
Abstract
Objective:
Many refugees experience prolonged separation from family members, which research suggests has adverse effects on mental health and post-displacement outcomes in refugee populations. We examine mental health differences in refugees separated and not separated from their families, and key post-migration factors and cultural mechanisms that may underlie this impact.
Methods:
A sample of 1085 refugees resettled in Australia, of which 23.3% were separated from all of their immediate family, took part in an online battery of survey measures indexing pre- and post-migration refugee experiences, mental health symptoms, disability and individualistic/collectivistic self-identity. Family separation was used as a predictor of mental health outcomes in a series of linear regressions, and the separated and non-separated groups were compared in multigroup path analysis models to examine group-specific indirect effects.
Results:
The separated group reported greater exposure to pre-migration potentially traumatic events and higher levels of post-migration living difficulties compared to the non-separated group. Family separation predicted higher post-traumatic stress and depression symptoms, but not disability, after controlling for potentially traumatic event exposure, age and sex. Path analyses revealed distinct indirect effects for separated and non-separated groups. Principally, higher collectivistic self-identity was associated with elevated post-traumatic stress, depression and disability symptoms via social-related post-migration living difficulties such as isolation and loneliness in the separated group; whereas collectivism was linked with increased depression symptoms via economic-related post-migration living difficulties in the non-separated group.
Conclusion:
These findings indicate that family separation powerfully influences mental health outcomes, but that its effect may be mediated by the type of post-migration stress experienced in the settlement environment and culturally bound differences in how the sense of self is interconnected with family.
Keywords
Families form the foundation of community, underpinning social cohesion by empowering individuals in their daily lives. As such, the experience of forced displacement and subsequent immigration policies that separate families can have an enormous impact on psychological health and wellbeing. In the context of forced displacement, family separation often occurs through the confused process of fleeing active conflict or leaving family members behind to seek asylum in the hope of eventual reunification (Oxfam and Refugee Council UK, 2018). Simultaneously, there is a global trend towards tougher policies around family reunification allowances for those seeking asylum in order to deter migrants and secure borders (Okhovat et al., 2017). Consequently, long-term family separation is a reality for many refugees. In Australia, refugees who are granted temporary protection visas because of their irregular mode of arrival (i.e. without a valid visa) currently have little chance for family reunification as they are either unable to sponsor family members to migrate to Australia or are blocked from travelling overseas without Government permission. Even with permanent residency, refugees frequently wait for years to be physically reunited with family members, with barriers including limited intakes, restricted definitions of ‘immediate family’ and prohibitive application costs (Okhovat et al., 2017). Australian policies are reflective of those now implemented in other countries, including the United Kingdom (Oxfam and Refugee Council UK, 2018). While there is substantial variation in the cause and experience of separation among refugees, it is clear that ongoing family separation has a negative impact on both mental health and settlement outcomes (Miller et al., 2018).
Studies have repeatedly demonstrated the adverse effect of family separation on the mental health of refugees. Alongside pre-migration trauma exposure, family separation has been associated with elevated depression, post-traumatic stress and anxiety symptoms (Chung et al., 2018; Miller et al., 2018; Nickerson et al., 2010; Rosseau et al., 2001; Savic et al., 2013; Schweitzer et al., 2006; Steel et al., 2002), increased disability (Nickerson et al., 2010) and reduced quality of life (Miller et al., 2018) among resettled refugee populations in Australia, the United States, Canada and Europe. Unresolved grief relating to missing family members can also have serious mental health repercussions (Miller et al., 2018). In addition, preoccupation with the safety of absent family members may interfere with the settlement of refugees, including engaging in productive tasks like acquiring language skills (Miller et al., 2018; Oxfam and Refugee Council UK, 2018).
Despite there being a clear negative effect of family separation on psychological health, trauma recovery and building a new life post-displacement, the mechanisms underlying the impact of family separation are still unclear. Themes arising from qualitative research provide hypotheses as to the underlying pathways. For instance, ongoing worry for separated family members may exacerbate risk for mental health symptoms (Kohrt et al., 2018; Miller et al., 2018; Nickerson et al., 2010; Savic et al., 2013; Oxfam and Refugee Council UK, 2018). Separation may have social or economic consequences, such as reduced support to buffer social stressors (Miller et al., 2018; Savic et al., 2013), and taking on unfamiliar roles in the family or increased financial burden (Oxfam and Refugee Council UK, 2018). Cultural factors may also be important. Many refugees are commonly from collectivistic cultural backgrounds (Hebbani et al., 2012; Jayawickreme et al., 2012). Collectivists hold a self-representation that is highly interconnected with their social environment – particularly their immediate and extended families (Cross et al., 2011; Liddell and Jobson, 2016; Markus and Kitayama, 2010). The implication of such a collectivistic self-representation is the high value placed on family cohesion, belonging and interdependence with others as central to self-identity. Qualitative studies have proposed this collectivistic perspective among refugees may heighten the impact of family separation on individual wellbeing (Miller et al., 2018; Savic et al., 2013).
While these themes have been suggested through previous research, quantitative studies have not yet measured the relative importance of these proposed factors in underpinning the impact of family separation on psychological health. Therefore, this study aimed to understand the relative contribution of these possible mechanisms to the mental health burden of family separation in a large cohort of refugees resettled in Australia. We first hypothesized that greater psychopathology – including depression and post-traumatic stress disorder (PTSD) symptomatology, and reduced functioning – would be observed in separated refugees compared to those with at least some immediate family with them. Moreover, it was predicted that family separation would be uniquely associated with elevated depression, PTSD and disability symptoms over and above other established predictors, such as exposure to potentially traumatic events (PTEs) and demographic factors. Second, we predicted that there would be different mechanisms underlying the relationship between pre-migration experiences and psychopathology in separated refugees compared to non-separated refugees. These mechanisms were hypothesized to included fear for family, social and economic post-migration living difficulties (PMLDs) and collectivistic self-identity.
Method
Participants
Participants were 1085 refugees resettled in Australia who entered the Refugee Adjustment Study (RAS) between May 2015 and January 2018. Inclusion criteria were that participants be refugees or asylum seekers who arrived in Australia after January 2011, be above the age of 18 years and be able to complete a survey in English, Arabic, Farsi or Tamil languages. Participants were screened on these criteria, and subsequently provided informed consent in accordance to approval from the University of New South Wales Human Research Ethics Committee. Participants were reimbursed with an AUD25 voucher for completing the survey. Two participants did not respond to the question on family separation, hence the final sample size for this study was N = 1083.
Study and recruitment procedure
The RAS is a cohort investigation of the mental health and settlement outcomes of refugees recently arrived in Australia. Participants were recruited into the RAS via advertising at refugee casework, counselling and support services across Australia, online advertising via social media to target language groups (e.g. Facebook) and snowball sampling methods where existing participants referred family or friends to the study. The majority of participants completed the survey online. Those without Internet access or poor computer literacy were given the option to complete the survey via pencil and paper sent in the mail (comprising 8% of sample). The survey took 45–60 minutes to complete.
Self-reported questionnaires
Measures were translated and blind back-translated from English into three languages – Arabic, Farsi and Tamil using gold-standard methods (Bracken and Barona, 1991). Minor discrepancies were resolved in consultation with community representatives, language, mental health and cultural experts.
Demographic variables assessed included age, sex, marital status, education, employment, visa status, physical health and family status. Family separation was indexed by a single item ‘What is your current family status?’ in relation to immediate family (i.e. parents, children, siblings, spouse), with response options being either no immediate family in Australia, some immediate family in Australia or all immediate family in Australia. We focused on separation from immediate family for this study, given cultural diversity in the importance of broader family links, and the lack of the nuclear family concept in many non-Western cultures participating in this study. For the purposes of this study, we computed a dichotomous variable to indicate whether respondents were currently separated from all of their immediate family vs had at least some (or all) of their immediate family with them in Australia (i.e. non-separated).
The Harvard Trauma Questionnaire (HTQ) was used to index lifetime exposure to 16 PTEs commonly reported by refugee populations including deprivation-related traumas, conflict, imprisonment, murder of family or friend, and torture (Mollica et al., 1992). An index of exposure to traumatic event type (experienced or witnessed) was computed for 15 items, as the PTE item ‘forced separation from family’ was excluded for the purposes of this study.
PTSD symptoms were measured by the 20-item Posttraumatic Diagnostic Scale for DSM-5 (PDS-5) which indexes current PTSD symptoms (Foa et al., 1997). Responses are given on a 0–3 scale (0 = not at all or only one time, 3 = five or more times are week/almost always). Mean scores were computed to index PTSD symptom severity. Internal consistency was strong (Cronbach’s α = 0.96).
Depression symptoms were measured by the Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001) – a brief nine-item measure of depression (DSM-5) severity widely used internationally with strong psychometric properties. Responses are provided on a 0–3 scale (0 = not at all, 3 = nearly every day) in response to the frequency of symptoms over the previous 2 weeks. To index depression symptom severity, responses for the nine items were averaged (Cronbach’s α = 0.93).
Daily functioning was measured by the 12-item World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0; WHO, n.d.), which indexes disability relating to daily activities over the past 30 days on a five-point scale ranging from (0 = none, 5 = extreme or cannot do). A total disability score was computed by summing all items (Cronbach’s α = 0.91).
The PMLDs checklist was used to index the current stressors experienced in the post-settlement environment (Silove et al., 1998; Steel et al., 1999), adapted to the current Australian migration context. The full scale used in the RAS comprised 36 items, indexing a range of social, economic, immigration, language, service access and fear-related difficulties commonly reported by refugees. Respondents were instructed to rate each living difficulty according to their experience over the previous 12 months on a five-point scale (1 = not a problem, 5 = a very serious problem). For the purposes of the current analysis, we computed indices reflecting PMLDs within four core domains: (1) social difficulties – comprising the mean of isolation, loneliness and discrimination items; (2) economic difficulties – comprising the mean of items measuring difficulties finding employment, appropriate housing and not having enough money to meet basic needs; (3) fear for one’s future – comprising mean of items regarding worry about ability to return home in an emergency or that visa status will not be resolved; and (4) fear for family – comprising items relating to worry about family at home or in immigration detention.
A shortened eight-item version of the Self-Construal Scale (SCS) was used to measure the levels of collectivistic or individualistic self-identity. The shortened version was created from the original 24-item version (Singelis, 1994), which was collected in a pilot sample of 55 resettled refugees in a separate study conducted in Sydney. Four items were selected to reflect individualistic self-identity and four to reflect collectivistic self-identity, based on inter-correlations and factor loadings in a confirmatory factor analysis (contact authors for details). Reponses are provided on a seven-point Likert-type scale (1 = strongly disagree, 7 = strongly agree). In the dataset used in the current study, internal consistency was satisfactory (collectivism: α = 0.74; individualism: α = 0.60).
Data analysis
We first examined group differences based on family separation on a number of key demographic, PTE exposure, PMLDs and mental health indices using non-parametric independent t-tests (Mann–Whitney’s U-test) or chi-square comparisons. A Bonferroni-adjusted significance threshold was used to control for multiple comparisons (p < 0.0016), and effect sizes (r estimate) were calculated. Linear regression analyses were subsequently conducted to test family separation group differences while controlling for PTE exposure, gender and age. These analyses were conducted in SPSS 25.
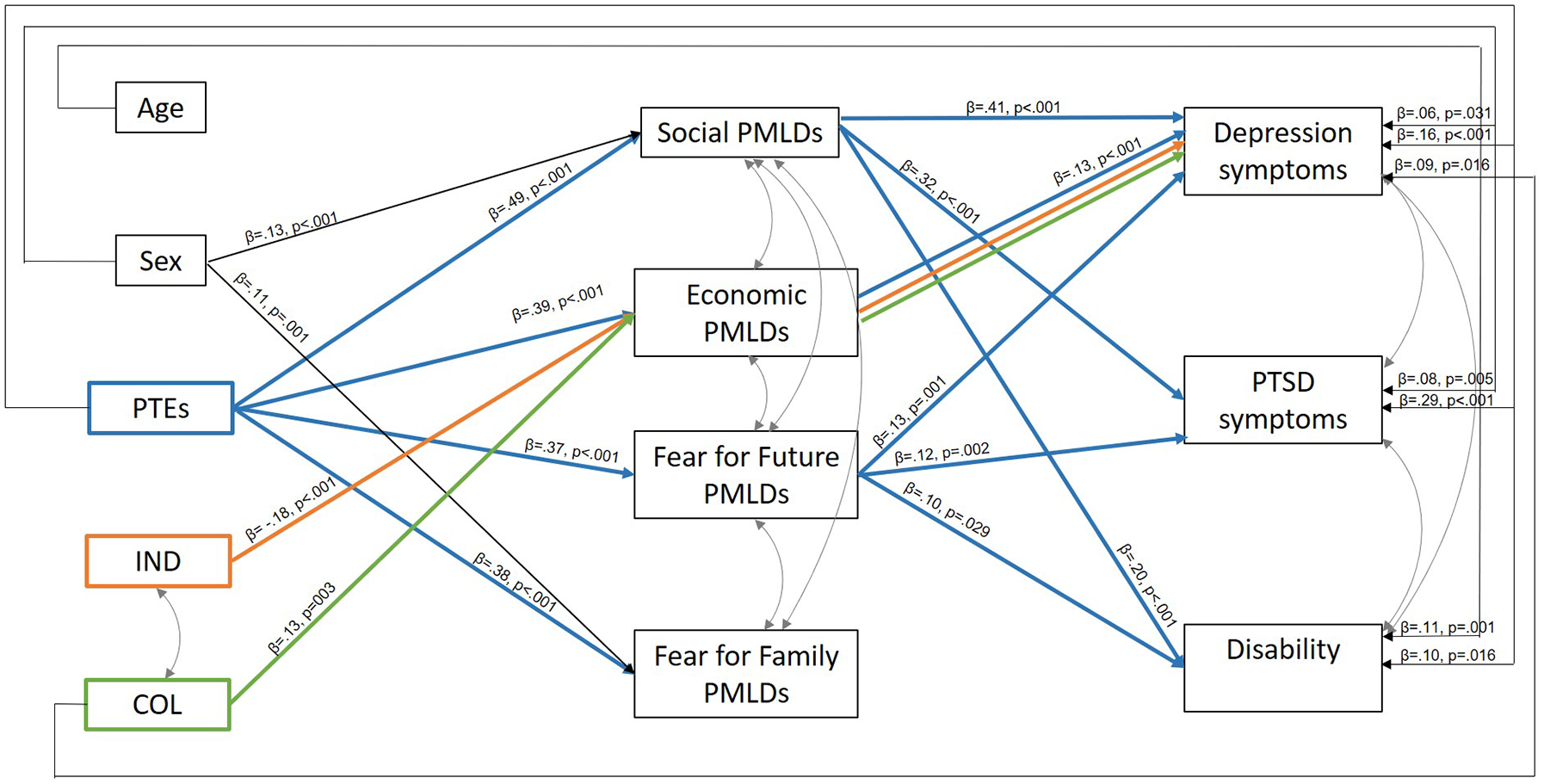
Second, we were interested in understanding the variables underpinning the impact of family separation on mental health outcomes. We conducted a multigroup path analysis which tests the moderating effects of a specified group variable (i.e. family separation) and allows us to examine differences in relationships between variables according to levels of the moderator (i.e. separated from family vs not separated from family). This is considered the preferred analytical approach to test for group differences in pathways (i.e. moderation; Little, 2013). The model tests both direct and indirect effects (i.e. mediating effects) between variables using maximum least likelihood estimates and was implemented in Mplus7 (Muthén and Muthén, 1998–2018). The following variables were entered into the model at each step: Step 1 – demographic, PTE exposure and both collectivistic and individualistic self-identity variables; Step 2 – four domains of PMLDs, including social, economic, fear for family and fear for future; Step 3 – mental health and functioning outcomes. The full theoretical model tested is presented in Figure 1. Although Cronbach’s alpha was lower for the individualism scale (but still in the acceptable range; Tabachnick and Fidell, 2001), we retained both collectivism and individualism sub-scales, given that self-construal is considered to be a continuous construct (Markus and Kitayama, 2010).
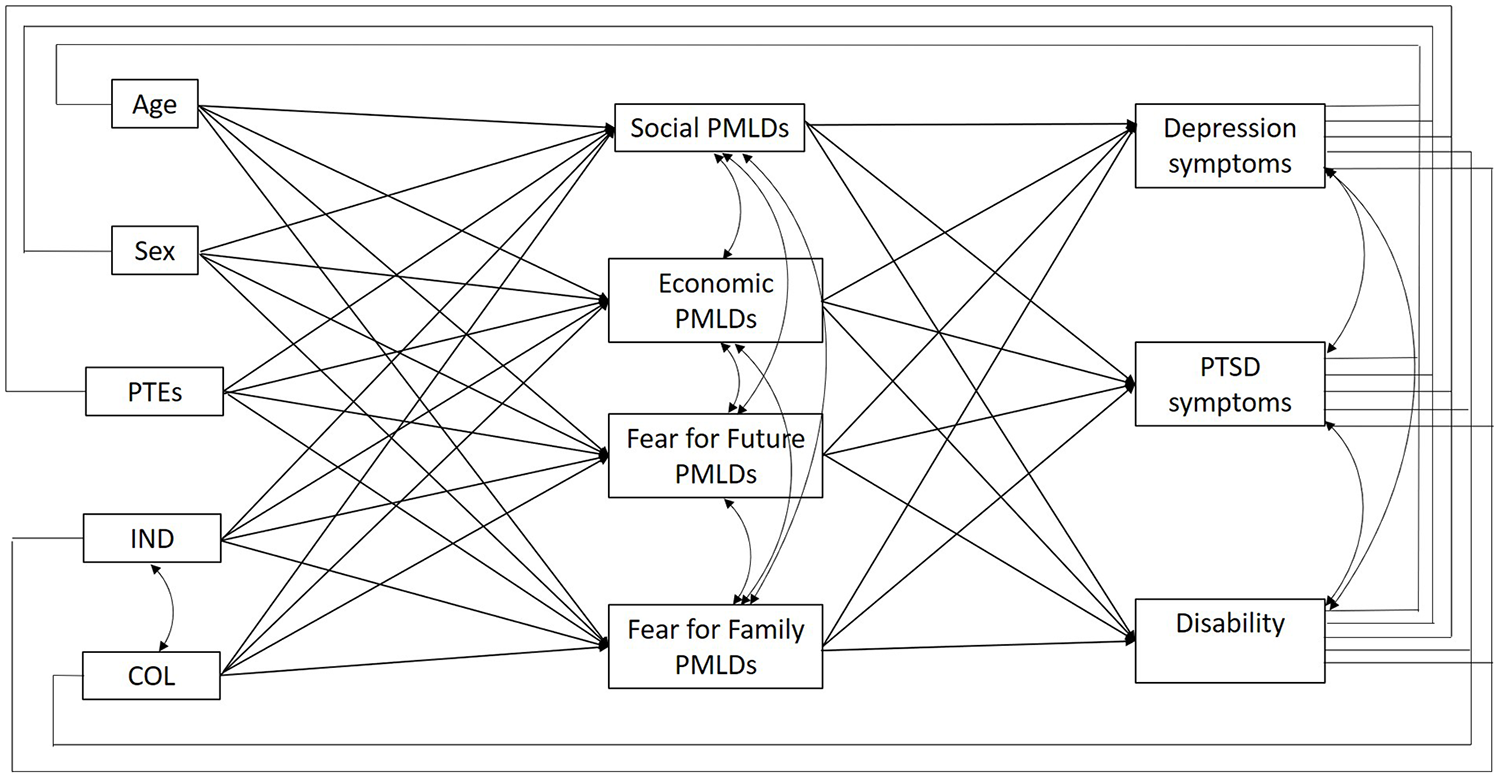
Theoretical model tested in path analysis.
In order to assess the validity of the model, a partially mediated model was tested where all paths were permitted to vary freely between groups. Next, a fully constrained model was tested whereby all paths were constrained to equality between groups. Evidence that the free model fit the data better was taken to indicate that the relationships between variables differed significantly across groups (p < 0.05). In the specified partially mediated model, first-step variables were allowed to influence second- and third-step variables, and second-step variables were allowed to influence third-step variables. Moreover, second- and third-step variables, as well as self-identity variables at the first step, were allowed to co-vary with one another. The key statistical indicators used to determine model fit were the chi-square test of model fit (p < 0.05), the comparative fit index (CFI) and Tucker–Lewis index (TLI; >0.9), the root mean square error of approximation (RMSEA; <1) and the standardized root mean square residual (SRMR; <0.05). Pathways, direct and indirect effects were significant at p < 0.05.
Results
Participant characteristics
Our participant sample of N = 1085 comprised refugees and asylum seekers who had arrived in Australia after January 2011 (mean length of time in Australia = 1.98 years; SD = 1.65). The largest proportion of participants were from Iraq (N = 589, 54.3%), followed by Iran (N = 174, 16%), Syria (N = 162, 14.9%), Sri Lanka (N = 58, 5.8%) and other countries (N = 102, 9.4%). The majority of participants were on some form of secure (permanent) visa (N = 826, 76.1%). A total of 23.2% (N = 251) reported being currently separated from all of their immediate family in Australia, whereas 76.8% (N = 832) reported having some or all of their immediate family in Australia.
Table 1 presents the group differences on key demographic, PMLDs and mental health variables, where several notable differences between the separated and the non-separated groups were observed. The separated group was more likely to be male, be younger, be Farsi-, Tamil- or English-speaking, be separated/divorced or single, be childless and have arrived in Australia by boat, compared to the non-separated group (Table 1). The separated group reported exposure to almost double the number of PTEs than the non-separated group and was more likely to have been exposed to each individual PTE. The severity of PMLDs in each domain was higher in the separated group. Depression and PTSD symptoms were also elevated in the separated group. No group differences were observed with regard to disability, or level of collectivistic/individualistic self-identity.
Participant characteristics.
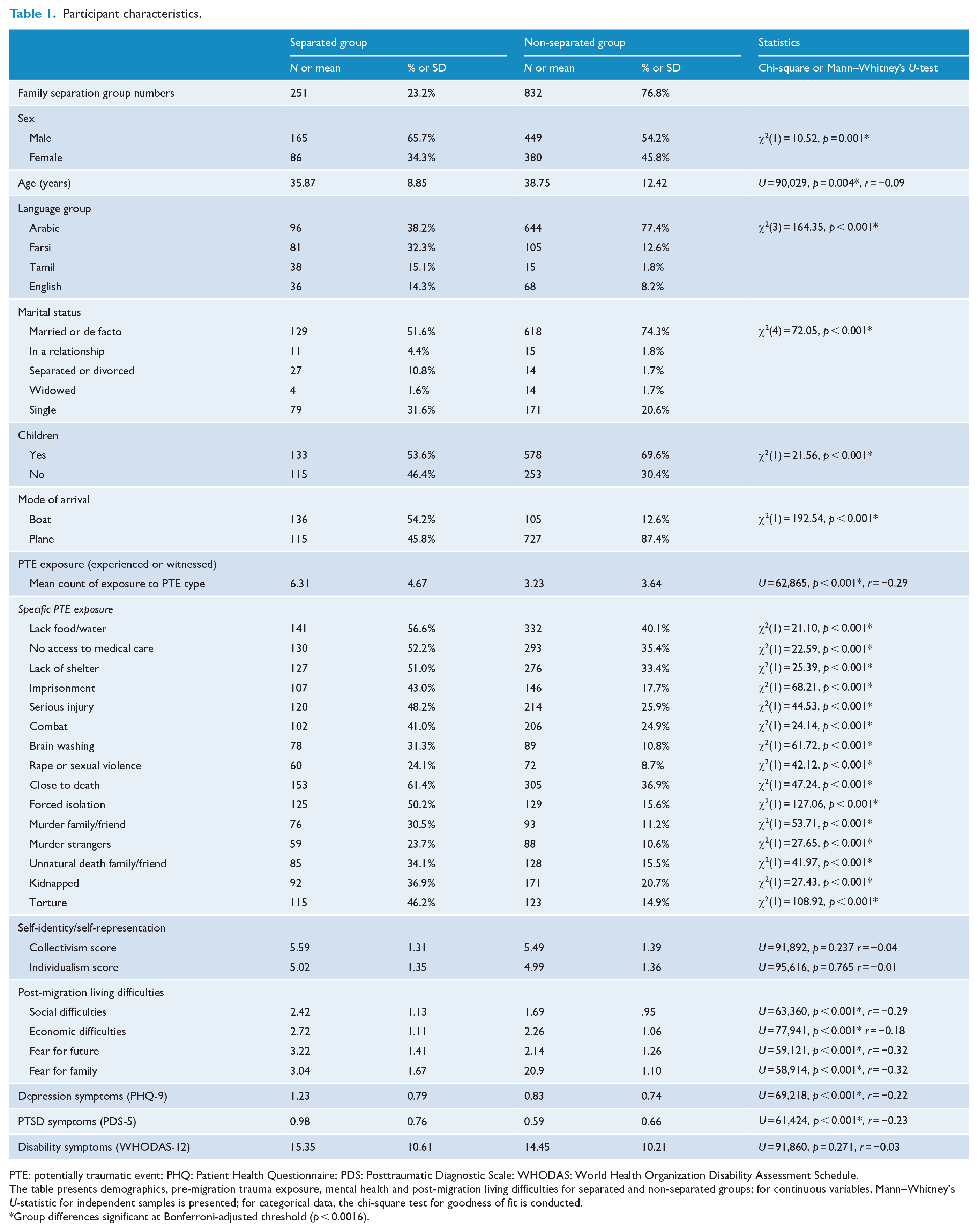
PTE: potentially traumatic event; PHQ: Patient Health Questionnaire; PDS: Posttraumatic Diagnostic Scale; WHODAS: World Health Organization Disability Assessment Schedule.
The table presents demographics, pre-migration trauma exposure, mental health and post-migration living difficulties for separated and non-separated groups; for continuous variables, Mann–Whitney’s U-statistic for independent samples is presented; for categorical data, the chi-square test for goodness of fit is conducted.
Group differences significant at Bonferroni-adjusted threshold (p < 0.0016).
The regression models testing group differences on mental health and disability outcomes while controlling for PTE exposure, age and sex are presented in Table 2. We found that family separation predicted increased PTSD symptoms, over and above the effects of PTE exposure, age and female gender, F(4, 998) = 117.86, p < 0.001, R2 = 0.32. Family separation also predicted elevated depression symptoms controlling for PTE exposure, age and female gender, F(4, 1035) = 77.799, p < 0.001, R2 = 0.23. However, family separation did not uniquely predict disability symptoms, F(4, 1027) = 21.241, p < 0.001, R2 = 0.08.
Linear Regressions Analyses predicting PTSD, depression and disability symptoms.
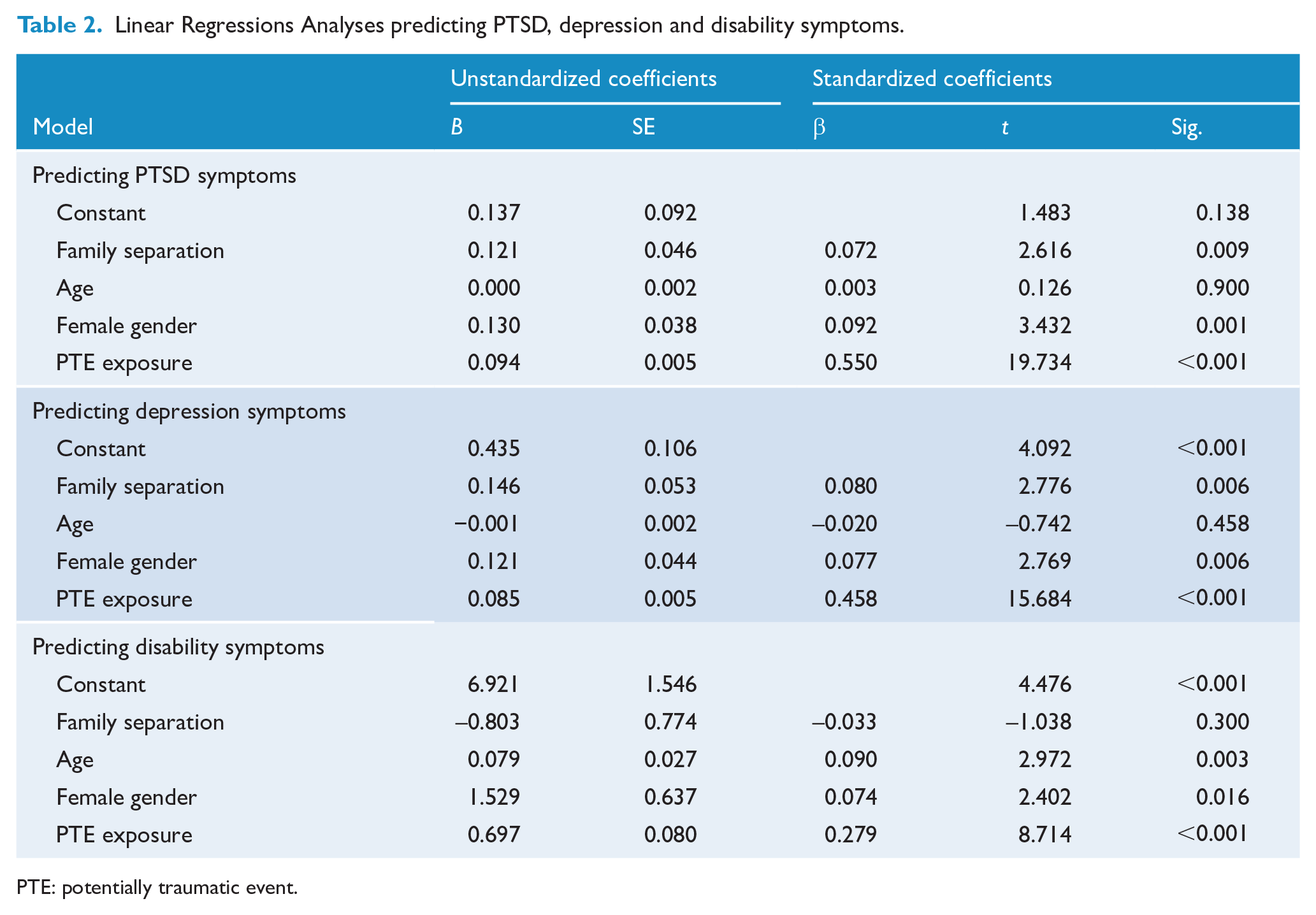
PTE: potentially traumatic event.
Path model
A multigroup path analysis model was specified that examined direct and indirect pathways between demographic, PTEs and collectivistic or individualistic self-identity, with depression, PTSD and disability symptoms via four domains of PMLDs. A multigroup approach enabled the significance of these pathways to be compared in the separated vs non-separated group. Due to missing data across these variables, the sample for the path analysis comprised N = 1061 participants, with N = 247 in the separated group and N = 814 in the non-separated group.
The multigroup path model showed evidence of good fit. The chi-square test of model fit was significant: χ2(12) = 38.962, p = 0.0001, CFI = 0.993, TLI = 0.934, RMSEA = 0.065, 90% CI = [0.043, 0.088], and SRMR = 0.023. This free model was compared to a fully constrained model, where the chi-square test of model fit was χ2(66) = 162.144 and p < 0.0001 that was significantly different from the free model (p < 0.001). This indicated that the models for the separated and not-separated groups in the free model were significantly different from one another.
Path analysis in the separated group
PTE exposure was directly related to depression (standardized coefficient [β] = 0.26, SE = 0.06, p < 0.001), PTSD (β = 0.40, SE = 0.05, p < 0.001) and disability (β = 0.20, SE = 0.07, p = 0.003) (Figure 2). The indirect effects of PTE exposure on depression were evident via social (β = 0.12, SE = 0.03, p < 0.001) and economic (β = 0.05, SE = 0.02, p = 0.023) PMLDs; on PTSD via social (β = 0.13, SE = 0.03, p < 0.001) and fear for the future (β = 0.06, SE = 0.03, p = 0.029) PMLDs; and on disability via social PMLDs (β = 0.08, SE = 0.03, p = 0.008).
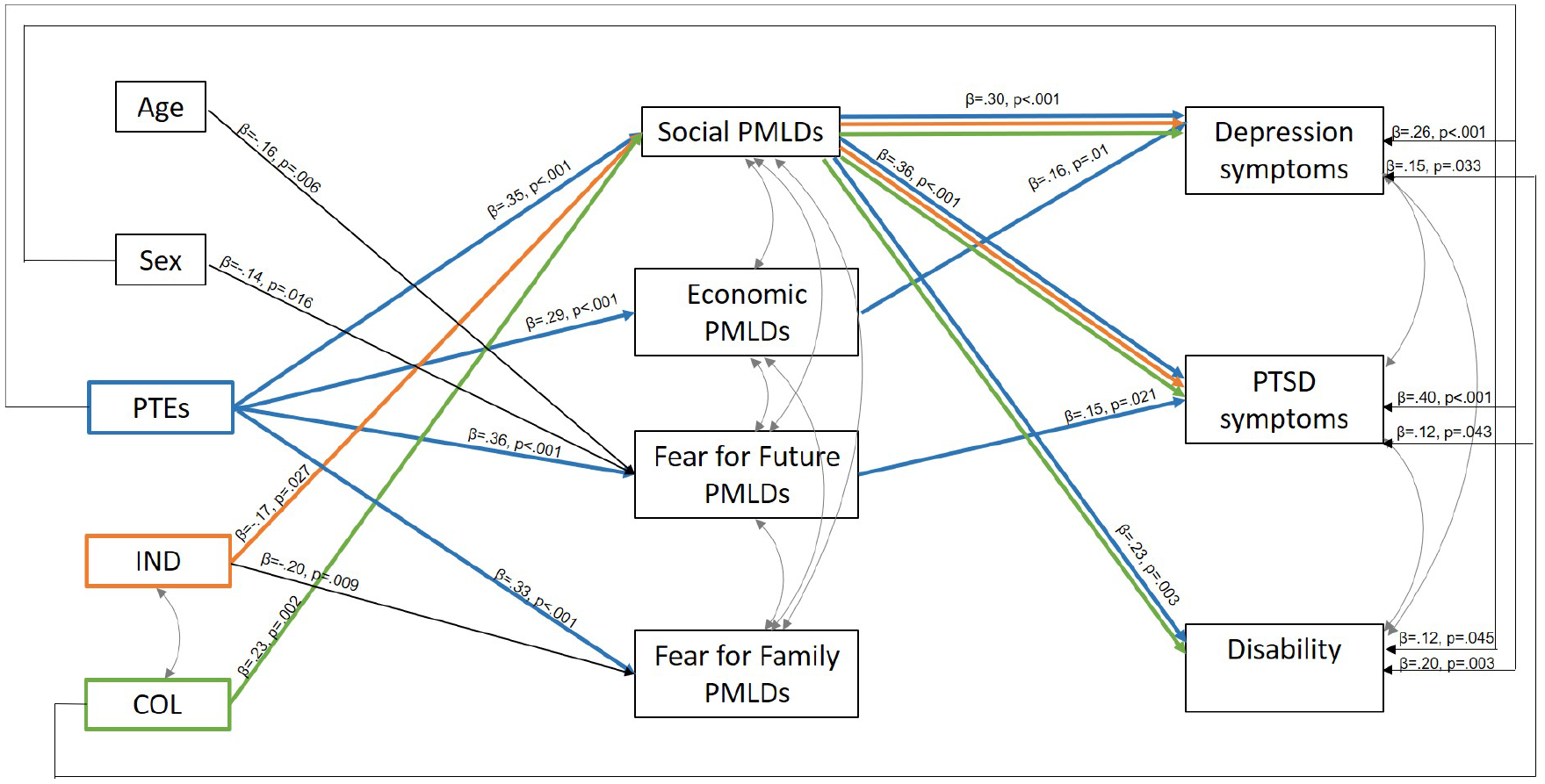
Significant pathways and indirect effects for the separated group.
Collectivism was also directly associated with elevated depression (β = 0.15, SE = 0.07, p = 0.033) and PTSD (β = 0.12, SE = 0.06, p = 0.043) symptoms. Moreover, higher levels of social PMLDs mediated the indirect effects between stronger collectivism and higher depression (β = 0.07, SE = 0.03, p = 0.011), PTSD (β = 0.08, SE = 0.03, p = 0.006) and disability (β = 0.05, SE = 0.03, p = 0.034) symptoms.
Individualism was not directly associated with mental health outcomes, but showed the inverse relationships observed with collectivism such that higher levels of individualism were associated with reduced depression (β = −0.05, SE = −.03, p = 0.048) and PTSD (β = −0.06, SE = 0.03, p = 0.039) symptoms via lower social PMLDs. Female sex was directly associated with elevated disability symptoms (β = 0.12, SE = 0.06, p = 0.045), while no direct effects with age were observed.
Path analysis in the non-separated group
Direct and indirect effects differentiated the non-separated group from the separated group (Figure 3). PTE exposure was directly associated with elevated depression (β = 0.16, SE = 0.03, p < 0.001), PTSD (β = 0.29, SE = 0.03, p < 0.001) and disability (β = 0.10, SE = 0.04, p = 0.016) symptoms. The indirect effects of PTE exposure on depression was observed via social (β = 0.20, SE = 0.02, p < 0.001), economic (β = 0.05, SE = 0.02, p = 0.001) and fear for the future (β = 0.05, SE = 0.01, p = 0.001) PMLDs; PTSD via social (β = 0.16, SE = 0.02, p < 0.001) and fear for the future (β = 0.04, SE = 0.02, p = 0.003) PMLDs; and disability via social (β = 0.10, SE = 0.02, p < 0.001) and fear for the future (β = 0.04, SE = 0.02, p = 0.032) PMLDs.
Significant pathways and indirect effects for the non-separated group.
Economic-related PMLDs mediated the indirect relationship between higher levels of collectivism (β = 0.02, SE = 0.01, p = 0.022) and lower levels of individualism (β = −0.02, SE = 0.01, p = 0.007) with depression symptoms in the non-separated cohort. Collectivism was also directly related to depression symptoms (β = 0.09, SE = 0.04, p = 0.016).
Female sex was directly related to depression (β = 0.06, SE = 0.03, p = 0.031) and PTSD (β = 0.08, SE = 0.03, p = 0.005), while older age was directly associated with elevated disability (β = 0.11, SE = 0.03, p = 0.001).
Discussion
This study examined the impact of family separation on the mental health and functioning of refugees settled in Australia. The findings revealed that refugees separated from their immediate family reported more PTE exposure, were experiencing higher levels of depression and PTSD symptoms (even when controlling for PTE exposure, age and sex) and reported elevated rates of PMLDs across multiple domains, compared to non-separated refugees. Critically, the path analysis model implicated cultural differences in self-identity as being an important factor driving the specific nature of the impact of family separation on the mental health of refugees. Significant indirect effects revealed that the association between collectivism and PTSD, depression and disability may be worsened in separated refugees via the impact on increased social-related PMLDs in the settlement environment. By contrast, higher collectivistic self-identity in non-separated refugees was related to increased depression symptoms via elevated economic-related pressures. Family separation appears to have a strong impact on mental health and functioning in resettled refugees, but its effect may be determined by cultural differences in self-identity and the specific post-migration stressors experienced.
Our finding that refugees separated from their families demonstrated higher PTSD and depression symptoms compared with non-separated refugees accords with previous research highlighting the negative impact of family separation on mental health in refugee groups (Chung et al., 2018; Miller et al., 2018; Nickerson et al., 2010; Rosseau et al., 2001; Savic et al., 2013; Schweitzer et al., 2006; Steel et al., 2002). The findings of the current study extend this work by demonstrating the adverse impact of family separation in a substantially larger sample comprising resettled refugees from diverse language groups. We also observed that refugees separated from their families reported greater exposure to PTEs overall, and across the range of individual PTEs, including torture, sexual violence and witnessing the murder of loved ones. This is consistent with other research showing greater trauma exposure in separated refugees (Miller et al., 2018). Higher degree of exposure to extreme pre-migration trauma may reflect the significant persecution and conflict-related push factors for individuals to seek asylum without their families. Alternatively, separation as a result of migration may have rendered individuals more vulnerable to trauma due to isolation.
A novel finding from this study was that cultural differences in self-identity differentially influenced mental health via different mechanistic pathways for those in the separated and non-separated groups. Specifically, in individuals separated from their families, higher levels of collectivism were linked to greater social stressors – marked by increased loneliness, isolation and the experience of discrimination, which negatively affected mental health and functioning. Stronger collectivistic self-representation refers to the perception of the self that is interdependent with others and is associated with a strong emphasis on family cohesion and relationality (Cross et al., 2011; Markus and Kitayama, 2010). Without immediate family to buffer the effects of such stressors, separated refugees with collectivistic self-identity may be particularly vulnerable to adverse mental health consequences. Such a finding is consistent with qualitative studies that point to collectivistic cultural expectations exacerbating the impact of family separation on refugees (Miller et al., 2018; Savic et al., 2013). We also observed the inverse relationship when considering individualism: higher levels of individualistic self-identity were associated with reduced mental health symptoms via decreased social stress in the separated group. Cultural models suggest that social environments that meet internal expectations result in less acculturative stress (i.e. if individualistic societies match an individualistic self-identity; Oyserman et al., 2014). If the sociocultural environment contradicts the active self-identity system of an individual, social stress may be increased and social regulation processes diminished without key social reference points (i.e. family members) to assist in navigating social stressors. Moreover, cultural research has also demonstrated that variations in individualism–collectivism self-identity affect cognitive appraisals of general and threatening situations (Bernadi et al., 2019; Krieg and Xu, 2018; Mesquita et al., 2016), with mental health consequences (De Vaus et al., 2017; Jobson, 2009; Liddell and Jobson, 2016). Considering how psychological and cultural mechanisms influence the impact of settlement policies on refugees may therefore be important (Nickerson et al., 2015), as well as how cultural differences may shape post-traumatic psychological symptoms depending on contextual factors like the experience of PMLDs (Jayawickreme et al., 2012; Jobson, 2009; Liddell and Jobson, 2016).
The path analysis findings highlight the direct association between PTE exposure and increasing risk for mental health symptoms in both separated and non-separated refugees, although these pathways were stronger in the separated group, thus supporting the majority of findings in the literature of such a dose–response relationship (Mollica et al., 1992; Steel et al., 2009). However, the quality of the post-migration environment is also important, demonstrating that the level of stress indirectly affected the association between PTE and mental health outcomes in both groups, according to epidemiological models highlighting the contribution of daily stressors to mental health in post-conflict settings (Miller and Rasmussen, 2010) and in displaced populations (Miller and Rasmussen, 2017; Steel et al., 1999). Social stressors appear to have a particularly powerful impact on wellbeing in refugees (Chen et al., 2017), especially isolation (Chen et al., 2017; Gorst-Unsworth and Goldenberg, 1998; Mollica et al., 2001) and discrimination (Correa-Velez et al., 2010; Ellis et al., 2008). While economic stress can increase feelings of helplessness in refugees (Porter and Haslam, 2005), our results showed a pattern by which collectivism was associated with depression via increased economic difficulties specifically in non-separated refugees. This may be that non-separated refugees with stronger collectivistic self-identities feel the additional burden of economic responsibility towards their present family members. Another potent stressor related to ongoing uncertainty relating to navigating the refugee status determination process (Procter et al., 2018) was related to PTSD symptoms in both groups, and depression symptoms in the non-separated groups. Unexpectedly, we did not observe fear for family directly or indirectly affecting mental health outcomes in either group – a factor previously highlighted as important in qualitative studies on family separation in refugees (Oxfam and Refugee Council UK, 2018). It may be that worry about immediate and extended family members remaining in situations of insecurity equally affect mental health outcomes in both separated and non-separated groups, although the separated group showed overall greater levels of such worries.
The strength of the study is its large sample, but the study did not implement representative sampling meaning that the findings may not be generalizable to all refugees resettled in Australia. The study is limited by its cross-sectional design, precluding analysis of the true mediation effects of post-migration living difficulty domains on mental health as a function of family separation. The relatively lower reliability of the individualism sub-scale of the SCS measure is also a limitation. In addition, the measurement of family separation was limited in this study. We focused on separation from immediate family, although separation from extended family may also adversely affect mental health in refugees which was not measured. We elected to treat the PTE event of ‘forced separation from family’ as a confound, because we did specifically measure how this item reflects current family separation for participants. We also did not measure the specific factors instigating the separation, the duration of the separation, from whom participants were separated from, nor the frequency of contact with separated family. These factors are likely relevant to the experience and impact of family separation on refugees that could be examined in future studies.
The findings of this study demonstrate the adverse effects of family separation on mental health in resettled refugees, and suggest that efforts to promote family reunification should be an important component of support provided to refugees at all stages of their migration journey.
Footnotes
Acknowledgements
The authors gratefully acknowledge the contribution of the participants in this study. They also acknowledge the contributions of Settlement Services International and the Australian Red Cross to this study and the special contributions of Rosanna Pajak and Susan Li to the conception and initial recruitment for this study. They wish to thank Amber Hamilton, Savannah Minihan, Candy Liu, Philippa Specker, Natalie Mastrogiovanni, Stephanie Murphy, Lillian Le, Joel Hoffman, Shraddha Kashyap, Ola Ahmed, Jessica Cheung, Miriam Den, Emma Doolan and Daniela Peiris for their assistance with participant engagement and recruitment for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the Australian Research Council (Grant No. LP160100670).