
Abstract
Clinical practice guidelines are important documents as they have the capacity to significantly influence and shape clinical practice in important areas of therapeutics. As such, they need to be developed informed by comprehensive and quality-based systematic reviews, involve consensus deliberations representative of the appropriate experts in the field and be subject to thorough critical review. A revised clinical practice guideline for the management of patients with mood disorders was recently published under the auspices of the Royal Australian and New Zealand College of Psychiatrists. However, this clinical practice guideline was not developed in a manner that reflects the appropriate standards that should apply to clinical practice guideline development and it has critical flaws, especially as it pertains to the use of repetitive transcranial magnetic stimulation treatment for patients with depression. The revision of the college clinical practice guideline has explicitly removed clear and unequivocal evidence-based recommendations that were found in a previous version of the clinical practice guideline and replaced these with consensus-based recommendations. However, the consensus-based recommendations were developed without consultation of the appropriate expert body within the college and contradict the scientific literature. There is substantive and unequivocal evidence supporting the antidepressant use of repetitive transcranial magnetic stimulation in the treatment of patients with depression and its use after a patient with depression has failed a limited number (typically around two) of antidepressant medication trials. Readers should refer to the college Professional Practice Guidelines for repetitive transcranial magnetic stimulation published in 2018 for thorough information about the use of this important new treatment.
Keywords
Mood disorders are common, frequently highly disabling and constitute a considerable component of both specialist psychiatric and general medical practice. As such, ensuring that the individuals treating patients with mood disorders receive up-to-date, accurate information and appropriate training on evidence-based therapies is a critical task of professional bodies such as the Royal Australian and New Zealand College of Psychiatrists (RANZCP). One mechanism that the RANZCP has used to provide this information has been the publication of clinical practice guidelines (CPGs). The mood disorder CPG, first published in 2015 (Malhi et al., 2015), was revised in 2020 and published recently at the start of 2021 (Malhi et al., 2021a). The purpose of this paper is to outline the concerns of the RANZCP Section of ECT and Neurostimulation committee (SENC) with the presentation of the evidence and treatment recommendations in the neurostimulation sections of the 2021 CPG revision.
Our primary concern relates to the section pertaining to treatment with repetitive transcranial magnetic stimulation (rTMS), although there are issues in relation to other forms of neurostimulation. The authors of the CPG have recently clarified their reasons for recommendations regarding the role of rTMS in the CPG (Malhi et al., 2021b). This explanation and the CPG make a number of scientifically unsupported generalisations, which are likely to leave the reader with an incorrect understanding of the evidence supporting the use of rTMS, which we aim to correct here.
Most importantly, the CPG failed to make an unambiguous statement about the effectiveness of rTMS and as such critically misleads the reader. In fact, the section on the efficacy of rTMS in depression in the CPG reads like a critique rather than a balanced assessment as is provided for other treatments in the guidelines. In their supporting article, the authors state ‘But rTMS has been posited as a treatment for depression largely because of its mechanism of action and not because of its clinical effect’. This statement fails to consider the substantive evidence base supporting rTMS therapy. The development and clinical implementation of rTMS treatment has been supported by the most rigorous level of evidence for new treatments. This includes an extensive series of double-blind, randomised, sham-controlled clinical trials which demonstrate the efficacy of rTMS, numerous meta-analyses (e.g. Berlim et al., 2013; Mutz et al., 2018; Sehatzadeh et al., 2019), umbrella reviews (reviews of previously published systematic reviews or meta-analyses) (Fusar-Poli and Radua, 2018) and network meta-analyses (Brunoni et al., 2017; Papadimitropoulou et al., 2017). The CPG authors do not appear to have considered the evidence contained in these studies or conducted a systematic literature review, regarded by the National Health and Medical Research Council (NHMRC) as an essential activity in guidelines development (NHMRC, 2019). As an example, the CPG cites a 2016 Health Quality Ontario (2016) analysis but not a more recent revision of this analysis published by the same group which happens to be more favourable towards the use of rTMS (Sehatzadeh et al., 2019).
There is also evidence to support the effectiveness of rTMS relative to other treatments, which the CPG authors note is required to ‘demonstrate(s) comparative efficacy to inform its positioning in any treatment algorithm’. For example, a recent systematic review and network meta-analysis explored antidepressant options in treatment-resistant depression at 2, 4, 6 and 8 weeks after the commencement of intervention. A superficial reading of the abstract gives the impression that superior outcomes were seen with quetiapine and risperidone for any time period after 2 weeks of intervention. However, rTMS effects were clearly superior to other interventions in regard to response rates at 4 and 6 weeks. ‘Pooled intensities of rTMS were found to be significantly more efficacious than placebo/sham throughout all analyses and numerically better than most pharmacological comparators with the exception of ketamine at 2 weeks’ (Papadimitropoulou et al., 2017). In fact, in regard to response rates after 6 weeks of treatment, rTMS was the only intervention where the confidence intervals were significant. In regard to remission rates, the effects of rTMS were similar to those with aripiprazole and ECT at 4 weeks and ‘at six weeks after baseline, rTMS (80-120%) showed the highest remission rates and ranked first amongst all competing pharmacological interventions’. The CPG does not appear to take this evidence into account, instead criticising the lack of direct comparisons between medication and rTMS therapies.
A further example of systematic evidence supporting the efficacy of rTMS can be found in a recent umbrella review of meta-analyses of randomised controlled trials conducted investigating the effectiveness of forms of non-invasive brain stimulation for depression (Razza et al., 2020a). This review was conducted to inform the development of national neuromodulation guidelines being developed by the Brazilian Association of Psychiatry. The review was prospectively registered, comprehensively conducted and utilised a formal validated process to evaluate the quality of studies (A Measurement Tool to Assess Systematic Reviews [AMSTAR]-2) (Shea et al., 2017) and the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) evidence profile approach (Guyatt et al., 2011). This is the type of comprehensive approach recommended by the NHMRC (2019) but not adopted in the development of the college CPG. This analysis concluded that there was high-quality evidence for the use of rTMS treatment in depression in terms of response rates, remission rates and change in depression scores, with large effect sizes for response and remission rates. The results of this systematic, structured and validated data analysis process support the contention of the SENC that there is undisputed and substantive evidence for the overall effectiveness of rTMS treatment in depression.
It is of considerable importance to note that the reader does not need to rely on the opinion of the current authors, or those of the CPG, to understand the quality of the evidence supporting the use of rTMS. This evidence was recently assessed in the highly independent and rigorous process undertaken by the Medicare Services Advisory Committee (MSAC) of the Australian Government Department of Health. This process involved an extensive evaluation of the efficacy, safety as well as cost-effectiveness of treatment. On the basis of this evaluation, which assessed the insertion of rTMS as a therapy within the existing treatment algorithm for depression, MSAC unambiguously recommended public funding of rTMS for the acute treatment of depression (after two failed medications) (assessment outcomes published in 2018 and 2019).
We also note that a clear statement in regard to the effectiveness of rTMS was made in the 2015 version of the college CPG, but it is unclear why the scientifically justified evidence-based recommendations (EBRs) in regard to the use of rTMS were removed in the 2021 CPG revision and replaced with consensus-based recommendations (CBRs), that is, opinions, primarily of the CPG author group (Table 1). It is essential to note that there has been no lessening of the evidence base supporting rTMS therapy since 2015 which would justify the removal of the clear EBRs. In addition, these CBRs were developed without the input of the members of the SENC and as such do not reflect a widely informed consensus of relevant experts, but rather the specific views of the authors of the CPG.
Evidence recommendation in the different versions of the college CPGs.
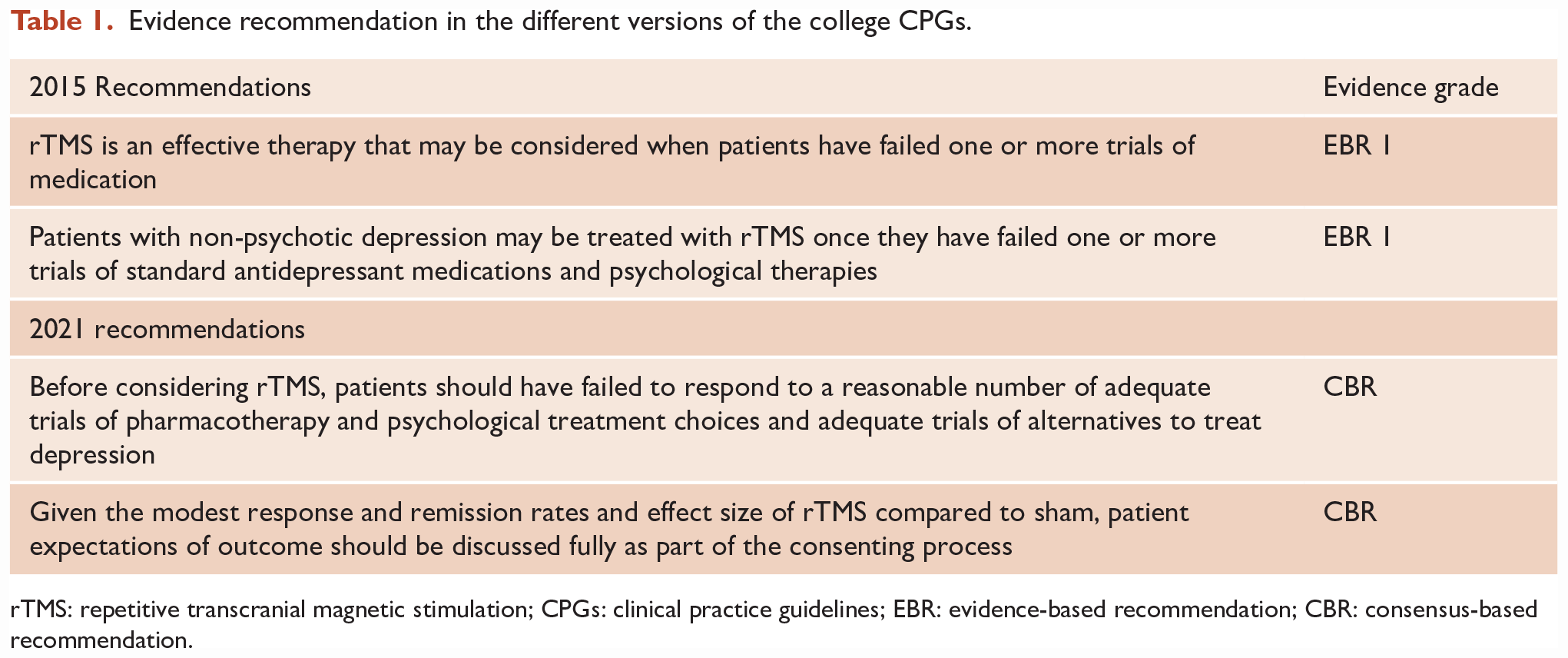
rTMS: repetitive transcranial magnetic stimulation; CPGs: clinical practice guidelines; EBR: evidence-based recommendation; CBR: consensus-based recommendation.
It is important to specifically address the two CBRs made about rTMS in the 2021 CPG. The first recommendation in the 2021 CPG indicates that for a patient to receive rTMS they should have failed to respond to ‘a reasonable number of adequate trials of pharmacotherapy and psychological treatment Choices and adequate trials of Alternatives to treat depression’ with a footnote that this would include the following: ‘Pharmacotherapy Choices should ideally include antidepressants from putatively different classes (e.g. SSRIs, SNRIs, TCAs and MAOIs) and, where appropriate, each antidepressant should be suitably optimised through use of therapeutic dosing (e.g. increasing dose) and augmentation’. An EBR would reflect the demonstrated efficacy of rTMS in patients who have failed to respond to one or more antidepressant medication treatments. This was the approach taken in the 2015 guidelines and other expert reviews of rTMS treatment published previously such as the Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines (Milev et al., 2016). The CBR seems to be premised on the erroneous belief of the authors that rTMS ‘is yet to show efficacy in depressed patients other than those with significant resistance to pharmacological therapy’ (Malhi et al., 2021b). On the contrary, the efficacy of rTMS is typically higher in those with lower levels of treatment resistance (Lisanby et al., 2009). The MSAC in assessing rTMS for public funding concluded the evidence supported use in patients with two medication failures, not the extensive treatment suggested in the CBR. We note the Food and Drug Administration (FDA) in the United States approved rTMS treatment in 2008 for patients who had failed a single medication trial.
Relevant to this discussion are the poor outcomes of repeated courses of pharmacotherapy after two failed medication trials, that is, the main alternative to rTMS. Evidence from the STAR-D study suggests that there is a likelihood of a less than 5% chance of persistent benefit over 12 months in patients who have failed more than two antidepressant medications with pharmacotherapy (Sackeim, 2016). This compares very poorly to the evidence supporting the use of rTMS therapy indicating both acute and sustained benefits (Papadimitropoulou et al., 2017; Senova et al., 2019) and as discussed above, emerging evidence of better outcomes with rTMS than any medication strategy in treatment-resistant depression (Papadimitropoulou et al., 2017).
In addition, a second CBR was made referring to the need for qualifying information to be provided on the ‘modest response and remission rates and effect size of rTMS compared to sham’ in the consent process. The effect size found in multiple meta-analyses of sham-controlled studies of rTMS is moderate, not modest (e.g. see Sehatzadeh et al., 2019). Response and remission rates, and effect sizes seen in trials of rTMS, are equal to or greater than those seen in trials of antidepressant medication and other therapies but the same ‘caveat’ statement was not made in regard to requirements around other forms of treatment in depression. Of note, some of these medication alternatives carry serious side effect risks, but no suggestion is made in the CPG that additional qualifying information be provided for these treatments.
In addition to these important changes in the text, the 2021 guidelines also now fail to present the use of rTMS in the extensive series of figures included in the CPG. In 2015, rTMS (‘if available’) was considered appropriate intervention at step 2 in the main figure presenting the overall structure of the management of patients with depression (see figure 6 in the original publication; Malhi et al., 2015). However, rTMS has been removed or omitted from the main figure summarising the management of major depression (figure 26 in the 2021 CPG). In response to the SENC feedback expressing concern about these omissions, the guideline authors stated that they were ‘unable to accommodate the full range of available treatments within the figures’. However, this was clearly possible in the previous version of the guidelines and there seems to be no reasonable reason for the exclusion of one additional line in figure 26.
It is important to note that the 2021 college guidelines now stand in contradiction to several documents published by the RANZCP as well as MSAC (see Table 2). The guidelines are also inconsistent with international recommendations. For example, the CANMAT guidelines, developed through a process of systematic review of the literature, in contrast to the approach used in the college guidelines, described rTMS as a ‘first-line recommendation for patients with MDD who have failed at least 1 antidepressant’ based on Level 1 evidence (Milev et al., 2016).
rTMS recommendations in college and other relevant publications.
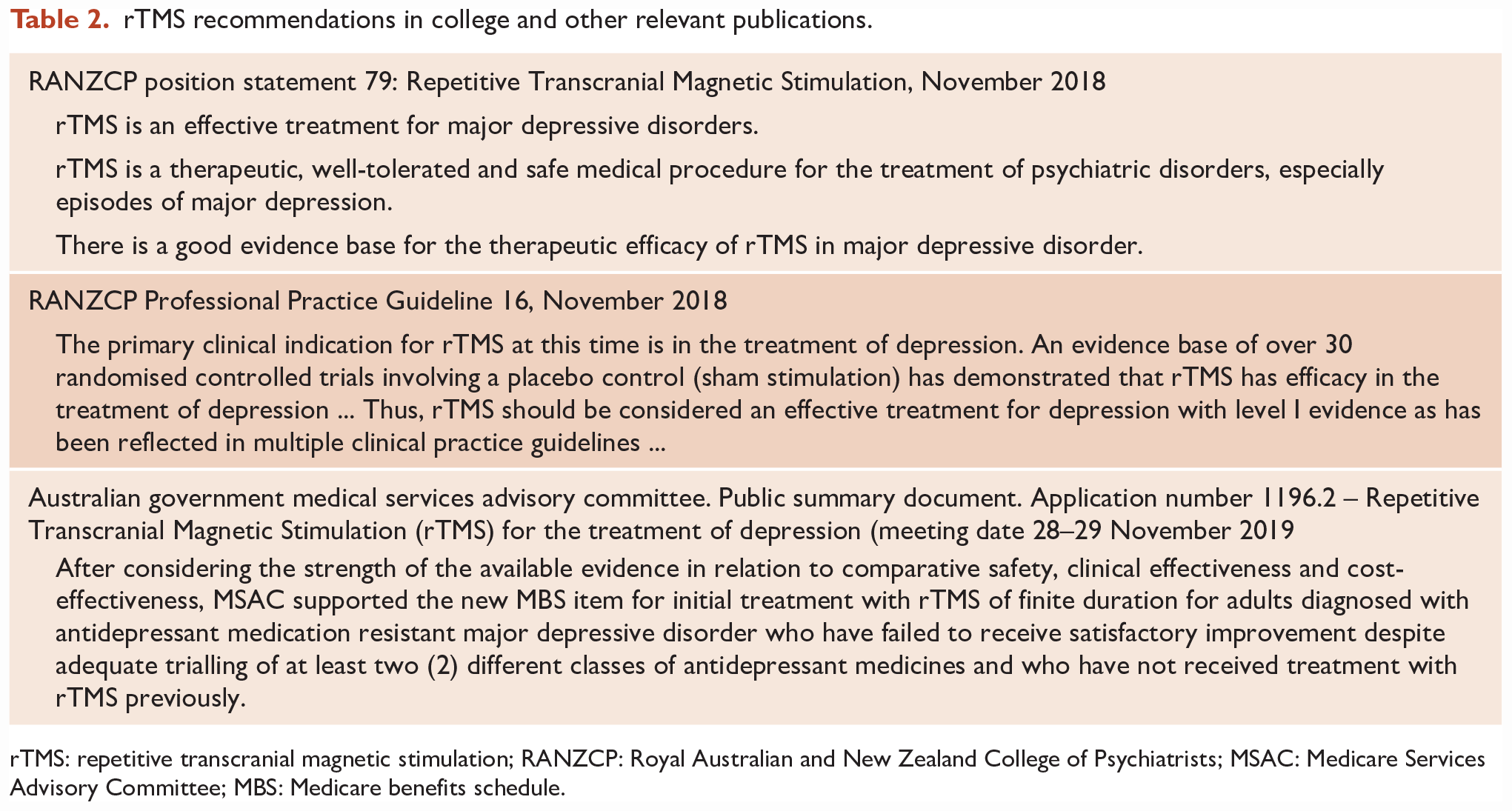
rTMS: repetitive transcranial magnetic stimulation; RANZCP: Royal Australian and New Zealand College of Psychiatrists; MSAC: Medicare Services Advisory Committee; MBS: Medicare benefits schedule.
We also believe that the status afforded to neurostimulation therapies within the framework used to present treatment choices in the management of patients with depression in the 2021 revision of the guidelines is problematic. The authors have adopted an approach such that ‘the guideline is organized around treatments that are essential in all cases (Actions), treatments that are available if these actions aren’t sufficient (Choices) and remaining treatments that may be considered (Alternatives)’. Brain stimulation treatments are exclusively considered under the heading ‘Alternatives’ which does not reflect that these modalities are usually delivered as a part of a comprehensive approach in combination with other treatments (pharmacotherapy, psychological and other interventions) and are core therapies for mood disorders. ECT is afforded ‘Choice’ status in specific circumstances but rTMS is not. This is also inconsistent with other interventions that are included. For example, there is extensive consideration of chronobiological treatments including approaches such as bright light therapy and total sleep deprivation within the ‘Actions’ section which by implication should be ‘essential in all cases’. While we are not questioning the specific evidence for these treatments, it does appear that the balance of representation here is inconsistent with the level of evidence for rTMS in depression and there is no evidence-based justification for this distinction.
Furthermore, it is worth mentioning the brief and inadequate attention paid to addressing the potential role of transcranial direct current stimulation (tDCS). This warranted less than 130 words in a document of over 70,000 words, with only two references. This is despite a recent systematic review and meta-analysis including 23 randomised controlled trials and over 1000 patients with depression finding a robust difference between the effect of active tDCS and sham stimulation in regard to antidepressant outcomes (Razza et al., 2020b). The overall antidepressant effects seen in this analysis were modest in nature, but the same can be said for many other interventions in depression, including those recommended in the current guidelines. The failure to address an emerging treatment like tDCS in a serious way within the guidelines is a clear indication as to the lack of substantive expert input and the failure to underpin the CPG development with adequate systematic review.
In regard to expert input, the CPG states that the guidelines underwent ‘revisions in light of feedback from key college committees’. However, we wish to clarify that the SENC was not given adequate time for input into the guidelines. The SENC was not consulted during the initial drafting of the guidelines and was only provided with a full draft of the guidelines, a document of over 71,000 words, with only 14 days to provide feedback. The guidelines were reviewed and discussed by the SENC who then wrote to the committee overseeing the development of the guidelines identifying what we considered to be major concerns regarding the content, offering the input and expertise of the SENC in a revision of the relevant sections. Given that the guidelines were explicitly making CBRs on therapies, we felt it was important that the ‘consensus’ included the opinion of the SENC who represent substantial clinical expertise in the area of ECT and neurostimulation and represent this expertise within the RANZCP. We made clear in this feedback that 2 weeks was inadequate to collate a full detailed response to the guidelines and that the sections required substantial revision. Examples of our concerns were given, but our written feedback at that time was clearly not meant to be a final, comprehensive series of comments on the content of the guidelines.
Unfortunately, the response that was received to these suggestions was limited. A few, relatively minor changes were made to the content of the guidelines and the offer to contribute to a substantive revision was not accepted. There was certainly no opportunity made available for the members of the SENC, or the Section in general, to contribute to a review of the relevant evidence or the consensus formulation of recommendations. We believe, therefore, that the statement that the guidelines underwent ‘revisions in light of feedback from key college committees’ is misleading and the CBRs should be explicitly identified as only reflecting the input of the limited group of the authors of the CPG.
In conclusion, it is our view that the current 2021 RANZCP Mood Disorders CPG fails to adequately address the role of some neurostimulation treatments in the management of mood disorders. The guidelines failed to adopt the standard defined by the NHMRC (2019) that ‘Recommendations made in guidelines should be informed by well-conducted systematic reviews’ and included CBRs which did not reflect the views of an adequately representative group of experts. The presentation of the role of rTMS treatment is especially inconsistent with the overwhelming evidence supporting the use of this treatment in patients who have failed two or more antidepressant medications as is likely to mislead the reader in terms of the potential role of this therapy. This has important real-world implications. Outcomes for patients who may be offered rTMS are extremely poor with other treatment options, especially repeated trials of different medications as suggested is appropriate in the CPG. Delaying treatment with rTMS on the basis of these guidelines will cause patients to experience unnecessary ongoing suffering and disability. We would recommend that readers refer to college publications specifically on neurostimulation, including recently updated Professional Practice Guidelines for rTMS and ECT, Clinical Memorandum on tDCS, and Position Statements on ECT, rTMS and tDCS for an up-to-date, accurate and detailed account of the evidence base and role of these treatments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: P.B.F. has received equipment for research from Medtronic, MagVenture A/S and Brainsway Ltd. He is a founder of TMS Clinics Australia. S.G. reports no COI. S.H. reports no COI. C.L. has received equipment for research from Mecta. S.S. reports no COIDR SC – Director of TMS Specialists Clinics Pty Ltd. A.W. reports no COI. D.G. reports no COI. S.P. reports no COI. B.S. reports no COI. C.D. reports no COI. T.C. reports no COI.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: PBF Is supported by a NHMRC Investigator grant (1193596).