
Abstract
Objectives:
This study aimed to assess the association of the quality scores of hotline psychological intervention and the reduction of subsequent suicidal acts among high suicidal risk callers.
Methods:
High-risk callers at a national crisis hotline service in China were recruited and prospectively followed for up to 3 months after receiving a hotline psychological intervention. The quality of the intervention was evaluated by supervisors who listened to the tape-recorded calls using the Counseling Skills Rating Scale for Psychological Support Hotlines, which assessed three counseling domains: process, attitude and communication skill. The primary outcome was the occurrence of suicidal acts during the follow-up period. Secondary outcomes were before versus after changes during the intake intervention call in hopefulness, psychological stress and suicide intention reported by the callers.
Results:
Over the 3-month follow-up, 45 of 778 high-risk callers reported 61 suicide attempts, and 3 other callers died by suicide. Subsequent suicidal act was significantly more common in callers classified as being at higher risk during the intake call. Higher scores on the quality of suicidality assessing of the Counseling Skills Rating Scale for Psychological Support Hotlines were associated with reduced risk of suicidal acts during follow-up (hazard ratio = 0.38, 95% confidence interval = [0.18, 0.85]). Higher scores on the communication skill domain were associated with increases in hopefulness (β = 0.09) after the intervention, and higher scores on the counseling process domain (β = −0.12) and higher suicidal risk scores (β = −0.12) were associated with decreased suicide intention after intervention.
Conclusion:
Several characteristics of a hotline intervention for suicide prevention were associated with decreased risk of suicidal acts during follow-up. Intervention skill training for hotline operators should emphasize these specific counseling skills.
Introduction
In 2016, suicide accounted for nearly 800,000 deaths worldwide, 80% of which occurred in low- and middle-income countries (LMICs) (World Health Organization [WHO], 2019). In China, there are about 100,000 suicide deaths per year (Jiang et al., 2018), and more than 6 times individuals presenting to hospitals due to suicide attempts (Tong et al., 2020).
Psychological interventions are important in suicide prevention, especially for psychiatric patients (Zalsman et al., 2016). Previous studies report that several interventions such as multisystemic therapy (Huey et al., 2004), cognitive therapy for suicide prevention (Brown et al., 2005) and collaborative assessment and management of suicidality (CAMS; Jobes, 2017) are effective in reducing suicidal behaviors. However, negative attitudes and the stigmatization of suicide (Reynders et al., 2014) combined with the limited availability and high costs of psychological services (Han et al., 2018) limit care-seeking among individuals at high risk of suicide. For many, the confidentiality (Coveney et al., 2012; Hunt et al., 2017) and accessibility (Bobevski et al., 1997; King et al., 2003) of free services provided by crisis hotlines is an attractive alternative. Previous studies report that hotline-based psychological crisis services are perceived by users to be helpful (Coveney et al., 2012) and are effective in reducing depression, suicidal thoughts and suicidal behaviors (Donohue et al., 2014; Gould et al., 2007; King et al., 2003; Mishara and Daigle, 1997), although the effectiveness of helpline support on reducing suicide death needs further investigation (Zalsman et al., 2016).
Factors associated with the effectiveness of hotline-based suicide prevention services include the counseling skills of the operator (Bobevski et al., 1997; Gould et al., 2017; Mishara and Daigle, 1997; Mishara et al., 2007b) and whether follow-up calls are made to high-risk callers (Gould et al., 2017). Callers’ assessed intent to die at the time of the intake calls is also associated with hotline call outcomes (Gould et al., 2007). Thus, available research supports the notion that standardized training programs focused on improving the quality of the psychological intervention provided during the crisis call is the key to effectively preventing suicidal behavior via hotline services (Draper et al., 2015; Gould et al., 2013; Mishara et al., 2007a). A major limitation of research on evaluating the effectiveness of crisis hotline services is that small samples and short follow-up times make it necessary to use proxy measures of suicidal behavior—depression, hopelessness, suicidal ideation etc.—that may not be sensitive predictors of fatal or non-fatal suicidal acts. Another problem with current research on crisis hotlines is the role of suicidal risk level has on the effectiveness of the intervention conducted over the crisis line.
Since it was established in 2002, the Beijing Psychological Support Hotline has fielded more than 400,000 calls; more than 10% of which involve callers who acknowledge a history of self-harm (Tong et al., 2019). In 2017 we developed a Counseling Skills Rating Scale for Psychological Support Hotlines (CSRSPSH) to provide a detailed assessment of the quality of hotline-based counseling (Liang et al., 2017). In this study, hotline callers deemed to be at high risk of suicidal behavior were followed up to identify whether they attempted suicide or died by suicide in the 3 months after the hotline intervention, and the quality of the intake hotline counseling intervention was assessed using the CSRSPSH. We aimed to identify characteristics of the hotline intervention associated with the reduction of suicidal acts among callers. The findings have key implications for the development of effective suicide prevention strategies in LMICs with limited resources where telephone-delivered psychosocial intervention represents a feasible and effective option (Baker et al., 2018).
Methods
Design, setting and participants
The study was conducted at the Beijing Psychological Support Hotline which provides services to callers from around China, three-fourths of whom live outside of the Beijing Municipality. Hotline operators are full-time employees with a psychology or psychiatry background who receive at least 3 months full-time training in the provision of hotline services before independently taking calls. The standard call includes collecting basic demographic information followed by an assessment of the level of hopelessness, psychological stress, suicidal intent and overall risk of suicidal behavior.
‘High suicidal risk callers’ who met the following criteria were consecutively recruited from 14 January to 31 December 2015: (1) score ⩾8 on the suicide risk scale (described below) (Tong, 2019) or operator considered caller at immediate risk of suicide (and, thus, skipped completion of the suicide risk scale); (2) total call time lasted >10 minutes; (3) caller agreed to be tape-recorded; (4) at the ending of the psychological intervention, caller agreed to participate in the follow-up assessments. If a caller had more than one eligible call during the enrollment period, only the first call was considered.
All callers assessed as high suicidal risk were immediately provided a semi-structured psychological intervention aimed at decreasing the caller’s suicidal risk that took up to 90 minutes (described below). The quality of the tape-recorded intervention was assessed by hotline supervisors who were blind to the subsequent outcome of the caller (i.e. with or without subsequent suicidal act) using the CSRSPSH.
The occurrence of subsequent suicidal acts, including suicide or suicide attempt, was assessed at each follow-up call. The information of suicide death was obtained from the family members of died callers, and the data of suicide attempt were provided by callers themselves.
Intervention and follow-up
We developed a semi-structured crisis line-based intervention for high-risk callers based on the principles and suggestions of previous studies (Gould et al., 2007, 2013; Mishara et al., 1997, 2007a, 2007b) and adapted for Chinese cultural factors. Overall, operators are taught to use active listening, show empathy and respect and provide emotional support to callers. After assessing caller’s suicidal risk, operators focus on non-directive and collaborative problem-solving and discuss feasible coping strategies for dealing with the adversities that are precipitating suicidal risk. For callers at imminent risk of attempting suicide, operators employed a variety of strategies including creating a safety plan with the caller; making contact with the caller’s family members, friends or police; or developing a collaborative agreement to not engage in suicidal act (Box 1).
Key elements of the hotline-based intervention for high-risk callers.
At the end of the intake call, the operator would discuss the planned telephone follow-up schedule: 1 day, 1 week, 1 month and 3 months after the intake call. In each of the scheduled follow-ups, the operator would provide emotional support, ask about whether the caller had suicidal ideation and provide psychological intervention if necessary. To assess the occurrence of suicidal act over follow-up, operators would also ask, ‘Have you attempted suicide since [the date of intake call]?’ If callers could not be contacted, family members who answered the follow-up call were inquired about whether the caller engaged in fatal suicidal acts, and an updated follow-up schedule was made for those living callers. For each scheduled follow-up time point, if the caller could not be contacted for 3 times, it would be coded as ‘lost’, and the operators would try to contact the caller again at the next scheduled follow-up time point until the caller was dead or after 90 days of the intake call.
Measures
The suicidal risk of each caller was assessed by the operator at the beginning of the call, using a 12-item measure (i.e. suicidal ideation and plan, severe depression, acute life stress, chronic life events, alcohol and substance misuse etc.). The total score ranged from 0 to 16, with higher scores indicating greater suicidal risk. The intra-class coefficient (ICC) of inter-rater consistency of the total score of the scale was 0.93, and the kappa value of the 12 aspects of the scale ranged from 0.54 to 0.95 (Tong, 2019). In this study, a score of 8 or higher was defined as high suicidal risk, a cutoff point with sensitivity of 77% and specificity of 57% for subsequent suicidal acts (Tong, 2019). Occasionally, in the beginning of a call, operators believed that the caller was at immediate risk of suicide so the suicidal risk assessment would be canceled or broken off; such callers were also classified as ‘high-risk’ even though the risk scale was not completed.
Callers’ hopefulness, psychological stress and suicide intention were assessed by asking callers to rate ‘To what extent do you feel hopeful?’, ‘To what extent do you feel psychological stress?’ and ‘To what extent do you want to take your life?’, respectively (range of scores from 0 to 100). Callers were instructed that a score of 100 means that the individual felt completely hopeful, at the highest tolerable of psychological stress or definitely wanted to take his or her life. Callers were instructed that a score of 0 means that the caller felt completely hopeless, no psychological stress or definitely wanted to go on living. The three questions were asked twice per call, i.e. at the beginning of and at the end of the call. The responses of the questions of hopefulness and psychological stress at the beginning of the call were also included in the suicidal risk assessment. The hotline ‘call-on’ system has been developed to assist operators taking calls. While an operator answers a call, the system would present questions or cues with one or more blanks on a screen set before the operator. The operator fills in the blanks based on the information collected from the caller. The collected data are saved automatically, in accordance with designated format.
The CSRSPSH was used to evaluate the quality of several primary elements and skills of hotline-based psychological counseling services (Liang et al., 2017). The CSRSPSH consists of three domains that are assessed with 21 items. The first domain, counseling process, consists of nine items that focus on execution of the counseling intervention smoothly and fluently (i.e. establishing a counseling relationship, calming caller down, focusing on problems, transition to assessing suicidal risk, assessing suicidal risk, preparation for problem-solving, problem-solving, making a conclusion and ready for finishing counseling). The second domain, counseling attitude, consists of five items pertaining to the operator’s general attitude and demeanor (i.e. voice and tone, respect, sincerity, support and acceptance). The third domain, communication skill, consists of 7 items pertaining to foundational communication skills for hotline intervention (i.e. active listening, empathy, asking questions, confirming and feedback, normalization, empowering and without significant faultiness).
A 5-point Likert-type scale (i.e. 1 = poor, 2 = fair, 3 = moderate, 4 = good, 5 = excellent) was used in the CSRSPSH. The score of each domain was the sum of the scores of items in the domain. The structure validity and reliabilities of the CSRSPSH have previously been shown to be acceptable (Liang et al., 2017). In this study, seven trained and qualified hotline supervisors used the CSRSPSH to evaluate the counseling quality of the psychological interventions delivered in the baseline calls. The inter-rater reliabilities (ICC) of total score and scores of the three domains of the CSRSPSH ranged from 0.59 to 0.67 (Liang et al., 2017). While rating the quality of hotline psychological intervention, the supervisors were blinded to the primary outcome of the evaluated caller.
Data analysis
The primary outcome was suicidal acts, including suicide and suicide attempt that occurred during the 3-month follow-up. In this study, the first suicidal act was the focus of analysis. The recruited callers were divided into two groups, those with and without suicidal acts during the 3-month follow-up.
The secondary outcomes were changes in hopefulness, psychological stress and suicide intention from the beginning to the end of intervention at the intake call. The changes were defined as the scores of the three variables given by callers at the end of call minus the scores given at the beginning of the call, reflecting the immediate outcomes of hotline psychological intervention. Compared with the beginning score, a higher ending score of hopefulness (increasing), or a lower score of psychological distress or suicide intention (decreasing), indicated improvement attributed to the hotline intervention.
The baseline characteristics (i.e. sex, age, suicidal risk score, hopefulness, psychological distress and suicide intention) and the scores of the three domains and 21 items of the CSRSPSH were compared between enrolled callers who did and did not subsequently engage in suicidal acts using χ2 tests and t tests.
Cox proportional hazard regression analyses were used to assess factors associated with suicidal acts in the 3 months following a crisis call among high-risk callers. The date of the intake call was taken as time zero, with the time until the first suicide attempt, until suicide death or until the censoring (90 days after the intake call, or the last date of follow-up within 90 days) for those without suicidal acts in the 3-month follow-up. Two Cox regression models were examined. Age and sex, as common correlates of suicidal acts, were always included in the two models. Backward selection was used to determine other significant predictors. In model 1, other factors included in the initial model were suicidal risk score and the scores of three domains of the CSRSPSH. In model 2, other factors included in the initial model were suicidal risk score and the scores of those items of CSRSPSH with p values lower than 0.30 (Hosmer et al., 2013). We dichotomized the scores of the three CSRSPSH domains (counseling process, attitudes and communication skills), as low and high, based on the mean of the scores. The scores of the 21 items of the CSRSPSH were not dichotomized due to the limited score distribution. The proportionality of hazards assumption was examined by testing the correlation of Schoenfeld partial residuals and event time, and the results indicated that the assumption could not be rejected (all p > 0.05).
Multivariate linear regression analysis was conducted to identify factors associated with decreasing callers’ immediate suicidal risk after the hotline psychological intervention. The changes of hopefulness, psychological distress and suicide intention were dependent variables separately, and the scores of suicidal risk, counseling process, counseling attitude and communication skills, and age and sex were independent variables. The scores of the three domains of the CSRSPSH were continuous measures in the linear regression model. A stepwise method was used to select independent variables. Data analyses were conducted using SPSS 18.0.
The study was approved by the Institutional Review Board of Beijing Huilongguan Hospital (2014-105). The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. Prior to connecting to a crisis line counselor, callers were informed by voice message that all calls are tape-recorded and that data about the call would be collected and analyzed anonymously. The identity of the callers was de-identified before data analyses.
Results
The details of recruiting and following up process are shown in Figure 1. In brief, from 14 January to 31 December 2015, there were 1034 calls assessed as high suicidal risk. Among them, 40 were repeated calls from same callers, 19 lasted less than 10 minutes and one caller refused to be tape-recorded, yielding 974 distinct callers for this study. These callers received the hotline psychological intervention which was evaluated by supervisors using the CSRSPSH.
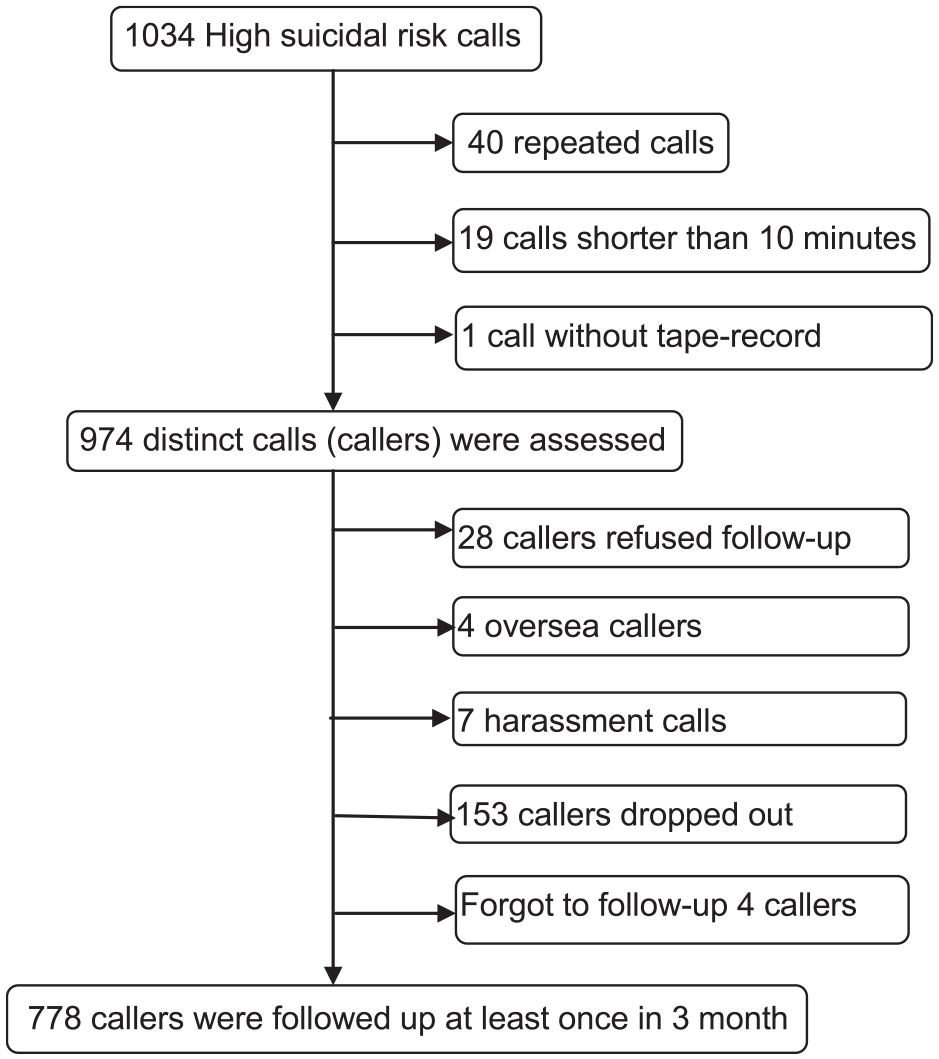
Flowchart of recruiting and follow-up high-risk callers.
In the 3-month follow-up period, 196 callers (20.1%) could not be contacted. There were no statistically significant differences between callers who were or were not followed up by sex (χ2 = 0.04, p = 0.846), age (28.68 vs 28.88, t = −0.30, p = 0.762), but the followed-up callers had a higher assessed level of suicide risk (9.38 vs 9.08, t = 2.46, p = 0.014). The remaining 778 (79.9%) callers were followed up at least once and were included in analyses including 381 males and 397 females. Of these individuals, 45 subjects including 27 males and 18 females made a total of 61 suicide attempts over follow-up, and 3 others died by suicide. Multiple attempts were made by six male callers (five for two episodes and one for four episodes) and four female callers (two for two episodes, one for three episodes and one for five episodes). All of the three suicide decedents were males. The difference in the likelihood of suicidal acts between male (30/381, 7.9%) and female (18/397, 4.5%) callers was a marginally statistical significance (χ2 = 3.75, p = 0.053).
Table 1 lists the baseline characteristics of callers including those who had suicidal acts over follow-up and those who did not. Callers who had suicidal acts in the follow-up period were younger than the callers who had not. Female high suicidal risk callers were marginally less likely to report suicidal acts during follow-up period. The suicidal risk score of the suicidal act group (9.85 ± 1.76) was higher than that of non-suicidal group (9.35 ± 1.53), and the difference was statistically significant (t = −2.14, p = 0.033). The callers in the suicidal act group also reported a higher suicide intention (74.84 ± 29.68) than the callers in the non-suicidal group (58.23 ± 33.38, p < 0.001). The level of hopefulness at the beginning of call in was marginally lower in the suicidal act group than that in the non-suicidal group (see Table 1). The decrease in psychological distress at the end of the intake intervention was significantly less in the suicidal act group than in the non-suicidal group (t = −2.13, p = 0.034). While the scores of the three domains of CSRSPSH were dichotomized as low and high, suicidal act group were less likely receiving high quality of counseling process than that in non-suicidal group (see Table 1). For the scores of the other two domains of the CSRSPSH, the differences between the suicidal act group and non-suicidal group did not reach statistical significance.
Baseline characteristics of suicidal act group and non-suicidal group of high suicidal risk callers.
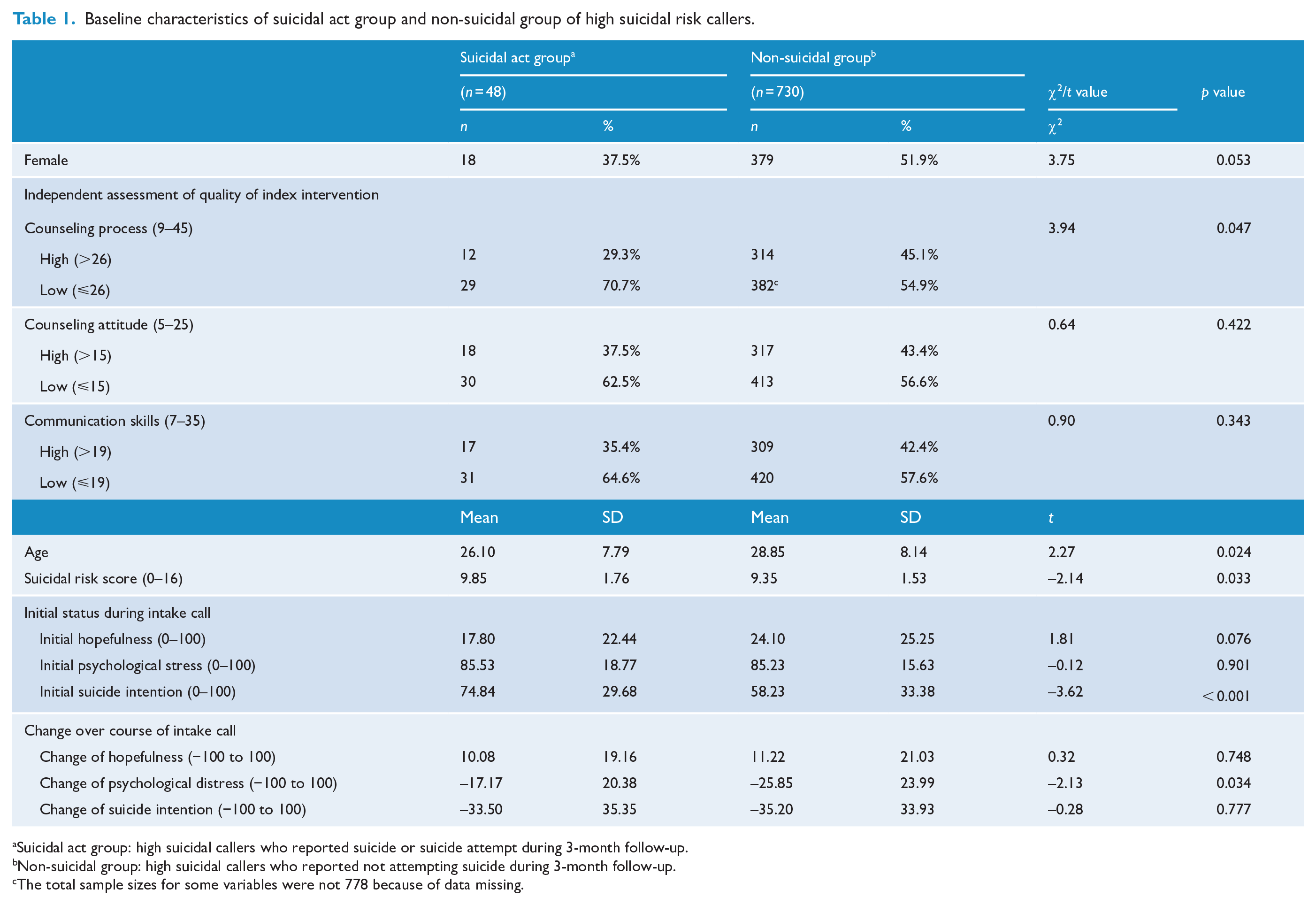
Suicidal act group: high suicidal callers who reported suicide or suicide attempt during 3-month follow-up.
Non-suicidal group: high suicidal callers who reported not attempting suicide during 3-month follow-up.
The total sample sizes for some variables were not 778 because of data missing.
We also compared the scores of 21 items of the CSRSPSH between the suicidal act group and non-suicidal group. As shown in Table 2, the scores of the items of assessing, preparation for problem-solving and problem-solving in the suicidal act group were lower than that in the non-suicidal group, but the differences were marginally statistical significance.
Comparisons of scores of 21 items of the Counseling Skills Rating Scale for Psychological Support Hotlines between callers of suicidal act and non-suicidal groups.
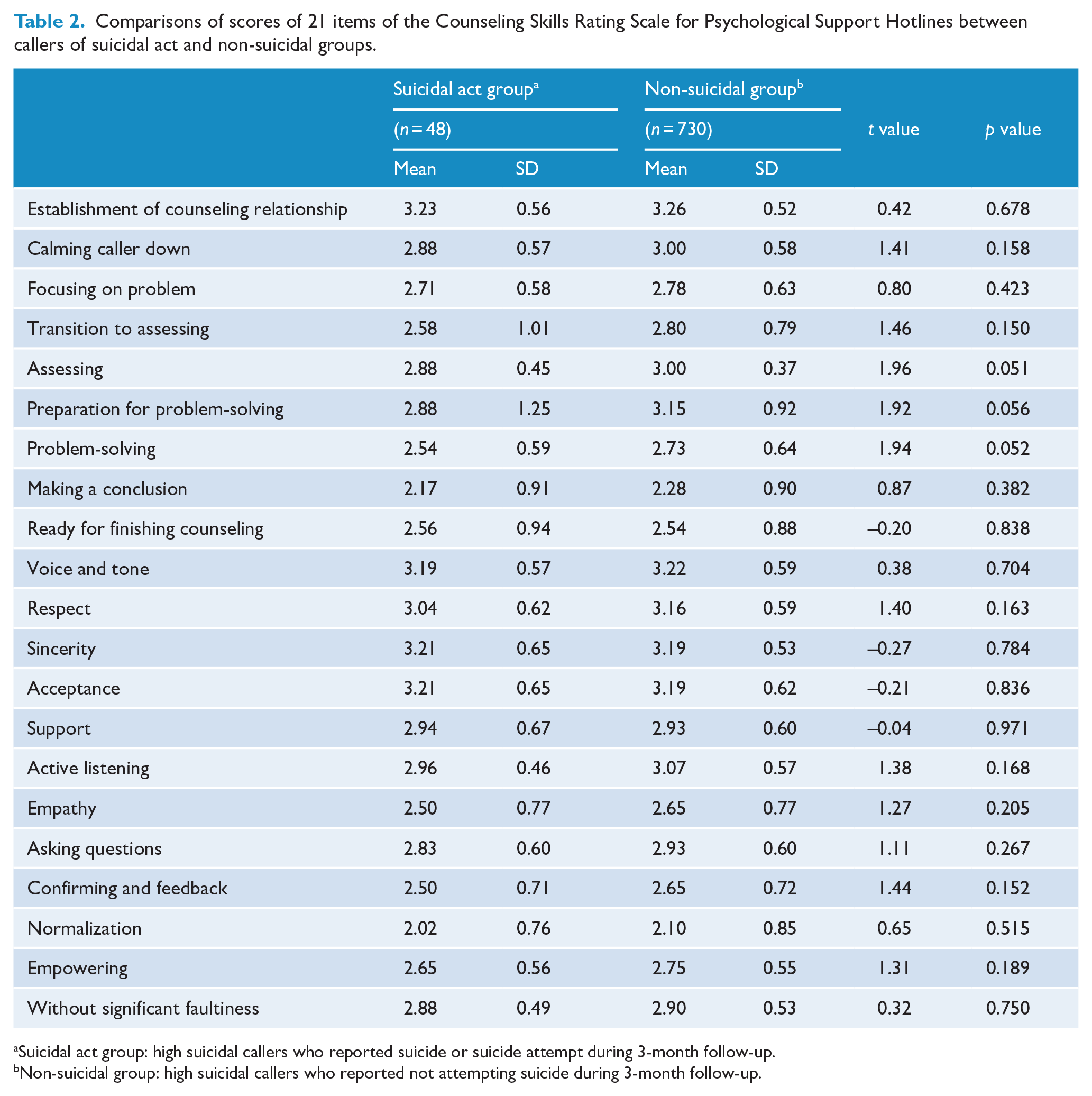
Suicidal act group: high suicidal callers who reported suicide or suicide attempt during 3-month follow-up.
Non-suicidal group: high suicidal callers who reported not attempting suicide during 3-month follow-up.
As shown in Table 3, suicidal risk was an independent predictor of suicidal acts in the follow-up period, in both model 1 (hazard ratio [HR] = 1.20, 95% confidence interval [CI] = [1.02, 1.42]) and model 2 (HR = 1.22, 95% CI = [1.04, 1.45]). Callers with a higher suicidal risk score were more likely to have suicidal acts over the 3-month follow-up than callers with lower suicidal risk score. Furthermore, a high quality of counseling process domain was marginally associated with lower risk of suicidal act during 3-month follow-up (model 1, HR = 0.53, 95% CI = [0.27, 1.05]), and the score of the item of assessing (model 2, HR = 0.38, 95% CI = [0.18, 0.85]) was associated with lower risk of suicidal act in 3-month follow-up period.
Correlates of reducing suicidal acts among high suicidal risk callers in 3 months after hotline intervention.
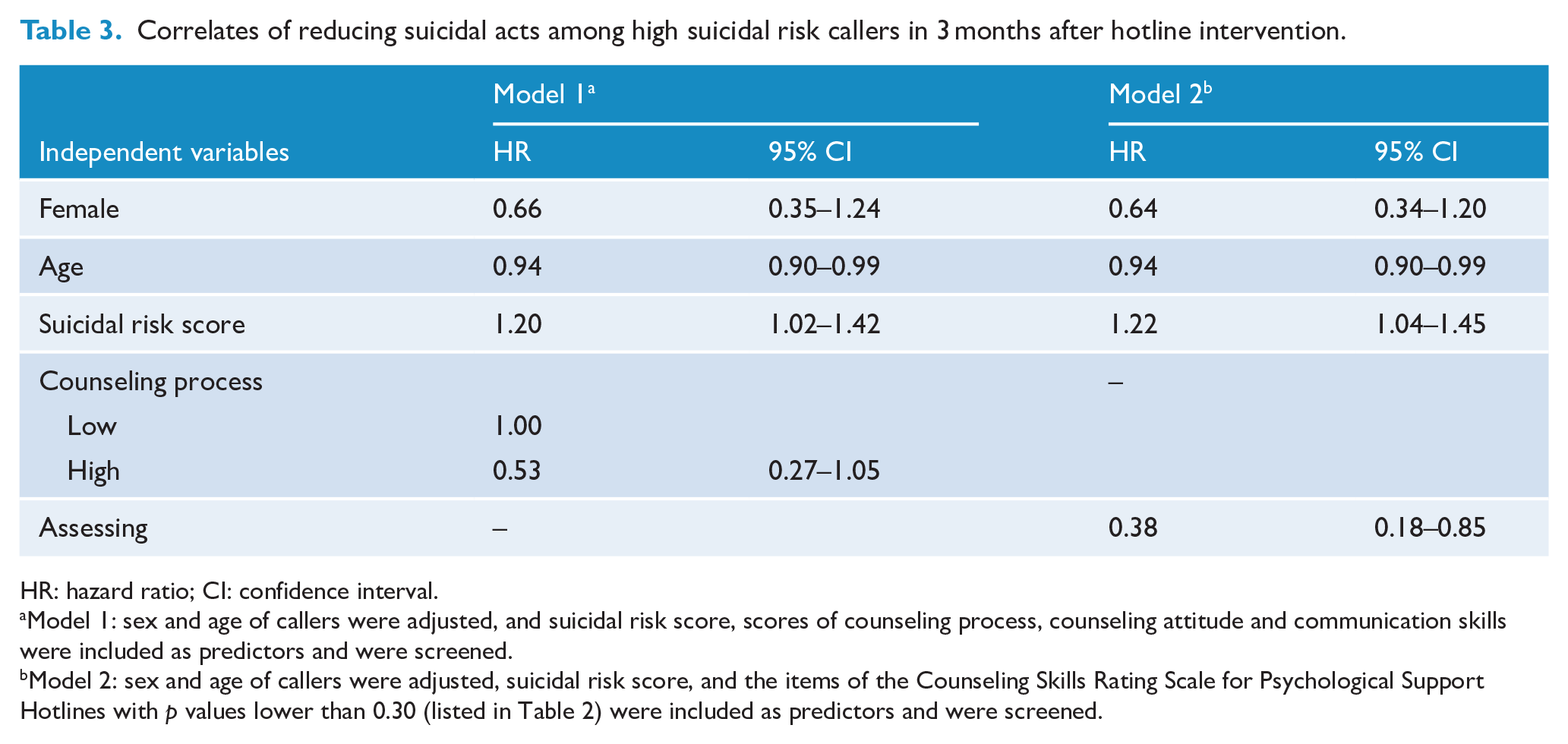
HR: hazard ratio; CI: confidence interval.
Model 1: sex and age of callers were adjusted, and suicidal risk score, scores of counseling process, counseling attitude and communication skills were included as predictors and were screened.
Model 2: sex and age of callers were adjusted, suicidal risk score, and the items of the Counseling Skills Rating Scale for Psychological Support Hotlines with p values lower than 0.30 (listed in Table 2) were included as predictors and were screened.
To address the correlates of reducing immediately suicidal risk, multivariate linear regression analyses were conducted. As shown in Table 4, high quality of communication skill was associated with the increasing hopefulness (β = 0.09, p = 0.030), and high quality of counseling process (β = −0.12, p = 0.003) and higher suicidal risk score (β = −0.12, p = 0.003) were associated with the decrease of intensity of suicide intention.
Factors significantly associated with before versus after changes in level of reported hopefulness and suicidal intent over the course of the index intervention hotline call.
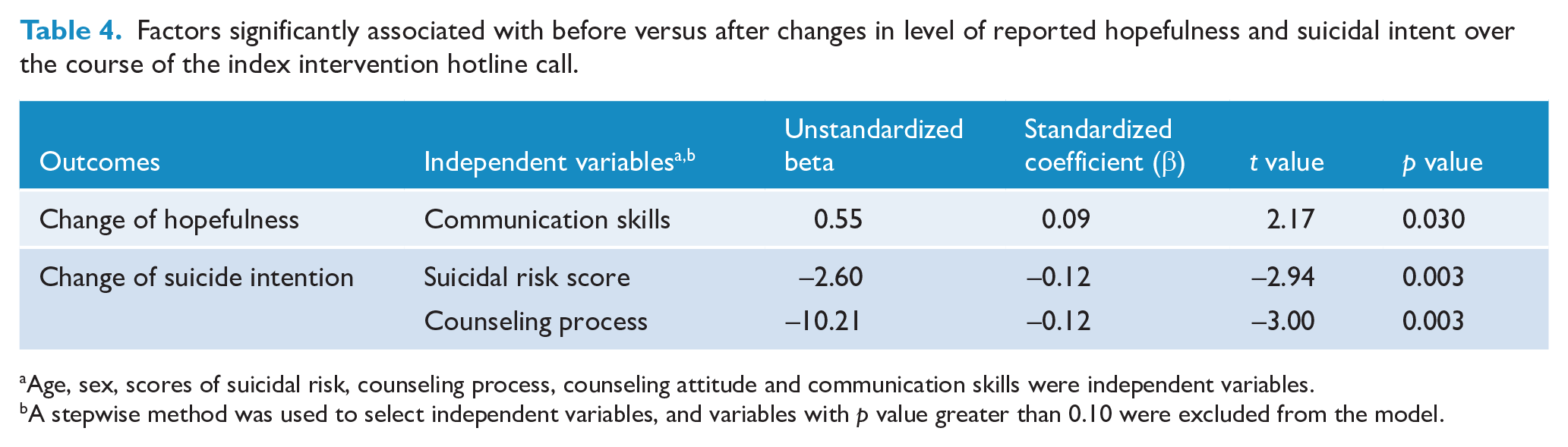
Age, sex, scores of suicidal risk, counseling process, counseling attitude and communication skills were independent variables.
A stepwise method was used to select independent variables, and variables with p value greater than 0.10 were excluded from the model.
Discussion
Main findings
Hotline is an easy accessible resource of mental health service (Ramchand et al., 2017), especially in LMICs with limited resources (Baker et al., 2018). Previous studies had addressed the effectiveness and correlates of reducing risk factors of suicide, such as depression, distress and suicide ideation (Bobevski et al., 1997; Coveney et al., 2012; Donohue et al., 2014; Draper et al., 2015; Gould et al., 2017; King et al., 2003; Mishara et al., 2007b; Ramchand et al., 2017). In this study, we examined high suicidal risk callers at a nationwide psychological support hotline in China and showed that those with higher suicidal risk score were more likely to engage in suicidal act over the 3-month follow-up. Moreover, results underscore the importance of the quality of the hotline psychological interventions in reducing risk for suicidal acts, with higher score of the item of suicidal risk assessing associated with decreased risk of suicidal act and high quality of counseling process domain marginally associated with the decline of suicidal risk. Furthermore, operator’s higher quality of communication skill domain was associated with increased callers’ hopefulness, and operator’s higher quality of counseling process domain was associated with decreased intensity of suicide intention among callers.
There is a growing consensus that suicidal risk assessment should be integrated as one important part of the intervention process during crisis hotline calls (Gould et al., 2013; Mishara et al., 2007a). However, data on this topic suggest that most hotline helpers/operators do not complete important components of intervention, especially suicidal risk assessment or asking about callers’ suicidal ideation (Coveney et al., 2012; Mishara et al., 2007a; Ramchand et al., 2017). Our findings shed light on the importance of addressing this shortcoming in practice. Our data show that higher score of the item of assessing suicidal risk was associated with reduction in the occurrence of suicidal acts among high suicidal callers, and the higher quality of hotline counseling process was marginally associated with the decline of suicidal risk after hotline intervention. An integrative counseling process includes emotional relief, assessing suicidal risk and related problems and collaborative problem-solving. To complete a high-quality counseling process, hotline operators were required to actively engage in communicating with callers, which would result in good contact and strong therapist-client alliance (Draper et al., 2015; Mishara et al., 2007b). Furthermore, detailed suicidal risk assessment and collaborative problem-solving were associated with the decreases of helplessness, hopelessness and depression—the precursors of suicidal behaviors (Mishara et al., 2007a, 2007b). The results of previous studies and our findings indicated that the hotline intervention skills training should emphasize how to raise hotline operators’ capability of getting through a comprehensive intervention.
Available evidence does not support the idea that assessing suicidal risk leads to suicidal ideation or increased risk for suicidal behavior (Dazzi et al., 2014). Indeed, hotline callers report positive emotional reactions to being asked about suicidal ideation (Coveney et al., 2012). Furthermore, our findings suggested that assessing suicidal risk of hotline callers could reduce subsequent suicidal acts, including suicide and suicide attempt, among high suicidal callers. Some have argued that suicidal risk assessment could not be used in clinical practice to determine allocation of intervention, because of the low positive predictive value of the existing assessment tools (Carter et al., 2017). Our findings suggest that suicidal risk assessment during hotline calls would reduce the risk of subsequent suicidal act. Similarly, others have documented the therapeutic value of suicide risk assessment in reducing risk for suicidal behavior in high-risk clinical populations (Geulayov et al., 2019).
In terms of immediate improvement, quality of hotline counseling process was associated with decreasing of intensity of callers’ suicide intention after the intervention, and quality of communication skills of operators was associated with increasing callers’ hopefulness after the intervention. Our findings were consistent with previous studies (Draper et al., 2015; Mishara et al., 2007b), in which collaborative problem-solving, active listening and empathy and were related to positive changes in distress, helpless, hopeless and depression among hotline callers. In this study, collaborative problem-solving was a primary element of the counseling process, and the active listening and empathy were components of communication skills. Unexpectedly, in our study, neither the consequent suicidal acts nor the immediate improvement was associated with the counseling attitude domain, which included respect, sincerity, support etc. The inconsistency might be due to the sampling differences. In our study, only the callers with high suicidal risk were recruited. High-risk callers might have strong desires of seeking professional help for mental health which may serve to overcome barriers associated with counseling attitudes.
Besides the hotline operators’ performance, callers’ characteristics were also correlated with outcomes of hotline intervention for suicide. Results in our study indicated that a higher suicidal risk score was associated with the consequent suicide attempt among high suicidal risk callers. Gould et al. (2007, 2017) have reported similar results, in which suicide risk or intensity of suicide intention of callers was associated with the effectiveness of intervention. Such findings implied that although suicidal risk score could not predict consequent suicidal act accurately, the high suicidal risk callers as a group should be paid more attention to, and they need intensive intervention.
Implication
Previous studies had verified the effectiveness of hotline intervention for suicide. Our studies extend prior research on hotline operators’ professional performance and the callers’ characteristics and their associations with hotline intervention outcomes. Based on our findings, we propose several recommendations. First, suicidal risk assessment should be integrated in the comprehensive suicidal risk management in hotline because the process of assessing suicidal risk may lower risk for suicidal acts among high suicidal risk callers. Second, to improve the quality of hotline intervention for suicide, standardized intervention skill training should be provided to hotline operators. The training should focus on the communication skills and how to get through the hotline counseling process. Our experience is that systematic training in the process of fielding a call is essential from greeting the caller, to assessing the caller’s concerns in detail, collaborative problem-solving, to finishing counseling session fully and smoothly.
Strength and limitations
There were several strengths in this study. First, it was a longitudinal study with follow-up over 3 months. Second, the primary outcome in this study was the occurrence of suicide or suicide attempt, an improvement over most prior studies that focused on depressive symptoms, suicidal ideation or other indicators of risk but not overt behavior. Third, we used a structured scale, i.e. the CSRSPSH, to evaluate the quality of hotline psychological intervention for high suicidal risk. The raters were blind to the callers’ outcomes after hotline psychological intervention. Accordingly, the results in our study might be more objective than previous studies using subjective evaluation such as callers’ perception. Fourth, the sample size was large, allowing for meaningful analyses of suicide and suicide attempts among high suicidal callers over follow-up.
There were also some limitations in the study. First, the hotline callers were younger than living community residents. Our findings could not be generalized to the elderly. The elder population in China was vulnerable to suicidal behavior but few of them sought mental health help (Zhou et al., 2018). Special hotline counseling skills might be needed for the old people. Second, the outcomes in this study relied on callers’ self-report. Third, the callers assessed as moderate or low suicidal risk were not recruited in this study. The findings in our study could not be generalized to the callers without high suicidal risk. Fourth, we did not address the potential influence of duration of follow-up. Gould et al. (2007, 2017) had reported that follow-up calls would reduce the perceived suicidal risk. The correlates of a longer term outcomes of hotline psychological intervention for high suicidal callers should be clarified in the future studies. Fifth, the suicide death and suicide attempt were combined in the study, although the two suicidal acts were overlapped but not one population. Sixth, although supervisors who evaluated quality of intervention did not know the primary outcome of callers, but they might know the scores of hopelessness, psychological distress and suicide intention at the beginning and ending of the intake call, which might confound the associations of hotline intervention and immediate outcome of the intervention. Seventh, several potential confounding factors, including the quality of safety plan in the psychological intervention, were not assessed in this study. Further studies are needed to address the weaknesses.
Conclusion
Our findings indicate that, besides the hotline caller’s suicidal risk level, hotline operator’s professional performance in the hotline-based psychological intervention for suicidal callers is associated with reduction of immediate suicidal risk, and more important, with decreased risk of suicidal acts during follow-up. Intervention skill training for hotline operators should emphasize specific counseling skills, including communication skills, suicidal risk assessment and collaborative problem-solving etc.
Research Data
research_data_of_suicidal_acts_hotline – Prospective study of association of characteristics of hotline psychological intervention in 778 high-risk callers with subsequent suicidal act
research_data_of_suicidal_acts_hotline for Prospective study of association of characteristics of hotline psychological intervention in 778 high-risk callers with subsequent suicidal act by Yongsheng Tong, Kenneth R Conner, Cuiling Wang, Yi Yin, Liting Zhao, Yuehua Wang and Yue Liu in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors thank Professor Michael R. Phillips and Dr Weihai Zhan for their valuable comments on an earlier version of the manuscript.
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the National Natural Science Foundation of China (81371501), Beijing Municipal Science & Technology Commission (No. Z131107002213075), Beijing Municipal High Rank Health Researcher Training Program (2015-3-111) and Beijing Selected Funding for Study Abroad Scholars.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.