
Abstract
The suicide rate in bipolar mood disorder is approximately 20-fold greater than that of the general population [1], and may afflict up to 19% of patients with this illness [2]. Because suicide can be difficult to define, and some deaths of uncertain or unknown cause (such as single vehicle accidents) may be the result of suicide but are usually not characterized as such, the actual prevalence may be higher.
Suicide research has largely focussed on risk factors, the single most important of which is the presence of psychiatric disorder. Improving diagnosis and treatment of illness should be a key investigational strategy in suicide prevention [3], but there is little research concerning the relationship of suicide to clinical and therapeutic variables in specific psychiatric disorders. In bipolar disorder the beneficial effect of lithium on suicide attempts has been identified [4] but the impact of other interventions has had little attention [1]. Isometsa et al. found that in 31 bipolar suicide cases in Finland, 79% of subjects were in the depressed phase, and while 74% were in treatment only 32% were being prescribed lithium [5]. The authors concluded that ‘few’ of the bipolar victims had received adequate treatment immediately before death.
The aims of the present study were to examine the clinical characteristics of treated patients with bipolar illness who had suicided and to evaluate the therapeutic interventions received by these patients prior to death.
Method
This study was conducted collaboratively by the Mental Health Research Institute of Victoria and the Victorian State Coroner's Office. All cases of suicide between March 1993 and December 2001 were made available. Cases were selected for further evaluation if there was a clinical record and patients were in treatment at the time of suicide. Their histories were then obtained from treating agencies, primarily public psychiatric services. Some information was obtained from psychiatrists and general practitioners who were prepared to assist. Cases were included only if information was sufficiently detailed to enable completion of the study protocol.
Subjects were diagnosed with DSM-IV bipolar disorder using a semi-structured protocol for post-mortem psychopathological evaluation, the Diagnostic Instrument for Brain Studies [6]. This instrument has satisfactory reliability characteristics [7], generates diagnoses in four diagnostic systems and records presence of symptoms and subsyndromes at any time during illness, as well as in the 3 months prior to death. Evaluation was carried out by two trained psychologists and then confirmed by a psychiatrist. Information concerning demographics, psychosocial factors, social network, and characteristics of suicide, alcohol/drug misuse, health service utilization, and traumatic life events was ascertained. The treatment history was summarized in a narrative chart from illness onset to death, with emphasis on the 2 years prior to suicide.
A clinical panel of three psychiatrists (NK, DC, SS) and a clinical psychologist (CH) then met with the research psychologists to review each case and its treatment history, blind to identifying details of the treating agency. The panel then completed a clinical evaluation protocol for each case. A retrospective suicide risk assessment was made, based on the accepted clinical criteria of risk factor presence, clinical features, past history and lethality. An evaluation of clinical interventions was carried out, and factors including adherence to treatment, substance use, psychopathologic variables, continuity of care, and adequacy of pharmacologic, psychotherapeutic and social interventions were examined. Information was insufficient to reach a conclusion in some instances.
As the benchmark for treatment, the panel utilized the American Psychiatric Association Guidelines for the Management of Bipolar Mood Disorder [8], which was current during most of the time period relevant to the treatment of the cases examined (1993–2001). Accepted doses and levels of medication were those in respective approved product information of the drugs concerned, although doses outside normal ranges were accepted if clinical rationale was evident.
Results
From 3752 deaths identified as due to suicide from the Victorian Coroner's database between March 1993 and December 2001, 35 satisfied all the criteria for entry into the study. Because access to clinical records was necessary to establish diagnosis of bipolar illness, it is not possible to estimate how many cases of bipolar suicide were not included in the study due to inadequate records, inability to access records or incorrect diagnosis reported to the Coroner. Adequate information for diagnosis could not obtained in 33 cases in which the Coroner had recorded bipolar illness.
The characteristics of the 35 patients are given in Table 1. Twenty-two were male and 13 were female. Mean age±SE was 40.3±1.8 years. Only one patient was over age 60. At death 31% were in a relationship while 40% had separated, 3% were widowed and 26% had never married. Forty-six per cent had completed secondary school and 20% had a tertiary qualification. Only 17% were in paid employment. Forty-six per cent of patients committed suicide by hanging, 17% by overdose of prescribed medication, 17% by carbon monoxide poisoning and 11% had jumped in front of vehicles. Alcohol abuse was diagnosed in 31% and substance abuse in 23% (all of whom had also abused alcohol). Ten patients (29%) had toxicological evidence of alcohol/substance use immediately prior to suicide.
Details of patients with bipolar illness who suicided
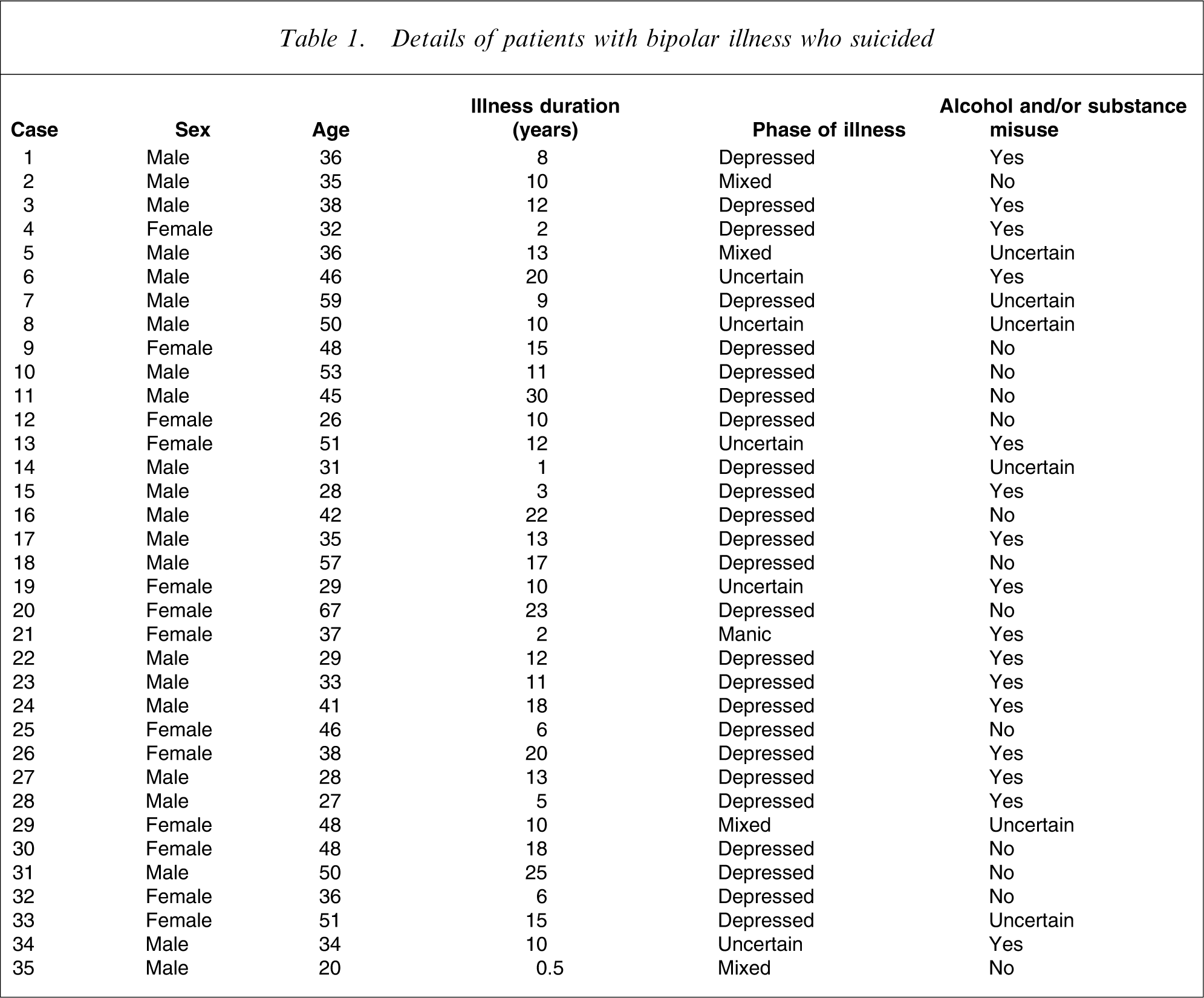
Illness onset had occurred before 20 years of age in 20% of patients, between 20 and 30 years in 51%, and after 31 years in 29%. Suicide had occurred within the first 2 years of illness in 15%. 86% had at least one previous suicide attempt, and 49% had been hospitalized ≥5 times. Mean illness duration was 11.9±1.1 years. A total of 63% had experienced psychosis. Life stressors were apparent in 77% in the 12 months before suicide, and in 46% within the last 4 weeks.
Of 86% patients in whom phase of illness could be determined, 87% suicided in depressed phase, 10% in mixed and 3% (n = 1) in the manic phase. Fifty per cent of subjects had been depressed for <1 month, and 76% for <2 months. The most common previous illness phase was mania (47%), but depression had occurred in 24%, mixed phase in 18%. Five were inpatients when suicide occurred (14%). Six patients (17%) had been discharged from hospital within the previous 4 weeks, and nine within 6 weeks (26%).
In two-thirds of cases it could be determined whether patients expressed hopelessness or manifested agitation during the last illness phase. Hopelessness was expressed by 81% of patients, while psychomotor agitation had been observed in 54%.
The panel performed a standard clinical suicide risk assessment for all subjects, proceeding to evaluate risk as if seeing the patient during the illness phase prior to death in a regular clinical setting, using available information. Risk was rated as severe in 48.6%, moderate in 25.7% and mild in 17.2% of cases within 4 weeks of suicide.
Four patients (11%) had electroconvulsive therapy (ECT) during the last illness episode.
Fifteen patients (43%) were taking lithium during the last 4 weeks of life, but lithium levels were subtherapeutic in one-third. Lithium levels were therapeutic in only four cases prior to suicide (11%) and there was no information in the remainder. Of the entire group of 35 patients, 11 (31%) had never been treated with lithium.
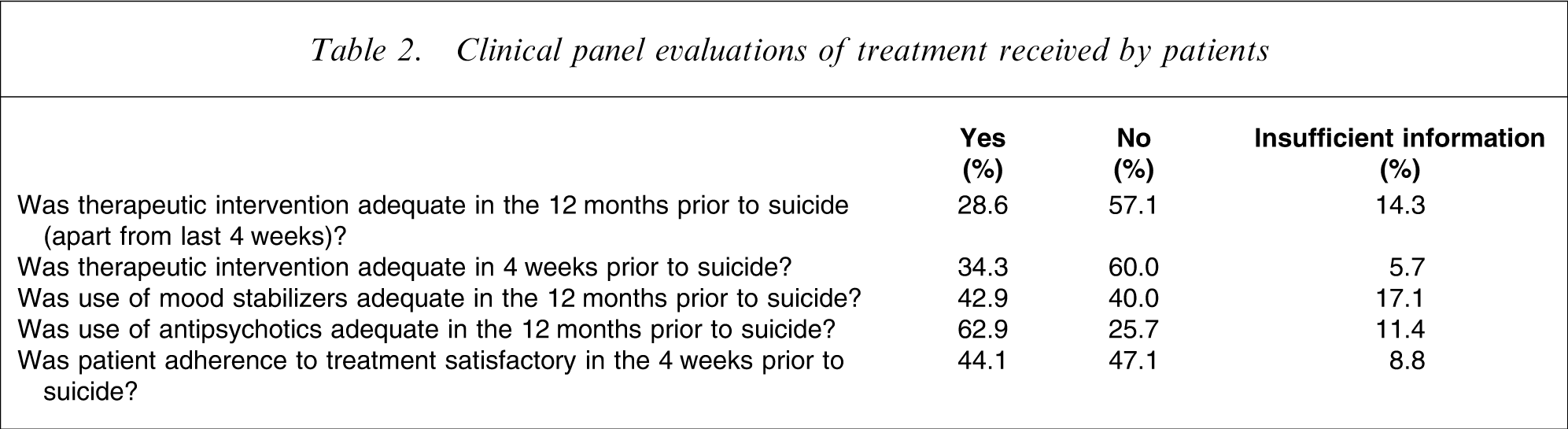
The clinical panel concluded that overall utilization of mood stabilizers during the last 12 months of illness was adequate in 43% of cases, but less than adequate in 40% (with information insufficient to make a determination in 17%). Use of antipsychotics was assessed as reaching benchmark standard during the preceding 12 months in 63% of patients (Table 2). A total of 46% of patients were taking antidepressants at the time of death.
Clinical panel evaluations of treatment received by patients
Psychosocial interventions in the last 12 months were assessed as not meeting adequate standards in 57% of cases. The panel's minimum requirement to rate psychotherapy as being provided was that patients were seeing a particular clinician regularly (at least monthly) for any psychosocial intervention.
The panel separately rated the overall standard of therapeutic interventions. In the 4 weeks prior to suicide, overall treatment was found not to be adequate in 60%. Treatment benchmarks were found to have been achieved in 34%, while in 6% the evidence was insufficient for a conclusion. In the 12 months prior to suicide (apart from the last 4 weeks) treatment was assessed as below standard in 57% of patients (Table 2).
The main reasons for therapeutic interventions failing to reach standards were inadequate pharmacotherapy (38%) and inadequate follow up (33%). Factors such as lack of cooperation by the patient affected the latter. There was evidence of problems with treatment adherence in 47% of patients during the last 4 weeks. In cases in which assertive outreach by community psychiatric services was clinically indicated but had not been provided, treatment was rated as not achieving appropriate standards.
The panel also found that the early signs of onset of the illness phase in which the patient died, were not addressed with adequate therapeutic intervention in 43% of cases. The mental state of patients during the terminal illness phase was not adequately monitored in 60%, due to reasons including non-adherence to treatment arrangements.
Discussion
This study evaluated the treatment of 35 patients with bipolar illness who had suicided in Victoria between 1993 and 2001. The present findings suggest that difficulties in treating bipolar illness may contribute to the occurrence of suicide. Preventative strategies aimed at improving treatment may decrease risk of suicide in bipolar illness.
The sample in the present study was not random; cases were selected retrospectively as being suicides with sufficient clinical records available to diagnose bipolarity and to complete the study protocol. Diagnosis of bipolar illness is frequently delayed; because the present subjects had established bipolar disorder, there was probable selection bias for subjects with longer illness duration. The present patients were being treated primarily by public sector services, although many were also attending private general practitioners and psychiatrists. There was no control group in the present study. It is possible that treatment in cases that could not be evaluated was better than in those with available records.
Another potential criticism of the present methodology is that the findings reflect poor record-keeping rather than poor treatment. It is of course possible that some treatment that did take place was not recorded and therefore did not come to attention. But the clinical panel made a definitive rating only when information was sufficient to make an assessment. If there was inadequate information or uncertainty, a rating of insufficient evidence was made. The method used to assess treatment utilized consensus opinion of experts with reference to accepted clinical guidelines. The process was subjective, no rating instrument was utilized, and the panel was aware of outcome and open to negative bias. In contrast, the panel was able to explore complex cases from a therapeutic perspective, which may not have been possible with more structured procedures. Panel ratings (which were made through discussion until consensus was reached) were not usually difficult to make.
Many of the clinical and illness-specific findings in the present study were as expected. Male subjects predominated, and 86% had made at least one previous attempt. Suicides occurred in well-established illness: only 5/35 suicides occurred within 5 years of onset, which does not support the observations that suicide is likely to occur early in bipolar disorder [4, 9]. Risk of suicide in later illness has also been emphasized by others [5, 10]. The mean age of the present subjects (40 years) does not support the contention that young patients are overrepresented in bipolar suicide [4], but sampling bias cannot be excluded as a reason for the findings. That only one patient was aged over 60 is a striking finding, given that risk of suicide generally increases with age over 70. The significance of this observation merits further examination.
Only a minority of subjects appeared to be receiving adequate treatment at the time of suicide. Although patients’ illness and social predicament often contributed, there was also problematic treatment. The interplay of factors was complex; for example, a number of patients were not prescribed lithium because it was felt that their adherence was inadequate for safe use of a drug with a narrow therapeutic index, although this could have been addressed with more psychosocial input.
A notable finding concerned risk assessment, which is now regarded as a core clinical skill [11]. The validity and reliability of clinical risk assessment has received little examination. Despite retrospective bias, only 49% of the patients were rated by the panel as constituting high risk. Although the panel's ratings were artificial, the question of whether a complex human behaviour such as suicide can be predicted reliably through a risk assessment has to be asked.
Suboptimal pharmacotherapy was the most common reason for inadequate treatment. A common issue was failure to adequately adjust dosages for drugs requiring titration, particularly carbamazepine: patients remained on low starting doses not adjusted to reach therapeutic doses. Other studies have also implicated inadequate pharmacotherapy in bipolar suicide [5, 12].
Lithium is the most effective antisuicide intervention in bipolar illness [1, 4, 13]. Patients on lithium are approximately 70% less likely to suicide and/or self harm [14]. In the present study only four patients were definitely receiving therapeutic lithium. Many patients had tried but ceased lithium, sometimes without clear reason. Approximately one-third had apparently never been trialled on lithium.
Lithium does have a narrow therapeutic index and can cause serious adverse effects. It requires reliable adherence. This can be achieved in challenging circumstances with more intensive psychosocial interventions. There is little information on the anti-suicidal effects of other mood stabilizers, particularly anticonvulsants and atypical antipsychotics.
The present findings concerning inadequate pharmacotherapy must be seen in context of the major unresolved issues in treatment of bipolar depression. Use of antidepressants remains controversial due to the possibility of affective switching and cycle acceleration, and lack of efficacy in controlled studies [15, 16]. Antidepressants have not demonstrated any anti-suicidal effect in bipolar disorder [1]. Clinicians commonly prescribe antidepressants for bipolar depression, usually in addition to mood stabilizers [17], which reduce but do not eliminate risks of inducing switch and cycling [1]. In the present case series the clinical conundrum was underlined by the observation that 46% of the patients were taking an antidepressant at the time of death, although most were depressed.
Only four subjects had ECT in the final illness phase. This suggests underutilization of an effective available treatment for depression. In contrast to use of antidepressants, ECT has a clear role in the treatment of bipolar depression [18], although the evidence base for its efficacy is admittedly quite poor [19].
In 63% of suicide cases in the present series the subjects had manifested psychosis at some stage of illness. This is comparable to the overall prevalence of psychosis in bipolar illness, estimated at 58% [2]. It is improbable that the present study was likely to select non-psychotic bipolar subjects in the sample, so the present findings do not support the possibility that presence of psychosis in bipolar illness increases suicide risk (because a higher proportion of psychosis would have been expected among the subjects were this to be the case). Recent correlations between bipolar clinical indices and suicide have also failed to identify psychosis as a specific risk factor [1].
The present findings relate to suicides, the most recent of which occurred in 2001. There is little reason to believe, however, that the treatment of bipolar illness, and particularly its depressed phase, has improved all that much since. The problems with use of lithium and ECT, inadequate psychosocial interventions, and difficulties with follow up continue as previously, according to our observations. In the absence of a control comparison group, we cannot claim that treatment in bipolar suicide cases was worse than that of patients who did not suicide, but the present findings suggest that improvements in treatment of bipolar illness will save lives.
Footnotes
Acknowledgements
This study was supported by a grant to the Mental Health Research Institute of Victoria from the family of the late Paul Leonard Carroll.