
Abstract
Australia accepted 12 349 humanitarian entrants in 2001–2002 and has accepted approximately 130 000 since 1990 [1], with an increasing number of refugees being accepted into Australia from African nations. A national longitudinal survey commissioned by the Department of Immigration, Multicultural and Indigenous Affairs (DIMIA) found that humanitarian entrants, such as refugees, experienced greater levels of stress and social difficulties than other migrant populations [2]. The research literature has also reported greater emotional distress among refugees, documenting high levels of posttraumatic stress, anxiety and depression and to a lesser extent other mental health issues such as psychosomatic disorders, grief-related disorders and crises of existential meaning [3, 4]. The emotional wellbeing of refugees appears to be influenced not only by pre-migration traumas and the post-migration adjustment experience but also by the biopsychosocial setting within which the participant exists [5–9]. The present study examines the psychological adjustment of a sample of 63 Sudanese refugees in Southeast Queensland over the year 2003 to determine the relative contributions of pre-migration trauma, social support and post-migration living difficulties in predicting mental health outcomes of refugees.
The roles of pre-migration trauma, post-migration living difficulties and social support in determining mental health
Before migration refugees are often exposed to human rights violations, torture and systematic violence. The traumatic experiences of refugees tend to be interrelated and generally cumulative, unlike single-event traumas [3]. These experiences can challenge their sense of empowerment, identity and meaning in life. A dose– response relationship has, with few exceptions [10], been found between trauma and the level of psychological stress among refugees, with increasing exposure to trauma associated with progressively greater psychological distress [9, 11, 12]. Steel et al. [9] found that participants reporting three or more trauma categories had an eightfold increase in risk of mental health illness and participants reporting one or more trauma categories had a twofold increase in risk compared to those who had experienced no exposure to trauma after 10 years of resettlement.
However, the long-term effect of trauma on mental health symptomatology is still debated. Evidence suggests that mental health symptoms improve over time for the majority but remain a significant risk factor for a minority in the long term [9,13–15]. Trauma may also have ongoing indirect effects by increasing the vulnerability of individuals to future stressors [16]. For example, a refugee who has experienced torture and has been able to pursue normal day-to-day functioning in the resettlement environment, may, when faced with acute stressors during resettlement develop symptoms of posttraumatic stress.
The relationship between trauma, coping strategies and outcome is complex. Silove [3] argues that trauma disrupts five broad systems: (i) personal safety; (ii) interpersonal attachments; (iii) sense of justice; (iv) identity or role; and (v) existential-meaning and that trauma can manifests in various psychosocial responses within these domains. Psychosocial factors impact on mental health by either increasing the vulnerability to, or protecting the individual from, the trauma and stressors of life. Psychosocial factors can include: social support, language proficiency, education, employment and world-view. Başoğlu and Paker [10] found that the impact of torture on mental health among political activists from Turkey was alleviated by factors such as social support and a high degree of expectancy for the trauma.
A person's self-concept and sense of meaning in life emerges from interactions and identification with family and cultural systems [17–20]. The refugee experience disrupts family and cultural systems and separation from the family and ethnic community. This is particularly so in the African context where there are large cultural differences with mainstream Australian culture that can challenge the sense of identity and belonging. The purpose or meaning of life is often built on a broad sense of identity and belonging. Trauma and the stressors of living in exile change the way of thinking not only of the past but also the present and future. They also challenge a person's belief in the world [3, 5, 17]. It has been argued that the inability to regain this sense of identity, agency and meaning in life can lead to feelings of aimlessness, helplessness and powerlessness [3]. Such feelings can manifest in poor social functioning and include symptoms of apathy, low energy, social withdrawal and impairment of daily roles such as parenting [12, 21]. Conceptualizing the mental health of refugees requires the recognition of the role of both pre-migration trauma and post-migration stressors and that psychological distress can manifest in various ways depending on the biopsychosocial context.
The present study
The present study examines the impact of resettlement on 63 Sudanese refugees in Southeast Queensland during the year 2003. Sudanese refugees might be considered an extreme group in terms of pre-migration traumas, many having lived through extreme hardships on the way to resettlement in another country. Sudan has been in civil war nearly continuously since independence from Britain in 1956. The civil war has been between the predominantly Islamic, Arabic north and a diversity of African ethnic groups in the south, mainly Christian or Animist [22]. Sudan is among the poorest countries in the world [23]. In the late 1980s and early 1990s an escalation in conflict, drought and the imposition of strict Islamic law and Arabic as the official language led to an increase in refugee movement. In 1993, it was estimated that nearly half a million Sudanese found refuge in other countries excluding the 1.3 million estimated to have died in the flight [22].
Refugees from Sudan are composed of numerous ethnic groups from the South as well as political refugees from the North. The Christian community while a minority in Sudan are disproportionately represented in the resettled populations globally. This community tends to be well educated and speak English as a second language. As many as 30 000 children and adolescents were separated from their families during flight to neighbouring countries in the late 1980s. Nowin early adulthood they also represent a significant proportion of the resettled refugees. Rudimentary Arabic is spoken by most Sudanese. Sudanese society is very patriarchal with clearly prescribed gender roles. Group and family cohesion is considered paramount. Reports of resettled Sudanese refugees emphasize that the refugees are extremely resilient and have high expectations for the future [22].
Since no studies have so far looked at the mental health of this group of refugees in Australia, an intention of this study was to present a profile of respondents in terms of mental wellbeing. Also, the impact of pre-migration trauma, post-migration living difficulties and social support was examined using multivariate methods. In regard to pre-migration trauma, post-migration living difficulties and social support, it was hypothesized that:
Hypothesis 1: Pre-migration trauma would be associated with increased rates of anxiety, depression, somatization and posttraumatic stress disorder (PTSD). Hypothesis 2: Post-migration living difficulties would be associated with increased rates of anxiety, depression, somatization and PTSD. Hypothesis 3: Social support would be associated with decreased rates of anxiety, depression, somatization and PTSD.
Method
Participants
The sample consisted of 63 humanitarian entrants, over 18 years of age, from Sudan. Participants immigrated via the Australian offshore humanitarian program. The humanitarian program includes three categories: (i) refugee and women at risk (experienced or fear of persecution); (ii) special humanitarian (experienced gross discrimination); and (iii) special assistance. The latter category includes specific groups of people in vulnerable situations who have community links in Australia. The Sudanese are able to apply under this category. Participants were recruited via snowball sampling: that is, two bilingual community liaison workers (one male, one female), who had strong links with the Sudanese refugee community, identified potential participants and approached them to participate in the study. The community workers also invited participants to nominate further potential participants.
Measures
Demographic and social characteristics
Information was collected on the demographic and social characteristics and migration history of each participant. Variables included: age, country of origin, religious background, dates leaving home country and arriving in Australia, level of education, occupation, English language skills, financial situation and social support. For the social support variables, participants were asked to rate the degree of support they received from: (i) members of their own ethnic group; and (ii) the broader community. To avoid small cell sizes these variables were later collapsed to form two categories – people who felt they received support (coded 1), and people who felt they received little or none (coded 0).
The Harvard Trauma Questionnaire (HTQ)
The HTQ includes two sections: a record of traumatic events experienced or witnessed and a posttraumatic stress symptom scale. The first section documents 16 common trauma events experienced by refugees, which range from ‘lack of food and water’ to ‘torture’. Participants were asked to indicate whether they had ‘experienced’ or ‘witnessed’ any of the events personally. In addition, this study asked whether any of these events were ‘experienced’ or ‘witnessed’ by family members. Each participant was given a cumulative score by adding up the events reported ‘experienced’ or in the case of the murder or unnatural death of family, friends or strangers ‘experienced’ or ‘witnessed’ [16].
The posttraumatic stress symptom section of the HTQ consists of 16 items reflecting PTSD criteria from the DSM-III (American Psychiatric Association, 1987). Each participant is asked whether they experienced these symptoms during the preceding week on a scale from 1 to 4 (‘not at all’, ‘a little’, ‘quite a bit’ and ‘extremely’). A symptom severity rating is derived by summating scores on the 16 items [24]. More recently, a DSM-IV algorithm has been developed by Mollica et al. to reflect probable caseness of PTSD[5, 25] with that method being applied across a number of cultural groups [26, 27]. In this study the HTQ was found to have an internal reliability of 0.87 (Cronbach's alpha).
Hopkins Symptom Checklist (HSCL-37)
The participant's overall wellbeing was assessed using the HSCL-37. This scale is an extended version of the HSCL-25 that has been validated on a general American population [28] with Indochinese versions being translated and validated by Mollica et al. [24]. Reviews have attested to the transcultural robustness of the measure and its appropriateness when applied to refugee populations [29–31]. The HSCL-37 measures symptomology over the week preceding the interview and includes 10 anxiety items; 15 depression items; and 12 somatization items scored on a four-point ordinal severity scale (‘not at all’, ‘a little’, ‘quite a bit’, ‘extremely’). An arithmetic mean for each subscale was calculated for each participant, the higher the mean the higher the level of psychological distress. An index of caseness based on the depression scale can be assessed using the procedures developed by Mollica et al. [25]. The internal reliability of the HSCL scales in the present study was 0.83 for anxiety, 0.89 for depression and 0.82 for somatization (Cronbach's alpha).
Post-migration Living Difficulties (PMLD)
The PMLD checklist was used to assess the levels of stress due to typical post-migration stressors developed from discussions with immigrant and refugee communities in Sydney [7, 9]. The checklist was shortened to seven items for the purposes of the present study covering several broad areas: communication, discrimination, worry about family back home, employment, immigration difficulties, access to health and welfare services and acculturation difficulties. The checklist asks respondents to rate their experience of the problems, during the last 12 months, on a five-point scale (‘was not a problem’ to ‘a very serious problem’). A high cumulative score indicates a high degree of postmigration stressors.
Procedure
A protocol comprising five questionnaires was administered through a structured interview process. The interview took approximately 60 minutes andwas conducted in Arabic, through the use of the bilingual assistant in English. The bilingual assistant translated the questions, in vivo, from the questionnaires written in English. Before the interview the participants were read the letter of information and the informed consent form in Arabic or English. Each participant was informed of the voluntary nature of the study, their right to withdraw at any time and the confidentiality of their responses. The participants were informed of their entitlement to contact a specialized counselling service for survivors of torture and trauma (Queensland Program of Assistance for Survivors of Torture and Trauma) for counselling at no cost.
Statistical analysis
The relationship between possible predictor variables and the four symptommeasures (HSCL depression, anxiety and somatization scores and HTQ posttraumatic stress scores)was investigated using group-wise hierarchical regression models reflecting the chronological nature of the refugee experience. For each symptom measure, the demographic variables age and gender were entered at step 1. At step 2, pre-migration variables were entered including the number of categories of trauma experienced personally or by immediate family members and the number of years is spent in transit before resettlement to Australia. At step 3, post-migration predictors were entered including the number of years of residence in Australia, whether the respondent was settled as part of an intact family group, two social support variables (social support from the ethnic community, and social support from the wider community), employment status, and the number of post-migration living difficulties endorsed. Only those variables significant at each step were included in subsequent steps.
All data were evaluated for the assumptions of regression. To avoid small cell numbers, a number of variables were collapsed into dichotomous variables for the regression analysis. These included: length of residency with a 60:40% split (0=less than 2 years, 1=2 years or more) and family status, dichotomized into those participants with intact family attachments (intact, coded 0) and participants without intact family attachments, single or one parent household (not intact, coded 1) with a 49:51% split. This categorization is similar to that used by Beiser [13]. To improve pairwise linearity and to reduce the skew the Hopkins Symptom Checklist and Harvard Trauma scales were subjected to a log-10 transformation.
Results
Participant profile
The sample consisted of a total of 63 participants, 21 female and 42 male, representing approximately 6.7% of the Sudanese population in Queensland [1]. The social and demographic characteristics of the participants are summarized in Table 1. The mean age was 34.2 (SD=8.5) years. In the present sample 49% had intact family attachments while 51% were without intact family attachments (single or in one parent households). These demographics broadly reflect DIMIA settlement statistics for Sudanese in Queensland [1]. The majority of participants (83%) were fluent in English or reported only some difficulty with English, 46% had completed secondary school and another 30% higher qualifications. Before arriving in Australia, 37% were in business, managerial or professional (and para-professional) professions however since arriving in Australia 76% were unemployed or not in the work force. Eighty-seven per cent were Christian and the remaining 13% of Muslim faith consistent with global Sudanese refugee figures [22]. For the social support variables, 62% of the sample reported having received support from their ethnic community, and 43% felt that they had received social support from the broader community.
Sample characteristics Sudanese refugees (n=63)
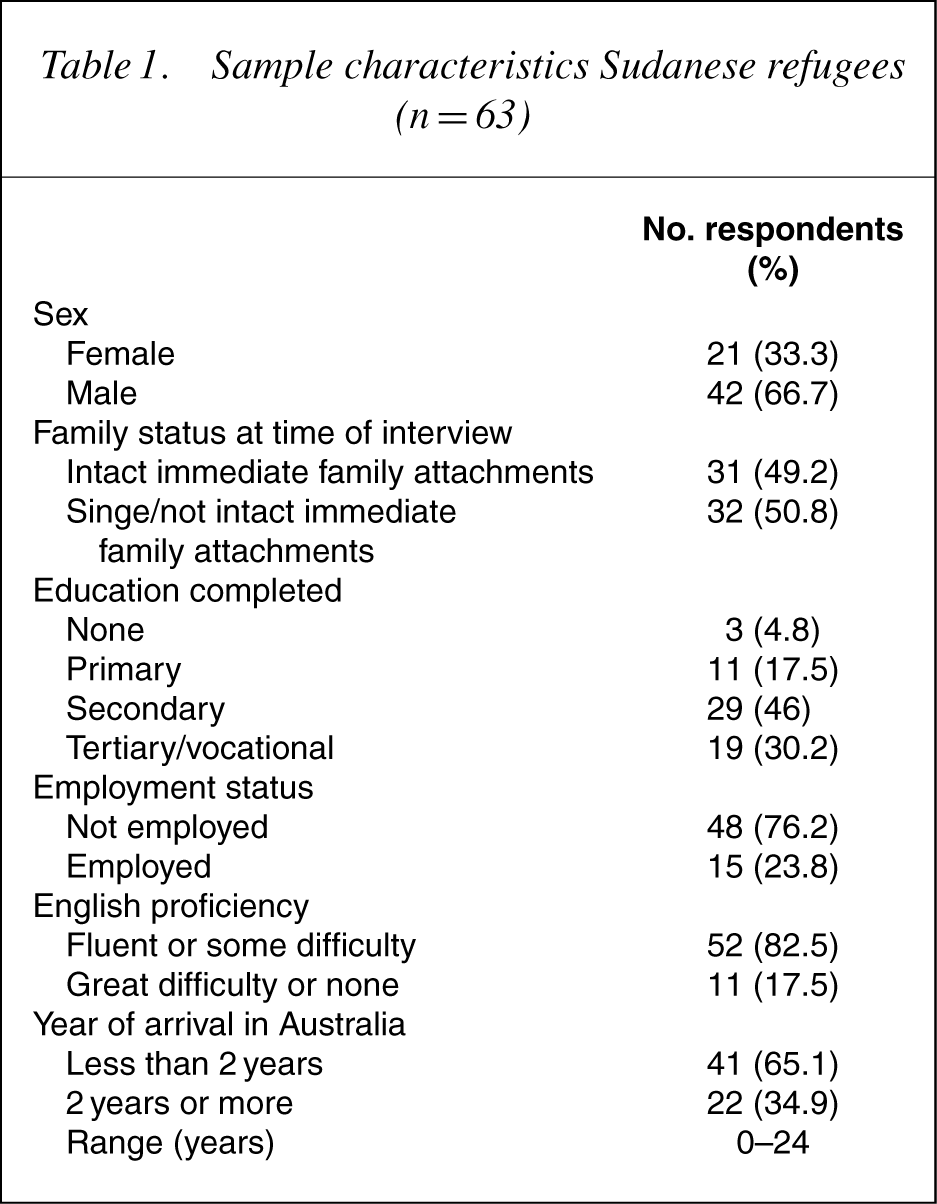
The average length of residency in Australia was less than 2 years. All participants fled from Sudan to Egypt and refugee camps in Kenya and Uganda. The period of transit was, on average, 7 (SD=4.46) years.
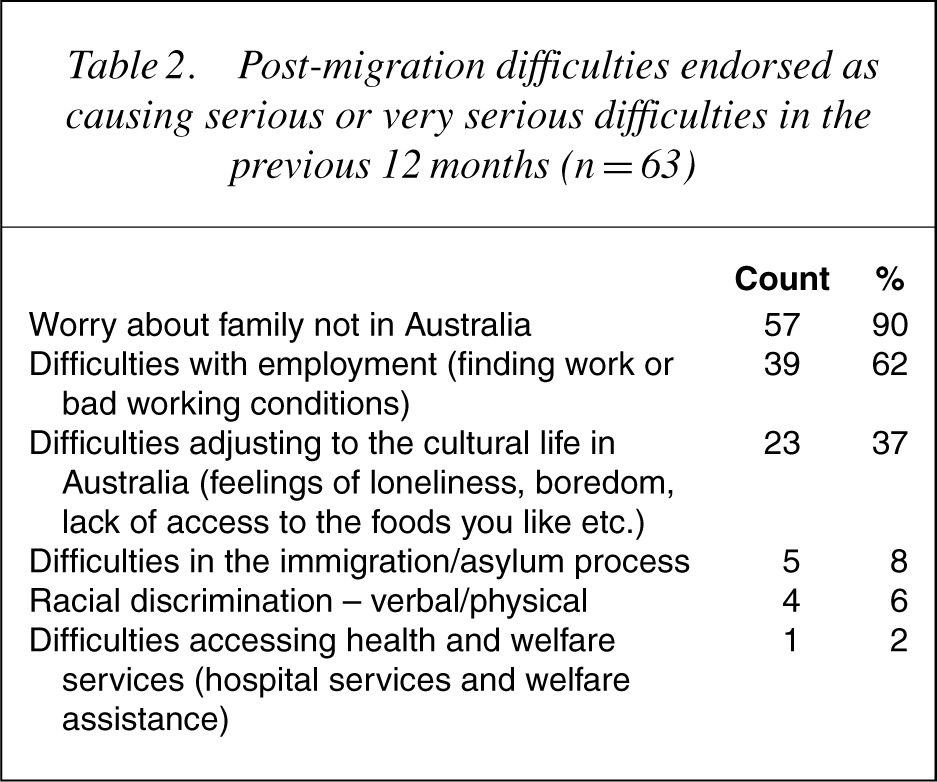
Table 2 presents the number of post-migration living difficulties endorsed as causing moderate to severe problems in the previous 12 months or at the time of interview. Worry about family back home (95%), employment opportunities (82.5%) and acculturation difficulties (73%) were the most commonly reported post-migration stressors. All participants migrated to Australia under official humanitarian programs and reported no difficulties with migration officials in the past 12 months. Twelve participants reported having experienced some degree of verbal or physical racial discrimination.
Post-migration difficulties endorsed as causing serious or very serious difficulties in the previous 12 months (n=63)
Ninety-five per cent of participants reported receiving some support from the Sudanese community on their arrival in Australia and 62% reported knowing someone in Brisbane before arrival, often extended family or someone from the refugee camps.
Trauma events
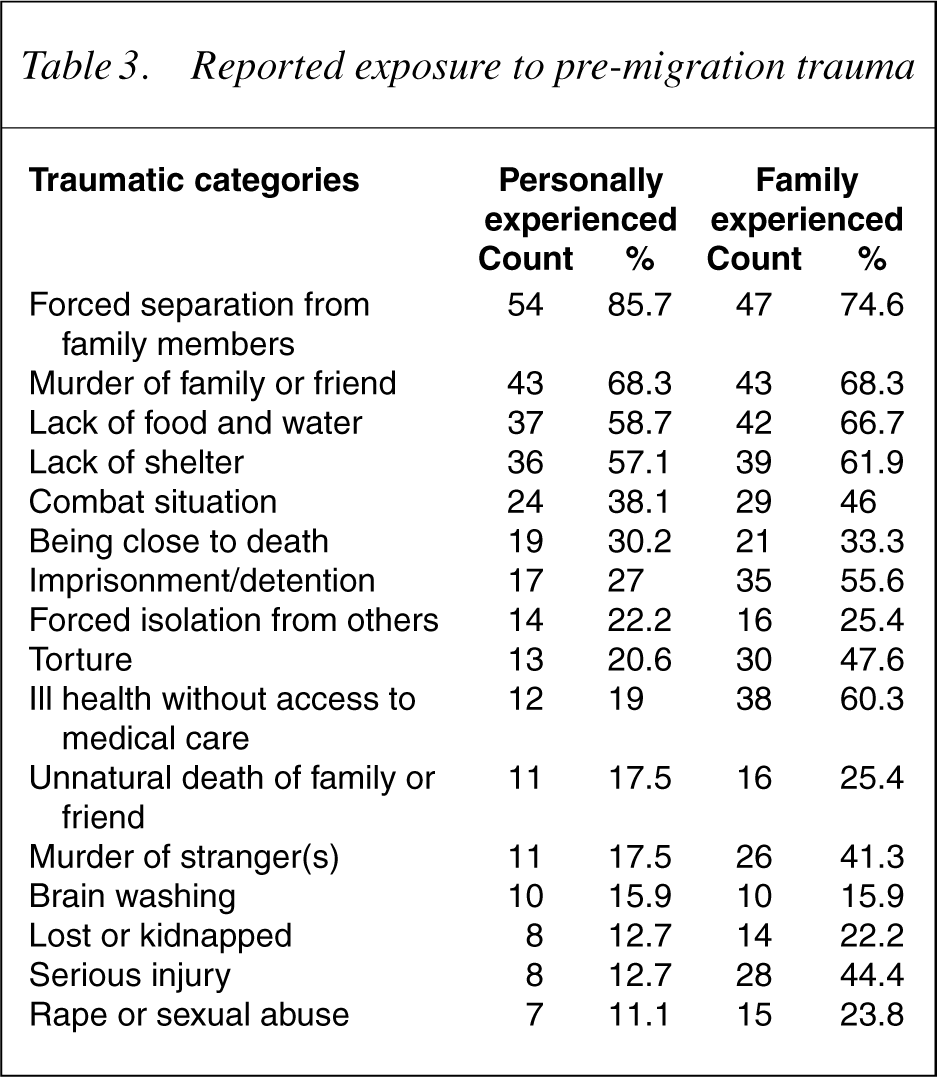
All of the participants reported experiencing at least one of the 16 categories of trauma assessed by the Harvard Trauma Questionnaire (Table 3). The mean number of types of trauma directly experiencedwas 5.6 (SD=4). Fifty-four per cent of the sample reported experiencing five or more categories of trauma and 12 participants (19%) reported experiencing 10 or more categories of trauma. The most frequently cited trauma experiences included: separation from family (85%), the murder of family or friend (68%), lack of food and water (59%) or shelter (57%). Torture was experienced by 13 participants (28%) and seven reported rape or sexual abuse (four females and three males for a total of 11%). All participants reported that their families had also experienced trauma. About half of the participants reported that a close family member had been imprisoned (56%) or tortured (48%).
Reported exposure to pre-migration trauma
Mental health: depression, anxiety, somatization and posttraumatic stress
The mean scores for the Hopkins anxiety, depression and somatization subscales were 1.48 (SD=0.44), 1.64 (SD=0.53) and 1.51 (SD=0.42), respectively on a scale of 1–4. These mean scores are comparable to those reported in research with other refugee groups [32]. Application of the DSM-IV scoring algorithm developed by Mollica et al. identified 10 (16%) participants as suffering from a major depressive disorder.
The mean posttraumatic stress symptom score on the HTQ was 1.62 (SD=0.46). Of the posttraumatic stress symptomatology experienced in the last week, 84% of the sample had experienced recurrent thoughts or memories of the most hurtful events, 62% had experienced recurrent nightmares, 59% reported trouble sleeping, and 71% reported avoiding thoughts and feelings associated with those traumatic events they had experienced. There was a highly significant, positive correlation between the posttraumatic stress score with pre-migration trauma (r=0.66, p<0.0001). Eight participants (13%) were classified as cases of PTSD based on application of DSM-IV criteria to the HTQ symptom scale.
Predictors of mental health
Table 4 displays correlations between the variables used to construct the multivariate models. Predictors included participant demographics of gender and age, pre-migration and post-migration experiences and the criteria were four indices of mental health, namely depression, anxiety, somatization and posttraumatic stress. The models are presented in Table 5.
Correlations among variables in the analysis
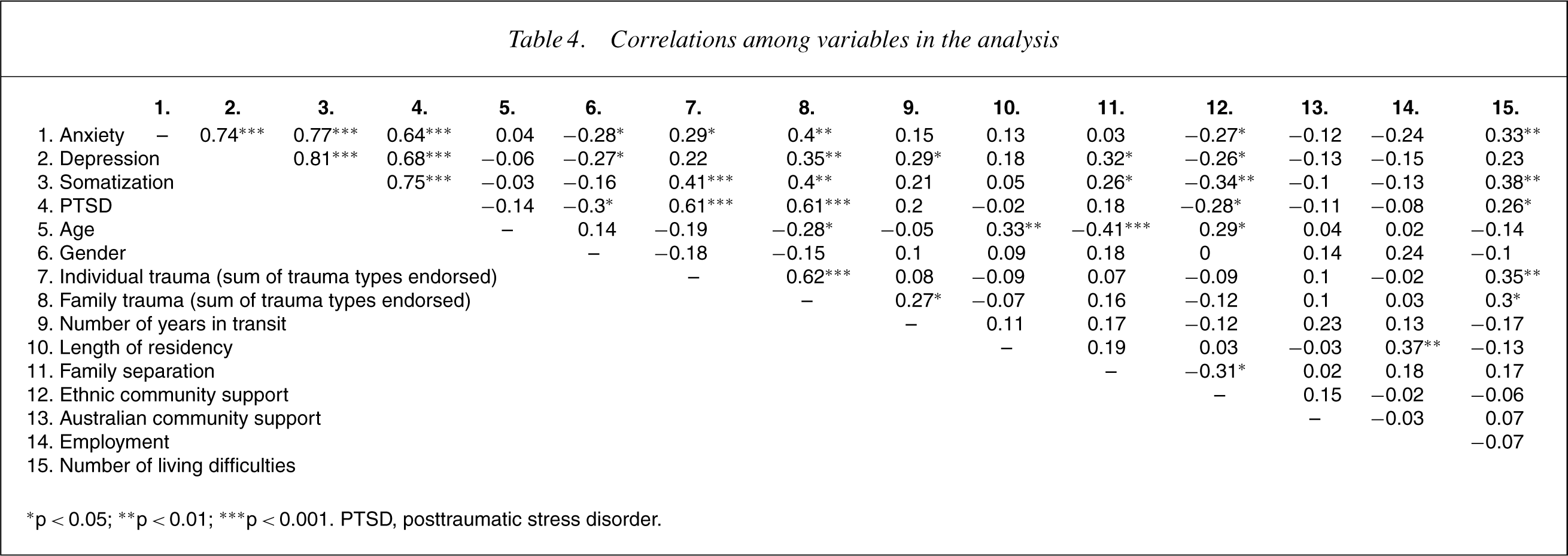
∗p< 0.05; ∗∗ p< 0.01; ∗∗∗ p< 0.001. PTSD, posttraumatic stress disorder.
Group-wise hierarchical multiple univariate regression models for depression, anxiety, somatization and posttraumatic stress (PTSD) symptom scores (n=63)
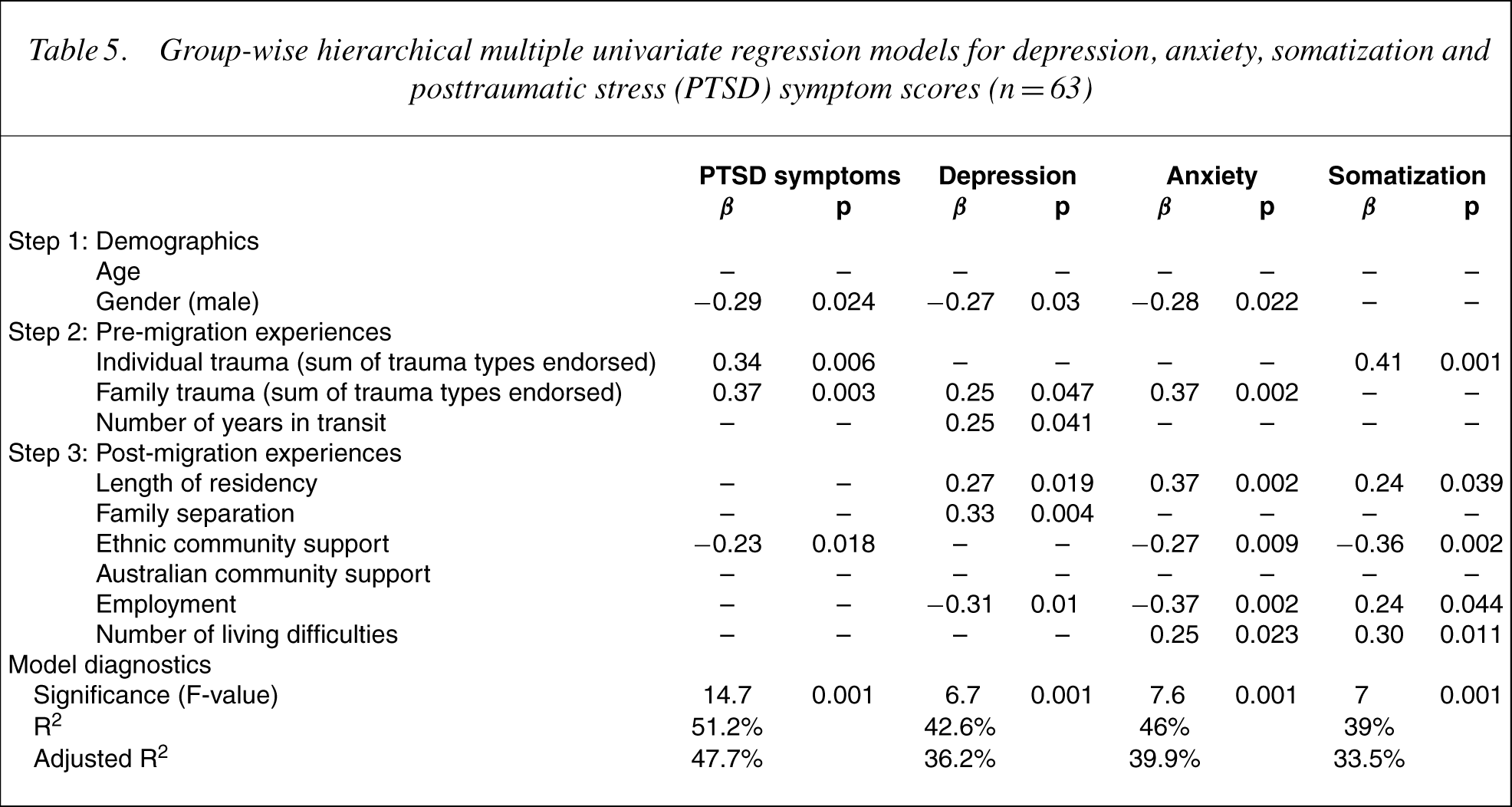
In a model predicting PTSD symptomatology, the demographic variable of gender was significant at step 1. Females in this sample experienced greater PTSD symptomatology than did males (Table 5). After accounting for this variable, trauma experienced by the individual, and trauma experienced by family were both significant predictors, while number of years spent in transit was not. In step 3, social support from the individual's own ethnic community was a significant predictor. The overall model was significant (R2 =0.51, adjusted R2 =0.47).
In the model predicting depression, gender was significant in step 1 with women overall experiencing greater depressive symptomatology than men. Trauma experienced by family members and number of years in transit both significantly predicted depression in step 2. In step 3, adjusting for preceding variables, length of residency, family separation and employment status were also significant predictors of depression. Surprisingly, individuals appeared to show greater levels of depression with longer periods of residency in Australia. Again the model was significant (R2 =0.43, adjusted R2 =0.362).
In the model predicting anxiety, again gender was the only significant demographic variable, females experiencing greater anxiety than males. At step 2, trauma experienced by family members significantly predicted anxiety. At step 3, significant predictors were length of residency, social support from the ethnic community, employment status and post-migration living difficulties. Again, longer periods of residency tended to be associated with greater anxiety symptoms. The overall model was significant (R2 =0.46, adjusted R2 =0.399).
For the model predicting somatization symptoms, neither age nor gender were significant at step 1. At step 2, only traumas directly experienced by the individual significantly predicted somatization. At step 3, the significant predictors were length of residency, support from the ethnic community, employment status and post-migration living difficulties. Once again longer periods of residency tended to be associated with greater somatization problems. The model was significant (R2 =0.39, adjusted R2 =0.335).
Discussion
The aims of the present study were twofold. To present a profile of Sudanese refugees in Southeast Queensland, in terms of the level and range of traumas they have experienced, and their current psychosocial functioning. The second aim was to test the combined influence of pre-migration trauma, post-migration living difficulties and social support, in determining mental wellbeing.
From the above data, it is evident that the Sudanese sample investigated in this study experienced a number of pre-migration traumas. Specifically, the vast majority of refugees reported being separated from their families, experiencing violence, witnessing murder of family or friends and being deprived of basic needs. Loss of significant loved ones in the migration process and social isolation in exile were also common. Traumatic experiences such as rape or sexual abuse, brain washing, being kidnapped and being isolated from others were reported by approximately a quarter of the refugees in this study.
These traumatic experiences are problematic as they may well be associated with increased vulnerability that combined with psychological stress result in poor adjustment. Indeed, the multivariate data identified premigration trauma as a significant predictor of mental wellbeing in each symptom domain examined. Not surprisingly, the effect of trauma has differential impact on different areas of functioning. Trauma experienced by the individual appears to directly predict PTSD symptomatology and also somatization problems. Trauma experienced by family members directly predicts levels of depression and anxiety in this sample. Females also experienced more mental health problems than males.
Although trauma was a significant predictor of mental health in the present study, post-migration experiences were also of importance in predicting psychological wellbeing. Post-migration experiences comprise both difficulties and levels of social support. With regard to post-migration difficulties, the most common items endorsed by refugees in the present study referred to concerns about family not living in Australia, difficulties in employment, and difficulties adjusting to cultural life in Australia. Such living difficulties were associated with increased depression, anxiety and somatization. However, social support variables were of particular salience in determining psychological wellbeing in the present study. Specifically, the presence of family, and social support from others within the Sudanese community, are significant determinants of mental health functioning, while social support from the wider community is not. It has been remarked elsewhere that frameworks of social support may differ widely between different communities [18, 33, 34]. From informal discussion with respondents, Sudanese cultural life is based largely around the extended family, and social groups form an important source of support, both emotional and instrumental. The loss of this sense of emotional and instrumental support may be an ongoing trauma to emigrants isolated in exile.
With regard to the influence of length of residency on mental health outcomes, there is a trend toward poorer mental health outcomes over time in this sample. Although previous studies [9] have found improvements in mental health outcomes over time, few longitudinal studies have been conducted, and so the implications of these cross-sectional data are unclear. If mental health does deteriorate over time for Sudanese adults in Australia, this may be an area of considerable concern. Experiences of living in the post-exile community may compound, rather than alleviate, mental health problems associated with migration and the refugee experience [7]. In terms of post-migration difficulties, the vast majority of this sample reported ongoing problems with employment and difficulties with acculturation. Although this group has by and large arrived in Australia only recently, it is a matter of concern that problems associated with employment and acculturation are so prevalent. It is possible that the relationship between length of residency and mental health in this sample may result from cohort effects – for instance, migrants seeking refuge during periods of greater or lesser social upheaval. This can only be properly investigated using a prospective design to determine the kinds of psychological changes that occur in the postexile community over time.
These findings form part of an emerging research literature examining refugee mental health issues in the Australian context. In this regard, it is interesting to note that refugees experience higher level of psychological distress when compared to general Australian community samples [2]. However, the rates of probable mental illness observed in the present study were generally comparable to those observed among other refugee populations [32]. For example, Table 6 compares the mental health of this sample of Sudanese refugees and a sample of Tamil refugees resettled in Australia [32]. This table shows the similarity in mean mental health symptoms between the two groups. However, in terms of clinical caseness, the rates of PTSD (16%) in the present study are significantly lower than that the 35% reported in Steel's [4] weighted meta-analysis examining a diverse range of refugee populations. Rates of depression were also slightly lower (13% in the present study compared to 14.6% in Steel's meta-analyses). These findings are not surprising given the lower levels of reported traumatic events reported by this population compared to those reported in other refugee populations such as Tamil refugees [32], Bosnian survivors of trauma [25] and Cambodian refugees [12].
Comparison of the mental health profiles: Sudanese and Tamil samples†
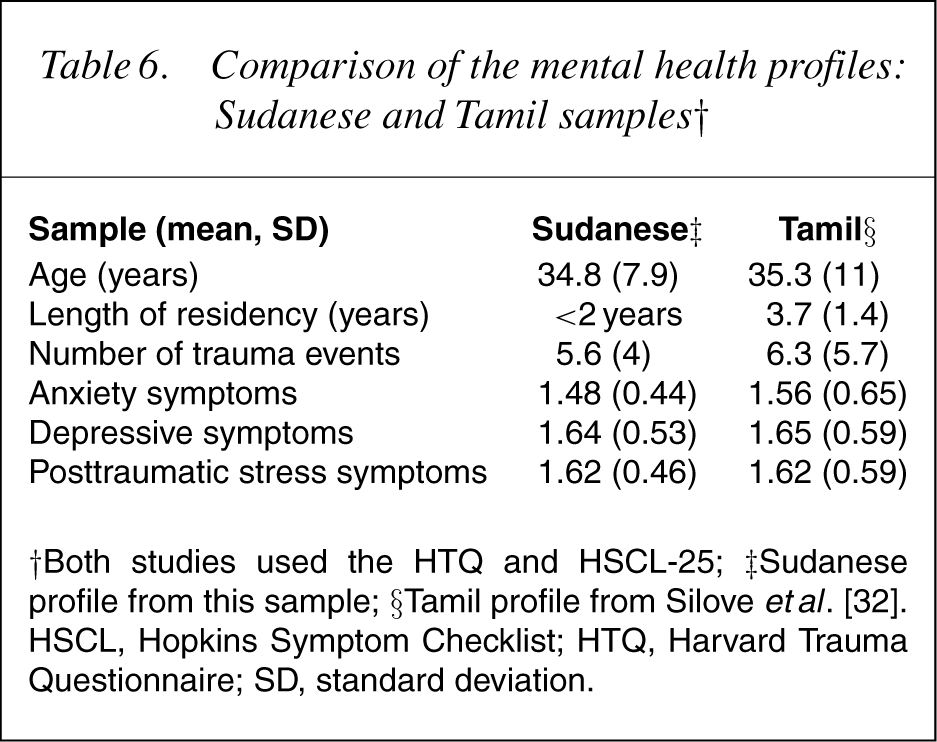
†Both studies used the HTQ and HSCL-25; ‡Sudanese profile from this sample; §Tamil profile from Silove etal. [32]. HSCL, Hopkins Symptom Checklist; HTQ, Harvard Trauma Questionnaire; SD, standard deviation.
A few limitations are associated with this study. The first relates to the reliance on questionnaire responses to identify probable mental illness. Although this procedure has been applied in the refugee literature in the past [25], the relationship between questionnaires relying on item endorsement and formal structured diagnostic interviews is unclear. Future studies may profit from investigating the relationship between findings based upon such instruments and structured clinical assessments. Second, the reliance on in vivo translation may have introduced transcultural error into the response items. However, the majority of respondents were able to communicate in English at a sufficient level to allow administration in that language and therefore, it is unlikely that transcultural error would have impacted on the overall results.
Third, the representativeness of the sample is unclear. Specifically, it employed a small sample that may not be considered fully representative of the larger community of refugees due to the snowball recruitment procedure. Future studies should aim to replicate this research in a larger sample and using more diverse sections of the refugee community. However, while we make no claim that the refugees under study in this paper are representative of other refugee groups – in that it is clear that different groups experience profoundly different difficulties in adjustment – the study of these unique groups of refugees and the particular traumas that apply to them is important in targeting and determining mental health services for them.
In conclusion, the Sudanese refugees in this study experienced considerable mental health difficulties as a result of pre- and post-migration trauma. The trend to increased difficulties over time following their arrival in Australia is of particular concern. Future studies should examine such mental health difficulties longitudinally to provide a more comprehensive understanding of the sequelae of both pre- and post-migration experiences. Longitudinal studies would enable researchers to determine the impact of pre- and post-migration life and would provide a more comprehensive understanding of the determinants of wellbeing in refugees.