
Abstract
Objective:
Post-traumatic stress disorder involves excessive retrieval of traumatic memories. Glucocorticoids impair declarative memory retrieval. This preliminary study examined the effect of acute hydrocortisone administration on brain activation in individuals with earthquake-related post-traumatic stress disorder compared with earthquake-exposed healthy individuals, during retrieval of traumatic memories.
Method:
Participants exposed to earthquakes with (n = 11) and without post-traumatic stress disorder (n = 11) underwent two functional magnetic resonance imaging scans, 1-week apart, in a double-blind, placebo-controlled, counter-balanced design. On one occasion, they received oral hydrocortisone (20 mg), and on the other, placebo, 1 hour before scanning. Symptom provocation involved script-driven imagery (traumatic and neutral scripts) and measures of self-reported anxiety.
Results:
Arterial spin labelling showed that both post-traumatic stress disorder and trauma-exposed controls had significantly reduced cerebral blood flow in response to retrieval of traumatic versus neutral memories in the right hippocampus, parahippocampal gyrus, calcarine sulcus, middle and superior temporal gyrus, posterior cingulate, Heschl’s gyrus, inferior parietal lobule, angular gyrus, middle occipital gyrus, supramarginal gyrus, lingual gyrus and cuneus, and the left prefrontal cortex. Hydrocortisone resulted in non-significant trends of increasing subjective distress and reduced regional cerebral blood flow in the left inferior frontal gyrus, left anterior cingulate gyrus, middle temporal gyrus, cerebellum, postcentral gyrus and right frontal pole, during the trauma script.
Conclusion:
Findings do not fit with some aspects of the accepted neurocircuitry model of post-traumatic stress disorder, i.e., failure of the medial prefrontal cortex to quieten hyperresponsive amygdala activity, and the potential therapeutic benefits of hydrocortisone. They do, however, provide further evidence that exposure to earthquake trauma, regardless of whether post-traumatic stress disorder eventuates, impacts brain activity and highlights the importance of inclusion of trauma-exposed comparisons in studies of post-traumatic stress disorder.
Introduction
Post-traumatic stress disorder (PTSD) is a debilitating condition which develops in a significant minority of people after exposure to a potentially traumatic event. Intrusive memories are one of the hallmarks of PTSD, reflecting excessive consolidation and subsequent retrieval of the traumatic memory, which retains its vividness and power to evoke distress (Brewin et al., 2010). An understanding of the neurobiology behind these intrusive memories is a crucial step in the development of effective interventions for PTSD.
Script-driven imagery involves presentation of autobiographical scripts of traumatic events in order to examine brain activity while traumatic memories are invoked (Bremner et al., 1999). Although mixed, the most common findings using this technique in PTSD have been reduced activation of the anterior cingulate gyrus (ACC) (Lanius et al., 2001, 2003), medial frontal gyrus (Lindauer et al., 2004; Shin et al., 2004) and hippocampus (Bremner et al., 1999). Patients with PTSD also show a negative correlation between amygdala and medial prefrontal cortex (mPFC) activation in response to fearful versus happy faces, suggesting a disconnect in the normal modulation of the amygdala by the mPFC (Shin et al., 2005). This literature supports the neuroanatomical model of PTSD as a failure of mPFC/ACC networks to regulate amygdala activity, resulting in amygdala hyper-reactivity to threat (Shin et al., 2006).
Abnormalities in glucocorticoid regulation have been demonstrated in PTSD, although findings are inconsistent. These include generally low endogenous cortisol levels (Bremner et al., 2007; Yehuda et al., 1996) (although recent meta-analysis suggests only in certain subgroups and circumstances; Meewisse et al., 2007), enhanced glucocorticoid sensitivity (Yehuda, 2001) and that reduced cortisol excretion in response to a traumatic event is associated with a higher risk of developing PTSD (Yehuda et al., 1998). Release of cortisol facilitates reinstatement of physiologic homeostasis and contains the sympathetic nervous system response to stress, and conversely, reduced cortisol may impede this, resulting in adrenaline facilitating consolidation of threat memory (McGaugh and Roozendaal, 2002). In support of this, a recent meta-analysis reported that early administration of hydrocortisone after a traumatic event is effective in prevention of PTSD (Sijbrandij et al., 2015).
Once PTSD is established, the efficacy of current treatments is limited (Watts et al., 2013) and alternative treatments such as glucocorticoids may offer important therapeutic advances. In this context, it is notable that acute elevation of glucocorticoid levels can temporarily inhibit both retrieval of episodic memory (De Quervain et al., 2000, 2003) and of particular relevance, retrieval of perceptually primed material in a ‘traumatic’ context (Holz et al., 2014). It has therefore been suggested that corticosteroids may diminish the retrieval of traumatic memories and promote extinction and inhibitory fear learning (Sijbrandij et al., 2015). This has been examined clinically in a pilot study of three patients with chronic PTSD, given low-dose cortisol (10 mg/day) for 1 month, which reported significant cortisol-related reductions in symptoms of traumatic memories (Aerni et al., 2004). Glucocorticoid administration has also been shown to enhance the efficacy of prolonged exposure treatment for PTSD (Yehuda et al., 2015).
Only one previous study has examined the effect of cortisol administration on brain activation in PTSD. Yehuda et al. used positron emission tomography (PET) during resting state to investigate hydrocortisone administration (17.5 mg) versus placebo in male combat veterans with (n = 16) or without (n = 16) PTSD (Yehuda et al., 2009). The overall effect of hydrocortisone administration was to restore a normal inverse association between the ACC and amygdala in the PTSD group.
The current study uses a similar approach to Yehuda et al. (2009) of examining the short-term effects of administration of hydrocortisone on brain activation as assessed by functional magnetic resonance imaging (fMRI). Essentially, the study aims to investigate some aspects of the mechanism of action of hydrocortisone by determining its effect in the specific context of trauma imagery. We also aim to examine this effect between groups – in individuals with PTSD and a group of similarly trauma-exposed healthy controls (TEC).
The sample in this study is unique in that all participants (PTSD patients and TEC) experienced similar traumatic events. Between the years of 2010 and 2012, a series of four major earthquakes struck the city of Christchurch, New Zealand, resulting in 185 deaths, substantial damage to the central city and over 10,000 subsequent aftershocks (Ardagh et al., 2012).
Key hypotheses in this study were that in response to trauma scripts (compared with neutral scripts), patients with PTSD versus TECs would have greater anxiety and would show reduced mPFC and greater amygdala activation. In addition, these subjective and imaging effects would be attenuated by hydrocortisone.
Methods
Participants
PTSD participants
Participants recruited into the study were those referred to a specialist outpatient, treatment programme for earthquake-related anxiety in Christchurch, New Zealand. All PTSD participants were aged over 18 years and were diagnosed with PTSD by an experienced clinician according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria (American Psychiatric Association [APA], 1994). Diagnosis at the time of neuroimaging was confirmed by a second clinician using the Clinician Administered PTSD Scale (CAPS) (Blake et al., 1995). PTSD symptomatology was directly related to the Canterbury earthquakes. Exclusion criteria were as follows: presence of contraindications to glucocorticoid therapy (e.g. tuberculosis, gastric and duodenal ulcers, Cushing’s disease, hypertension, pregnancy), significant physical disease, current topical/inhaled glucocorticoid therapy, current psychosis, bipolar disorder, severe depressive disorder (total score ⩾17 on Hamilton Depression Rating Scale-17 Item [HAM-D-17]) or substance-related disorder (screened using the Mini-International Neuropsychiatric Interview [MINI]; Sheehan et al., 1998), severe personality disorder, severe cognitive impairment or organic psychiatric disorder, random blood glucose measurement above normal range, or any contraindication to fMRI. In relation to antidepressant medication use, seven PTSD patients were on no medication, two were prescribed selective serotonin reuptake inhibitors (SSRIs), one a serotonin-noradrenaline reuptake inhibitor (SNRI) and one a tricyclic antidepressant (TCA).
TEC
The TEC group consisted of volunteers over 18 years old from the general population in Christchurch who had experienced the earthquakes. They were recruited through flyers posted in public places. These participants fulfilled criterion A1 for PTSD from DSM-IV in relation to the earthquakes (i.e. experienced the earthquakes as life-threatening) but did not fulfil diagnostic criteria for PTSD or any other mental disorder (screened with the MINI). Exclusion criteria were identical to the PTSD group. PTSD and TEC groups were matched for age, gender and, where possible, handedness. All participants were fluent in English. Patients and TECs were recruited simultaneously, and at a similar rate, between November 2013 and February 2016.
Study design
This was an fMRI study of participants exposed to earthquake-related trauma: one group with and the other group without PTSD. Each participant underwent two fMRI scans at the same time of day, 1 week apart, in a double-blind, placebo-controlled, cross-over design. On one occasion, they received hydrocortisone (20 mg), and on the other, a placebo, 1 hour before scanning and script-driven imagery. This dose was chosen to be in the range of that used in the only previous study of brain activation in individuals with PTSD (Yehuda et al., 2009). The identity of the drug/placebo (lactose) was concealed by being encapsulated, and therefore, looked identical. This study was approved by the National Health and Disability Ethics Committee (Southern Branch; 12/STH/69) and all participants gave informed written consent.
Scripts
At least 1 day prior to the first fMRI scan, all participants provided an autobiographical description of their most traumatic experience related to the earthquakes and of a neutral life event. The script-driven imagery methodology used was adapted from previous neuroimaging studies (Lanius et al., 2001; Shin et al., 1999, 2004). Participants were asked to think carefully about the events, to give a detailed narrative of what happened and encouraged to include a description of bodily senses experienced during the trauma. These narratives were converted by a Research Nurse (L.W.) into scripts written in the first person and present tense that were able to be presented onto the fMRI computer screen. The same number of words was used for the neutral and traumatic conditions (70 words). In addition to the scripts, three keywords were agreed on between the participant and Research Nurse that represented the neutral and traumatic scripts for use during the blood-oxygen-level-dependent (BOLD) measurements (see below).
Procedure
One hour prior to each fMRI scan, participants provided the first of three saliva swabs as a baseline measure of salivary cortisol. Immediately following this, they took either hydrocortisone or placebo. During this hour, they were familiarised with the Subjective Units of Distress Scale (SUDS) which was used as a measure of state anxiety or distress, with 0 = ‘completely relaxed’ and 10 = ‘highest anxiety/distress ever felt’. Immediately before the fMRI scan began, participants provided their first SUDS rating to the Research Nurse and their second saliva swab.
Each scanning session included the following: a high-resolution T1-weighted scan, T2 and T2 fluid-attenuated inversion recovery (FLAIR) acquisitions (to exclude incidental clinical findings), a resting state functional connectivity acquisition, two cerebral perfusion acquisitions and one functional BOLD acquisition. Perfusion scanning occurred after the T1 and resting state acquisition. During the first perfusion run (6:46), participants were presented with their neutral script. Participants were presented with their traumatic script during the second perfusion run. Order of script presentations was fixed for each participant. During the presentation of these scripts, participants were instructed to imagine being present at the event, and to recall emotions and bodily sensations experienced at the time of them. At the end of each script presentation, participants were asked to provide a current SUDS rating. After acquiring the T2 and T2-weighted images, a 10-minute BOLD fMRI run was acquired. During this, participants were asked to read alternating presentations of the three keywords for each script (neutral and traumatic) for periods of 30 seconds, for a total of 10 minutes, to allow measurement of BOLD signal. At the end of the fMRI scanning session, participants provided their final saliva swab sample and SUDS rating.
Details about image acquisition, structural pre-processing and analysis, arterial spin labeling (ASL) pre-processing and analysis, and functional pre-processing and analysis are provided in Supplemental Material A.
Cortisol analysis
Cortisol data were collected using Salivette tubes (Sarstedt). Participants first placed a cotton swab provided in each Salivette tube in his or her mouth and gently chewed on it for about 1 minute. The swab was then placed back in the tube. Tubes were kept at −20°C until analysis. Briefly thawed saliva (250 µL) was extracted with 1.0 mL of dichloromethane and 500 µL portions evaporated to dryness. Dried extracts were reconstituted in 125 µL of buffer and analysed for cortisol by enzyme-linked immunosorbent assay using a series of standards from 0 to 280 nmol/L (as described in Lewis et al. (1992)). Sample sets from each participant were analysed in the same batch to avoid inter-assay variation and the intra-assay variation was 7.6%.
Statistical analysis (non-imaging)
Statistical analyses of demographic, clinical and cortisol data were conducted using SPSS version 22-x for Windows (IBM Corporation, 2013). To assess demographic and clinical data, χ2 tests or independent samples t-tests were used, with group (PTSD vs TEC) as the between-participants factor. For cortisol and SUDS data, repeated measures analysis of variance (ANOVA) was used with group (PTSD vs TEC) as the between-participants factor and drug (hydrocortisone vs placebo) and time (cortisol: baseline, pre-scan and post-scan; SUDS: baseline, pre-neutral script, post-neutral script, post-trauma script, post-scan) as the within-participant factors.
Results
Thirteen patients with PTSD and 12 TECs consented to and commenced study procedures. One patient with PTSD dropped out of the study as they refused a follow-up session due to distress associated with the scanning procedure. Two participants (one PTSD and one TEC) were excluded from all imaging analyses: one had a major frontal artefact and with the other participant, there were technical issues with the scanner. Thus, 11 patients with PTSD and 11 TEC participants were included. Groups did not differ in age, gender, years of education or date of testing (number of months after February 2011 earthquake) (see Table 1). Total CAPS score in the PTSD group was 60.2, representing moderately severe PTSD, and total HAM-D score was 10.6, representing mild depression.
Demographic and clinical characteristics of post-traumatic stress disorder (PTSD; n = 11) and trauma-exposed control (TEC; n = 11) groups.
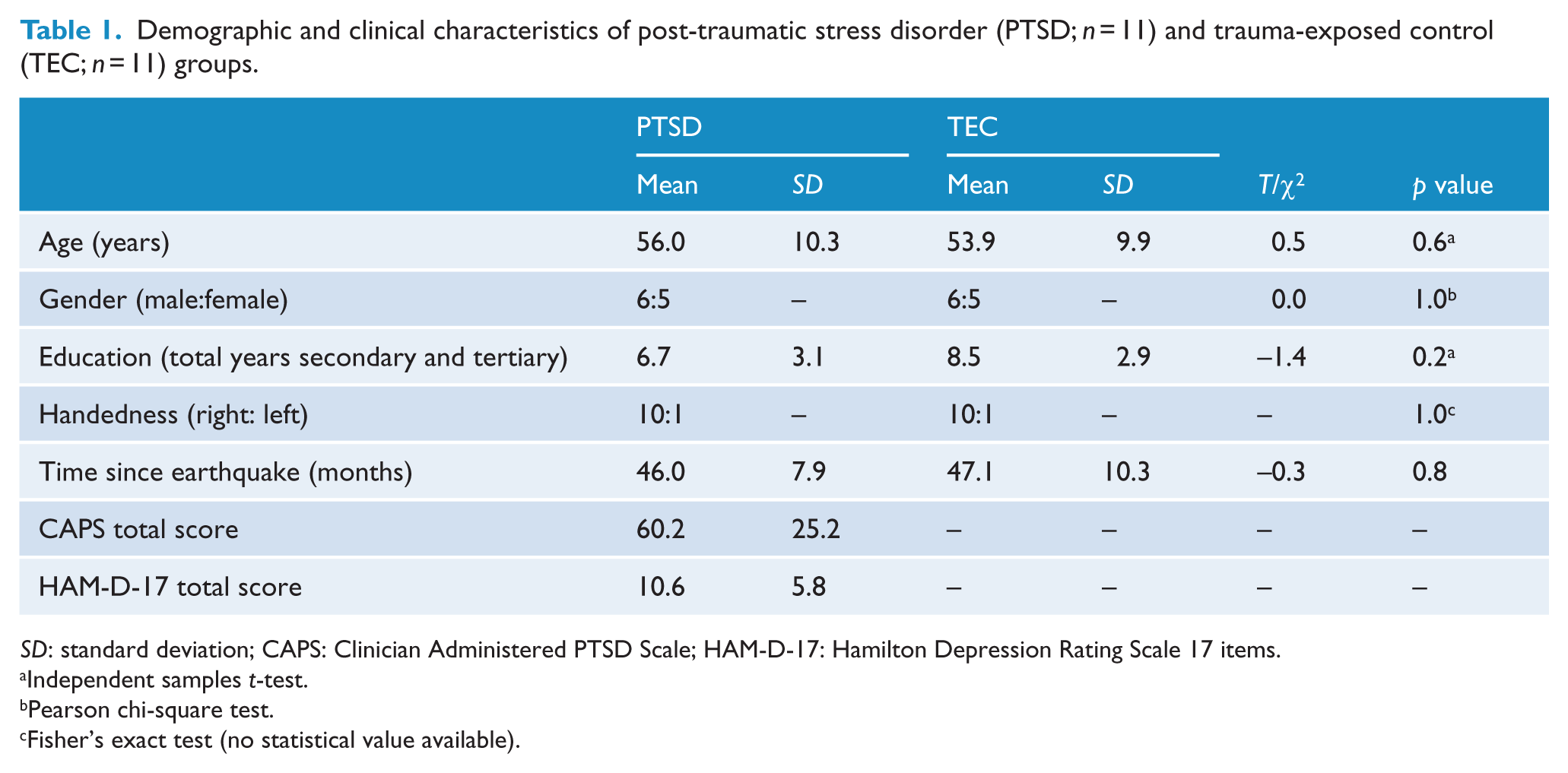
SD: standard deviation; CAPS: Clinician Administered PTSD Scale; HAM-D-17: Hamilton Depression Rating Scale 17 items.
Independent samples t-test.
Pearson chi-square test.
Fisher’s exact test (no statistical value available).
Subjective anxiety ratings
Repeated measures ANOVA of SUDS ratings showed a significant effect of Group (F = 11.1, p = 0.003), with ratings being significantly higher in the PTSD group compared with the TEC group (see Figure 1). In both groups, subjective anxiety peaked after presentation of the trauma script (T4), as reflected in a significant effect of time (F = 8.1, p < 0.0001), but the peak in subjective anxiety was much more pronounced in the PTSD group compared with the TEC group, as reflected by a significant Time by Group interaction (F = 4.2, p = 0.004). Repeated measures ANOVA showed a trend towards an effect for Drug (F = 3.5, p = 0.08) and for a Drug × Group interaction (F = 3.7, p = 0.07), with the hydrocortisone condition related to greater SUDS ratings in the PTSD compared with the control group.
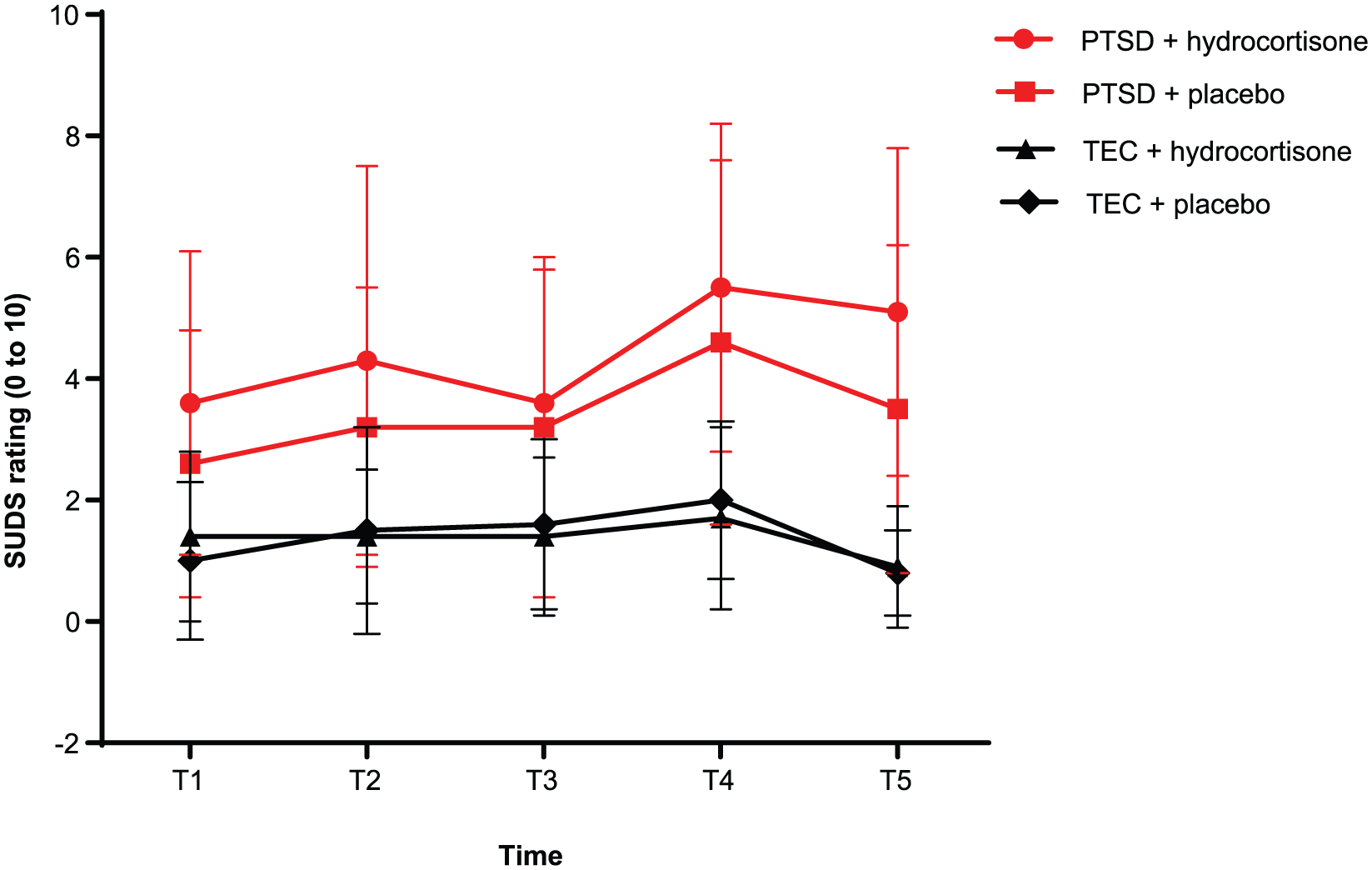
Mean (SD) Subjective Units of Distress Scale (SUDS) score over time after administration of hydrocortisone or placebo in PTSD and trauma-exposed healthy control (TEC) groups.
Imaging results
Missing and excluded data
One participant (PTSD group) was excluded from the ASL analyses as the trauma script was not displayed at baseline, and another (TEC group) was excluded from fMRI analyses, as functional images were not acquired at follow-up. Thus, group numbers were as follows for imaging analyses – structural analyses: PTSD patients n = 11, controls n = 11; ASL analyses: PTSD patients n = 10, TEC n = 11; and fMRI analyses: PTSD patients n = 11, TEC n = 10.
Structural analyses
Whole brain analyses, controlling for age and gender, revealed no significant differences between the PTSD (n = 11) and TEC (n = 11) groups.
ASL analyses
Whole brain analyses revealed a significant main effect of condition (trauma vs neutral; false discovery rate (FDR)-corrected p < 0.001). Regional blood flow was significantly reduced in the trauma condition versus neutral condition in the following areas: right hippocampus, parahippocampal gyrus, calcarine sulcus, middle and superior temporal gyrus, posterior cingulate, Heschl’s gyrus, inferior parietal lobule, angular gyrus, middle occipital gyrus, supramarginal gyrus, lingual gyrus and cuneus, and the left middle and inferior frontal gyrus (pars triangularis) (see Table 2 and Figure 2). No significant main effects of Group or Drug were found, nor were there any significant interactions between Group and Drug, or Group, Condition and Drug.
Cluster sizes of brain regions from ASL that showed significant differences between trauma and neutral script conditions in post-traumatic stress disorder (PTSD; n = 10) and trauma-exposed control (TEC; n = 11) groups.
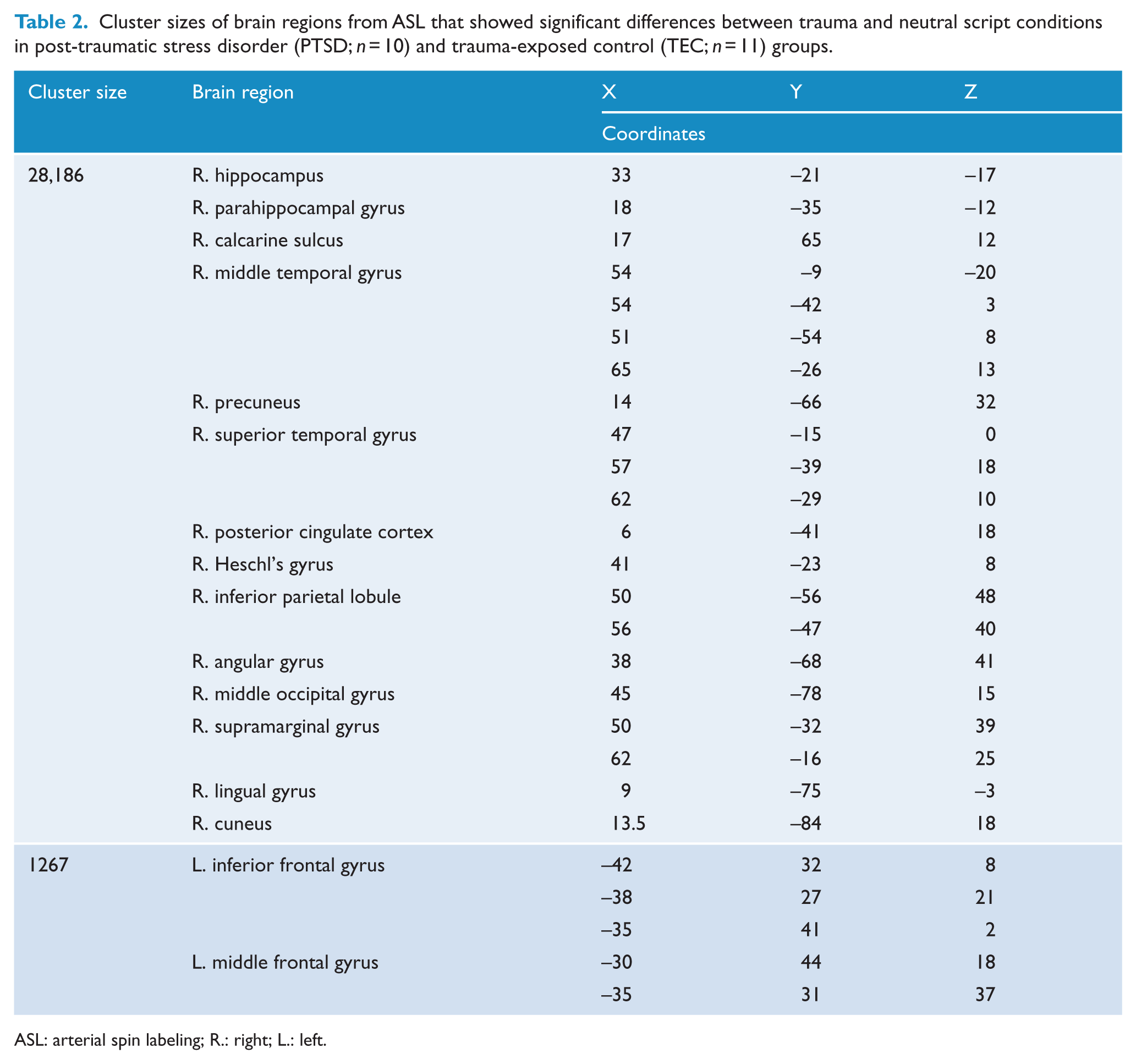
ASL: arterial spin labeling; R.: right; L.: left.
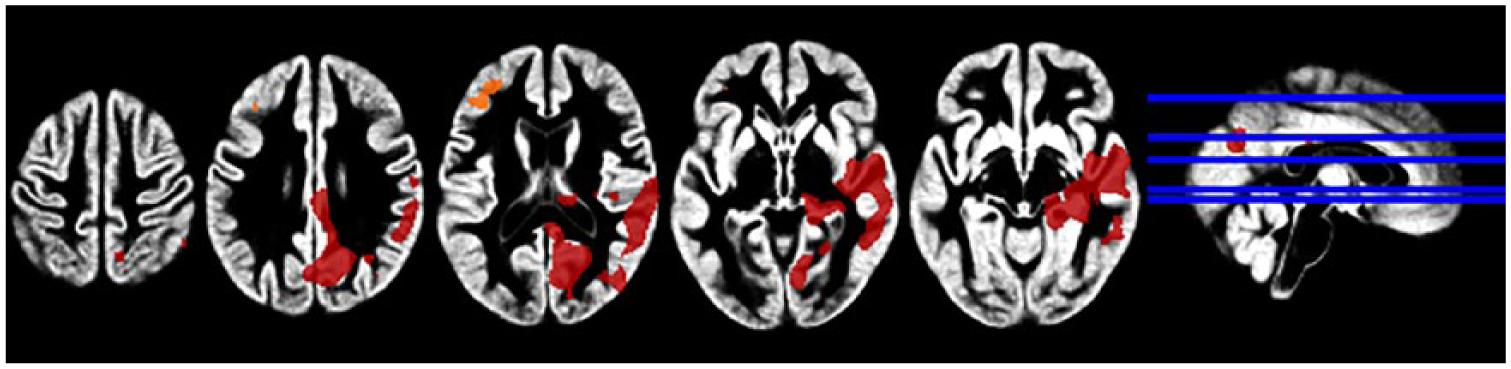
Regions of cerebral blood flow decrease in the traumatic versus neutral comparison in all participants (PTSD and TEC groups, cluster-wise FDR < 0.001; n = 22).
Prior to correcting for multiple comparisons, a significant Condition × Drug interaction was found (see Table 3 and Figure 3). Regional blood flow in the left inferior frontal gyrus, left ACC, left middle temporal gyrus, left cerebellum, right frontal pole and left postcentral gyrus was significantly reduced after hydrocortisone administration compared with placebo administration during the trauma script presentation. With the neutral script, the regional blood flow was unchanged between hydrocortisone and placebo. This interaction did not remain after correction for multiple comparisons.
Cluster sizes of brain regions from ASL that showed significant differences between hydrocortisone and placebo conditions during trauma script presentation in post-traumatic stress disorder (PTSD; n = 10) and trauma-exposed control (TEC; n = 11) groups.
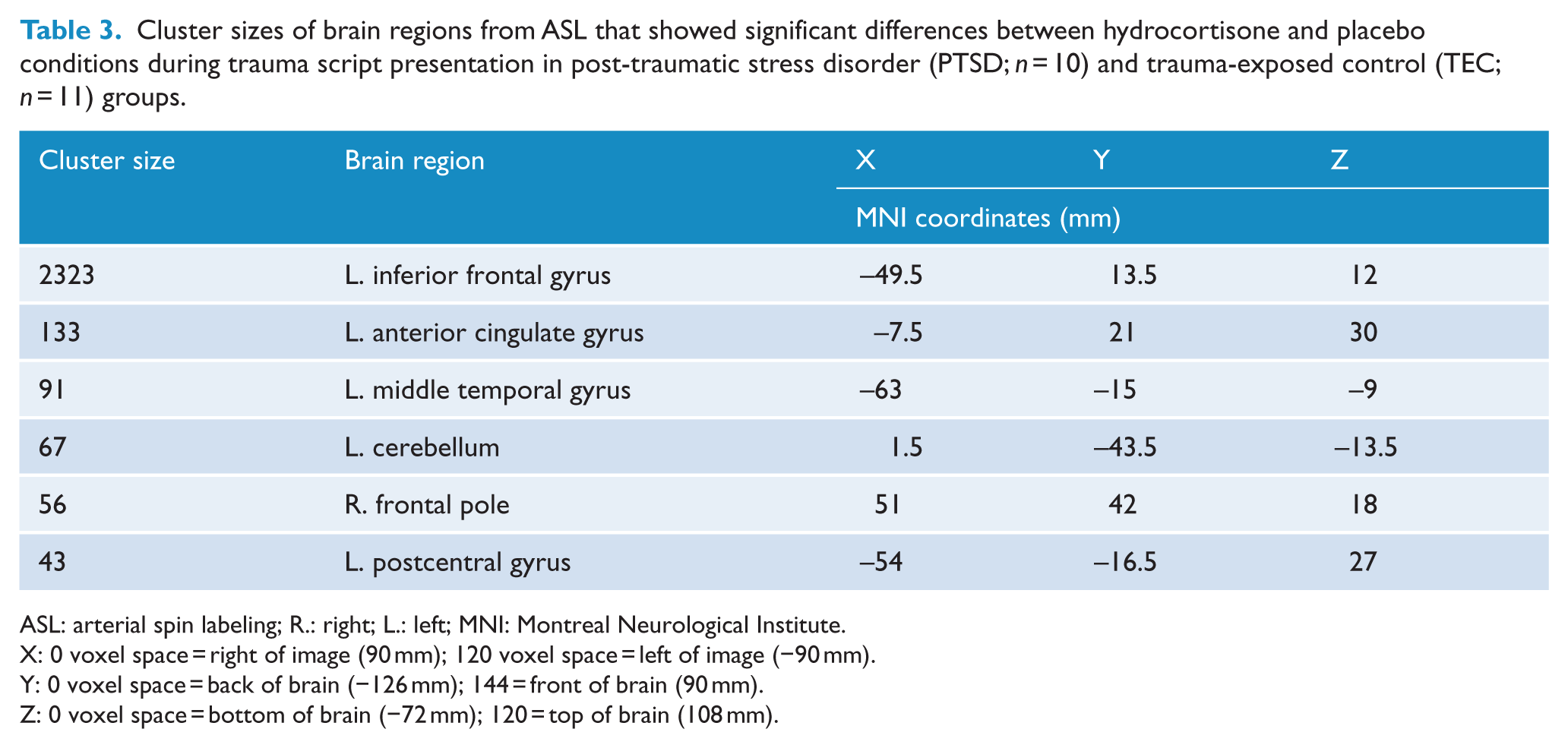
ASL: arterial spin labeling; R.: right; L.: left; MNI: Montreal Neurological Institute.
X: 0 voxel space = right of image (90 mm); 120 voxel space = left of image (−90 mm).
Y: 0 voxel space = back of brain (−126 mm); 144 = front of brain (90 mm).
Z: 0 voxel space = bottom of brain (−72 mm); 120 = top of brain (108 mm).
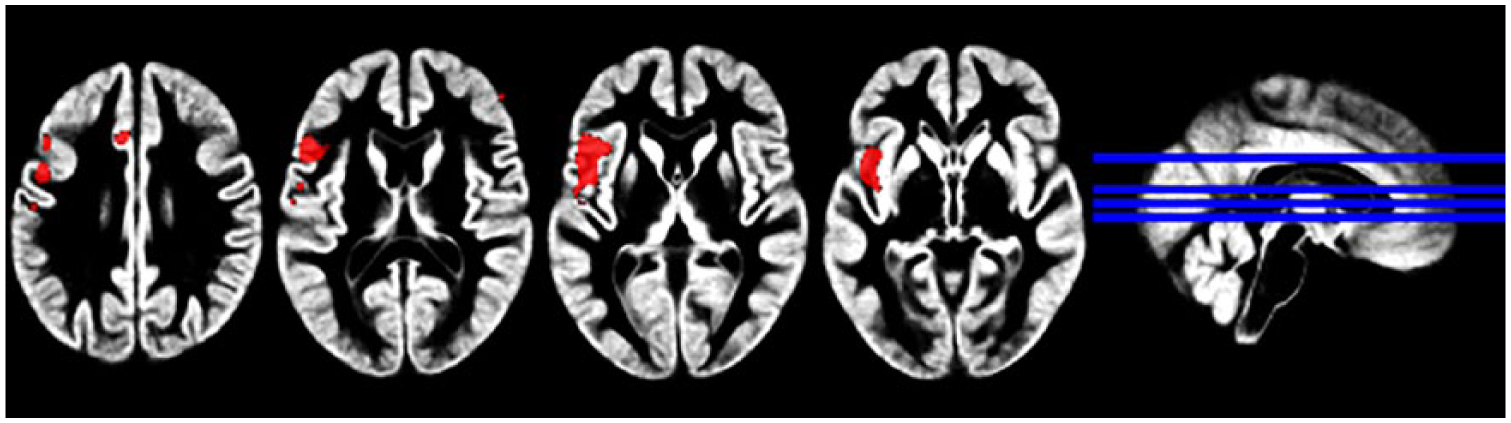
Regions of reduced cerebral blood flow in the hydrocortisone versus placebo condition during trauma script presentation in all participants (PTSD and TEC groups, cluster-wise FDR < 0.001; n = 22).
BOLD functional analyses
Whole brain analyses, controlling for age and gender, revealed no significant main effects of Condition (trauma vs neutral words), Group or Drug, as well as no significant interactions.
Cortisol levels
Baseline cortisol levels were not significantly different between PTSD and TEC groups (t = 0.06, p = 1.0). Repeated measures ANOVA showed significant effects of Drug (F = 71.0, p < 0.0001), with cortisol levels being significantly higher when hydrocortisone was administered compared with when the placebo was administered (see Figure 4). A significant effect of Time (F = 23.2, p < 0.0001) reflected peak cortisol levels that occurred 1 hour after hydrocortisone administration (i.e. immediately prior to imaging session; see Figure 4). No effect of Group (F = 2.4, p = 0.14) was found, nor was there a significant interaction between Drug and Group (F = 3.1, p = 0.09).
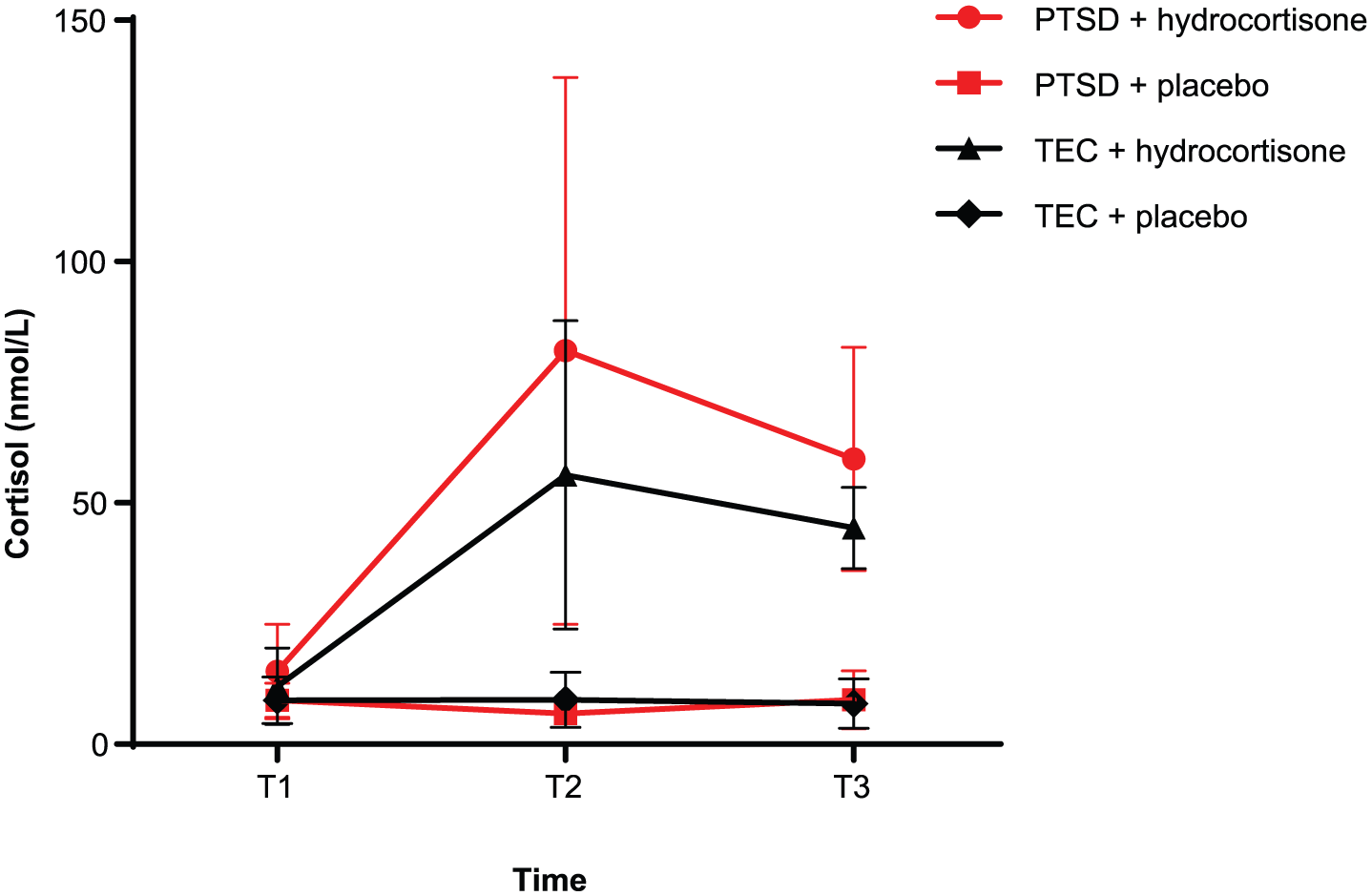
Mean (SD) cortisol levels (nmol/L) following glucocorticoid versus placebo administration over time in PTSD and trauma-exposed control (TEC) groups.
Discussion
This is the first neuroimaging study to investigate the effect of acute glucocorticoid administration on brain activity during symptom provocation using script-driven imagery, in patients with PTSD and TECs. Key hypotheses were that in response to trauma scripts (compared with the neutral scripts), patients with PTSD (compared with TECs) would have greater anxiety and would show reduced mPFC activation and greater amygdala activation, and that these subjective and imaging effects would be attenuated by hydrocortisone administration.
Trauma scripts resulted in increased anxiety
Both the PTSD and TEC groups reported increased anxiety in response to trauma compared with neutral scripts. As expected, patients with PTSD experienced the script-driven imagery procedure as subjectively more anxiety-provoking (SUDS) than the TEC group. This has been a consistent finding in neuroimaging studies using script-driven imagery (Lanius et al., 2007; Lindauer et al., 2004).
Cerebral blood flow changes in response to trauma scripts
In both groups, recollection and imagery of traumatic versus neutral personal events was associated with significantly reduced cerebral blood flow in the right hippocampus, parahippocampal gyrus, calcarine sulcus, middle and superior temporal gyrus, posterior cingulate, Heschl’s gyrus, inferior parietal lobule, angular gyrus, middle occipital gyrus, supramarginal gyrus, lingual gyrus and cuneus, and the left inferior and middle frontal gyri. These findings are consistent with previous reports of decreased activation of the ACC (Lanius et al., 2001, 2003), the medial frontal gyrus (Lindauer et al., 2004; Shin et al., 2004) and the hippocampus (Bremner et al., 1999) in patients with PTSD. It has been suggested that reduced activity in these brain regions may impair the extinction of fear and thereby play a role in the development or maintenance of symptoms of PTSD (Van Elzakker et al., 2014).
Although the neurocircuitry model of PTSD described above (Hayes et al., 2012) proposes amygdala hyper-reactivity, we did not find amygdala activation in response to traumatic (vs neutral) scripts in either group. This surprising lack of amygdala activation has however been reported previously by studies of similar design using script-driven recall (Lanius et al., 2001; Lindauer et al., 2004).
We had hypothesised that in response to trauma scripts, the PTSD group would show greater amygdala activation and reduced mPFC activation compared with the TEC group. Overall, we found no differences in cerebral blood flow during script-driven imagery between PTSD and TEC groups, which was an unexpected and notable finding. This finding, however, was consistent with the most comparable previous study using single-photon emission computed tomography (SPECT) in 30 police officers with PTSD compared with TEC (Lindauer et al., 2004). Recent meta-analyses have also reported that differences in amygdala activation are not observed when comparisons are between patients with PTSD and TECs (rather than non-TEC) (O’Doherty et al., 2015; Patel et al., 2012). Our finding of no difference in mPFC activation between groups is, however, different from that reported by the Lindauer study (Lindauer et al., 2004) and meta-analyses of functional (Hayes et al., 2012; Patel et al., 2012; Stark et al., 2015) and structural (O’Doherty et al., 2015) brain imaging studies which provide evidence for decreased activity and volume in the mPFC, left inferior cortex and ACC in PTSD compared with trauma-exposed and non-exposed controls.
It may be that differences in findings are explained by the form in which the trauma-related information is presented. Some previous studies have presented trauma-related pictures, some have presented audiotaped scripts (Lanius et al., 2007; Lindauer et al., 2004), while in the current study the trauma scripts were presented visually. Interestingly, studies which have reported amygdala hyper-responsivity have typically used external cues (such as pictures) suggesting that heightened amygdala activation in these studies is related more to the processing of external rather than internal stimuli (Phan et al., 2002; Reiman et al., 1997). The results may also be different partly because of the slightly different imaging modality (SPECT vs BOLD).
The finding of no significant difference in brain activation between the groups emphasises the importance of including TEC comparisons, which has been an area of increasing interest. Meta-analyses have reported that when patients with PTSD are compared only with TECs (rather than including non-TEC), there was only differential involvement between the groups in the basal ganglia (Stark et al., 2015). This suggests that the experience of trauma (whether it leads to symptoms consistent with PTSD or not) may have lasting effects on the brain, which has been supported by many recent imaging studies (Chen et al., 2018; Lu et al., 2017; Malhi et al., 2019). Of note, a long-term (41 months) study of functional connectivity in TECs exposed to earthquakes in China, compared with non-TEC, reported greater grey matter density in prefrontal-limbic systems (dorsal ACC, medial PFC, amygdala and hippocampus; Li et al., 2017). Similarly, a study following up soldiers exposed to combat reported persisting brain connectivity changes in the mid-brain 1.5 years after combat-exposure (Van Wingen et al., 2012).
Effect of hydrocortisone
Hydrocortisone significantly elevated cortisol levels over the course of the brain imaging session in both groups. It also resulted in a trend towards increasing subjective measures of anxiety in the PTSD group compared with the TEC group. This was counter to our hypothesis and is an interesting finding, but is tempered by the fact that this was only seen at statistical trend level. Although previous studies have been of small sample size, they have suggested that hydrocortisone in PTSD patients has therapeutic effects in reducing re-experiencing symptoms (Aerni et al., 2004), diminishing avoidance and numbing symptoms in response to script-driven imagery (Suris et al., 2010), reducing drop-out rates and improving the outcome of prolonged exposure treatment (Yehuda et al., 2010, 2015).
We had hypothesised that hydrocortisone would attenuate the predicted amygdala hyperactivation and/or mPFC hypoactivation in response to the trauma scripts. In a previous study using PET imaging in older veterans, hydrocortisone restored the normal inverse relationship between activity of the ACC and amygdala in the PTSD group (Yehuda et al., 2009). As described above, we found reduced mPFC activation (but not amygdala hyper-activation) in response to the anxiety-provoking trauma scripts, but also that there was no significant difference between groups. The effect of hydrocortisone was also not significantly different between groups. Hydrocortisone, in both groups, resulted in a reduction in regional cerebral blood flow in the left inferior frontal gyrus, left ACC, left middle temporal gyrus, left cerebellum, right frontal pole and left postcentral gyrus, but only during the trauma script presentation. Neurocircuitry models would suggest that reduced activation in these regions results in decreased regulation of mPFC/ACC networks to regulate amygdala activity, resulting in hyper-reactivity to threat (Shin et al., 2006). These findings are not consistent with the glucocorticoid hypothesis of PTSD described earlier. A possible explanation for the reduction in cerebral blood flow in response to hydrocortisone may reflect findings from previous studies in non-TEC, which reported that hydrocortisone impairs declarative memory retrieval processes and reduces cerebral blood flow in the right posterior medial temporal lobe, cerebellum and left visual cortex (De Quervain et al., 2003). A recent systematic review of studies of PTSD in the context of ongoing threat (Fragkaki et al., 2016) reported that, although inconsistent, there was a pattern of increased cortisol being more pronounced in PTSD patients than TECs, which may explain our finding of a trend towards hydrocortisone increasing anxiety in the PTSD group. It is important to note that these findings of the effects of hydrocortisone on cerebral blood flow were equivocal in that they did not remain after correction for multiple comparisons.
One of the possible reasons for a lack of effect of hydrocortisone on measures of brain activation is the dose used in this study (20 mg). This is a relatively low dose. Doses of 20 mg twice per day have often been used to attempt to mimic the cortisol levels seen in depression (Young et al., 1999). Behavioural data (SUDS) did show a difference following administration of hydrocortisone at a trend level. This is suggestive of, but not proof of, at least some effect of this dose of hydrocortisone. Another related issue is the pharmacokinetics of hydrocortisone. We timed the scan to occur around the time of peak levels (1 hour after dosing). As can be seen from Figure 1, levels were highest in the sample immediately before the scan (T2) but were still very significantly raised at the end of scanning (T3). The pharmacokinetics of hydrocortisone are also likely to be relevant for treatment effects. The only preliminary treatment study administered 10 mg daily for 1 month. At this point, it is clearly not known whether beneficial effects would be seen following higher doses for a shorter period of time or whether a constant elevation of cortisol levels, which for instance might be seen with twice daily dosing, would be more beneficial. This study suggests that a single relatively low dose does not have profound effects.
Cerebral blood flow: ASL versus bold analyses
This study used both an ASL paradigm during prolonged trauma recollection and a BOLD approach which contrasted response to trauma-related words with neutral words. Use of hydrocortisone was the reason for selection of the ASL method in this study (Stewart et al., 2014). The prolonged ASL paradigm showed differences between the traumatic and neutral script presentation. One previous study used a prolonged presentation of trauma-related stimuli but measured the BOLD response. Surprisingly, the BOLD response, which has been most extensively used in previous studies, showed no differences between groups or between the trauma-related and neutral words in the current study. It is possible that this may be explained by the order of the scanning sessions, with BOLD acquisition being performed after the cerebral perfusion acquisitions (i.e. after the neutral and trauma scripts). SUDS ratings indicated that after trauma scripts, both groups reported increased distress, and this is when the BOLD runs were acquired. There may, therefore, have been carry-over effects into this run.
Unique aspects and strengths of this study design
What sets the current study findings apart from the previous literature is the lack of differences in activation between the PTSD and TEC groups during symptom provocation. This suggests that it is exposure to earthquake-related trauma itself that impacts brain activation when recollecting memories related to the traumatic memories, and that this is not specific for the diagnosis of PTSD. We have previously reported similar findings in terms of impacts of the earthquake exposure of emotion processing and neuropsychological functioning (Bell et al., 2017, 2018).
There has been increasing interest in understanding PTSD under circumstances of ongoing threat, such as that occurring in this study with the ongoing exposure to aftershocks (over 10,000 in a 2-year period) and post-earthquake stressors (Fragkaki et al., 2016). Clinically, it could be hypothesised that this continued exposure could fuel symptomatology and have persisting impacts on brain neurobiology and neuroendocrinology, resulting in both groups being in a chronically hyperaroused state. Interestingly, however, the TECs although fulfilling criteria for exposure to a Criterion A event from DSM-IV definition of PTSD did not report symptoms reaching threshold for other criteria (suggesting that levels of hyperarousal were not significant).
Both patient and TEC samples recruited in this study are different in several ways from those in previous studies. Importantly, both groups in this study experienced the same traumatic event. Many script-driven imagery studies have recruited PTSD and control samples who have experienced different types of trauma, including various traumatic events likely to occur to a police officer (Lindauer et al., 2004), samples with a combination of male combat veterans and female nurse veterans (Shin et al., 2004) or a combination of sexual abuse and motor vehicle accidents (Lanius et al., 2003). While previous studies have typically included control groups who have experienced similar trauma to PTSD groups, no specific measure of the control groups’ interpretation of the trauma has been included (with the exception of Lanius et al. (2003)). That is, TEC participants may have experienced a severe trauma but they may not have interpreted the trauma as life-threatening or traumatising. In the current study, the TEC group experienced the earthquake trauma as traumatising and life-threatening and fulfilled criteria for exposure to a DSM-IV PTSD Criterion A event. Both groups had also been exposed to the post-earthquake environment and the prolonged series of aftershocks over at least a 2- to 3-year period. In addition, many previous studies have examined patients with long-standing PTSD related often to wars or sexual abuse. The patients in this study had relatively recent onset PTSD from exposure to earthquakes a maximum of 4 years earlier. The time passed since the onset of the earthquakes was also similar between groups, as TEC participants took part in the study immediately after completion of an age- and gender-matched patient. Finally, individuals with PTSD in the current study had low levels of comorbidity due to the exclusion process. Many previous imaging studies have included PTSD samples with high levels of major depression and other psychiatric disorders, and thus, the possibility that their findings may be, in part, related to features of comorbid conditions may have complicated findings.
We suggest that the design of this study, and specifically, similarities between the two groups in terms of trauma exposure, low psychiatric comorbidity, and well-matched demographic characteristics, gives considerable weight to the findings and may explain the differences in our findings in comparison with the previous literature.
Limitations
The study was small and lack of positive results may relate to lack of power, and as such, these results can be considered only preliminary. However, previous brain imaging studies of PTSD using symptom provocation have reported significant findings with similar sample sizes to the current study (Bremner et al., 1999; Lanius et al., 2001, 2003; Shin et al., 1999). This criticism is true to a lesser extent when considering the hydrocortisone compared with placebo comparison in which individuals were their own controls. There are also a number of other limitations of the current study. First, in order to determine whether exposure to earthquake trauma (not necessarily progression to PTSD) results in changes in brain activation, a control group consisting of non-exposed controls would have been required. This would have involved recruitment of a group of participants outside of the Canterbury region, which was not feasible in the current study. Second, although the TEC group did not have any mental disorder, we did not have a measure of a count of PTSD symptoms using, for example, the CAPS, which may have informed further description of this group. In addition, although the TEC group was exposed to a similar trauma as the PTSD group, and interpreted the trauma as life-threatening, a systematic measure of trauma exposure was not included in order to compare the extent of trauma exposure between groups. The Traumatic Exposure Severity Scale (TESS; Elal and Slade, 2005), which was designed specifically to assess trauma severity to natural disasters, would have been a useful addition to this study in order to compare earthquake exposure severity between groups. Third, 4 of the 11 PTSD participants were taking antidepressant medication, which was too small a number to comment on, although previous studies have suggested that that this may affect activation in the medial frontal gyrus but with little or no impact on other mPFC regions (Dahlgren et al., 2018). Fourth, research suggests that symptom provocation may result in two different brain activation patterns depending on whether the patient responds to trauma recollection and imagery with symptoms of hyperarousal or dissociation (Lanius et al., 2006). While anxiety was assessed throughout the symptom provocation procedure in the current study, dissociative responses were not. If the sample was heterogeneous in terms of having dissociative or hyperarousal responses to trauma recollection, this may have served to weaken any effects seen.
Implications and conclusion
The preliminary study has considerable strengths, particularly the groups being well matched for trauma exposure. The findings do not fit with some aspects of the accepted neurocircuitry model of PTSD (i.e. failure of the mPFC to quieten hyperresponsive amygdala activity and the potential therapeutic benefits of hydrocortisone). The uniqueness of the setting of this study, with ongoing earthquake and aftershock exposure, may provide some explanation for this. The study suggests the importance of including a TEC group in studies of PTSD and the role of ongoing threat. In addition, findings provide further evidence that repeated exposure to earthquake trauma, regardless of whether PTSD eventuates from this exposure, impacts brain activity. Individuals who cope well with stress related to traumatic events may still be affected from a neurobiological perspective, but become resilient through other pathways. Future neuroimaging studies involving longer term follow-up (i.e. once aftershocks have ceased) of earthquake-exposed controls in comparison with non-exposed controls would be of use to elucidate brain areas involved in the stress and threat from earthquake exposure.
Supplemental Material
Supplemental_material – Supplemental material for Traumatic imagery following glucocorticoid administration in earthquake-related post-traumatic stress disorder: A preliminary functional magnetic resonance imaging study
Supplemental material, Supplemental_material for Traumatic imagery following glucocorticoid administration in earthquake-related post-traumatic stress disorder: A preliminary functional magnetic resonance imaging study by Katie M Douglas, Samantha Groves, Richard J Porter, Jenny Jordan, Lynere Wilson, Tracy R Melzer, Richard G Wise, Jonathan I Bisson and Caroline J Bell in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors thank the participants and staff involved in the running of this study at the Department of Psychological Medicine (University of Otago, New Zealand) and New Zealand Brain Research Institute (Christchurch, New Zealand) for their cooperation in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Project Grant to KD from the Canterbury Medical Research Foundation (CMRF), New Zealand. The CMRF had no further role in any aspect of the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.