoms, whereas the maximum score of 24 indicated a very negative mood state. The alpha reliability of this scale was acceptable, α = 0.80.
Rosenberg self-esteem scale
Self-esteem was measured using Rosenberg's self-esteem scale [29]. This scale comprises 10 items and respondents indicate their level of agreement (1 = strongly agree, 2 = agree, 3 = disagree, 4 = strongly disagree). The scoring range was from 10 (low self-esteem) to 40 (high self-esteem). This measure has also been extensively used in South Australian adolescent research by Tiggemann and Winefield [28]. This scale had very good internal reliability in the present sample, α = 0.87.
General health questionnaire (GHQ-12)
General psychological and medical health was measured using Goldberg and Williams (GHQ-12) [30]. Participants indicated the frequency of various symptoms over the ‘last few weeks’ (e.g. losing sleep due to worry, feeling constantly under strain) on four-point scales that vary slightly depending upon wording of the question and the direction of scoring. An example includes: 1 = more so than usual, 2 = same as usual, 3 = less so than usual, 4 = much less than usual). Scoring involved assigning one point for every response of 3 or 4, so that the maximum score of the scale was 12 with a minimum of 0. The alpha reliability of this scale was very good, α = 0.84.
Social alienation (Dodder and Astle [31])
The social alienation scale comprised nine statements and respondents were required to indicate whether they agreed or disagreed with each statement. This scale was designed to measure a person's perception of disengagement, or disillusionment, with society. Previous research by Winefield
Popularity and peer relations
As a measure of peer relations, adolescents were asked to indicate what percentage of their class liked them, and what percentage they did not like.
Financial Scale
The Financial Scale was used to measure perception of financial security. This measure was first used in Tiggemann and Winefield [28]. Participants were required to rate their agreement with 12 statements according to a four-point scale (1 = strongly agree, 4 = strongly disagree). Reliability analysis of this measure was good, α = 0.79.
Leisure activities
Respondents were asked to indicate how they spend their spare time both in terms of four broad categories and also specific activities. The broader questions were based on Tiggemann
Alcohol consumption
Young people were asked to indicate how often they usually drink alcohol, where 0 = never, 1 = less than once per week, 2 = 1–2 days per week, 3 = 3–4 days per week, 4 = 5–6 days per week and 6 = every day. They were also provided with a description of a standard drink and asked to indicate how many standard drinks they usually consumed on each occasion.
Cigarette smoking
Young people were asked to indicate whether they smoked cigarettes and how many they would typically smoke per day.
Drug use
Respondents were asked whether they used any drugs and, if so, what sort. Options included: marijuana, heroin, speed, ecstasy, cocaine or other.
Results
Identifying problem gamblers
Both the DSM-IV-J and VGS (scored 21 +) are considered conservative measures of problem gambling. As Gupta and Derevesky [2] showed, one usually obtains lower prevalence estimates in adolescent samples using DSM-IV-J than other measures. Similarly, as McMillen [33], found, the VGS tends to yield lower prevalence estimates in adult populations than other established measures such as the Canadian Problem Gambling Index (CPGI) and SOGS when one uses the 21 + cut-off score. In the present study, it was found that 41 (4.4%) of the sample scored in the problem range for the DSM-IV-J (scores 4 +), and that only 31 (3.3%) scored above 21 on the VGS. Pearson correlation analysis applied to the full scale scores showed a high correlation between the two measures,
More detailed cross-tabulation analysis showed that only nine participants scored in the problematic range for the VGS, but not on DSM-IV, whereas there were 19 cases who scored positively on the DSM-IV, but not on the VGS. In other words, as McMillen
As indicated above, the debate as to whether scores on these measures provide genuine indicators of problem gambling, or ways of identifying young people with the early warning signs of problem gambling remains unresolved. Some leading international experts in the adolescent gambling field support the validity of these measures [26], but this view is not shared by others [34] who suggest that the measures overestimate the actual proportion of problem gamblers. The current study has adopted the methodologies utilized in previous studies in order to provide relevant comparative data for Australia, but was not specifically designed to address the contentious issue of false positives in prevalence estimates. Instead, the primary focus of this research was to utilize these measures as standardized tools to identify groups of adolescents who have been affected by gambling to different degrees. As indicated in Table 1, scores on both measures differed significantly between the two groups with non-problem gamblers averaging close to zero on both.
Prevalence of substance use among problem and non-problem gamblers
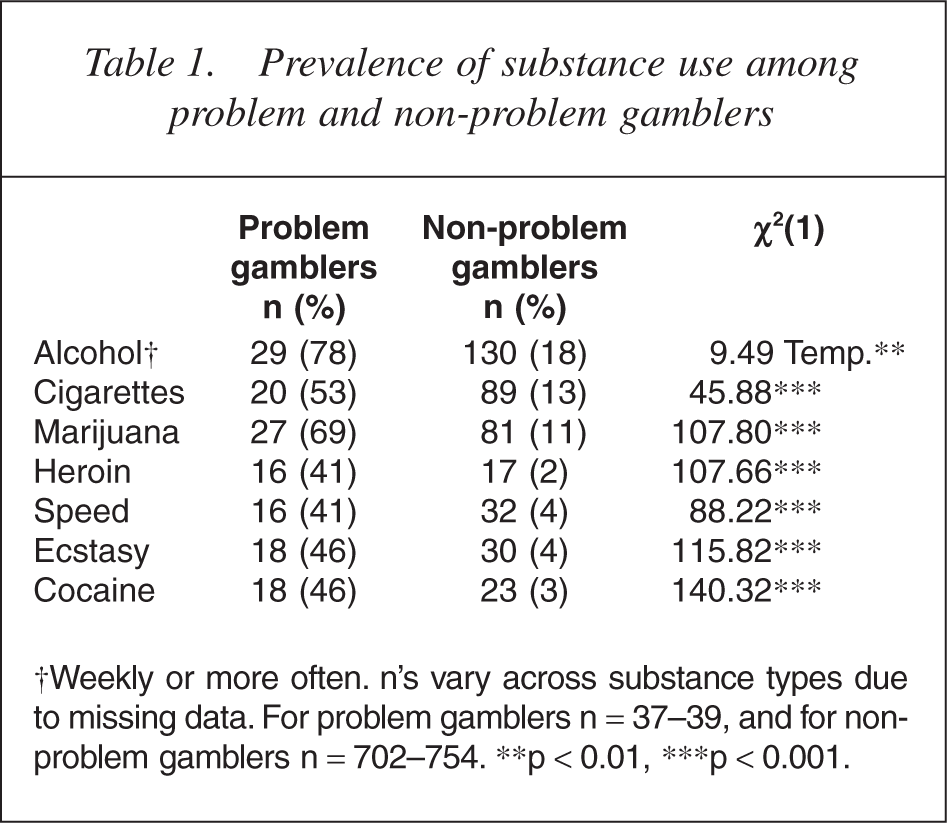
†Weekly or more often. n's vary across substance types due to missing data. For problem gamblers n = 37–39, and for non-problem gamblers n = 702–754. ∗∗p <0.01, ∗∗∗p <0.001.
For the purposes of our analyses and to obtain a sample suffi-ciently large to allow comparisons between a problematic and nonproblematic sample, we focused upon the results for the 41 participants who scored positively on the DSM-IV and also included the nine who scored positively on the VGS (total n for the problem gambling group = 50). A series of analyses conducted with and without the additional nine participants classified on the VGS revealed an identical pattern of results for all variables considered below. Accordingly, the results presented below were based on the combined sample of 50 participants.
Problem gambling and gambling involvement
Analysis of gambling frequency data showed that the two groups differed substantially in terms of their gambling involvement. The problem group gambled on significantly more activities (M = 4.7, SD = 2.31
Prevalence of weekly gambling participation of each form of gambling
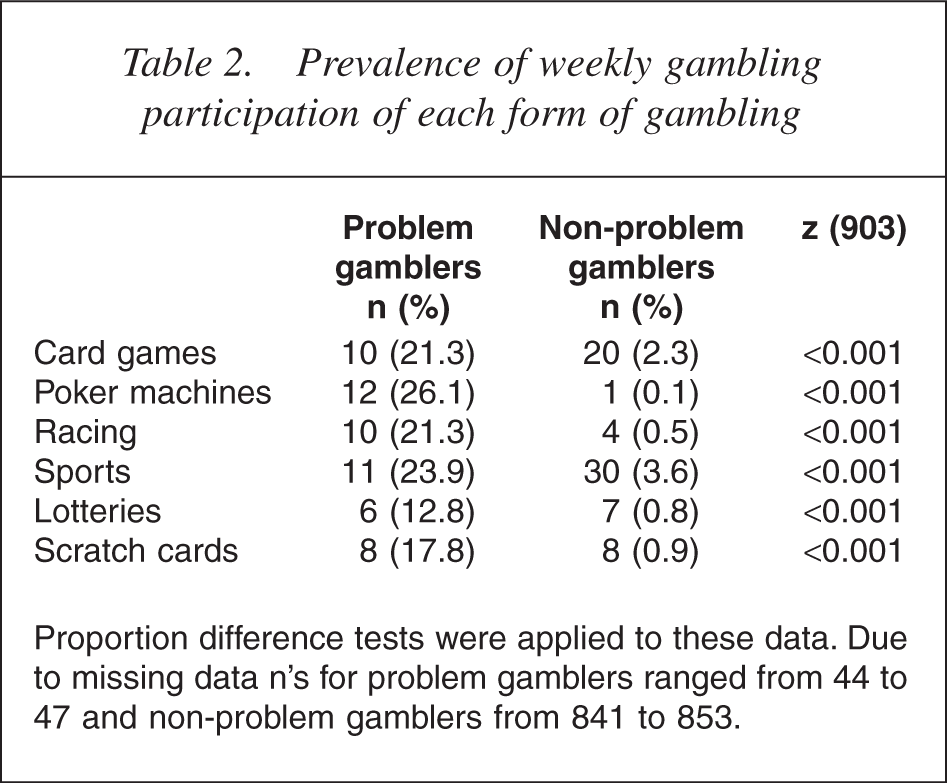
Proportion difference tests were applied to these data. Due to missing data n's for problem gamblers ranged from 44 to 47 and non-problem gamblers from 841 to 853.
Problem gambling and other high-risk behaviours
Respondents were asked to indicate how often they drank alcohol on a six-point scale ranging from 0 = never to 6 = daily, and were divided into principal groups: those who drank less than once per week, and those who drank at least weekly. For other substances, the question asked whether they were currently using any other drugs. As indicated in Table 1, over three quarters of problem gamblers drank alcohol on a weekly basis compared with only half of the non-problem sample. The prevalence of smoking among problem gamblers was four times the rate, for marijuana over six times the rate, and for harder drugs, at least 10 times the rate recorded for the non-problem sample. Analysis of the quantity of alcohol and cigarettes consumed on each occasion revealed a mean daily consumption of 4.58 (SD = 4.74) standard drinks per day for the non-problem group and 5.89 (SD = 4.18) for the problem group. The problem group smoked an average of 17.38 (SD = 17.49) cigarettes per day versus 10.37 (SD = 11.14) for the nonproblem group. Neither of these differences was statistically signifi-cant. In other words, the principal difference between the two groups in terms of alcohol and cigarette consumption was the frequency of participation.
The psychological wellbeing of problem gamblers
Problem gamblers and non-problem gamblers were compared in terms of their scores on five measures of psychological wellbeing. As indicated by Table 3, problem gamblers experienced significantly poorer mood states, had lower self-esteem, poorer general health, felt more alienated from society and were more likely to feel that they did not have sufficient money to satisfy their needs. The effect sizes for all of these analyses were moderate, with the strongest effect being observed for social alienation.
M (SD) scores on measures of problem gambling and psychological functioning among problem (n = 50) and non-problem gamblers
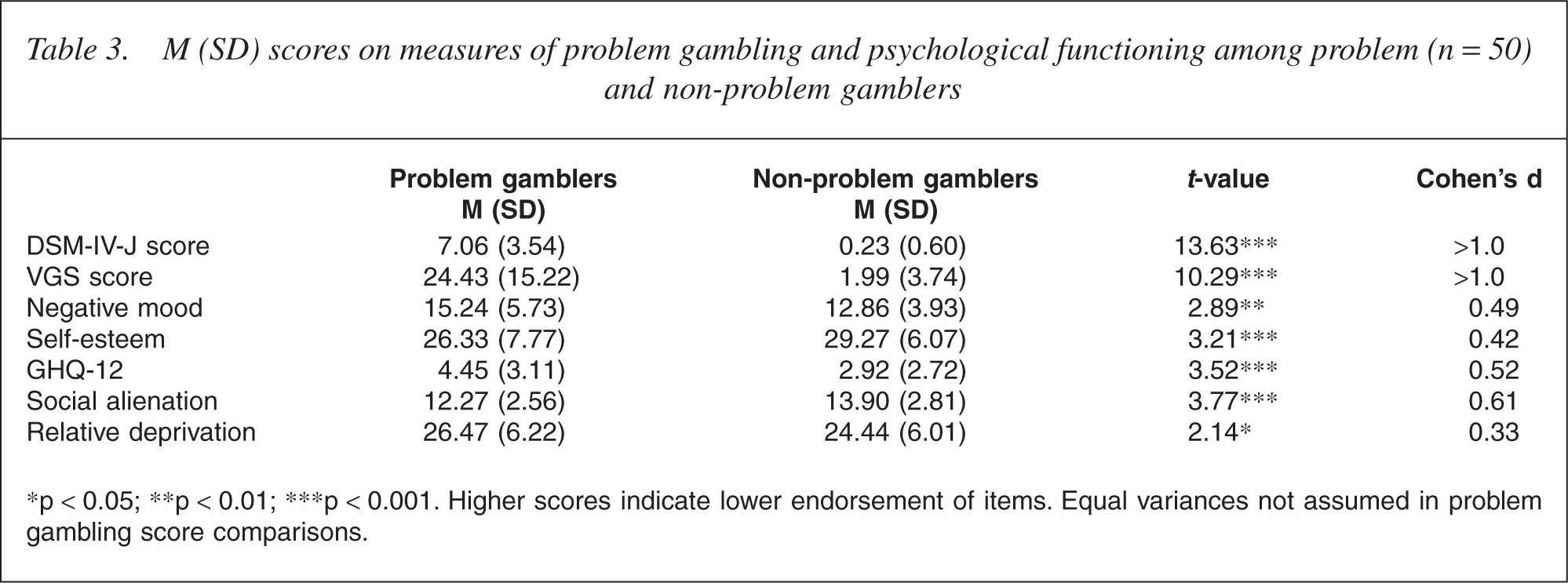
∗p <0.05; ∗∗p <0.01; ∗∗∗p < 0.001. Higher scores indicate lower endorsement of items. Equal variances not assumed in problem gambling score comparisons.
In order to identify the strongest psychological predictor of problem gambling, all of these variables were entered into a logistic regression analysis with problem gambler status as the dependent measure (Table 4). The model correctly classified 95% of cases and showed that social alienation was the strongest predictor of problem gambling status (Wald = 6.37, p < 0.01, odds ratio = 0.84). In other words, each unit decrease in endorsement (higher score) was associated with a 1/ 0.84 = 20% reduced likelihood of being in the problem gambling group.
Logistic regression: psychosocial predictors of problem gambler status
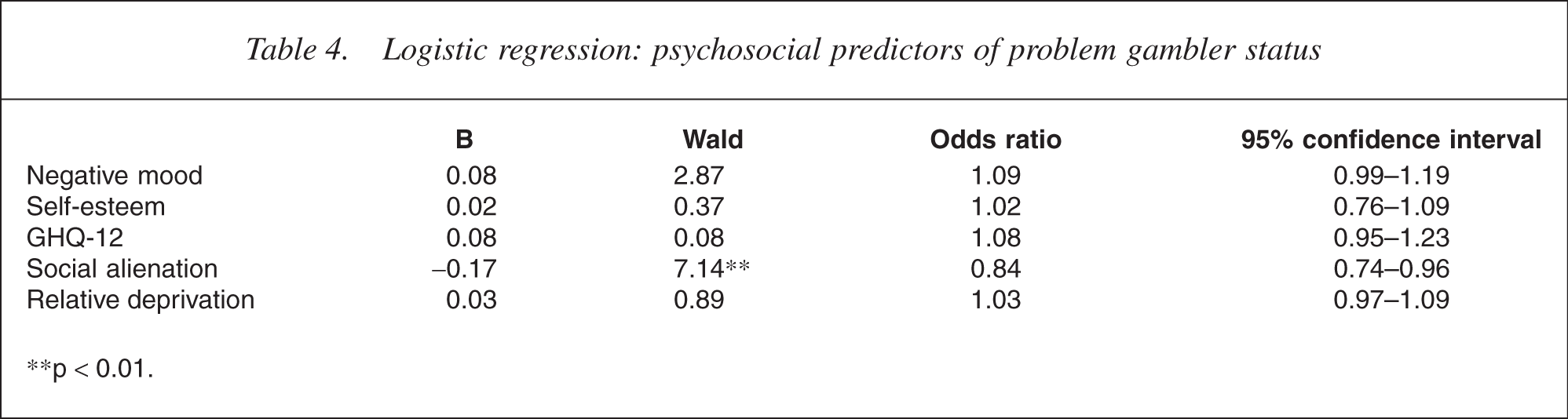
∗∗p <0.01.
Peer relationships
Respondents were also asked to indicate how many close friends they had, how many peers in their class they disliked and how many disliked them. The results showed that problem gamblers reported having as many close friends as other young people in the sample, but appeared to have a poorer relationship with other peers in their class. In response to the question about others in their class, problem gamblers indicated that they disliked twice as many classmates as other respondents (M = 12.24, SD = 10.39
A further series of questions asked respondents to indicate how they usually spent their leisure time (doing nothing, activities alone, activities with others, going out) on a five-point scale. No significant differences were observed for all items except that problem gamblers indicated undertaking more activities with others than did the rest of the sample (M = 3.16, SD = 0.95
Problem gambling and substance use: controlling for gender
A potential problem with the above analyses is that gender is significantly associated with problem gambling, and scores on some of these measures of adjustment also differ significantly between boys and girls and in the same direction as the gambling-related effects. For example, boys are more likely to smoke marijuana, and to use all of the hard drugs. In order to determine the relative importance of gambling status, a series of hierarchical logistic regression analyses were undertaken. Involvement in the high-risk activity was the dependent measure (0 = not involved, 1 = involved), gender was entered on the first step and gambling status on the second step. In the interest of parsimony, this analysis was confined to a generic question that asked whether participants used any other substance apart from alcohol, nicotine/ cigarettes and marijuana. The analysis convincingly showed that problem gambling was the critical variable. In the final model which correctly classified 87% of cases, gender was a non-significant predictor, whereas problem gambler status was highly significant with an odds ratio of 0.062. In other words, if a person responded ‘yes’ to the ‘any other substance’ question, he or she was 1/0.062 = 16 times more likely to be a problem gambler.
Discussion
The results of this study were generally consistent with previous international research that has revealed an association between adolescent problem gambling and poorer psychological and social functioning. Adolescent problem gamblers in this sample were found to be significantly more disillusioned with society, had lower self-esteem and were significantly more likely to engage in a range of other high-risk behaviours than other adolescents. For example, problem gamblers were 10–20 times more likely to have used hard drugs compared with the rest of the sample, and 75% revealed that they drank alcohol without adult supervision on at least a weekly basis. When asked how they felt about their peers, the results showed that problem gamblers were generally socially isolated from their general peer group, with many feeling that they were not well liked by many of their classmates. However, at the same time, the results also showed that young problem gamblers were not necessarily deprived of social contacts. On the contrary, most reported being actively involved in leisure activities with other people, and reported having a well-developed group of close friends. Thus, contrary to the view that problem gambling is a solitary and antisocial activity [35], the results here suggest that Australian adolescent problem gamblers are likely to form distinct and potentially identifiable subgroups within the school population. Based on the results above, this group is more likely to be male than female, is generally dissatisfied and disillusioned with many aspects of life, and in many cases, gambling is incorporated into a range of other high-risk or delinquent behaviours undertaken with other young people with similar attitudes and circumstances.
The very strong role of social or peer influences in the development of adolescent problem gambling has been previously observed in a number of studies [8, 9, 35]. Young people who have friends who gamble and/or who hold positive attitudes towards gambling are significantly more likely to engage in gambling themselves. A positive interpretation of these findings is that gambling and other high-risk behaviours are merely vehicles for social interactions, and a part of the experimentation and exploration that is often characteristic of adolescent development. However, as Hardoon
Whether problem gambling is the cause of psychological and social problems, or a symptom of these difficulties remains unclear because of the limited longitudinal evidence currently available concerning the development of adolescent gambling problems. However, there is evidence to suggest that the relationship probably goes both ways. Griffiths [36] found that adolescent problem gamblers tend to experience depression following unsuccessful gambling sessions, suggesting that the activity can have a direct and negative affect on mood states. On the other hand, other research in support of the opposite view, has shown that gambling can fulfil important physiological or psychological needs, in that there may be young people who are particularly prone to developing gambling problems [37, 38]. One view arising from Jacob's general theory of addictions [11] is that gambling helps young people deal with anxiety and depression caused by unhappy life experiences, early abuse or trauma. According to this view, gambling is not seen as an intractable pathology maintained by fundamental flaws in the person's character or biological makeup. Instead, people are seen as becoming dependent or ‘addicted’ to gambling because it is positively reinforcing and can serve to regulate their mood states. An alternative view is that this pattern of behaviour may also arise from individual differences in risk-taking propensity. For example, Burnett
Both Zuckerman and Jacob's theories therefore share some similarities in that arousal and mood regulation play important roles in the development and maintenance of the behaviour. However, the difference is that, whereas in Zuckerman's model risk taking is considered to be positively reinforcing, and that the desire for stimulation arises from genuine individual differences in physiology, Jacob's theory is based on the idea that the need is not inborn, but arises from traumatic or unhappy experiences. Gambling is negatively reinforcing as a result of its capacity to alleviate negative mood states and extinguish distressing memories rather than being gratifying for its own sake.
However, irrespective of which theoretical position is most correct, the findings here and both theoretical perspectives, all support the view many young people are particularly vulnerable to the early development of gambling problems. Therefore, taken together, the results support the view that adolescent problem gambling is an important public health issue because it has clear implications, not only for understanding the aetiology of adult gambling, but also for protecting the mental health of a significant proportion of young people. For example, the fact that gambling coincides with other high-risk behaviours immediately suggests that existing educational programs designed to raise awareness of drug use among adolescents could also be extended to include gambling. Furthermore, given the strong association between problem gambling and psychosocial maladjustment, it is suggested that general psychological or psychiatric screenings, and particularly those involving vulnerable adolescent populations (e.g. correctional populations), should be extended to include measures of adolescent gambling. As some recent New Zealand research by Abbott
Conclusions
As with any findings based on cross-sectional selfreport data, there is always a need to exert some caution when interpreting these results. One cannot, for example, be certain that young people answered all of the questions relating to problem gambling honestly. Nor is it possible to determine whether the difficulties observed in psychological and social functioning were the cause or the outcome of excessive gambling. Nevertheless, the similarity of these findings with others obtained around the world in different jurisdictions and using a variety of different measures and methodologies (e.g. classroom
At the same time, we believe that two principal conceptual limitations remain and need further attention in future studies. The first concerns the long-term implications of adolescent gambling findings, and the second relates to the definition of problem gambling. Although it is well established that many adult problem gamblers commenced gambling during adolescence, there is very little prospective evidence available to indicate what proportion of adolescents with gambling problems become problem gamblers during adulthood. At the same time, doubts also remain concerning the use of term problem or pathological gambler for adolescent gambling. Although adolescents may share many of the same behavioural traits as adult problem gamblers (e.g. spending more than they can afford, chasing losses, being preoccupied with gambling), there is little evidence to suggest that they are experiencing the significant harms (loss of jobs, relationships or assets), or gambling with the same intensity (see Table 2). For this reason, doubts will remain as to whether adolescent and adult problem gambling measures are capturing the same construct (a combination of problematic behaviours and harms). However, to the extent that these measures appear very successful in being able to differentiate groups of adolescents with clearly different gambling and psychosocial profiles, they remain useful in identifying problematic behavioural patterns and psychosocial factors likely to have longer term development consequences for young people.
Footnotes
Acknowledgements
This project was supported by Australian Research Council Linkage Grant LP0348759. The authors are grateful to the support provided by the Australian Capital Territory Gambling and Racing Commission, ACT (Australian Capital Territory) Department of Education and Training, Catholic Education Office and Association of Independent Schools.