
Abstract
This perspective piece is a detailed analysis of the critique by Gordon Parker of the mood disorders clinical practice guidelines (MDcpg2020), in which he claims that bipolar II disorder has been ‘banished’ despite its formal status in current taxonomies. In this article, I defend the reasoning used by the Committee to adopt a dimensional model for describing and managing mood disorders, in particular bipolar disorder. I also robustly contend the many erroneous inferences made by him in his Viewpoint regarding management recommendations within the MDcpg2020 and demonstrate that there is no valid justification for subtyping bipolar disorder – especially in the manner proposed by the Diagnostic and Statistical Manual of Mental Disorders, 5th edition. Thus, I argue that it was appropriate for the MDcpg2020 Committee to pursue an alternative model to the usual subtyping of bipolar disorder into ‘thing one’ and ‘thing two’ and conclude that the now clearly redundant model of Bipolar II should be altogether removed from our lexicon and clinical practice. Indeed, it is time to develop new and alternative models for defining bipolar disorder and among these a dimensional model should be given consideration.
‘There’s just one kind of folks. Folks’.
Introductory remarks
The ‘dismissal’
Professor Gordon Parker concludes his critique of the recently published clinical practice guidelines for mood disorders (MDcpg2020) (Malhi et al., 2021) with an amusing quip – ‘The dismissal now has a second Australian connotation’ (Parker, 2021). The implication is that the Mood Disorders Committee (Committee) that wrote the MDcpg2020 has dismissed bipolar II disorder from its considerations in a manner akin to the occasion when Governor-General Sir John Kerr ousted Prime Minister, Gough Whitlam in 1975. In this momentous event, known officially as the Australian constitutional crisis and colloquially as the Dismissal, Kerr summarily dismissed Whitlam, who was at the time the leader of the Labor party, and transferred power to the Leader of the Opposition, Malcolm Fraser. It was, in the words of Humphrey from Yes Minister, a truly ‘courageous decision 2 ’.
I have to admit that likening the actions of the Committee to the Dismissal is simultaneously hilarious and flattering. Most certainly it is a significant change to classification, and one that warrants serious and detailed scrutiny, and hence the debate at hand. But surely it is not of the same ilk as the Dismissal? Furthermore, the Committee’s decision to adopt ‘alternative schemas that better approximate clinical description with reality and enrich diagnostic formulation’ is stated explicitly and openly at the outset, and there is certainly no hint of treachery or subterfuge.
Approach
Parker’s Viewpoint and my Rebuttal
The critique by Parker, which is presented as a Viewpoint, will be referred to as the Critique or the Viewpoint whereas my response, which is also a perspective piece, will be referred to as the Rebuttal or Perspective.
The Committee and me
Although the Critique begins with a few comments concerning the Committee, it is clear from the outset that the blame for ousting Bipolar II from the MDcpg2020 is largely being assigned to me. This is evident from Parker’s reference to my contribution to his 2019 monograph (Malhi, 2019), in which I commented that I do not regard Bipolar II ‘as a discrete subtype of bipolar disorder’ and nor do I believe it has a ‘distinct underlying pathophysiology’. Furthermore, because of this, I stated that ‘its treatment does not need to be necessarily unique’. Parker goes on to suggest that this statement is the basis for the ‘Committee’s stated views about classifying and managing the bipolar disorders’ and returns to his concern regarding the Committee’s process in the final paragraph of his Viewpoint where he raises the possibility of dissent in the Committee and that perhaps ‘arguments were used to convince the dissenters’. The reality couldn’t be more different.
As Chair of the Committee and given that the insinuation of exerting undue influence is directed at me, I have taken it upon myself to respond to the Critique personally. However, it is important to note that throughout the development of the MDcpg2020 each member of the Committee contributed actively (e.g. in weekly zoom conferences) and decisions, such as the scope of the guidelines, the evidence to be used and the strength of specific recommendations, were all decided collaboratively and consensus was achieved through open discussion.
Strategy
I could begin my Rebuttal, by completely dismissing Gordon’s Viewpoint, and ask that you not waste your time reading his article because it is unsophisticated, poorly written and difficult to follow. But I can’t do this, because the article is none of these things. In fact, as one would expect, it is a well-written and robustly argued Viewpoint in which Gordon raises some important questions. In fact, I would go as far as to say it is an instructive example of how to mount an argument and express it succinctly. However, this does not mean that I agree with what Gordon has to say, indeed, I disagree with him emphatically and to a considerable extent. And so, while I recommend that you do read his Viewpoint, I strongly advise that you reserve judgement as to what he claims – at least until you have also read my Perspective. Then, make up your own mind, as to whether his Critique of the Guidelines is justified, and what is the most useful way to classify bipolar disorder.
So, let’s begin. And there is no better place to start than the beginning. 3
The Crux of Parker’s Critique
The Critique begins by claiming that Bipolar II has been ‘banished’ and then questions the basis on which this was enacted. It outlines the inclusion of Bipolar II in the 4th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), its retention in the 5th edition (DSM-5) and recent inclusion in the International Classification of Diseases (11th Revision, ICD-11). It states that no justification is offered, as to why Bipolar II does not feature in the mood disorders guidelines. As a consequence, Parker looks for clues and initially draws on his monograph (Parker, 2008; now in its third edition) to apportion blame and insinuate that the change has essentially been driven by one opinion, namely me (see Committee and me, above).
Broadly speaking, Parker’s Critique puts forward two main arguments that are directed against the two postulates upon which the ‘Committee’s stated views about classifying and managing the bipolar disorders’ are purported to rest. It is important to understand each of these properly because, although they are linked and ultimately address the same underlying issue, each of Parker’s arguments is constructed slightly differently and therefore it is easier to understand them if they are considered separately.
In his first argument, concerning diagnostic subtyping of bipolar disorder, Parker argues against the position adopted by the Guidelines, which base their management recommendations on the premise that there is no meaningful distinction between mania and hypomania. As a consequence, the guidelines do not observe any formal division of bipolar disorder into subtypes. Contrary to this, Parker argues that Bipolar II is a discrete construct that is separate from Bipolar I.
In his second argument, because the Guidelines do not subtype bipolar disorder, Parker incorrectly infers that the treatment recommendations are intended to apply uniformly to the management of all manifestations of bipolar disorder. He then argues that management should vary according to subtype and that because bipolar II and bipolar I disorder are separate entities their management must also be distinct.
In the remainder of the Viewpoint, Parker draws selectively on available evidence to support his criticisms. And so, I will examine his arguments and discuss the evidence in detail, starting with the need to partition bipolar disorder.
The first question: are there two types of bipolar disorder?
To argue that bipolar II is a discernibly distinct subtype, Parker proposes two mutually exclusive alternatives. First, either there is only one kind of bipolar disorder, and in this unitary model illness severity is the principal source of variance, or second, bipolar disorder is inherently binary and there are ‘two principal categorical types’. To prove the existence of his binary (subtyping) model, Parker discusses a number of his studies.
Bimodal or unitary (subtyping vs severity)
Echoing Kendell, Parker correctly states that if there are two types of bipolar disorder, then the symptoms that define each of these subtypes should be separable. This separation manifests as a point of rarity and Kendell (1976) suggests that this can be found by mapping symptom scores, which then should show a bimodal distribution.
The first study that Parker considers examined the clinical symptoms of just over a thousand patients (n = 1081) diagnosed with bipolar disorder (Parker et al., 2016). They were subdivided into bipolar I and bipolar II subtypes using DSM-IV (n = 497) and clinical judgement, and their manic symptomatology was rated using the Mood Swings Questionnaire (MSQ). This is a 46-item questionnaire and on the basis of this, putative bipolar I and II populations were determined, and further analyses were conducted to create a plot of the number of patients with different MSQ symptom scores. When charted, there are two overlapping normal distributions that are estimated to comprise the observed data and are thought to represent a putative bipolar II and bipolar I population (see Figure 1). Remarkably, Parker’s (2021) Critique describes this as showing ‘a distinct bimodal distribution, supporting a binary model’ even though the results of the paper clearly state that ‘the entropy statistic indicated limited separation and there was no distinctive point of rarity’. In other words, the original paper interpreted the findings more tentatively – stating that ‘findings favour the categorical distinction of bipolar I and II disorders’ as there is no clear separation and indeed no clear ‘point of rarity’. In fact, the overlap is so large and so extensive that the smaller population (putative bipolar I) is essentially subsumed by the larger, putative bipolar II population (see Figure 1). For example, MSQ scores of 60–70 could happily belong to both distributions and in practice, this means that to differentiate the two putative subtypes, a clinical feature is still needed. Hence, Parker ties his definition of bipolar I to psychosis.
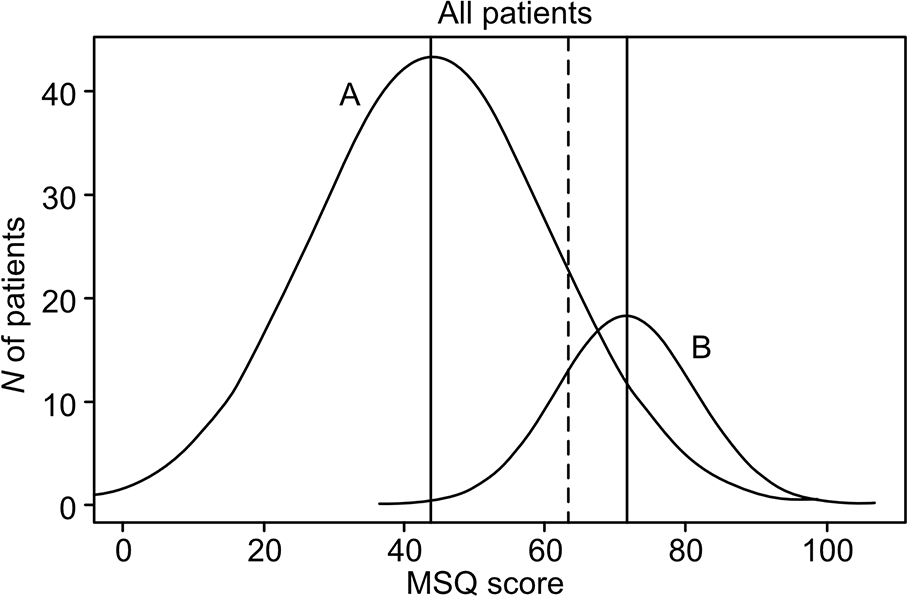
Reproduction of histograms depicted in Parker et al. (2016) showing estimates of observed data as normal distributions. Distributions A and B are thought to represent putative Bipolar II and Bipolar I populations. (For further details see Parker et al., 2016, Figure 1: 107).
In the second study, Parker turns to a more recent project that I briefly contributed to when it first began. It is worth noting that of the original 64 investigators only 11 continued to the stage of analysis. In other words, nearly 83% withdrew – including me. Regarding the findings from this study, Parker once again asserts that the distribution of symptoms in bipolar patients that had been recruited and assessed by the various investigators from around the world is best explained by a ‘two-class solution’. The original paper (Parker et al., 2020) concedes that there was a ‘lack of consistency between patients and clinicians in their rating and reporting of psychotic features’, and while patients are appropriately excused on the basis that patients when severely unwell may not recall their symptoms once they have recovered, the admission that ‘some of the clinicians might have failed in accurately identifying psychotic features in the patients they recruited’ for the study, is an extraordinary limitation, and a particularly important point given that Parker’s bipolar I subtype is largely defined by the presence of psychotic symptoms. Furthermore, once again, the figures depicting the distribution of total symptom scores (for 6, 13 and 15 items) in this study do not immediately show a point of rarity. Indeed, without the smoothed line estimating the density of symptoms, the bar chart for the total score on six items, for example, provides no evidence whatsoever of bimodality. Nevertheless, Parker concludes that the study provides ‘empirical evidence rejecting a single bipolar disorder entity’.
In summary, both studies fail to identify a point of rarity and are unable to demonstrate the existence of any meaningful bipolar subtypes. Remarkably, this is the best evidence that can be mustered and yet, it is still insufficient to cut the mustard.
DSM-5
The arbitrariness of it all?
Parker then turns to DSM-5 (American Psychiatric Association, 2013), and one of his criticisms is that the Committee describes the DSM-5 specification of Bipolar II as ‘arbitrary’. However, I would argue, the fact that Parker defends DSM-5 to some extent and contends that its criteria for bipolar disorders make use of a ‘system’, is of greater concern. Fortunately, he quickly regains composure and adds that DSM is ‘open to some criticism about some illogical nuances’.
Parker’s Viewpoint succinctly summarises DSM’s approach, namely ‘first define a bipolar condition irrespective of subtype’, and ‘then differentiate bipolar I from bipolar II disorder by several criteria’. His critique then focuses on the latter and outlines how DSM achieves this differentiation on the basis of psychotic status, hospitalisation, impairment and duration. He also notes that each of these criteria is ‘somewhat problematic’. Here, we are in agreement and I will return to this issue momentarily. But first, I want to consider the initial distinction made by DSM-5, namely the differentiation of a bipolar condition from a depressive one, a distinction that Parker does not critique and therefore presumably regards as accurate. In practice, this is an important first step and it is particularly significant because of its clinical implications.
In essence, bipolar disorder usually manifests initially as depression, and hence, early in the course of the illness, patients with bipolar disorder are often misdiagnosed as having depression and treated accordingly. But in DSM-5, conferral of a bipolar diagnosis can only occur once manic symptoms are evident. However, the clinical reality is far more complex, and the initial distinction is not limited to that between mania (bipolar disorder) and depression (major depression), because in addition, a significant number of patients first present with mixed mood symptoms.
Nevertheless, DSM continues to maintain its largely polarised view of mood disorders because its taxonomy is predicated on distinguishing mania and depression. In fact, mixed symptoms are described as features, which serve merely as specifiers of mood episodes. And so, in practice, many early presentations of bipolar disorder go undetected, and in the context of depression, mixed mood states are often misdiagnosed as comorbidity or personality dysfunction.
These more complex presentations can perhaps be better captured by mapping the symptoms of mood disorders dimensionally (Malhi et al., 2018, 2019a). And so, while Parker correctly criticises the criteria DSM uses to differentiate Bipolar I and II, it is equally important not to overlook the more fundamental issue of how to distinguish bipolar disorder from major depression.
Partitioning bipolar disorder (subtyping)
Some of the criteria used by DSM-5 to partition bipolar subtypes are clearly irrational.
For example, the use of hospitalisation as a diagnostic criterion, and especially one that transmutes any presentation with manic symptoms into bipolar I disorder, has no clinical validity and is unhelpful both for research and modern-day psychiatric practice where admission to hospital is almost entirely dependent on the level of resources. However, its inclusion is an important reminder as to the origins of the term bipolar II, where initial observations of patients hospitalised with mood disorder were subtyped according to whether they had a history of having been admitted for mania (bipolar I) or depression (bipolar II) (Dunner, 2017).
The other feature that has the same transformative effect on diagnosis as hospitalisation is that of psychotic symptoms. However, the role that these play in the context of mood disorders is somewhat more complicated, and while Parker’s Critique finds fault in the confusing language that is used (first to exclude a manic episode from the criterion for bipolar II disorder [p. 134; American Psychiatric Association, 2013] but then allow specification of the episodes within bipolar II disorder using psychotic features and specifiers, with mood congruent or incongruent symptoms), a somewhat more forgiving interpretation of this could be that these specifiers only apply to depression, and in practice, this could well be the case. However, close inspection of the layout within DSM does not make this clear, and the potential ‘error of logic’ pointed out by Parker is valid.
And so, here again we find a small patch of common ground. First, that hospitalisation is not a useful criterion for diagnosis and especially for subtyping bipolar disorder, and second, the role of psychosis as portrayed by DSM-5 is potentially confusing. However, our views diverge once again as regards how to model psychosis in the context of bipolar disorder.
The next criterion is impairment. Here, the Viewpoint criticises DSM-5’s criterion E of hypomania, where ‘the episode is not severe enough to cause marked impairment in social or occupational functioning’. Parker argues that it is dimensional, subjective and lacking in operational criteria and that because of this, it risks misclassification. In addition, he draws on a recent publication in which the point is made that a change in functioning may not necessarily result in impairment and that, as he puts it, ‘a distinct percentage of individuals experience genuinely improved functioning in both hypomanic and manic states’ (Parker et al., 2020). Again, DSM does allude to this, and leaves the door open somewhat in criterion C of a hypomanic episode, in which it states it is ‘associated with an unequivocal change in functioning that is uncharacteristic of the individual when not symptomatic’ and although perhaps not commonly interpreted as such, this may allow for an inclusion of an improvement along the lines reported by Parker and colleagues. And while these points merit analysis, there is another broader and more important application of functioning in bipolar disorder that is perhaps being overlooked.
Strictly speaking, these criteria are being used cross-sectionally to capture the distress being caused by an episode, i.e. a period of illness. But in reality, as we now know, the illness is present all the time. Indeed ‘impairment’ and its impact on functioning extends beyond episodes per se. That is to say, even when patients are seemingly well (euthymic), cognitive impairment is not uncommon. And so, if criteria such as impairment and functioning are going to be used to define episodes of illness, it is important to have a baseline measure when patients are putatively well so as to identify change. This can be meaningfully quantified by using the same scales to measure these constructs throughout. Once again this is more readily achieved if we adopt a dimensional model and also incorporate a longitudinal perspective. Thus, restricting the consideration of impairment and functioning to episodes, as DSM-5 does, is unrealistic and of little practical value.
Furthermore, the social and societal consequences of having any type of bipolar illness are far-reaching. And therefore, the importance of impairment and functional compromise extends beyond mere classification and designation of episodes to all aspects of a person’s life. Adopting a broader view, and arguably clinically more important perspective, it can be seen that attempting to subtype the illness into bipolar I and II, on this basis perhaps misses the point and risks undermining and devaluing the person’s experience. This is critical, and thus while impairment and functioning need to be evaluated and indeed should be given further prominence in clinical assessments, they should not be a feature upon which subtyping distinction is predicated.
The final DSM feature that Parker’s Critique lists as problematic is that of duration (of an episode). Here, he recognises that duration criteria have been derived from ‘clinical consensus rather than empirical evidence’ and agrees that in this instance the Committee’s use of the term arbitrary ‘is cogent’. It is important to note that the initial definition of hypomania had a minimum 3-day duration criterion and that the decision to extend this to 4 days was ‘not based on data but rather on a concern of the leadership of DSM-IV to limit the diagnosis of bipolar II’ (Dunner, 2017).
Further highlighting the arbitrariness of this criterion, Parker’s Viewpoint notes that the duration criteria do not distinguish meaningfully between bipolar I and II and that instead this criterion introduces the risk of ‘excluding those with a true bipolar condition’. This is precisely the point I made in an article some years ago, in which I sharply criticised the minimum duration criteria for hypomania (Malhi et al., 2016a). Interestingly, this short-coming is tacitly acknowledged within DSM-5 in its ‘Conditions for further study’ section, with the inclusion of the diagnosis ‘Depressive episodes with short duration hypomania’. For this label, the cut-off for the duration of manic symptoms is dropped to at least 2 days (p. 787, American Psychiatric Association [DSM-5]).
On the basis of these criticisms of DSM-5, it would appear that Parker’s Viewpoint supports the Committee’s decision to not give bipolar II credence. However, although Parker disagrees with the manner in which DSM-5 defines bipolar II, he nevertheless supports the subtyping of bipolar disorder, arguing that separate subtypes are ‘likely to have differing clinical features, causes, and responses to differing treatments’. He thus proposes an alternative model that he describes as being more parsimonious. In this, which I shall refer to as Parker’s proposal, bipolar I disorder is used to describe only those bipolar patients who experience psychotic manic states.
Parker’s proposal
In Parker’s proposal, patients with psychotic mania also commonly experience psychotic depressive episodes, and this ‘group’ is distinct from those with bipolar II disorder, who have never experienced a psychotic episode. If this is taken to mean that psychosis changes things, and that the presence of psychotic symptoms indicates the emergence or presence of ‘another disorder’, then this is a notion to which I can lend some support. However, this is a relatively small proportion of bipolar patients, and it does not address the main problem from which all these difficulties derive, namely the categorisation of bipolar disorder. Here, while defining this more ‘parsimonious diagnostic model’, Parker’s proposal includes a description of bipolar II, as those that have ‘categorical hypomanic states’. In other words, those with psychosis in the context of manic symptoms are bipolar I, the remainder are bipolar II. But importantly, ‘hypomania’ remains a category. In other words, while the delimitation of mania is centred around psychosis and its minimum duration criterion is less critical, the lower boundary for hypomania remains loosely in place and approximates to that of DSM-5 (see Figure 2). Once again, this begs the question: what then defines the boundaries of the various bipolar subtypes, especially as we have seen, all of the supposed demarcations and attempts at delineation are extremely problematic, and even the detection of psychotic symptoms to define subtypes appears to be unreliable.
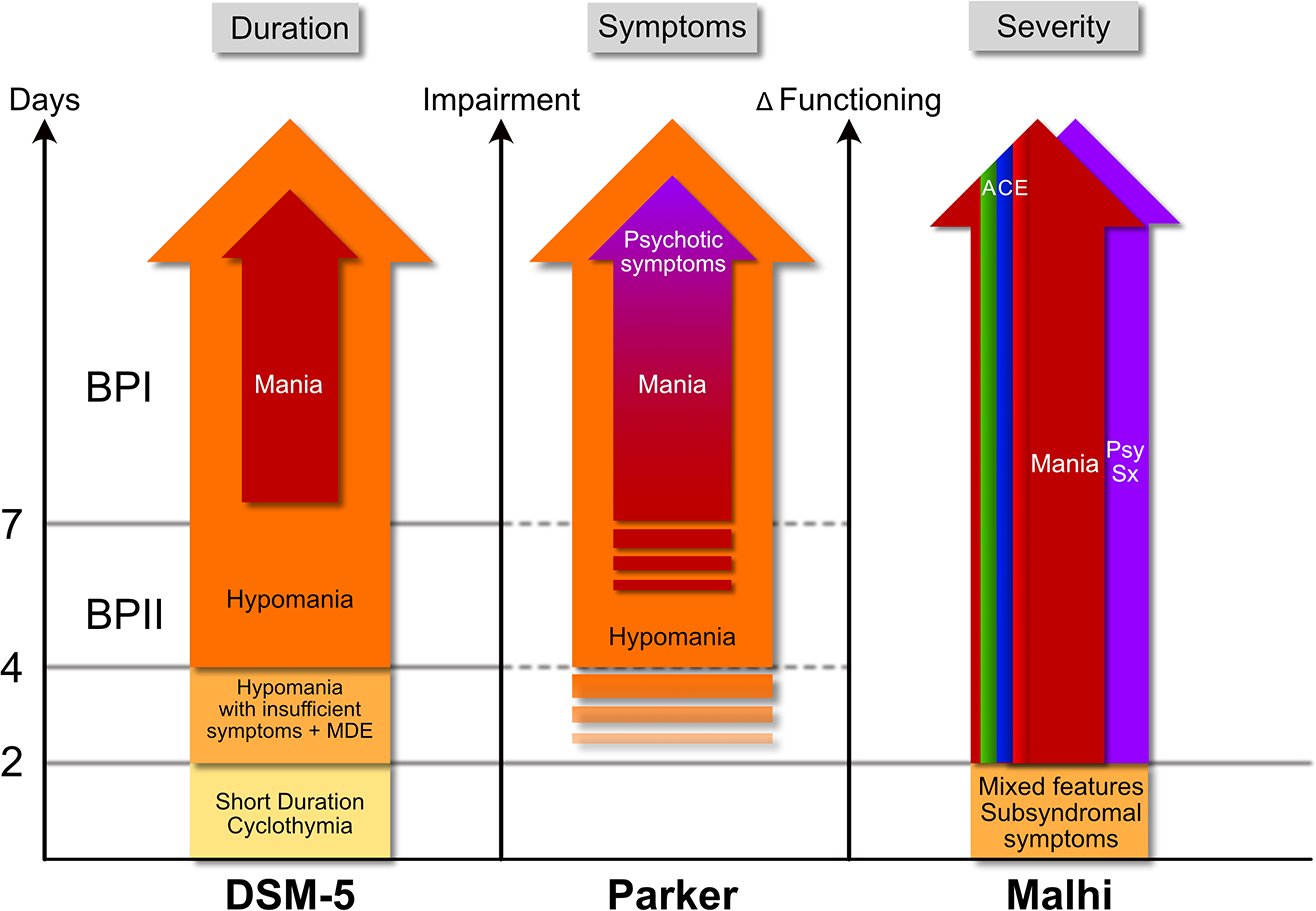
Comparisons between proposed models for the classification of bipolar disorder. The schematic illustrates the different criteria used by DSM-5 (left), those proposed by Parker (centre) and those proposed by Malhi (right) to define bipolar disorders. Each model uses different criteria to inform classification, with DSM-5 relying on duration and Parker employing symptoms to subtype bipolar disorder, and Malhi utilising severity as a dimensional proxy. DSM-5 uses minimum duration criteria to specify bipolar II (4 days of manic symptoms) and bipolar I (7 days of manic symptoms), but it also includes a category of hypomania with insufficient symptoms (with the addition of a major depressive episode), and short-duration cyclothymia, which entails subsyndromal mood symptoms over multiple episodes. Parker’s proposal, which focuses on symptoms, loosely maintains the minimum of 4 days duration criterion for hypomania as outlined in DSM, but relies more specifically on the presence of psychosis of any duration to delineate bipolar I from bipolar II. Finally, Malhi uses the three domains of Activity (green), Cognition (blue) and Emotion (red), which constitute the ACE model to identify symptoms and gauge their severity (modelled dimensionally) and to define the presence of mania or mixed episodes; this model also accommodates mixed features and subsyndromal symptoms. In addition, psychotic symptoms are depicted in a separate domain that runs alongside manic symptoms. These can feature at any time and at any level of impairment/change in functioning and are not necessarily a defining feature of the disorder per se. Broadly speaking, the longer symptoms last the greater the impairment and change in functioning they are likely to cause however, this is a loose association as opposed to a tight correlation, and hence the three measures are represented along the x-axes separately.
The second question: should treatment be tailored to subtype or severity of bipolar disorder?
The second major argument outlined in the Viewpoint stems from Parker’s criticism that the guidelines promulgate a ‘singular management model for managing all the bipolar disorders’ and that a standardising approach such as this has ‘attendant clinical risks’. Clearly, an approach that is not tailored to individual needs, or does not respect natural illness variation may lead to inappropriate treatment, and this is undesirable. I agree, wholeheartedly, and the Guidelines do not advocate for a single management model. Hence, the question I have posed is not whether we should tailor treatment, but that on what basis should this be achieved.
Lamotrigine or lithium?
Contrary to Parker’s assertion, the Guidelines manifestly adopt a tailored and personalised approach throughout and outline very clearly how this should be enacted. This is emphasised in particular in relation to treatment, and so, the criticisms in Parker’s Viewpoint that concern treatment are truly baffling. Parker repeats his criticisms and adds the ‘Committee’s model risks a procrustean treatment approach, where management is identical in those with psychotic and non-psychotic mood swings’ and warns of ‘over-treatment for those not having a bipolar I condition’. This is simply not true. In the Guidelines, the treatment of psychotic symptoms is very clearly noted as is the importance of administering targeted treatment. For example, when considering the management of mania with medication, the guidelines clearly state (Figure 27, p. 73; MDcpg2020) that ‘three elements need to be treated: mania, agitation and psychosis’. In other words, the clinical presentation of mania is not conceptualised as unitary and for the purposes of management, the clinical picture is explicitly broken down into its constituent parts. The guideline then continues ‘if agitation or psychosis are present, then they will need targeted treatment’, and medication ‘Choices take into consideration treatment of all 3 components (mania, agitation, psychosis) whenever possible’ (p. 73, MDcpg2020).
Next, while acknowledging that the Committee addresses different phases of bipolar disorder in the guidelines, Parker’s Viewpoint concerns itself mainly with the maintenance phase, beginning with ‘let me focus only on the maintenance phase medication recommendations’. Using Parker’s own words, ‘no argument is offered for this stance’, and indeed, this narrowing of attention for which no explanation is provided, severely limits therapeutic considerations when discussing phenotypic specificity. The decision to focus on maintenance therapy is perhaps a tacit acknowledgement that the management of acute bipolar depression does not significantly vary between putative bipolar II disorder and bipolar I disorder. But despite paying particular attention to this phase, Parker’s Critique mistakenly claims that ‘the committee’s preferred monotherapy is lithium, with alternative or second-line options being valproate, quetiapine and asenapine. Lamotrigine is not in that prioritised list, although it is later considered as an option in nuanced, non-maintenance situations’. This is clearly inaccurate, because alongside these agents, lamotrigine and aripiprazole are both also recommended as monotherapy Choice agents, and all six medications are recommended for consideration depending on polarity predominance. This oversight is puzzling as there is a clear explanation in the guidelines (p. 83, referring to Figure 32; MDcpg2020), which states that
the chart comprises three overlapping areas, shown by different colours – namely, depression, mania and both. A key consideration at the outset is to determine whether efforts to prevent future episodes need to be focused on one of these particular phases. This has been termed ‘polarity predominance’ and it is best determined on the basis of reviewing past history.
The chart (in Figure 32, p. 84; MDcpg2020) goes on to explain that initially monotherapy is preferable and that where there is a need to prevent future relapses of both mania and depression, lithium is the preferred agent, along with valproate, quetiapine and asenapine. Furthermore, where there is a preponderance of depression ‘lamotrigine may be a suitable option for monotherapy’ and similarly, aripiprazole is a suitable choice where there is a preponderance of mania (p. 85, MDcpg2020). Thus, all six agents are regarded as potentially useful and nominated as Choice agents for monotherapy for the maintenance of bipolar disorder. However, four of these agents (lithium, quetiapine, valproate and aripiprazole) are given some additional emphasis, only because there is modest evidence in support of their use in combinations (see Figure 32, p. 84; MDcpg2020). Thus, contrary to Parker’s assertions, lamotrigine is given sufficient weighting as a monotherapy and it is important to note that it is also positioned as a foundation medication upon which to construct combination strategies when considering Alternatives (p. 85, MDcpg2020).
Having erroneously suggested that lamotrigine was sidelined in the maintenance management of bipolar disorder, Parker suggests that this is because the medication has struggled to gain recognition as a mood stabiliser and this ‘may have contributed to the limited support for it provided by the committee as a maintenance medication’. Once again, this is simply not true, but the key point I wish to emphasise here is that the Committee did not have any bias for, or against, lamotrigine and as such, has represented its use even-handedly throughout the guidelines. However, at the same time, it is important to bear in mind that lamotrigine is simply very different to lithium and that its clinical profile ‘does not accord with a subtype’ per se. Arguably, the only medication that can make such a claim is the prototypical mood stabiliser, namely lithium (Malhi and Geddes, 2014).
Interestingly, having argued for the use of lamotrigine, Parker makes a remarkable statement that ‘the evidence-base in relation to bipolar II disorder maintenance therapy is essentially non-existent’. This begs the question, when arguing for a subtype on the basis of supposed therapeutic specificity, why does Parker choose to focus on the maintenance treatment phase of bipolar disorder? Maybe the real reason is that Parker wishes to argue for subtyping largely on the basis of clinical opinion, as opposed to empirical evidence, and hence he states ‘thus, management options currently weight clinical opinion’. With this statement Parker opens the door to expert opinion, but then rather than discussing individual perspectives he chooses to crudely summate them and report the overall change in the ‘number of invited experts in managing bipolar II disorders’ that expressed a particular opinion as a ‘statistic’, across the first two editions of his monograph (Parker, 2008, 2012). Then, referring to bipolar II disorder, he uses this data as ‘evidence’ to support his assertion that a greater number of clinicians have ‘come to favour or judge lamotrigine as a foundational treatment for this condition’.
Notably, there is no mention of the most recent edition of this same monograph, in which there are 18 chapters that provide detailed commentaries written by different bipolar experts from around the world (Parker, 2019). Each of these clinically experienced academics were furnished with a number of questions, and rather than simply trying to sum up their responses boradly using a number, it is perhaps more informative to examine what they said.
The two initial questions that are also perhaps the most important in relation to our present discussion are as follows:
Question 1: Does the management of bipolar II simply involve an extrapolation model, whereby the treatments that are effective for bipolar I can be viewed as applicable for bipolar II management?
Question 2: What is your preferred mood stabiliser for managing bipolar II, and why?
Extrapolation model
Essentially, question 1 is asking whether the disorder ought to be viewed as dimensional (severity) or categorical (subtype). If it is the latter, that is to say there are distinct subtypes, then perhaps management should also be separate. Whereas if a spectrum model is observed, then perhaps extrapolation of management (where there is evidence) from bipolar I to other subtypes is appropriate.
In response to this question, the majority of respondents endorsed an extrapolation model. Some qualified this, stating that there was really no alternative, given there is no evidence pertaining to the management of bipolar II disorder. Heinz Grunze from Germany (Grunze, 2019) summarised this problem succinctly stating
if we assign bipolar II a bipolar category on its own – saying that it is different from bipolar I or unipolar depression – we need to build an evidence base of suitable treatments. Sadly, our knowledge of optimal treatments for bipolar II has not really progressed.
Tadafumi Kato from Japan (Kato, 2019) extends this point and writes that ‘patients currently diagnosed with the bipolar II condition are highly diverse and cannot be treated as a single illness group’.
Others suggested that it was logical to extrapolate from Bipolar I to Bipolar II disorder, and a few linked their management directly to their dimensional perspective of bipolar disorders as a spectrum. And while most agreed, some such as Robert Post from the United States (Post, 2019) – the architect of the kindling hypothesis – responded ‘yes but with some exceptions’. Interestingly, another North American, Michael Thase (2019), a co-developer of the staging model for treatment-resistant depression (TRD), writes ‘I view bipolar II (BPII) as relatively heterogeneous and, for the first pass in picking therapeutics, try to make a goodness-of-fit judgement for the two relevant extrapolations (i.e. bipolar or recurrent major depressive disorder)’, hinting at the diagnostic conflation of milder bipolar presentations with major depression that I discussed earlier. And finally, Allan Young from the United Kingdom (Young, 2019) writes, ‘at present, the management of bipolar II (BPII) tends to involve extrapolation of the evidence for both treatments from bipolar I (BPI) (i.e. typically mood stabilisers) and major depressive disorder (MDD) (i.e. antidepressants and psychological treatments)’.
Thus, extrapolation is clearly a logical and popular model. However, while there is recognition that nearly all symptoms and syndromes are dimensional, there is an understandable hesitancy when progressing from diagnosis to treatment, because the step taken to administer treatment is a discreet action and so some form of threshold has to be applied. In other words, for the purposes of treatment, we need to be confident that there is a ‘thing’ that we are trying to treat.
This tension is reflected in the answers of the experts, and the ‘mood of the group’, if I can use this phrase, is best summed up by Robert Post’s comment ‘by and large’. The implication being that the majority of clinicians have to be pragmatic and they use the term bipolar II to refer to symptoms that they need to treat. However, this does not mean that they regard it as a genuine disorder per se, or that it has anything more than phenomenological delimitation. In other words, there is no separate substrate that defines the illness and it is not a separate entity. And based on the evidence to date, or more accurately the lack of it, this remains my view.
Preferred mood stabiliser
A pragmatic approach is also reflected in the responses of the experts to the preferred mood stabiliser question posed by Parker, where once again, lithium is repeatedly the preferred choice, and lamotrigine is usually nominated where depression predominates. Even Jay Amsterdam, for example, a strong advocate for antidepressants, states clearly ‘our preferred mood stabiliser treatment is lithium monotherapy’ (Amsterdam and Lorenzo-Luaces, 2019). Lakshmi Yatham, the lead author of the CANMAT guidelines for bipolar disorder nominates lithium as his preferred mood stabiliser because it ‘has the best data for preventing mood episodes in Bipolar II and furthermore, is clearly effective in treating hypomania’ (Yatham, 2019). Similarly, Ayal Schaffer, a fellow Canadian, nominates lithium and states ‘in my experience, approximately one-third of patients with BP II will experience sustained remission when treated with lithium’ (Schaffer, 2019). Interestingly, he also points out that ‘the nature of the response is also qualitatively different –for some patients, lithium can almost feel curative’. Finally, Allan Young once again sums up the sentiments of most experienced clinicians, with the statement In my opinion, lithium should be offered to every patient with BPII who requires long term pharmacotherapeutic treatment ... BPII patients should not be denied the possibility of this and the associated benefits on long term mortality risks from lithium treatment. (Young, 2019)
This is an extremely important comment because it highlights the unique additional properties of lithium and its diverse clinical benefits.
Mistaken equivalence
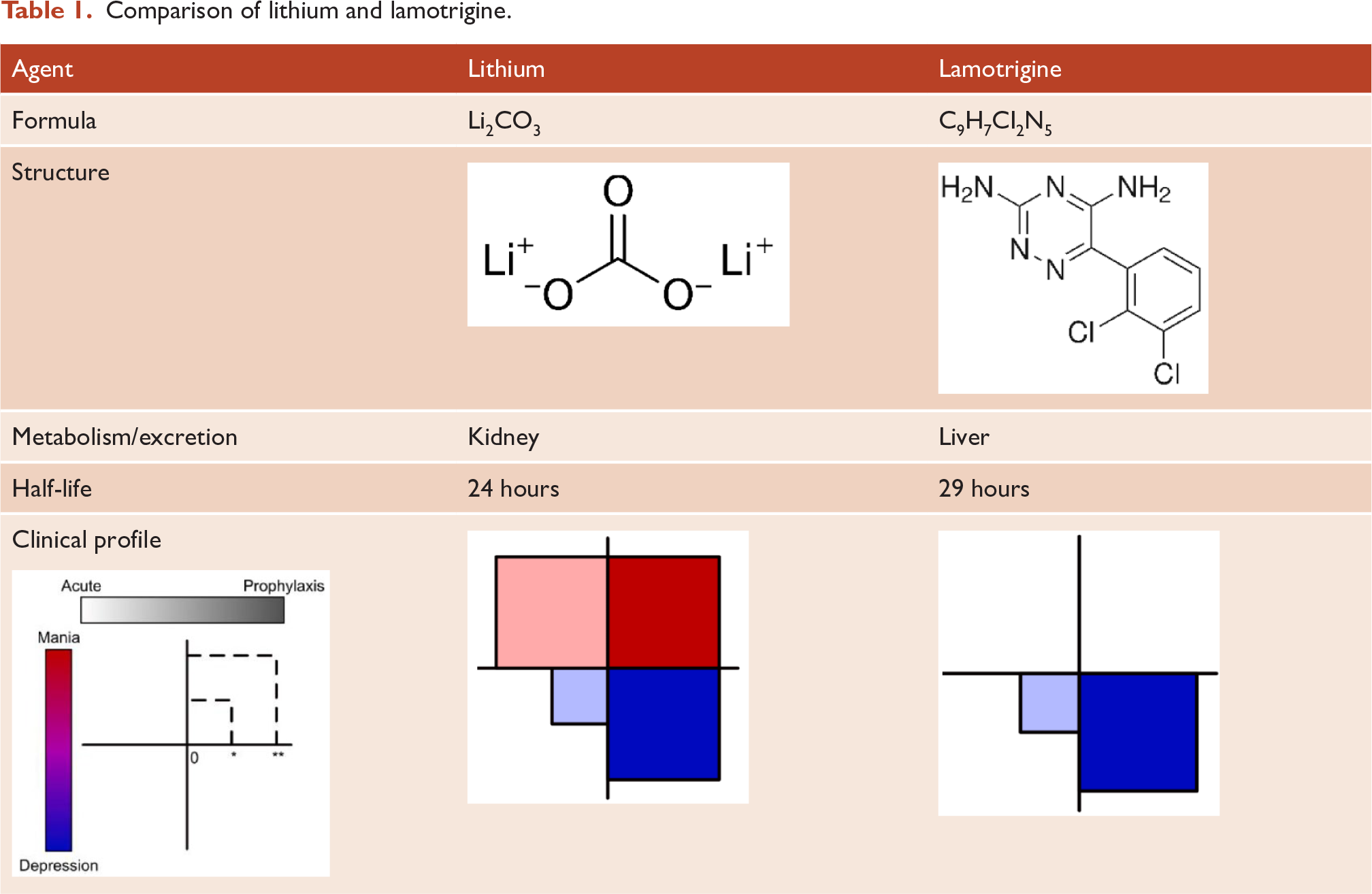
As discussed, and contrary to Parker’s incorrect assertions, the Guidelines clearly recommend lamotrigine monotherapy for the management of both acute bipolar depression and maintenance bipolar therapy. However, it is important to note that even though the two agents are presented alongside one another, this does not mean they are the same. On the basis of his maintenance study Parker implies equivalence when he states, ‘the two medications appeared broadly comparable in their efficacy’. But the reality is that lithium and lamotrigine are unique and very different molecules, as a consequence of which they have distinct pharmacokinetic and pharmacodynamic properties and separate clinical profiles (see Table 1).
Comparison of lithium and lamotrigine.
Parker suggests that lamotrigine somehow has specificity for the putative bipolar II subtype. Repeatedly, he makes the claim that lamotrigine is ‘comparable’ in efficacy to lithium. To substantiate this, he cites evidence, first from his maintenance therapy study, in which 16 patients received lamotrigine and 12 received lithium (Parker et al., 2020), and then from an acute bipolar II depression study, conducted by Suppes and colleagues (Suppes et al., 2008) in which 21 patients received lamotrigine and 19 received lithium. But neither study included a placebo control and therefore predictably, the findings from these small exploratory studies do not demonstrate any differential efficacy. However, Parker interprets this as equivalence of effect. Furthermore, in addition to not being able to separate these agents in terms of effectiveness, Parker fails to appreciate that by arguing for the two molecules to be regarded as comparable in the treatment of putative bipolar II, he is in fact endorsing the view that there is only one bipolar disorder, and that lamotrigine does not show any subtype specificity, as shown by a recent pooled analysis of randomised placebo-controlled trials (Peters et al., 2021). Indeed, if any agent can claim to have some phenotypic specificity it is lithium, which is particularly effective in treating recurrent mood disorders and especially those with discrete episodes that are separated by clear periods of remission (Gershon et al., 2009). This clinical pattern, akin to that of classic manic-depressive illness, is the profile of a lithium responder, and it is important to note that it cuts across DSM-5 and Parker’s bipolar subtypes.
On the basis of treating less than 30 subjects who complete the study, of which only 12 were on lithium, Parker overstates the risks of potential side effects with lithium. Indeed, it is extraordinary the study was aborted ‘because of severe cognitive side-effects reported by several receiving lithium’ and that this occurred even though ‘lithium serum levels did not exceed 0.8mmol/L’. Of course, lithium may affect cognition but these changes are seldom marked and since bipolar disorder is itself associated with cognitive impairment, the cause of any cognitive compromise has to be determined carefully (Malhi et al., 2016b; Wingo et al., 2009).
Somehow, based on inconsistent findings from studies, many of which are clearly underpowered, Parker surmises that ‘lithium may be the preferred first option for managing bipolar I disorder, while lamotrigine is the preferred first option for managing bipolar II disorder’. He adds that in the case of lamotrigine, its efficacy in treating bipolar II disorder ‘may or may not be superior, but the side-effect profile is distinctly superior which argues for a distinct cost-benefit advantage’. An alternative explanation for any variations in efficacy and tolerability across putative subtypes, and one that seems more logical, is that lithium is more effective in treating those patients that have genuine bipolar disorder, and therefore it performs better than lamotrigine in cases of putative bipolar I where the diagnosis is usually clearer. But as soon as the diagnosis is less well defined, as is often the case in putative bipolar II, where patients may have complex mood presentations such as mixed depression or altogether different disorders related to personality, anxiety and substance misuse, in addition to all manner of comorbidities, the efficacy of lithium is much less, and as a consequence it no longer separates from lamotrigine or other agents. Furthermore, if lithium is prescribed to treat conditions for which it is not ideally suited, then in the context of poor therapeutic benefit, its side effects are likely to seem more pronounced.
Bipolar views
Gordon titled his Viewpoint ‘Polarised views’ and so it is unlikely that he will alter his perspective. However, this is not critical as I am not trying to persuade him to change his mind. The reasons for this are twofold. First, to do so, I would require definitive incontrovertible evidence in favour of my position, but as yet, because alternative models have only been proposed relatively recently, there is insufficient proof to unequivocally claim that mood disorders are completely and uniformly dimensional. And so, just because Gordon is unable to support his perspective with watertight evidence, as I have shown, this is not a good enough reason for you to accept my view instead. Indeed, I too need to offer sound reasoning and base my arguments logically on evidence that is beyond dispute. In other words, I need to be able to substantiate my claims and prove my hypotheses. And while I believe wholeheartedly that I am correct, and that the dimensional model I have argued for will be borne out to be true – I cannot simply assert that it is so, and further that it should not be challenged. Hence, I have welcomed debate on this matter and argued this openly (Malhi et al., 2019b; Nierenberg, 2019). However, my position is still far better than that maintained by proponents of subtyping bipolar II. They argue that they have evidence of bipolar subtypes, even though as I have shown, they do not. This is remarkable, and especially noteworthy, given that Bipolar II devotees have had several decades to test their notions and generate the necessary evidence.
Recently, at the 2021 Global Virtual Conference held by the International Society for Bipolar Disorders, a number of eminent experts participating in a Keynote Debate that centred on the use of lithium in the treatment of bipolar disorder, noted with dismay, the complete lack of meaningful evidence for the optimal management of bipolar II. An obvious explanation for this is that both in research and in clinical practice, Bipolar II (as defined by DSM-5) remains difficult to capture with reasonable fidelity. But this is to be expected, and can be explained even more plainly by the fact, that ‘bipolar II’ simply does not exist, other than as an ‘imaginative thing’.
The second reason for not asking Gordon to relinquish his position is that he is committed to using the same approach that he has applied to subtyping depression. As regards the latter, he was correct (Parker, 2000). Melancholia is different and quite separate from the garden-variety depressive disorders that are routinely encountered in primary care. However, his attempt to maintain a bipolar II subtype is not a useful advance because, as I have shown, it fails to meaningfully inform clinical management.
Hence, the Guidelines adopted a dimensional framework that better captures the reality of mood disorders. The ACE model (Activity, Cognition and Emotion) readily maps the complexity of bipolar disorder manifestations including, in particular, mixed states, which current classificatory systems fail to accommodate properly. Similarly, psychosis also gives mood disorders a different complexion, and it too occurs in both depression and mania. Hence, how it impacts the core elements of mood disorders is an important area for further inquiry. In this regard, Parker’s model is useful as it draws attention to psychosis and its need for special consideration. But the mechanisms that drive psychosis are likely to be very different to those that generate mood disorders, and the conceptualisation of psychosis as a separate entity can also be achieved by modelling it as an additional domain that runs alongside those of the ACE model (see Figure 1). A dimensional perspective such as this ‘allows’ psychotic symptoms to occur independent of mood severity, and simultaneously does not limit them to any particular mood disorder presentation. It also ensures that psychosis is given specific consideration when formulating management.
Conclusion
In this Rebuttal to Parker’s claim that the Committee made a mistake to exclude bipolar II disorder from the mood disorders guidelines (Malhi et al., 2021), I have first addressed the failings of Parker’s bipolar II subtype and then countered his justification of subtyping on the basis that it confers therapeutic specificity.
A key problem that Parker faces is that he does not agree with the DSM-5 definition of bipolar II but, at the same time, he wishes to maintain the diagnostic label and has therefore tried to separate mania and hypomania. In Parker’s view, once a definitive diagnosis of bipolar disorder has been categorically made on the basis of longitudinal and cross-sectional features, Bipolar II is defined predominantly by the absence of any lifetime psychotic mania or psychotic depression. This means that mania and hypomania have the same features and the only distinction is the presence or absence of psychotic features. It is therefore unclear why the term mania or alternatively hypomania is needed? Parker could simply have mania and psychotic mania? Indeed, retention of the misleading term hypomania just causes unnecessary confusion.
Parker therefore subtypes bipolar disorder into bipolar I (mania) that is defined by psychosis, and bipolar II, which comprises hypomania and consists of increased energy and elevated mood. It is notable that this is not the same as DSM-5, where the distinction is made largely on the basis of the duration of manic symptoms, and associated impairment and hospitalisation, and although the presence of psychotic symptoms can promote the diagnosis to bipolar I disorder/mania, the subtype is not viewed as an entirely separate entity, and nor is it the only characteristic that defines mania. Therefore, there is considerable difference between DSM-5 bipolar II and Parker’s bipolar II. However, in order to justify his bipolar II subtype, Parker builds a case based on there being a differential in efficacy and specificity of treatment between lamotrigine and lithium. Specifically, he suggests that in bipolar I lithium is more suited, although lamotrigine may also be utilised, however in bipolar II, the two treatments are of comparable efficacy, but that lamotrigine is preferable because of its better tolerability. As discussed, the data from which these inferences are drawn are markedly flawed and the conclusions are inaccurate. But even if this was not the case, the argument lacks validity because the evidence is based on findings from studies conducted in patients with bipolar II disorder that has been diagnosed using DSM criteria – with the exception perhaps of Parker’s own research. Furthermore, if subtypes are defined on the basis of treatment responsivity, then any signal of differential treatment response cannot be used to validate a particular subtype.
In contrast, I remain critical of DSM-5, especially as the necessary research to definitively support a bipolar II subtype has not been conducted. I see no merit whatsoever in the arbitrary cut-offs used in terms of the duration of manic symptoms, nor indeed the context-specific criterion of hospitalisation. However, psychosis can be aligned with the ACE model as depicted in Figure 2 and can be regarded dimensionally, and this creates a more complete and accurate picture of mood disorders that allows for mania, depression and mixed states and the co-occurrence of psychotic symptoms.
In the closing paragraphs of his Viewpoint, Gordon attempts to broaden the discussion and he appeals to ‘other forms’ of mania, which are induced by medication and trauma, and is incorrect in suggesting that the guidelines have advocated for lithium to be used indiscriminately for all bipolar presentations. This is clearly not the case. He also exaggerates the potential side effects of lithium, in particular its effects on cognition. These futile attempts to defend his position reflect the fact that there is no real evidence to support the definition of bipolar II in DSM-5 and that Parker’s own modification of this, with greater emphasis on psychosis, is also incomplete and likely incorrect. Instead, a dimensional approach is needed to better capture the reality of bipolar disorder and treat the illness more effectively. However, this model will also need to be rigorously tested and, at the same time, our taxonomies will need to change. In addition, our current way of thinking about bipolar disorder has to evolve, and so I suggest we start straightaway, by stopping subtyping as ‘thing one’ and ‘thing two’.
Footnotes
Acknowledgements
My thanks to Erica Bell for assistance with preparation of the figures and the article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: G.S.M. has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier; and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.