
Abstract
The present study explores the mental health of humanitarian entrants from Burmese refugee backgrounds recently arrived in Australia, as well as the contributions of gender, pre-migration trauma and post-migration living difficulties in predicting psychological well-being. Prolonged and violent ethnic conflict in Burma (controversially named Myanmar) since 1984 has resulted in the internal displacement of over one million people. A further million have fled Burma, seeking initial refuge in neighbouring countries including Thailand, India, Bangladesh, China and Malaysia [1]. With the assistance of the United Nations High Commissioner for Refugees (UNHCR), a growing number of these individuals have arrived in Australia for resettlement since 2005, and in the 2008 to 2009 period, refugees from Burma received 2412 off-shore visas [2], second only to the 2874 visas granted to people from Iraq. While several Burmese ethnic groups are represented, including Rohingya, Chin, Mon, Karenni and Kachin amongst others, Karen people constituted the largest ethnic group arriving in Australia from Burma in the 2005 to 2009 period. According to the Department of Immigration and Citizenship (DIAC) settlement data base, 4756 of the 8116 Burmese arrivals self-identified as Karen [Watters, A: personal communication]. This is probably an underestimate, as many Karen may also be amongst the 1996 arrivals self-identified as the super-ordinate ‘Burmese’.
Pre-migration traumas have been associated with negative mental health. Previous research findings indicate that being subjected to or witnessing traumatic events is a common pre-migration experience for people from refugee backgrounds. Traumatic experiences have been associated with mental health problems such as post-traumatic stress disorder (PTSD), major depression and anxiety [3,4,5]. A systematic review of literature [6] suggests that 9% of adults and 11% of children from refugee backgrounds resettled in western countries report symptoms consistent with post-traumatic stress disorder; around ten times prevalence rates for the general population. While research examining relationships between pre-migration trauma and post-migration psychopathology suggest dose–response correlation [7], with greater exposure to trauma associated with higher levels of PTSD symptoms, the relationship between trauma and PTSD remains complex.
Ethnicity and gender appear to interact with psychological distress following traumatic events [8,9]. Davidson, Murray and Schweitzer [10] pointed to variation in the incidence of specific clinical disorders across refugee populations. The impact of culture on belief systems and on the experience and expression of distress [11,12] mean that different ethnic groups may vary in their appraisal and response to traumatic events. In addition, gender has been found to impact mental health outcomes. For example, in a group of Sudanese refugees resettled in Australia for under two years, female gender predicted greater PTSD, depression and anxiety symptoms [9].
Previous research suggests post-migration stress also affects psychological well-being. Recent research in Sweden examined impacts of previous trauma and resettlement stress on recently settled Middle Eastern refugees’ mental health [13]. While previous trauma contributed 22% of the variance in predicting PTSD symptoms, resettlement stressors contributed 24% of the variance of depression, anxiety and somatization. Findings are consistent with Australian research by Schweitzer et al. [9] who reported that level of post-migration living difficulties predicted anxiety and somatization. Poorer outcomes have been found for females with prior high economic status or from rural backgrounds [14].
Successful settlement of refugees requires that government bodies and service providers respond effectively to the mental health needs of newly arrived people. While previous research points to the potential vulnerability of new arrivals [9,15,16], there exists little research into the mental health of people from Burma refugee backgrounds. In addition, an early study assessing the mental health of 104 Burmese political dissidents living in exile in Thailand [17] found high levels of depression (38%), as measured by the Burmese version of the Hopkins Symptom Checklist 25 (HSCL-25) [18]. The study also found high levels (23%) of PTSD symptoms as assessed by the Harvard Trauma Questionnaire (HTQ) [19]. Consistent with findings by Allden et al. [17], a more recent study by Lopes Cardozo et al. [20], which documented the mental health of 495 Karenni refugees residing in Thai camps, reported high levels of depression (42%) and anxiety (41%), as well as physical complaints. Surprisingly, PTSD symptoms were lower (4.6%) than for other refugee populations, such as Cambodian refugees (37.2%) in the Thai-Cambodian border camps, also assessed by the HTQ [21].
To our knowledge, the mental health status of refugees from Burma recently resettled in Australia has not been documented. On humanitarian grounds, Australia is currently committed to the intake and settlement of approximately 13 750 refugees in 2010 [2]. Further, Australia's DIAC is dedicated to managing the settlement of people from refugee backgrounds in ways that promote social and economic benefits to Australia. Australia's humanitarian and socio-economic interests mean that responding to the mental health needs of people resettling in Australia after forced migration is a primary concern [22]. Research determining the predominant mental health issues of this population, as well as the contributions of gender, pre-migration and post-migration factors to psychological well-being has potential to inform policy and practice which seeks to enhance the welfare of vulnerable and trauma-affected populations more widely. The aims of the present study were to identify the mental health status of newly arrived refugees from Burma, and to determine the contributions of gender, pre-migration trauma and post-migration living difficulties to mental health status. Based on previous research investigating the mental health status of other refugee groups outlined above, the following hypotheses were made.
Hypothesis 1: Female gender would predict higher levels of PTSD, depression and anxiety symptoms.
Hypothesis 2: A greater number of trauma experiences would predict higher levels of PTSD, depression, anxiety and somatic symptoms.
Hypothesis 3: A higher level of post-migration living difficulties would predict higher levels of PTSD, depression, anxiety and somatic symptoms.
Method
Participants
Participants were 70 individuals (40 females; 57.1%), with a mean age of 34.13 years (SD = 13.88; range = 18–80 years) from Burmese refugee backgrounds, who: (i) had recently arrived in Australia as part of the Australian offshore humanitarian programme with a mean time in Australia of 3.61 months (SD = 2.36 months; range 2–16 months); (ii) were aged over 18 years old, and; (iii) had provided voluntary informed consent to participate in the research. Individuals were recruited through the assistance of a non-government agency, funded by DIAC to assist refugees’ initial settlement. The agency receives all newly arrived refugees who are allocated for settlement in a specified Brisbane location and is responsible for their orientation programme, housing and, where indicated, counselling. Individuals were recruited consecutively over a 7-month period, and comprised 93% of adult clients allocated to the settlement service.
Materials
Demographic characteristics
Participants gave permission for the researchers to use the demographic information already available through the service agency. Information accessed included name, gender, age, visa type, marital status. highest education level, previous occupation, country of origin, ethnic group, language and date of arrival in Australia.
Harvard Trauma Questionnaire
The HTQ [23] is a measure of trauma experience and symptoms. It was specifically designed for use with refugee populations and has been used widely in refugee research, including studies examining the mental health of Burmese refugees [17,20]. In the current study the HTQ symptom scale had good internal reliability, with Cronbach's alpha of 0.89.
Hopkins Symptom Checklist-37
The HSCL-37 is a self-report inventory which measures symptoms along three subscales: anxiety (10 items), depression (15 items) and somatization (12 items). The HSCL is a valid and reliable index across diverse refugee populations [24]. The HSCL-37 was found to have good reliability in the current study with a total scale Cronbach's alpha of 0.92 and subscale alphas for anxiety (0.83), depression (0.83) and somatization (0.8).
Post-migration Living Difficulties Checklist
The Post-migration Living Difficulties Checklist comprises a series of questions relating to post-migration stressors and has been used in previous studies examining the mental health of refugees, asylum seekers and temporary protection visa holders [9,15,25]. The items cover areas commonly identified as difficulties by refugees in Australia [26,27]. Since each item is considered as a separate stressor, the notion of internal reliability is not applicable.
Procedure
After receiving ethical approval through the university Human Research Ethics Committee counsellors working for the partner organization provided new clients with information about the research along with an invitation to participate. Where the client expressed interest in research participation, the counsellor referred the client to the researcher or facilitated a meeting with the researcher. Cognizant of potential vulnerabilities, client and participant welfare was prioritized throughout the research process. The researcher and counsellors worked with interpreters to ensure optimal communication and ethical processes. Where clients provided informed consent to participate, the researcher worked with interpreters and participants to complete the battery of questionnaires, usually over two or three 1-h sessions at the office of the settlement organization.
Analysis
Following preliminary descriptive, assumption and correlation analyses, a series of hierarchical multiple regression analyses examined the relative contributions of gender, pre-migration trauma and post-migration living difficulties on traumatization, depression, anxiety and somatization. For each symptom outcome: gender was entered at step 1; number of trauma events personally experienced was entered at step 2, and; level of post-migration living difficulties was entered at step 3.
Results
Participant characteristics
Table 1 shows participants’ self-identified religious, ethnic and language groups. The majority of participants were Christians from Karen ethnic and language backgrounds. Table 2 shows the participants’ visa, marital and educational status. Participants came to Australia on refugee (90%) or women at risk visas (10%). The majority identified themselves as married (53%), single (36%) or widowed (9%). While most had secondary (47%) or primary education (37%), a significant proportion had no education (13%).
Demographic characteristics as a proportion of the Sample (N = 70)
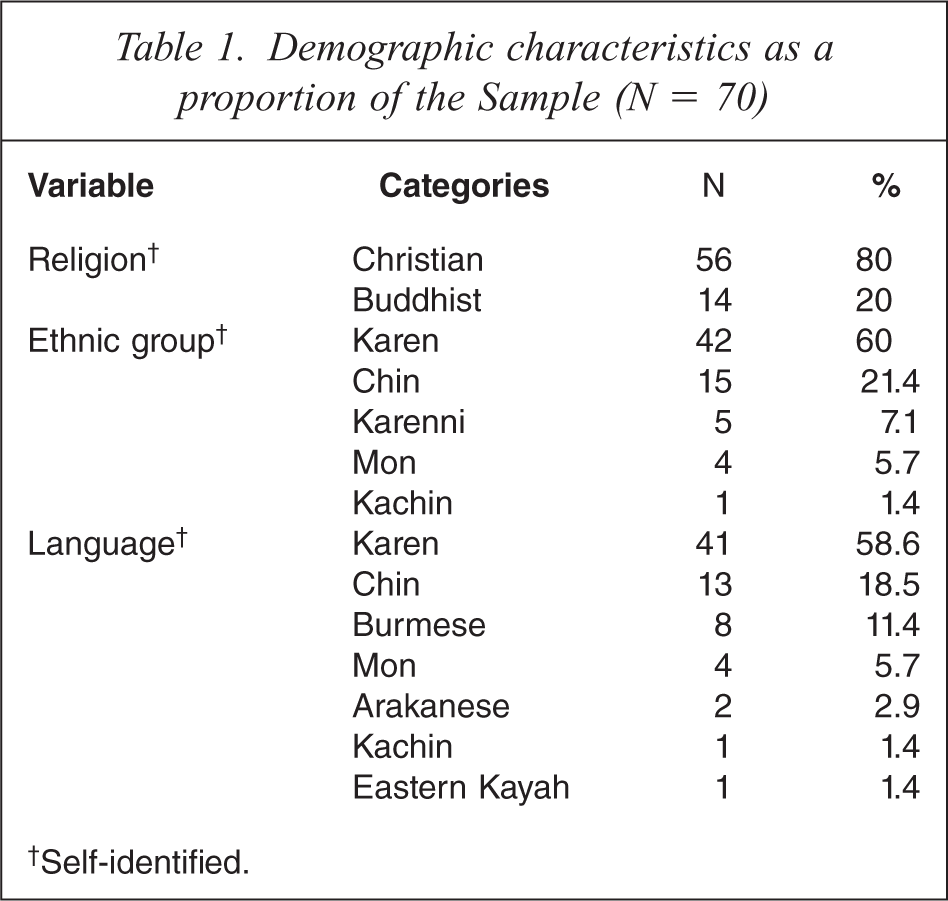
†Self-identified.
Participant characteristics as a percentage of the sample (N = 70)
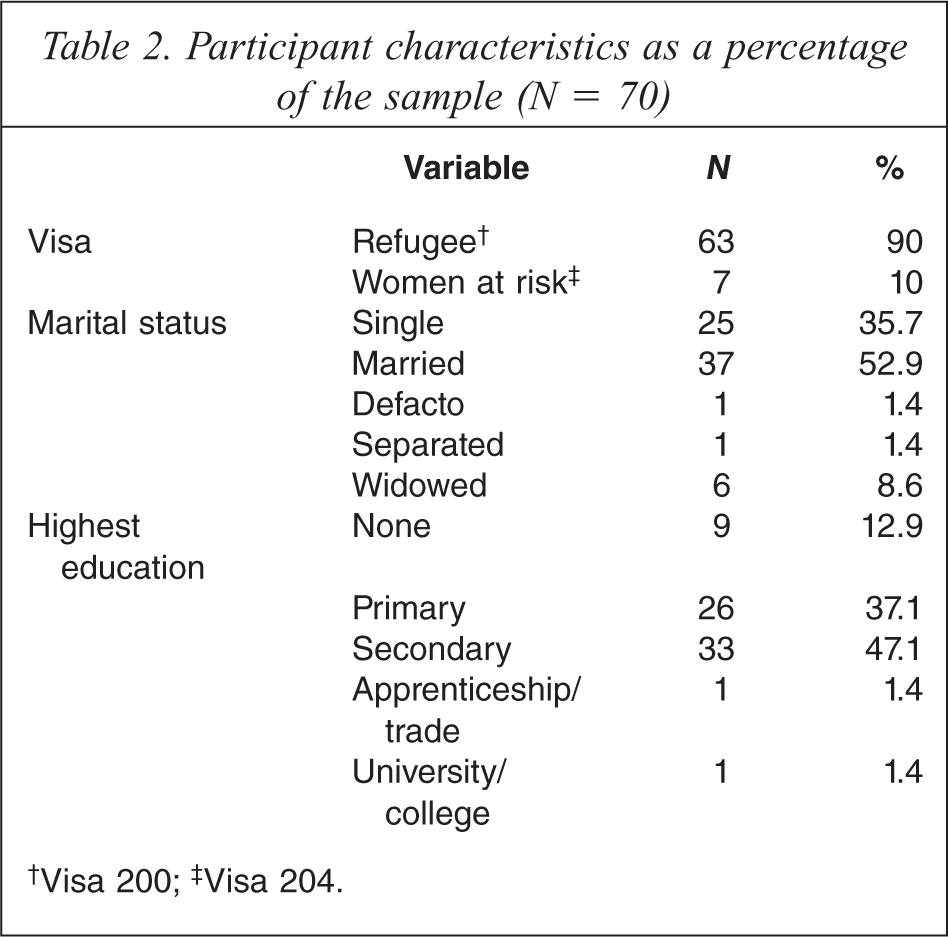
†Visa 200;‡ Visa 204.
Participants’ experience of traumatic events
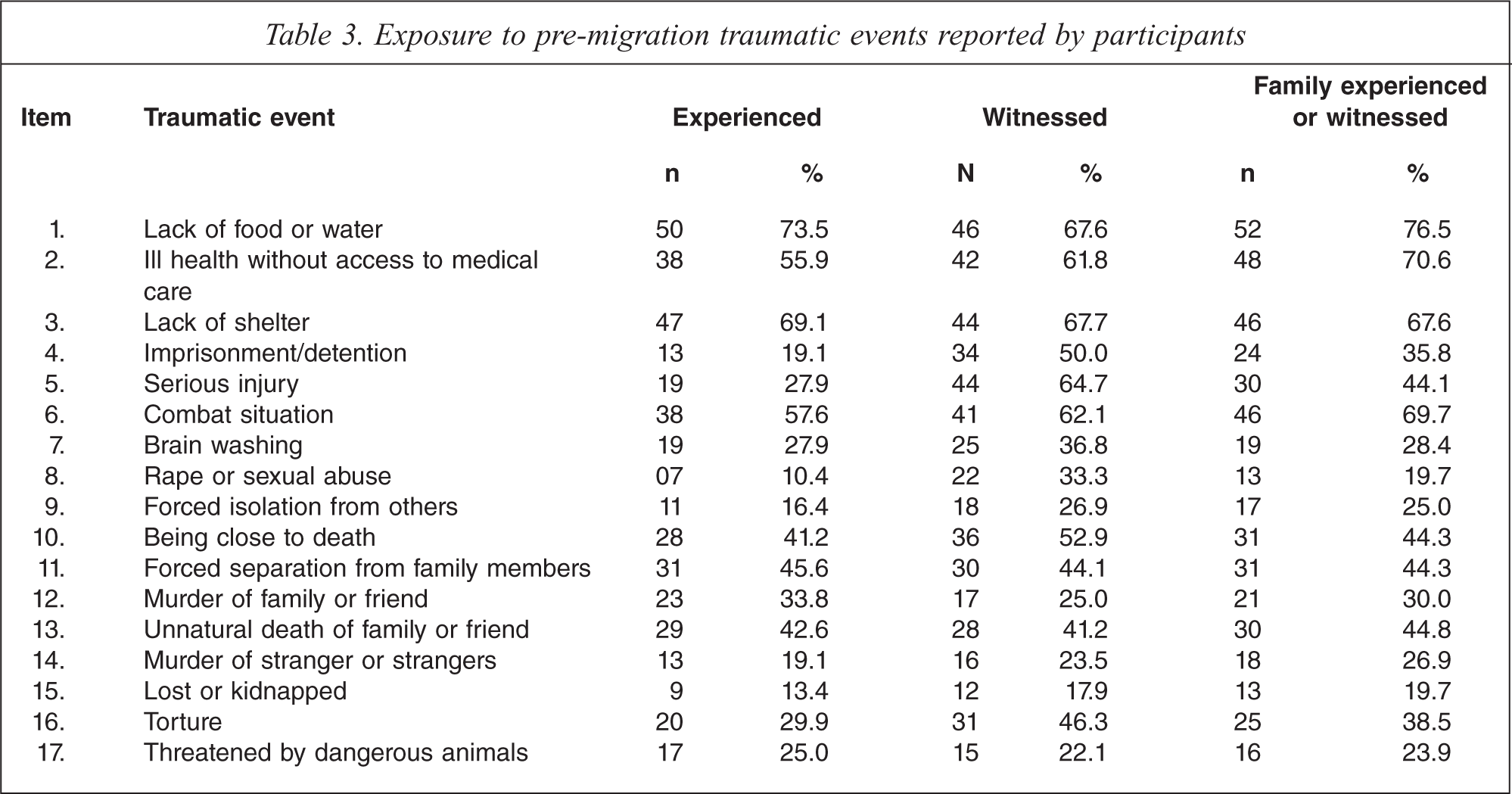
Table 3 shows the exposure to traumatic events experienced or witnessed by participants and their families. The most frequent types of personally experienced trauma reported were lack of food or water (74%), lack of shelter (69%), combat situations (58%) and ill health without access to medical care (56%). Participants also reported high levels of witnessing others experiencing traumatic events, including serious injury (65%), torture (46%) and rape (33%), or that their families had experienced or witnessed traumatic events.
Exposure to pre-migration traumatic events reported by participants
Participants’ post-migration living difficulties
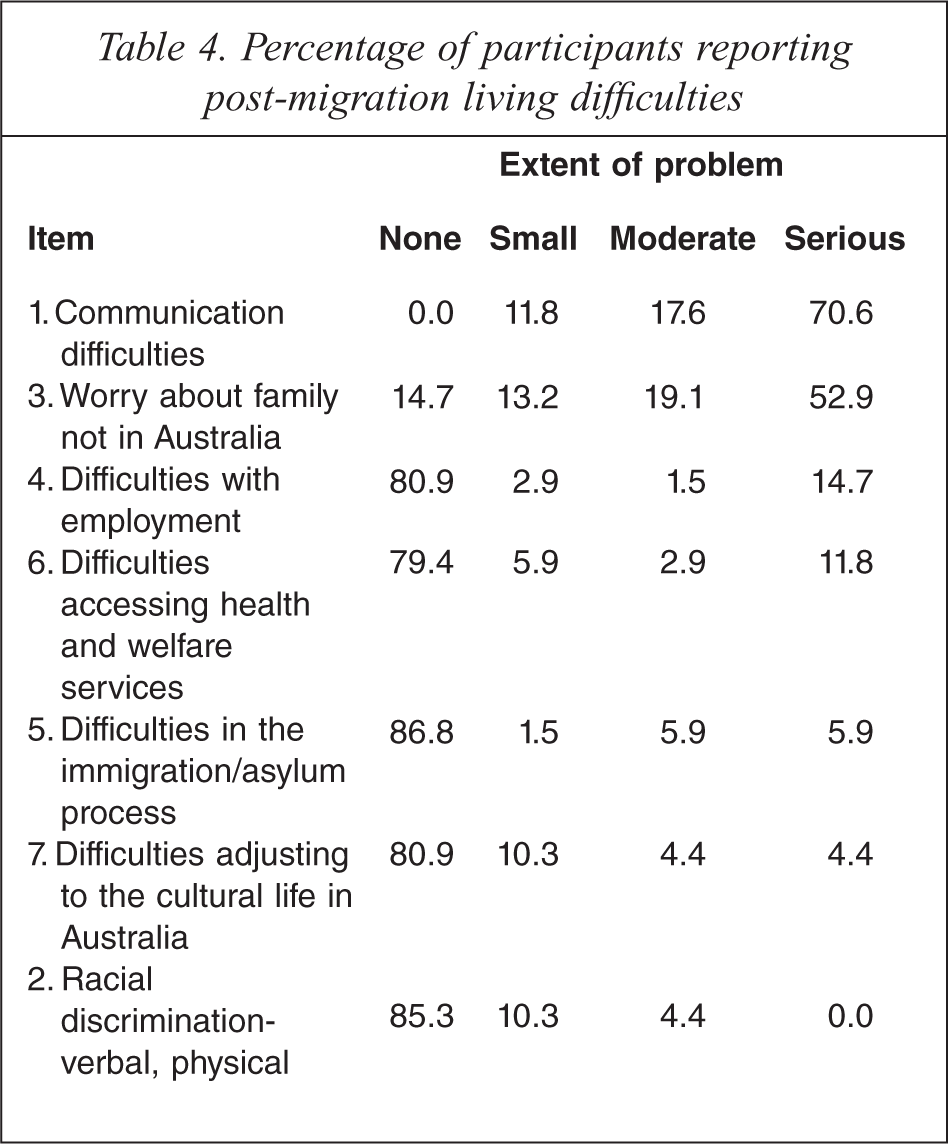
Table 4 presents proportions of participants experiencing a range of post-migration living difficulties since arrival in Australia. All participants reported communication difficulties; 71% reporting this as a serious difficulty. A majority of participants (72%) reported worrying about family not in Australia as causing moderate or serious difficulty. All participants arrived in Australia on refugee or women at risk visas and the majority of people (87%) reported no problems with immigration processes.
Percentage of participants reporting post-migration living difficulties
Participants’ mental health status
Table 5 shows proportions of participants’ psychological distress, as well as mean scores and standard deviations, as indicated by reported trauma symptoms on the HTQ [23] and reported symptoms of anxiety, depression and somatization on HSCL subscales [18]. Significant proportions of participants reported experiences symptomatic of trauma (26%), anxiety (20%), depression (36%) and somatization (37%). Based on the application of DSM-IV criteria to HTQ symptoms, nearly 9% of participants reported trauma symptoms that were consistent with meeting the diagnostic criteria of post-traumatic stress disorder (PTSD).
Percentage of participants reporting symptoms of psychological distress
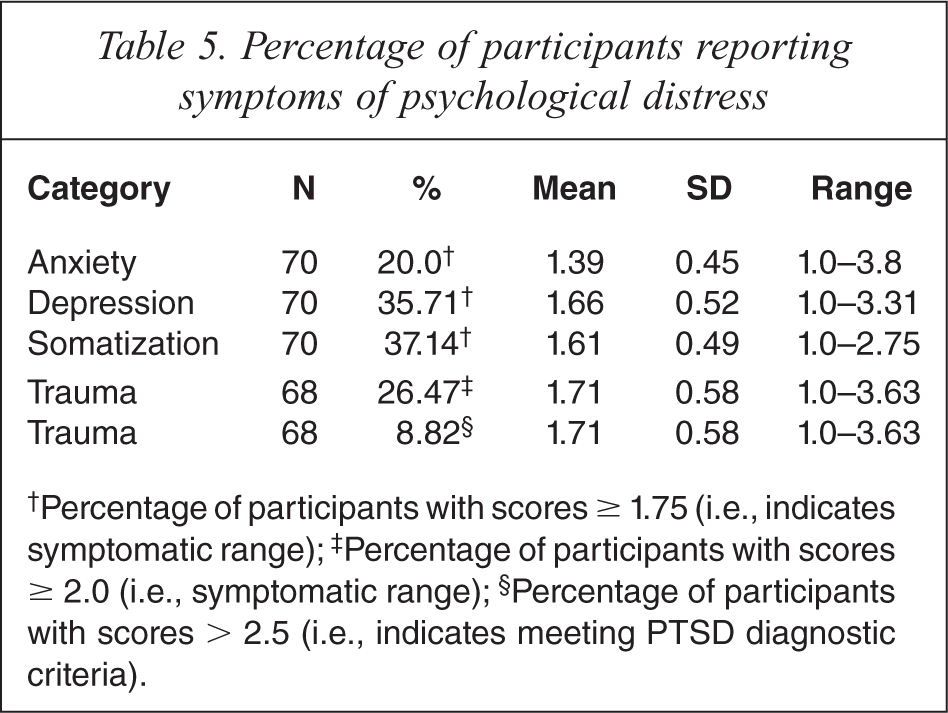
†Percentage of participants with scores ≥ 1.75 (i.e., indicates symptomatic range);‡ Percentage of participants with scores ≥ 2.0 (i.e., symptomatic range);§ Percentage of participants with scores > 2.5 (i.e., indicates meeting PTSD diagnostic criteria).
Correlations
Since univariate score distributions for traumatization, depression and anxiety were positively skewed, correlation analysis used Spearman's Rank Order Correlation to calculate the strength of relationships among predictor and outcome variables (Table 6). Correlation coefficients suggested that symptoms of traumatization, anxiety, depression and somatization were strongly and positively correlated. Gender was not significantly related to pre-migration, post-migration and symptom variables and the magnitude of correlations was small. Pre-migration trauma events were correlated with post-migration living difficulties, somatization and traumatization, but not with depression, anxiety or gender. Post-migration living difficulties were correlated with traumatization, depression, anxiety, and somatization.
Summary of bivariate inter-correlations among predictor and outcome variables using Spearman's rank order analysis
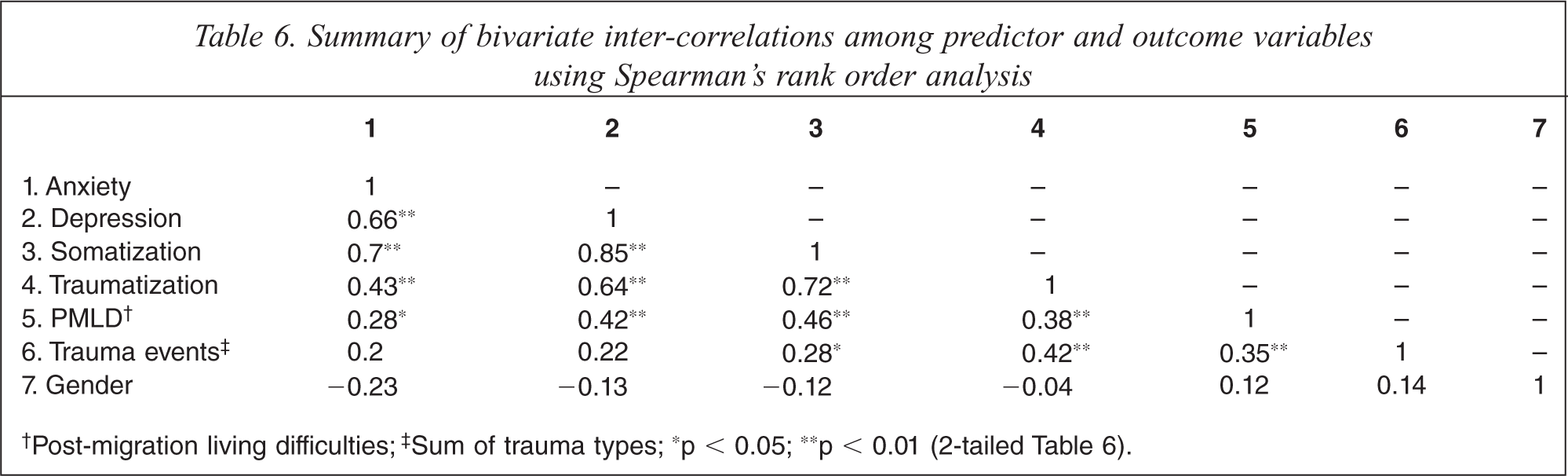
†Post-migration living difficulties;‡ Sum of trauma types; ∗p < 0.05; ∗∗p < 0.01 (2-tailed Table 6).
Predictors of mental health symptoms
Considering that regression analysis is generally robust to violation of univariate normality, focus was on assumptions relevant to regression analyses. Examination of residual scatter plots of the regression on the anxiety symptom scores identified violation of the assumption of heteroscedasticity, which was rectified by square root transformation of anxiety scores. Since substantive results from transformed analyses did not differ from untransformed analyses, results from untransformed scores are reported. Table 7 displays results from the regression analyses. The models for each symptom outcome are described below.
Hierarchical multiple regression analyses predicting trauma, depression, anxiety and somatization symptoms
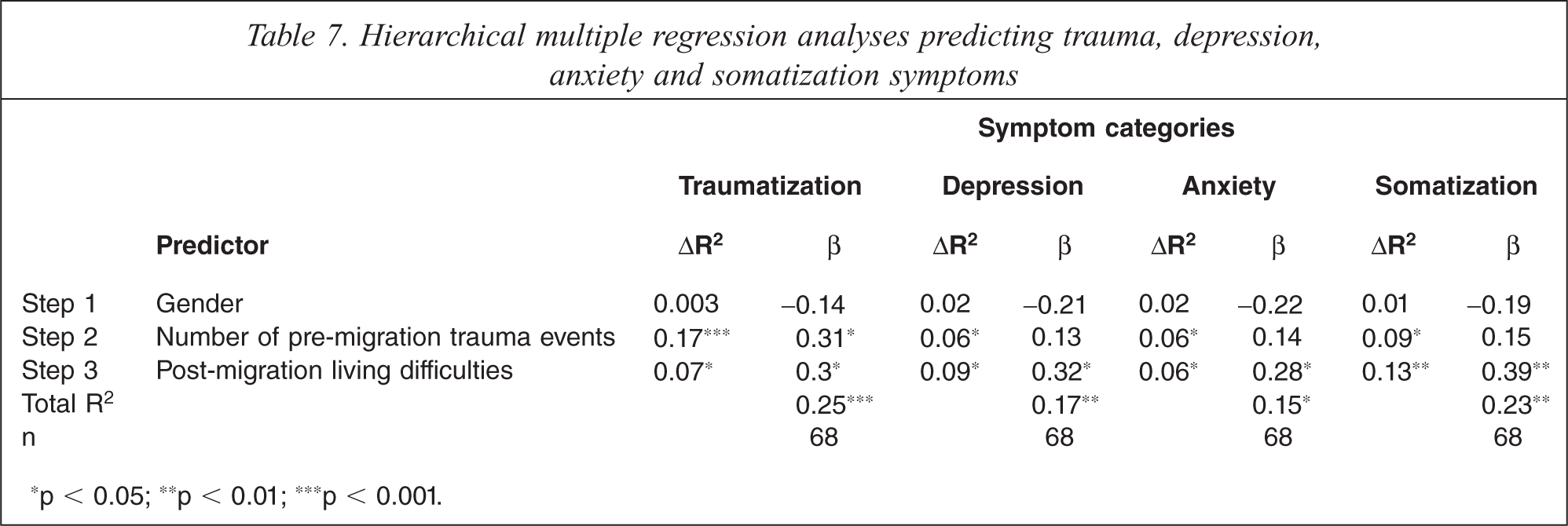
∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Traumatization
The overall model, including gender, number of trauma events and post-migration living difficulties, was significant, F(3, 64) = 7.06, p < 0.001, accounting for 24.9% of the variance in traumatization scores. Exposure to traumatic and post-migration living difficulties each explained additional variance in traumatization scores when added to the model. Traumatic events and post-migration living difficulties made statistically significant unique contributions to traumatization symptoms, but gender did not.
Anxiety
The overall model, including gender, number of trauma events and post-migration living difficulties, was significant, F(3, 64) = 3.68, p = 0.016, accounting for 14.7% of the variance in anxiety scores. Exposure to traumatic and post-migration living difficulties each explained additional variance in anxiety scores when added to the model. Post-migration living difficulties made a statistically significant unique contribution to anxiety symptoms, but the number of trauma events did not. Gender made a unique contribution to anxiety only at p = 0.07.
Depression
The overall model, including gender, number of trauma events and post-migration living difficulties, was significant, F (3, 64) = 4.34, p = 0.008, accounting for 16.9% of the variance in depression scores. Exposure to traumatic and post-migration living difficulties each explained additional variance in depression scores when added to the model. Post-migration living difficulties made a statistically significant unique contribution to depression symptoms, but trauma events did not. Gender made a unique contribution only at p = 0.08.
Somatization
The overall model, including gender, number of trauma events and post-migration living difficulties, was significant, F(3, 64) = 6.33, p = 0.001, accounting for 22.9% of the variance in somatization scores. Exposure to traumatic and post-migration living difficulties each explained additional variance in somatization scores when added to the model. Post-migration living difficulties made a statistically significant unique contribution, but trauma events did not make a significant unique contribution. Gender made a unique contribution only at p = 0.09.
Discussion
The aims of this study were to identify the mental health status of newly arrived refugees from Burma, and to determine the contributions of gender, pre-migration trauma and post-migration living difficulties to mental health symptoms. Significant proportions of participants reported psychological distress in symptomatic ranges, including PTSD (9%), anxiety (20%) and depression (36%). Many reported symptoms of substantial traumatization (26%) and somatization (37%). Contrary to the first hypothesis, gender did not predict symptom outcome. The second hypotheses received only partial support: the level of exposure to pre-migration traumatic events predicted trauma symptoms, but not anxiety, depression or somatization. Findings supported the third hypothesis: post-migration living difficulties predicted mental health symptomatology, making unique contributions to traumatization, anxiety, depression and somatization.
Pre-migration trauma
Newly arrived Burmese people, participating in this study, reported being exposed to multiple and severe pre-migration traumas. Such exposure is consistent with the experience of Karenni refugees living in Thai-Burmese border camps reported by Lopes Cardozo et al. [20], and similar to reports from other refugee populations who have fled from ethnic and military conflict [9]. The current research used a shortened 17-item version of the HTQ events schedule, and one significant item omission was ‘forced labour’ which emerged frequently in conversations and was endorsed by 34% of Karenni refugees in previous research [20].
Post-migration living difficulties
Participants reported experiencing a range of post-migration living difficulties. All participants reported problems with communication, with 71% reporting this as a serious difficulty. A majority reported that worrying about family not in Australia caused moderate to serious difficulty. Anecdotally, compromised communication exacerbated participants’ worries about future employment and educational opportunities, and underpinned many of their concerns about accessing health and welfare services. The difficulty was related to concerns that doctors often did not use interpreters, or used phone interpreters inadequately, to the extent that the new arrivals were fearful of incorrect diagnoses and medication.
Difficulties around communication were consistent with research by Momartin et al. [15], which also found this to be the primary concern of Persian-speaking refugees residing in Australia for an average of three months. In contrast, people from Middle East refugee backgrounds, settled in Sweden for an average of 12 months (SD = 8.1 months) reported worries about family abroad as their major concern [13]. Concerns of newly arrived Burmese refugees can also be compared with those of Sudanese refugees, 35% of whom had been in Australia for two years or more [9], who reported worry about family not in Australia, difficulties with employment and adjusting to the cultural life in Australia.
Results are consistent with Gonsalves’ early arrival and destabilization stages of resettlement [28], which highlights the importance of individuals learning the language of the land. Migrants, however, remain involved with their homeland; often experiencing guilt about those left behind. Based on the work of Grove and Torbiorne [29], Burmese refugees were likely embedded in their own cultural frame of reference, perceiving cultural differences of their new country as ‘quaint’ or ‘fascinating’ (p. 214), although this needs further qualitative investigation.
Mental health
Significant proportions of participants reporting psychological distress in symptomatic ranges underlines the need for services. While acknowledging the imperative to address the distress of individuals who are experiencing PTSD symptoms, findings reveal the importance of avoiding ubiquitous assumptions of PTSD and instead attending to the range of practical and psychological needs of people from refugee backgrounds.
Burmese refugees were experiencing levels of psychological distress substantially higher than 12-month prevalence rates in the general Australian population for generalized anxiety disorder (2.7%), depression (4.1%) and PTSD (6.4%) [30]. Perhaps understandably, given less certainty about their future, previous research of Karenni refugees in the Thai–Burma border camps by Lopes Cardozo et al. [20] found much higher prevalence of anxiety (41%) and slightly higher prevalence of depression (42%) compared to the current study. Investigating the mental health of south-east Asian refugees in the United States, Kinzie and Manson [31] reported that 49% presented primarily with depression. Based on positive associations of anxiety and depression symptoms with post-migration living difficulties found in the current study, it is possible that higher levels of depression and anxiety found in the Thai camps and in the United States may relate to a greater level of post-migration living difficulties in those contexts. The positive relationship between post-migration living difficulties and symptomatology found in the current study is consistent with previous research with a sample of south-east Asian refugees [32], which found a lack of English proficiency associated with depression, and concluded that language skill may act as a stress buffer on mental health during resettlement.
High prevalence of somatization (37%) is consistent with high levels of physical symptoms found in the Thai–Burma border camps [20] and high levels of somatic complaints (39%) reported by south-east Asian refugees in the USA [31]. High levels of somatization in south-east Asian populations may relate to a culturally nuanced expression of distress and may underpin lower levels of anxiety, depression and traumatization scores reported by recently arrived Burmese people compared to people from Persian-speaking backgrounds, recently resettled in Australia for a similar period [15]. Compared with the HSCL and HTQ anxiety depression and traumatization symptom scores of people from Persian-speaking refugee backgrounds [15], recently arrived Burmese people reported lower levels of anxiety depression and traumatization.
PTSD rate in the current study was consistent with the 9% rate found in a systematic review of 6743 adult refugees across seven western countries [6] and with the 10% rate found in an investigation of 2773 south-east Asian refugees in California [33]. This level was lower than the 13% rate for Sudanese refugees resettled in Australia for less than 2 years [9], 23% rate reported for Burmese political dissidents living in exile in Thailand [17] and the 37.2% rate for Cambodian refugees in the Thai-Cambodian border camps [21]. High PTSD rates of other groups may reflect higher pre-migration exposure to trauma or may reflect culturally specific responses to traumatic events. Alternatively, higher PTSD proportions may represent impacts from post-migration living difficulties, given existing pre-migration vulnerabilities. If the latter explanation is possible, a post-migration PTSD rate higher than the 4.6% rate for Karenni refuges in the Thai–Burma border camps [17] could reflect a type of stress-diatheses in which post-migration living difficulties experienced by newly arrived Burmese people exacerbates existing vulnerability resulting from previous trauma.
Contributions of gender, pre-migration trauma, post-migration living difficulties to mental health symptoms
Findings from the current study revealed that levels of pre-migration trauma and post-migration living difficulties both play significant roles in the mental health of recently arrived refugees from Burma. Gender was not associated with levels of traumatization or post-migration living in the group of participants from Burma, and in contrast to previous research with Sudanese refugees [9], did not predict mental health symptoms.
While exposure to traumatic events impacted on participants’ mental well-being, post-migration living difficulties had greater salience in predicting mental health outcomes of people from Burmese refugee backgrounds. The finding that exposure to pre-migration traumatic events predicts traumatization symptoms is consistent with previous research [3,4,5,7]. Findings from the current study revealed that post-migration living difficulties made a unique and almost equal contribution as traumatic events in predicting trauma symptoms. While pre-migration traumatic events did not make a unique significant contribution to anxiety, depression and somatization symptoms with this group of participants, difficulties of post-migration living predicted these mental health symptoms. Findings from the current study underline the role of post-migration stressors in creating mental health problems and raise the possibility of a type of stress diathesis in which post-migration living difficulties may trigger or exacerbate existing predisposition to PTSD caused by exposure to pre-migration trauma.
Findings from the research are limited by several factors including the small number of participants and potential bias in relation to the recruitment of participants. As participation was voluntary, some self selection bias may be present. A larger sample size would provide greater confidence in the generalizability of findings. Because of the diverse range of languages across the different ethnic participant groups, the research relied on interpreters, raising potential inconsistency in the questionnaire administration. Results are limited by reliance on questionnaire methodology, particularly salient in the context of research with people from culturally and linguistically diverse backgrounds in relation to social constructions of different pathologies.
We acknowledge that the conceptualization of disorders within the cultural context draws upon western models of psychopathology, and we hope in further publications to describe some of the culturally related phenomenon that pertain to people from this refugee group. Despite these concerns, the measures used have been used successfully across diverse cultural populations and in the current study the questionnaires had face validity in distinguishing between different pathologies. While debate on the use of empirical questionnaires in culturally and linguistically diverse populations continues, rather than assuming the presence of traumatization and implementing potentially aversive interventions such as exposure therapy, the current findings speak to the importance of a comprehensive and culturally sensitive assessment of psychological distress in refugee populations so that therapists may implement appropriate and effective intervention.
Footnotes
Acknowledgements