
Abstract
Objective:
There is considerable research evidence for the effectiveness of repetitive transcranial magnetic stimulation in the treatment of depression. However, there is little information about its acceptability and outcomes in clinical settings.
Method:
This naturalistic study reports on a clinical repetitive transcranial magnetic stimulation service that has been running in Adelaide, South Australia (SA), for 6 years. During this time, 214 complete acute courses were provided to patients with treatment-resistant Major Depressive Disorder. Patients received either sequential bilateral or right unilateral repetitive transcranial magnetic stimulation treatment involving either 18 or 20 sessions given over 6 or 4 weeks respectively. Data included patient demographic details, duration of depression, and medication at the beginning of their repetitive transcranial magnetic stimulation course. The Hamilton Depression Rating Scale was used to assess response to repetitive transcranial magnetic stimulation.
Results:
Of those undergoing a first-time acute treatment course of repetitive transcranial magnetic stimulation (N = 167), 28% achieved remission, while a further 12% met the criteria for a response to treatment. Most patients (N = 123, 77%) had previously been treated with five or more antidepressant medications, and 77 (47%) had previously received electroconvulsive therapy. Referral rates remained high over the 6 years, indicating acceptance of the treatment by referring psychiatrists. There were no significant adverse events, and the treatment was generally well tolerated. In all, 41 patients (25%) had a second course of repetitive transcranial magnetic stimulation and 6 (4%) patients had a third course; 21 patients subsequently received maintenance repetitive transcranial magnetic stimulation.
Conclusion:
This naturalistic study showed that repetitive transcranial magnetic stimulation was well accepted by both psychiatrists and patients, and has good efficacy and safety. Furthermore, repetitive transcranial magnetic stimulation can provide a useful treatment alternative as part of outpatient mental health services for people with depression.
Keywords
Introduction
Depression is a disabling disorder which results in a substantial burden for the individual and their family, and the community more broadly, with lifetime and 12-month prevalence figures of 14.6% and 5.5% respectively in higher income countries (Bromet et al., 2011). Although the introduction of antidepressant medications has been associated with a reduction in the mean length of depressive episodes, many patients experience recurrent episodes (Mulder and Frampton, 2014). Only one-third of patients respond to their first antidepressant medication (Rush et al., 2009). Even fewer patients respond to subsequent antidepressants (Rush et al., 2009). Many patients also receive psychological therapies, augmentation with lithium or an atypical antipsychotic, and/or electroconvulsive therapy (ECT). Patients who have failed two antidepressant drugs, in adequate dose and duration, are considered treatment-resistant (TR) (Rush et al., 2009).
Repetitive transcranial magnetic stimulation (rTMS) provides another option for TR patients. It has been accepted as an evidence-based treatment for depression by the American Psychiatric Association (2010), the Canadian Network for Mood and Anxiety Treatments (Kennedy et al., 2009) and the World Federation of Societies of Biological Psychiatry (WFSBP; Lefaucheur et al., 2014). A group of European experts concluded that based on evidence up to March 2014, there is Level B (probable efficacy) evidence for the antidepressant effect of low-frequency rTMS to the right dorsal lateral prefrontal cortex (DLPFC) (Lefaucheur et al., 2014). Three TMS machines have been cleared by the US Food and Drug Administration (FDA) for use in treating depression. The Interventional Procedures Advisory Committee of the National Institute for Health and Care Excellence (NICE) in the United Kingdom published provisional recommendations for rTMS in June 2015, as part of a public consultation process. In Australia, rTMS has been approved by the Therapeutic Goods Administration, and the Royal Australian and New Zealand College of Psychiatry (RANZCP, 2009) have published a position statement.
The cost of treatment is one of the barriers to more widespread use of rTMS. In Australia, rTMS does not have a Medicare item number and is generally not covered by private insurers. The situation is similar in most parts of the Western world. Given that cost-effectiveness is an important issue, there have been surprisingly few economic studies involving rTMS. A comparison between rTMS and antidepressant pharmacotherapy found that rTMS was cost-effective, especially if it was used early in treatment in preference to repeated switches of antidepressant (Simpson et al., 2009). While an earlier study found rTMS was more cost-effective than ECT (Kozel et al., 2004), more recent work has suggested that ECT has economic advantages (Vallejo-Torres et al., 2015).
The rTMS protocols for depression involve applying repeated magnetic pulses to the area of the scalp over the DLPFC. The magnetic pulses generate a brief electrical current which stimulates the underlying nerve cells. A meta-analysis by Slotema et al. (2010) indicated that patients commonly receive between 5 and 25 treatments. Excitatory stimulation over the left DLPFC was the most common form of treatment, with inhibitory stimulation over the right DLPFC being the next most common. Some patients received bilateral treatment, with both forms of treatment given sequentially during each treatment session. There is no need for an anaesthetic and rTMS is generally well tolerated. Seizure is the most serious adverse event reported, with an estimated risk of 0.003% per treatment exposure (Carpenter et al., 2012). Numerous reviews and meta-analyses, drawing upon published data for more than 2000 patients, have consistently demonstrated the efficacy of rTMS (Gaynes et al., 2014; Schutter, 2008; Slotema et al., 2010).
The majority of rTMS studies have been conducted in research settings. In clinical practice, patients are not subject to rigid selection criteria, and tend to have more medical and psychiatric co-morbidities. Naturalistic studies provide an avenue through which findings from research can be translated to practical settings (Carpenter et al., 2012). To date, there have been few published studies describing clinical rTMS services. In one of the biggest studies in a community setting, Carpenter et al. (2012) described 307 patients treated across 42 clinical practices. Patient-reported response and remission rates were 41.5% and 26.5%, respectively. Dunner et al. (2014) followed 257 of these patients and found that 62.5% of those reaching the criteria for response or remission at the end of their acute course still met response criteria at 12-month follow-up. While the outcome measures are arguably less robust than might be desired (Clinical Global Impressions–Severity of illness scale; 9-Item Patient Health Questionnaire; and Inventory of Depressive Symptoms–Self Report scale), the results were consistent with those found in research settings. Another study by Frank et al. (2011) reported on an unselected group of 232 patients treated with between 10 and 20 treatments of 20-Hz of left unilateral rTMS. In their naturalistic sample, data was available for 130 patients, with 40.8% responding to treatment.
Further research is needed to evaluate the usefulness and effectiveness of rTMS in everyday clinical practice. This is particularly important given that the population in clinical samples may differ from those recruited in research settings. In addition, the context in which treatment occurs, including characteristics of the mental health service, availability of alternative treatments for depression and attitudes of clinicians towards neurostimulation treatment, can all impact on clinical rTMS services. Research studies are isolated from these considerations. There are few studies of consecutively referred patients receiving a first course of treatment in a clinical setting.
In August 2008, a TMS unit was established at The Adelaide Clinic, a private psychiatric hospital (see Galletly et al., 2010). The service has been funded by Ramsay Health Care (SA) Mental Health Services. The inclusion criteria were broad, reflecting TR patients seen in routine practice. This report presents data from patients taking part in an acute course programme during the first 6 full years this service has been operating.
Method
Patients
Patients were referred by private psychiatrists affiliated with Ramsay Health Care (SA) Mental Health Services, and were required to have private health insurance. All patients met the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria for Major Depressive Episode. This was confirmed by a TMS psychiatrist and the Mini International Neuropsychiatric Interview (Sheehan et al., 1998). They were excluded from rTMS treatment if they had insufficient English skills to complete assessments, metal plates/implants in their skull, a history of epilepsy, or were withdrawing from drugs or alcohol. Patients with co-morbid psychiatric disorders including anxiety disorders and personality disorders, or with medical co-morbidities (other than those listed previously) were not excluded. The majority of patients were taking antidepressant medications (93%) and/or antipsychotic medication (66%). Some were taking sedatives (30%) and mood stabilisers (21%). There were some patients who were also taking medications for physical health conditions. There were no restrictions on the medications patients were taking before treatment, but referring psychiatrists were requested not to make any changes after referral for rTMS or during the rTMS treatment.
Patients were assessed by a TMS psychiatrist who confirmed the patient’s suitability and undertook a mapping procedure. All treatments were delivered at 110% of the motor threshold. The resting motor threshold was determined using visual methods (Pridmore et al., 1998). The motor threshold was individually determined for both left and right sides for bilateral treatment courses. The site of stimulation was determined by first locating the point at which maximum stimulation of the abductor pollicis brevis muscle was achieved and measuring forward 6 cm from the coil. A template was prepared for each participant to ensure the coils were positioned correctly at each treatment session. Patients were treated as outpatients and remained under the care of their private treating psychiatrist during and after rTMS treatment.
rTMS session parameters
During treatments, patients sat in a reclining chair and were provided with disposable earplugs or headphones. Treatments were administered using a MagPro R30 machine and MCF B65 figure-of-eight coil (MagVenture A/S, Denmark). Only one TMS machine was used throughout the 6 years of this study. In general, the machine operates 3–5 days a week. The TMS clinicians received training through the Monash Alfred Psychiatry Research Centre, Melbourne. Treatment is given by trained staff with nursing or allied health qualifications. Three research officers were involved over the 6 years; all were psychology graduates and received training to ensure good inter-rater reliability.
In the initial years of the service, sequential bilateral rTMS was used, based upon the literature at that time which indicated a combined benefit of both left and right stimulation (Fitzgerald et al., 2006). A comparison of bilateral with low-frequency stimulation over the right DLPFC was then undertaken, as unilateral treatment was less time consuming and, if efficacy was similar, could be adopted instead of the bilateral protocol (Loo and Mitchell, 2005).
In bilateral treatment sessions, intermittent high-frequency rTMS (10 Hz) delivered in 5-second intervals with a 25-second intertrain interval (1500 pulses) was applied to the left DLPFC for 15 minutes, followed immediately by 15 minutes of unilateral low-frequency rTMS (1 Hz) applied to the right DLPFC continuously at a rate of one pulse per second for 15 minutes (900 pulses). In unilateral treatments, continuous low-frequency rTMS (1 Hz) was applied to the right DLPFC for 15 minutes only.
rTMS protocols
Three different treatment protocols were used over the 6 years as part of a series of studies to identify the most effective, time-efficient rTMS programme (Galletly et al., 2012; Gill et al., 2014). Bilateral treatment courses were delivered either five times per week for 4 weeks (20 treatments), N = 48 completed courses, or three times per week for 6 weeks (18 treatments), N = 65 completed courses. No significant differences in efficacy were found between these two protocols (see Galletly et al., 2012). Subsequently, 101 full courses of right unilateral rTMS three times a week for 6 weeks (18 treatments) were administered.
Measures
All patients were assessed just prior to beginning rTMS and immediately following the conclusion of treatment. The 17-item Hamilton Depression Rating Scale (HAM-D; Hamilton, 1960) was the primary outcome measure. The Montgomery–Åsberg Depression Rating Scale (MADRS; Montgomery and Åsberg, 1979), the Zung Self-Rating Depression Scale (Zung, 1965) and the 14-item Hamilton Anxiety Rating Scale (HAM-A; Hamilton, 1959) were included as secondary outcome measures. Using the STAR*D criteria (Rush et al., 2004), response was defined as at least a 50% reduction in HAM-D score. A reduction between 25% and 50% in HAM-D score was defined as partial response. A patient with a HAM-D score of 7 or less was defined as being in remission. For a patient to receive a second or third course of treatment, they needed to have shown a 50% reduction in symptoms as measured by the HAM-D (Rush et al., 2004) in their previous acute rTMS course. The Mini International Neuropsychiatric Interview (Sheehan et al., 1998) was used to assess for co-morbidities.
Data analysis
SPSS Version 21 (IBM SPSS Statistics for Windows, Armonk, New York) was used to analyse the data. Differences in demographic and protocol variables were tested using Pearson Chi Square tests (χ2) and Mann–Whitney U tests. Shapiro–Wilk tests were used to assess the distributions of each measure. As these continuous variables were not normally distributed, Wilcoxon signed-rank tests (Z) were used to compare baseline with post-treatment measures. All statistical significances were set at p < 0.05.
Ethics
The clinical service and associated research conducted throughout were approved by the Ramsay Health Care (SA) Mental Health Services Research and Ethics Committee. All patients provided written informed consent.
Results
Referrals
The rTMS service has been well accepted with approximately 60 psychiatrists referring patients. Referral rates have remained relatively steady across the 6 years, although there has been an increase of recent.
Patients
The progress of patients through the rTMS treatment service is presented in Figure 1.
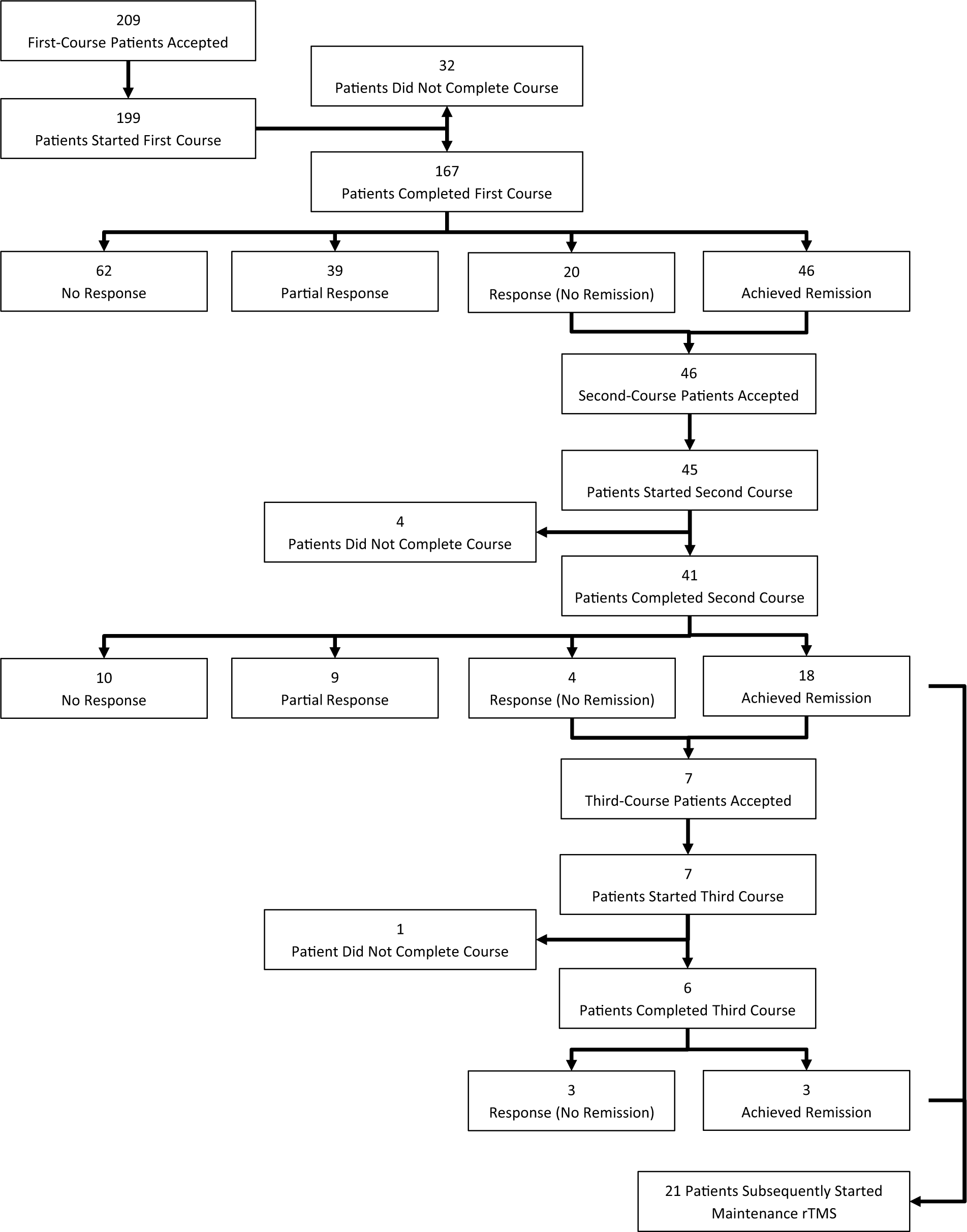
Progress and treatment outcome of patients accepted for rTMS treatment.
From 2009 to 2014, a total of 214 complete courses of rTMS were delivered. Forty-one of these were second-time courses, and six were third-time courses. Descriptive statistics regarding patients receiving their first course of rTMS treatment are presented in Table 1. Thirty (18%) first course patients met criteria for bipolar disorder. Twenty-two (13%) met criteria for a co-morbid alcohol and/or substance abuse disorder. One hundred (60%) met the criteria for a co-morbid anxiety disorder, the most common being generalised anxiety disorder and social phobia. Finally, 16 (10%) met criteria for obsessive compulsive disorder, while 13 (8%) met criteria for posttraumatic stress disorder.
Descriptive statistics for patients (N = 167) at the time of their first course of rTMS.
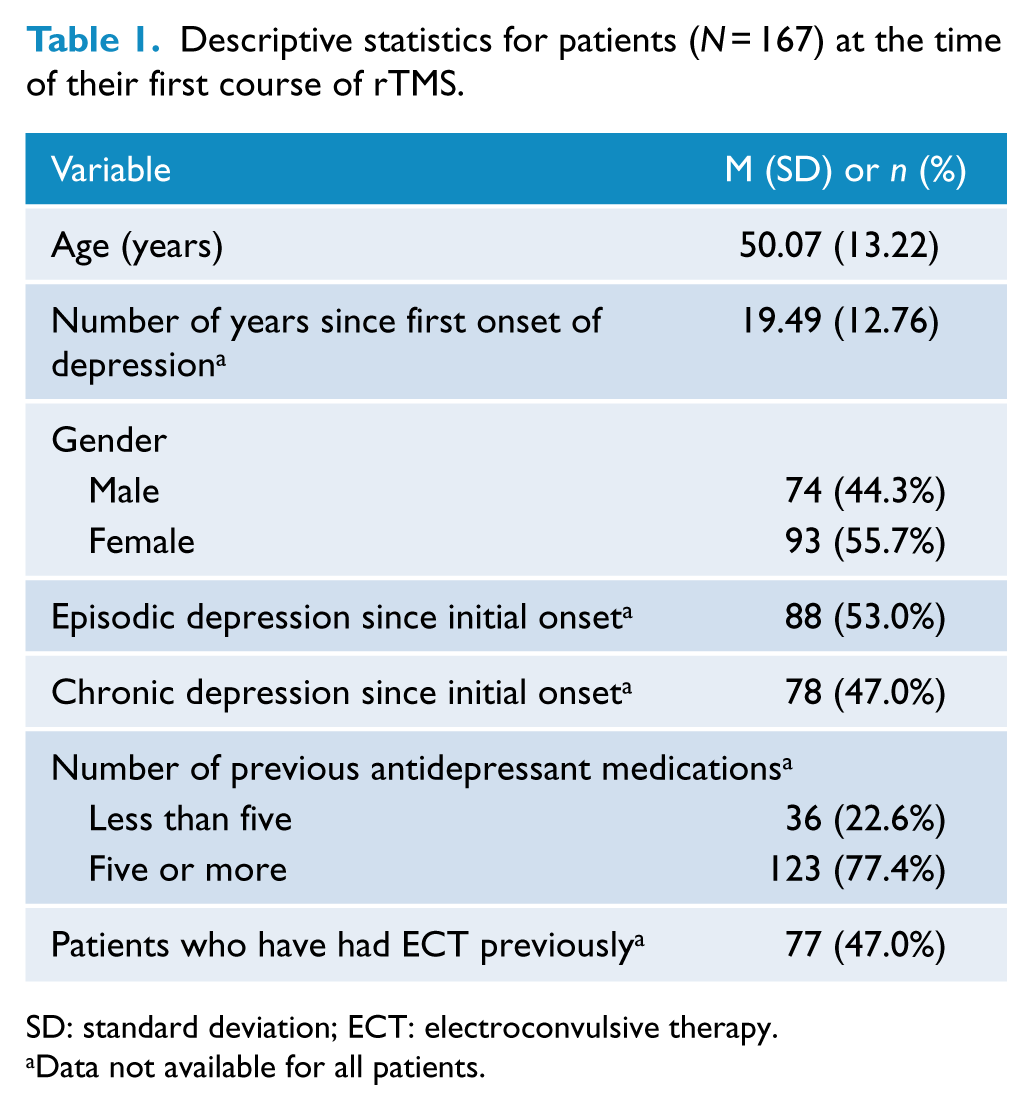
SD: standard deviation; ECT: electroconvulsive therapy.
Data not available for all patients.
First rTMS courses
For patients undergoing their first course, Wilcoxon signed-rank tests revealed a statistically significant change in scores on the HAM-D, the MADRS, the Zung and the HAM-A following treatment with rTMS, indicating that symptom severity had decreased (see Table 2). All analyses revealed large effect sizes.
Mean (SD) pre- and post-treatment scores, mean change in scores and associated significance tests for patients (N = 167) treated with their first course of rTMS.
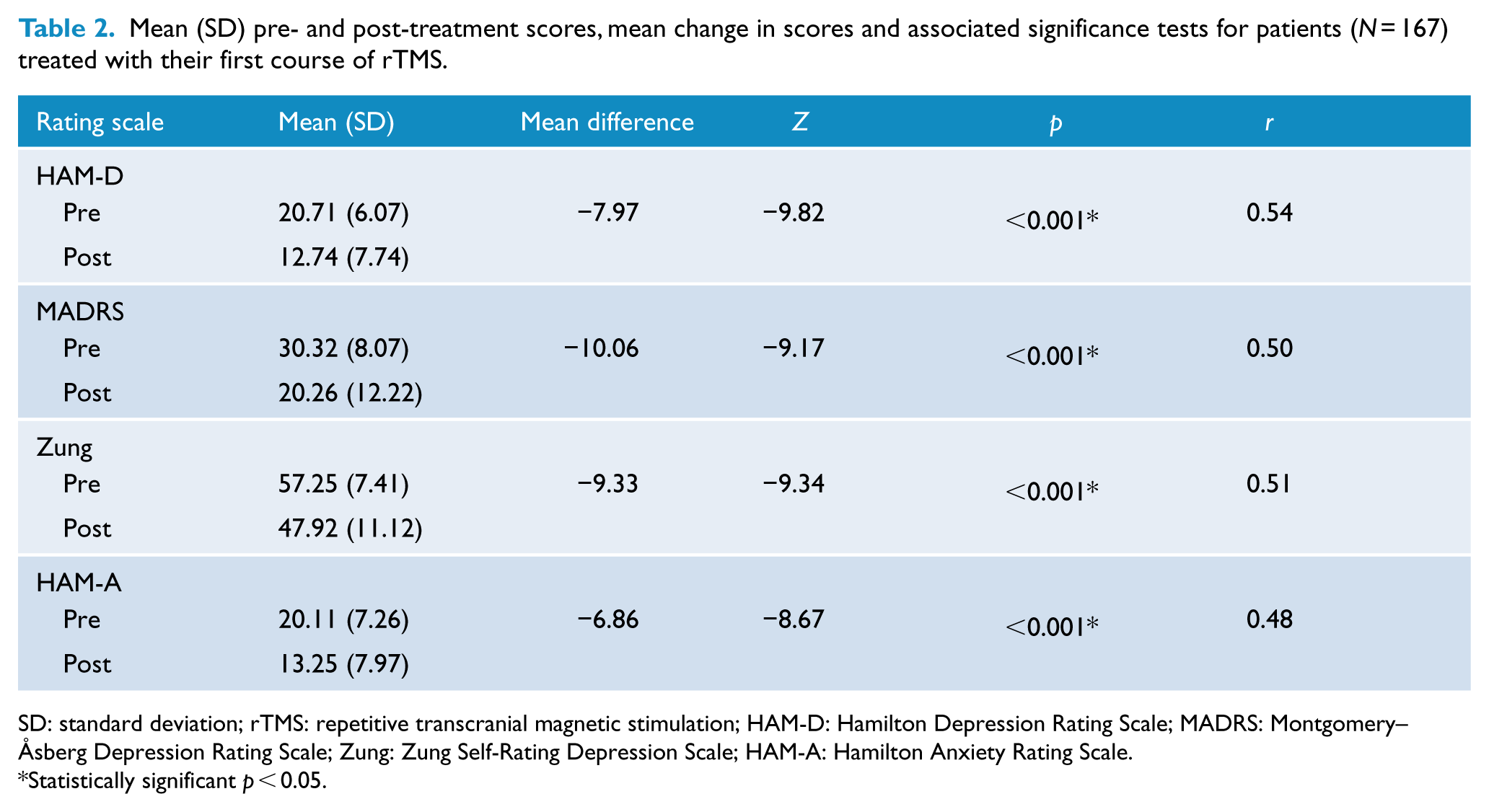
SD: standard deviation; rTMS: repetitive transcranial magnetic stimulation; HAM-D: Hamilton Depression Rating Scale; MADRS: Montgomery–Åsberg Depression Rating Scale; Zung: Zung Self-Rating Depression Scale; HAM-A: Hamilton Anxiety Rating Scale.
Statistically significant p < 0.05.
Of the 167 patients who completed a first course, 46 (28%) achieved remission. A further 20 patients (12%) met the criteria for a clinical response (but not remission), while another 39 (23%) met criteria for a partial response. Of those who responded to a first course, there was an average improvement in HAM-D scores of 15.05 points.
There were no significant differences between responders and non-responders in age (N = 167, U = 3273.0, p = 0.99) or gender (N = 167, χ2 = 0.38, p = 0.54). However, non-responders were more likely to have been treated with five or more antidepressant medications (N = 159, χ2 = 6.29, p = 0.012) and to have received ECT (N = 164, χ2 = 3.89, p = 0.049). Of those having previously been treated with five or more antidepressants, the response and remission rates were 33% and 24%, respectively. For those who had trialled fewer antidepressants, the response and remission rates were higher at 56% and 39%, respectively.
There was no statistically significant difference in response, χ2(1) = 3.01, p = 0.08, and remission rates, χ2(1) = 2.43, p = 0.12, between patients receiving bilateral and unilateral protocols, however there is a small trend favoring bilateral rTMS.
Subsequent rTMS courses
Of the 41 patients who completed a second course of rTMS, 22 (54%) responded to treatment and 10 (24%) showed a partial response. Eighteen (44%) also achieved remission. Of the six patients who completed a third course, all responded to treatment, with three also meeting remission criteria. For those who responded to a second and third course, the average improvement in HAM-D scores was 15.33 and 16.67 points, respectively.
If a patient had responded to two acute rTMS courses, they could be referred by their treating psychiatrist for maintenance rTMS. This was delivered at intervals of 1–4 weeks. Twenty-one patients have been treated with maintenance rTMS.
Number of treatments
Over the 6 years, a total of 6112 treatments have been administered for the treatment of depression within this clinical service. Of these, 1092 (18%) were maintenance rTMS treatments.
Safety and tolerability
There have been no serious adverse events. In particular, there have been no seizures or switches to mania. The most commonly reported adverse events have been localised discomfort, mild headaches and some tiredness following treatment sessions. The majority (69%) of patients treated with rTMS reported no side effects, while only 4% experienced side effects severe enough to interfere with their functioning (see Clarke et al., 2015).
Dropout rates
Of the 251 patients who began a course of rTMS, 20 dropped out during treatment (8%). Most commonly, patients did not return for their remaining treatment sessions. Only five patients dropped out due to their condition declining. A further 17 patients did not have acceptable data as they completed the course but did not participate in a follow-up assessment (N = 5); their course of treatment was substantially interrupted, for example, due to physical illness (N = 10); or the intensity of stimulation had been reduced below an acceptable level on request of the patient (N = 2).
Discussion
The current study demonstrates that rTMS is an effective treatment option for patients with TR depression. These results are consistent with previous research from randomised, controlled trials (e.g. Gaynes et al., 2014). In the present study, 40% of patients responded to an acute treatment course of rTMS, a figure consistent with other clinical services reported by Frank et al. (2011) and Carpenter et al. (2012). The response to rTMS seems to be consistent in that the majority of those who responded to a first course also responded to a second course.
There is no established process for introducing new non-pharmacological treatments in psychiatry. When new medications become available, the pharmaceutical companies undertake product familiarisation, clinician education, and marketing. New information about monitoring or safety is promptly communicated to all prescribers. In contrast, novel non-pharmacological treatments are introduced in an ad hoc way and there can be a major disconnect between the relevant research and the use of the treatment in the real world. With rTMS, the situation is good, with several high-quality, research-based training courses for clinicians now available in Australia (Black Dog Institute, 2015; Brain Stimulation, 2015). More work is needed to define the optimal parameters for treatment, and work out the place of rTMS in the algorithms for TR depression. Naturalistic studies make a useful contribution to the gradual adoption of a new treatment into everyday practice. They provide a bridge between rigorously performed research studies, with restrictive inclusion criteria and often with sham or placebo conditions, and everyday clinical practice.
Our own work shows the acceptability of rTMS and that it is effective in a non-research setting. However, many questions remain. For example, guidelines to assist in deciding whether a patient should have rTMS, ECT, or a further trial of antidepressants would be helpful. Very little is known about predictors of response to rTMS; given the cost and time commitment required for treatment, such predictors would be very helpful. There is a need for more information about the use of rTMS as a first-line treatment, and in special populations such as adolescents, pregnant women, or the elderly. The funding of rTMS remains an issue that limits access for many patients. Our service is supported by Ramsay Health Care, but patients who do not have private health cover are restricted in their access to this service, and there is no public rTMS service available in SA.
There are some limitations to this study. First, as a private hospital, the patient group was not typical of the Australian population as a whole. The method used to locate the DLPFC, while commonly reported in the literature, is not considered the most reliable measure (Herwig et al., 2001). Neuroimaging, regarded as the gold standard, is not practical for all patients in a clinical service, but an approach that accounts for the size of the patient’s head (such as the F3 Beam method; Beam et al., 2009) would offer a more precise measure. Patients continued their medication throughout rTMS treatment and it is possible that there may have been some delayed response to medication. Given the open nature of the treatment, placebo responses are possible, and there is no control data. However, the response rate was consistent with other studies using a sham control condition.
In conclusion, this study adds to the small number of naturalistic studies of rTMS. In people with TR depression, ECT has advantages over rTMS in terms of both efficacy (Micallef-Trigona, 2014) and cost-effectiveness (Vallejo-Torres et al., 2015). Switching antidepressant medications appears to be comparable in efficacy to rTMS; however, rTMS is considered more cost-effective in this regard (Simpson et al., 2009). Considering also its safety and tolerability though, rTMS provides a beneficial treatment option for TR depression. However, further work is needed to define the place of rTMS in the management of depression. Nonetheless, the current study provides support for the growing literature on the effectiveness and usefulness of rTMS as a treatment option for depression in routine clinical practice.
Footnotes
Acknowledgements
The authors wish to acknowledge Ms Carol Turnbull (CEO, The Adelaide Clinic), Dr Tom Paterson (Psychiatrist), Ms Elizabeth Kaye (ECT/TMS Coordinator, The Adelaide Clinic) and the TMS Unit clinical staff.
Declaration of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.