
Abstract
Durkheim's [1] view of suicide as an event reflecting broader social dysfunction has been borne out in recent epidemiological studies of youth suicide. Its precursors are often evident in an individual's developmental and family background well before the social adversity that often immediately precedes suicide. Thus, risk factors such as poor family cohesion and a childhood history of abuse may be evident years before the appearance of serious suicidal behaviour. In the current review preventive interventions addressing all well-established risk antecedents have been considered. These antecedents have been classified according to their origin in the individual, family, school and community backgrounds of young people [2].
Identifying risk and protective factors
The evidence examining risk and protective factors for youth suicide has been comprehensively reviewed by Beautrais [3]. In judging the value of a risk factor as a target for suicide prevention, several considerations are relevant. The most promising risk factors are likely to be common, predate the onset of serious suicidal behaviour and have strong, statistically significant associations with suicide or suicidal behaviour after adjustment for confounding. Risk factors should be modifiable and there should be some understanding of the risk processes leading to suicide. This understanding is not evident for all risk factors. For example, it is unclear whether family history of suicidal behaviour reflects an inherited constitutional predisposition to impulsivity, or learned patterns of behaviour, each with a different implication for prevention.
Levels of intervention
The mental health intervention spectrum covers various levels of intervention [2].
Clinical interventions
Clinical interventions such as early identification and treatment can potentially influence suicide rates. Risk factors for youth suicide such as depression and substance abuse are also targets for clinical intervention. The extent to which clinical interventions might affect suicide rates depends on whether services identify young people at most risk and the effectiveness of the available interventions in modifying the course of disorder across the risk period for suicide. Thus, the impact of the intervention needs to be gauged over longer follow-up periods.
Indicated interventions
Indicated interventions are designed for young people already exhibiting symptoms of a disorder, such as deliberate self-harm, experimentation with drugs or subsyndromal depression. Effectiveness depends on the program's capacity to identify a discrete target population (through systematic screening or clinical identification) and the capacity of services to provide an adequate intervention to all selected individuals. Disadvantages may include the effects of labelling and stigmatisation. In practice, many explicit ‘suicide prevention’ programs have adopted a strategy of indicated prevention.
Selective interventions
Selective interventions delineate a group at high risk for future suicide or suicidal behaviour who are not currently manifesting clinical symptoms (young males in remote communities). Success depends on the extent to which the risk factor identifies a population carrying a substantial proportion of risk. They may be further divided into vulnerability-focused interventions (e.g. family psychopathology) that aim to promote resiliency in an individual through enhancement of the social environment or the development of skills and event-centred interventions (i.e. focused on adverse life events), which commonly use counselling or debriefing strategies.
Universal interventions
Universal interventions are designed to favourably shift risk and/or protective factors across a whole population [4]. They may directly target immediate antecedents of suicidal behaviour, such as depressive symptomatology, or more remote antecedents, such as parental divorce. Universal interventions are designed to affect some aspect of the social environment (environment-focused) and/or aim to promote knowledge, skills and resiliency in an individual (person-centred) [5].
Choice of prevention strategies
Timing is important. For some risk factors where exposure or onset is in early childhood (e.g. antisocial behaviour or academic failure) an intervention might be expected to optimally take place or at least commence earlier in the risk process. Risk factors commonly cluster; interventions for one may bring benefits for another. Thus, an intervention to reduce antisocial behaviour may also influence academic achievement, an independent risk factor for suicide.
Another consideration is the relationship that exists between risk factors for suicidal behaviour and other poor health outcomes. Early antisocial behaviour is associated with later suicidal behaviour, but is also a risk factor for substance abuse, sexual risk behaviour and injury. In general suicide-inclusive risk factors have received less attention in earlier reviews of suicide prevention than suicide-specific risk factors such as access to lethal means. Interventions for suicide-inclusive factors have the potential to bring a wider range of health benefits, a relevant consideration when developing strategies for funding and coordinating suicide prevention with other areas of health promotion [6].
Judging the utility of preventive interventions
Describing interventions
To judge the local applicability of an intervention several elements must be clear: the setting for which an intervention has been designed, the target population and details of the intervention, specifically the intensity and duration. Many reports derive from overseas studies, and transferability to an Australian context requires careful consideration. Local risk profiles for suicide, as well as the cultural context of the intervention, are likely to differ substantially from those found in other countries.
Evaluating interventions
Four facets of evaluation are relevant when judging the utility of an intervention: (i) level of implementation; (ii) efficacy in changing targeted outcomes; (iii) cost-effectiveness; and (iv) the availability of a model of dissemination.
The capacity to reach a target audience, as well as recruitment and retention rates, needs consideration in judging the success of interventions. For example, interventions targeting late-secondary school may miss or fail to engage chronic absentees or school dropouts, both high-risk groups for suicidal behaviour and psychopathology.
Randomised, controlled trials (RCTs) remain an optimal strategy for evaluating the efficacy and cost-effectiveness of interventions. In practice, however, there have been difficulties in implementation. In the case of suicide prevention, the design is often neither feasible (given suicide's rarity as an outcome) nor ethical. Even in studies where proximal outcomes such as suicidal behaviour are used, difficulties often arise in randomisation procedures, with many studies being forced into weaker methods of randomisation. Other common problems derive from contamination of control groups, lack of blindness in observer ratings of outcomes and a long time-lag to show intervention effectiveness.
Quasi-experimental and ecological designs have been adopted as an alternative to RCTs. Interrupted-time-series analyses, in which an intervention effect with a discrete onset (e.g. removal of lethal means) is compared with a baseline series of observations, are prominent among these designs. Problems arise in interpretation, as secular processes other than the intervention may bring changes in suicide rates. If combined with more specific analyses (e.g. patterns of injury related to intervention) an interrupted-time-series approach may provide stronger evidence of effect.
Interventions targeting individual risk factors
Table 1 shows the effects of preventive interventions for individual risk factors for youth suicide.
Evidence on the effects of preventive interventions for individual risk factors for youth suicide
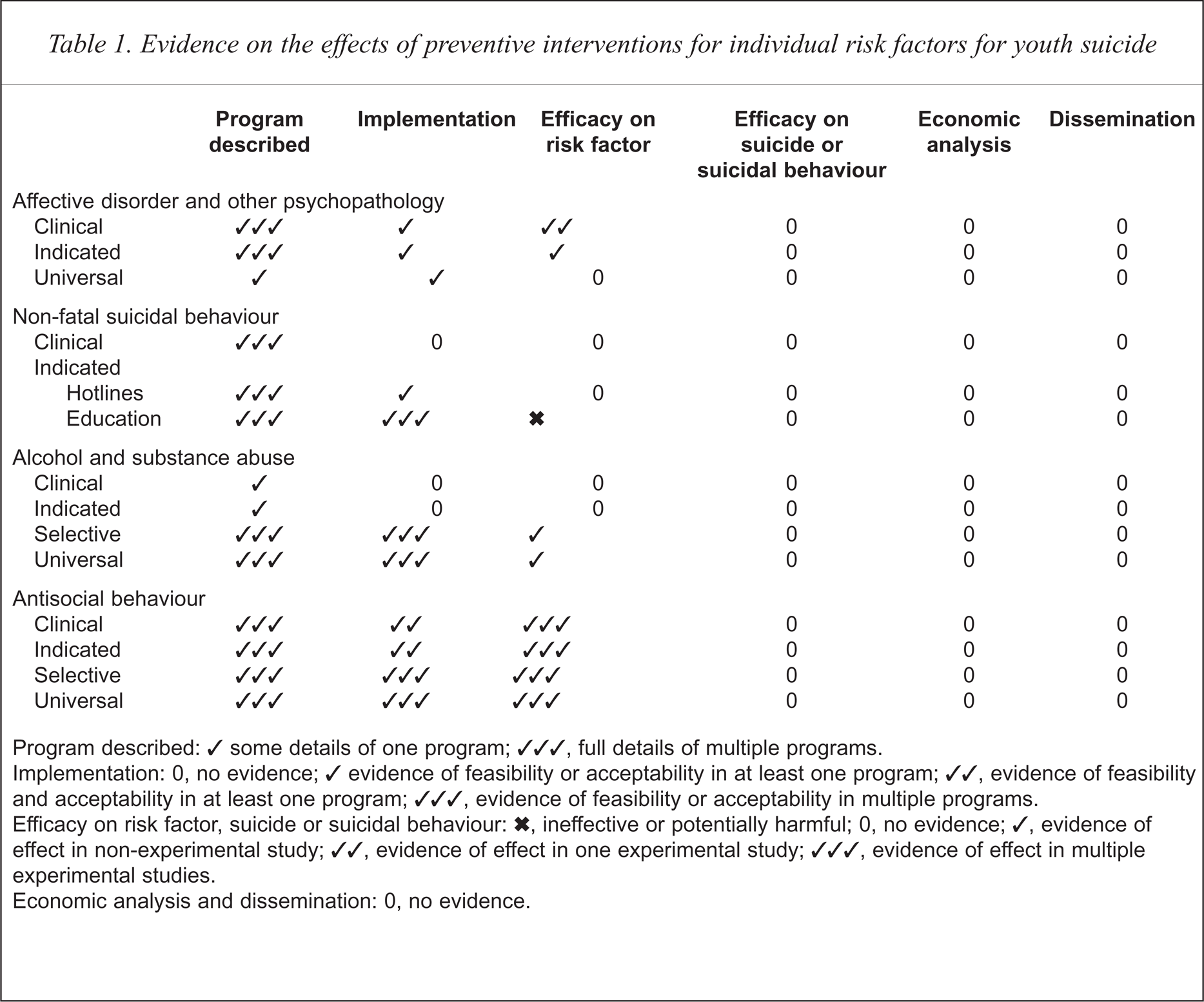
Program described: ✓ some details of one program; ✓✓✓, full details of multiple programs.
Implementation: 0, no evidence; ✓ evidence of feasibility or acceptability in at least one program; ✓✓, evidence of feasibility and acceptability in at least one program; ✓✓✓, evidence of feasibility or acceptability in multiple programs.
Efficacy on risk factor, suicide or suicidal behaviour: ×, ineffective or potentially harmful; 0, no evidence; ✓, evidence of effect in non-experimental study; ✓✓, evidence of effect in one experimental study; ✓✓✓, evidence of effect in multiple experimental studies.
Economic analysis and dissemination: 0, no evidence.
Affective disorder/psychopathology
Depression emerges consistently as an important antecedent of youth suicide and has understandably been a major focus in youth suicide prevention. Clinical interventions targeting conspicuous depressive symptoms have been the most commonly trialed. More recently indicated interventions, identifying ‘high-risk’ subjects defined by the presence of sub-syndromal depression, have been attempted.
Clinical interventions
Cognitive–behavioural therapy (CBT) has been the principal treatment for adolescent depression with both individual and group approaches having been described [7–12]. Treatments have varied in intensity from six to 16 sessions and have generally included multiple components (e.g. problem solving and understanding cognition). Comparisons have been made between active and non-directive supportive treatment [13].
The lack of adequately designed pharmacological studies examining the treatment of youth depression is striking. In a meta-analysis examining the use of tricyclic antidepressants only three studies, with 80 patients in total, fell clearly into the adolescent age range (12–20 years) [14]. Trials of newer antidepressants are emerging [15].
Implementation
For depressed adolescents who reach mental health services, specific psychological and medical interventions appear acceptable [13,14]. Evidence, however, suggests that many depressed young people do not reach clinical attention and Australian general practitioners do not feel equipped to deal with this group [16,17]. The availability and utilisation of specific youth-oriented psychological treatments in primary care is unclear.
Efficacy
Specific psychological treatments such as CBT can bring quicker symptom remission in major depression [13]. There is, as yet, no evidence that CBT has medium- to longer-term benefits in symptom reduction or relapse prevention. Given the evidence supporting relapse prevention in adults, this is an important area requiring investigation [18]. Evidence is emerging supporting the short-term effectiveness of newer antidepressants for adolescents [14]. The medium- to long-term benefits are unknown.
Cost-effectiveness and dissemination
Cost effectiveness and dissemination evidence is not available.
Indicated interventions
Several studies using school sampling frameworks have examined the scope for indicated interventions to prevent adolescent depression [19–25]. Subjects are identified using self-report questionnaires for depressive symptomatology. Those identified as high-risk are given a structured intervention based on CBT principles. Typically, psychologists using group meetings over a 12–15-week period have administered this.
Implementation
The capacity to detect and engage young people at risk for depression is problematic. Participation rates in the Penn Prevention Program [20,21] were less than 20%, and of those participating in the survey over half were identified as being at high-risk. Participation rates and follow-up evaluation was more satisfactory in the study of Clarke et al., with close to half of those identified as being at high risk agreeing to further assessment and intervention [19]. Audiotape evaluations in this project indicated a high adherence to protocol. Studies targeting older youth were not identified. This group has a greater risk of suicide and indicated strategies could be more appropriate.
Efficacy
Indicated interventions may lead to short- to medium-term benefits. Two studies had important methodological limitations related to non-blind assessment and the failure to find differences on self-report measures [19,24]. Suicidal behaviour was not examined as an outcome in any study. Potentially adverse consequences resulting from incorrect identification and/or stigmatisation has not been adequately addressed.
Cost-effectiveness and dissemination
Formal reports of cost-effectiveness and dissemination are not available. Approaches using health staff to provide group sessions are likely to require substantial resource deployment. The alternative approach of using counsellors or other education staff to run groups is perhaps more economically feasible in the long term, but also requires substantial funds being made available for training.
Universal interventions
The risk relationship between depression and suicidal behaviour follows a linear trend, with risk increasing progressively with level of depression. There is no discrete point or sharp transition at which an individual becomes high-risk. This risk pattern supports consideration of universal strategies for prevention [26]. To date, however, only two small studies targeting middle-school students have utilised universal strategies [27]. These were based on psycho-educational interventions using a CBT framework.
Implementation
Evidence suggests that teachers and/or health professionals may achieve reasonably high uptake rates [27,28]. Clarke et al. [27] report an 86% compliance rating when teachers' use of a structured manual was observed. The capacity to deliver longer or more complex interventions remains unexplored.
Efficacy
Small sample sizes of universal intervention studies make it difficult to detect changes [27]. The possible contamination between school classes requires consideration.
Suicidal behaviour
Associations between suicidal behaviour and suicide are robust and the prevalence of suicidal behaviour in adolescence is high [29,30]. Furthermore, suicidal behaviour in older subjects appears modifiable. There is evidence, albeit modest, from RCTs in adult populations for the efficacy of approaches that enhance an individual's capacity to deal with social adversity. Brief therapies focusing on problem solving alone have shown lower repetition rates of self-harm [31]. When extended to include intensive CBT [32] and interpersonal skills [33], there have been trends to lower repetition rates, improvements in problem-solving capacities and a reduction in other risk factors such as depression, hopelessness and suicidal ideation. Study interpretation is limited by small sample sizes (see Hawton et al. [34]).
Clinical interventions
Early studies targeting adolescents who attempted suicide neglected self-harm either as a focus for intervention or as an outcome measure and, therefore, the effect on subsequent suicide risk was uncertain. Problems of non-attendance for clinical follow up has been well documented [35–37]. Adherence rates with follow up for non-hospitalised adolescents range between 20% and 30% [38,39]. Rates of follow up for adolescents admitted to hospital following self-poisoning have generally been below 50% [40], with high rates of withdrawal from subsequent treatment [41]. Models of intervention vary and have included easier access to care, psychoeducation, peer support and structured psychological interventions [42–46].
Implementation
There is a discrepancy between the proportion of young people manifesting suicidal behaviour at a community level and those attending treatment services, suggesting many do not present for treatment. Population-based estimates in Australia, North America and Europe suggest a prevalence rate of up to 5% for deliberate self-harm over the previous 12 months [29,30]. Estimates of admission to Accident and Emergency Departments over a 12-month period are around 0.5% [47]. In addition, consultation rates before death in young, male victims appears low in comparison with females and older groups [48]. Vassilas and Morgan [49] reported that only 22% of male suicide victims under the age of 35 years came into contact with health services in the 4 weeks before death. For males over 35 years and younger female suicide victims, contact rates were 52% and 57%, respectively.
Similar doubts have been raised about the capacity of service systems to engage and follow up young people after an episode of suicidal behaviour. A trial of ‘green-card tokens’, allowing hospital readmission on demand brought no differences in clinically conspicuous suicidal behaviour at 12-month follow-up [42].
Efficacy
Data on efficacy of clinical intervention for suicidal behaviour are not available.
Indicated interventions
Strategies to identify at-risk individuals have included telephone counselling, school-based screening or suicide education and ‘gatekeeper’ training. The aim is to detect subjects at risk by identifying recent suicidal behaviour or ideation and taking appropriate steps to further counselling or clinical intervention [50].
Crisis centres and hotlines
Crisis centres and hotlines use trained volunteers or paid staff provide telephone or other counselling services for those in emotional distress. These services may also offer direct counselling, are often linked to mental health services and may provide mobile community assessment for suicide risk and postvention. Suicide prevention and crisis centres, telephone counselling services and hotlines have become widespread in Australia and other developed communities since the 1970s [51–58].
Implementation
Few quantitative studies are available. There is evidence that crisis lines can reach populations at higher risk although their accessibility to and use by young males appears limited. For example, Miller et al. [57] compared 28 USA communities with crisis centres with 48 cities without crisis centres. Young, white females were the commonest callers and, thus, it was assumed that any effect should be most marked in this group. An estimated reduction of 1.75 per 100 000 was found for young, white females, however, no significant reduction was found in any other group. The proportion of suicide victims using crisis lines in the months preceding their death is unclear. There is also evidence that responses are not standardised and vary considerably depending on the characteristics of the caller [59].
Efficacy
Interrupted-time-series studies have examined the effect of the introduction of crisis centres, but little evidence has emerged of beneficial effects on rates of suicide [51–54,56–58]. Their impact on non-fatal suicidal behaviour and other mental health outcomes has not been examined.
Cost-effectiveness and dissemination
Data are limited on cost-effectiveness and dissemination. The appeal of prevention centres comes from the low cost of service provision and this, rather than evidence of their effectiveness, is one reason why they have been established broadly. Quality-assurance reports monitoring suicide prevention centres are not available.
Suicide education programs
Suicide education has in the past been widely employed in secondary schools, where students, teachers or parents learn about suicide, its warning signs and how to seek help [50]. Typically, programs aim to raise awareness, train participants to identify adolescents at risk and provide education on community mental health resources. Program content might include information on the epidemiology of suicide, a list of warning signs (perhaps with an emphasis on depression) and information on community health resources and referral pathways. Interventions range from brief one-class sessions to longer interventions spanning multiple classes per week over a period of months. Many programs have been criticised for misrepresenting the facts of youth suicide by denying a role of mental disorder, exaggerating the extent of the problem and normalising deviant behaviour, thereby making it more acceptable. Recently, programs have differed in many important respects by including a focus on adolescents at risk of school dropout [60], incorporating a broader social and psychological focus for intervention [61,62], including teacher delivery of materials [63,64] and adapting the approach to particular ethnic groups [65].
Implementation
Few studies report details on teacher training or classroom instruction. There is concern that at-risk individuals do not receive the programs (i.e. school dropouts and/or chronic absentees) [50].
Efficacy
There have been many curriculum-based programs operating in the last decade, but there are relatively few published evaluations and most are poorly designed [66–70]. The evidence from programs focusing on identification of high-risk students suggests they are not effective. Outcomes from interventions focusing on attitudes to suicide are mixed, but the larger and better-designed studies show little beneficial effect. Interventions in which suicide education is incorporated within a life-skills approach show more consistent evidence of effect, but the effect of the suicide specific element is uncertain.
Community gatekeeper training
Gatekeeper training is based on the premise that people at risk of suicide come into contact with ‘gatekeepers’: police, clergy, youth workers and other members of the public who have a capacity to direct those individuals towards help. The programs typically occur at 1- or 2-day workshops and are designed to increase the gatekeepers' sense of confidence and competence in intervening. Program aims include enhanced recognition of warning signs, increased knowledge of referral pathways and access to the mental health-care system. The Centre for Disease Control and Prevention has described a range of these programs in the United States [71].
Implementation and efficacy
There is some evidence that gatekeepers' attitudes towards intervention shift following training, but little evidence regarding training or post-training implementation. There is no efficacy evidence.
Universal interventions
Evidence is not available on universal interventions for suicidal behaviour, however, self-harm is sufficiently common to warrant consideration of population-based approaches.
Alcohol and substance abuse
There is a long history of prevention efforts targeting adolescent alcohol and substance abuse [72]. School-based drug education programs were first trialed in the 1960s with poor outcomes. Recent programs are multicomponent and broader based, addressing a range of social risk factors (e.g. peer and adult role models, media and community influences) as well as promoting individual life skills. These studies have not measured suicidal behaviour specifically.
Clinical/indicated interventions
Behavioural and social skill interventions have been adapted for use with adolescent substance abusers. For example, Hawkins et al. [73] used a combination of behavioural skills training and social network development in a therapeutic community setting to treat young substance abusers. Haggerty [74,75] adapted this approach for use with young offenders with alcohol-abuse problems. Other multi-faceted interventions have targeted youth manifesting multiple-risk behaviours [60].
Implementation/effectiveness
The limited number of published evaluations is surprising. Participation, patient compliance and relapse rates are unknown.
Selective interventions
Strengthening Families and Focus on Families are examples of multifaceted interventions targeting children whose parents are substance abusers [76,77]. Program aims include improving parenting skills and family functioning, preventing parental relapse and working on expectations around drug and alcohol use.
Other selective interventions targeting ethnic groups at higher risk of alcohol and substance abuse include that of Cheadle et al. [78,79]. This study targeted American Plains Indians, a group with a suicide rate 20 times the USA average. The intervention spanned 5 years consisting of both person-focused, school- and community-wide components. Importantly, the program used traditional tribal structures with elders taking a leading role in implementation. Effects included a delayed onset of drinking, a halving of the rates of binge drinking and a reduction in other drug use.
Implementation
The capacity to detect families at risk for substance abuse appears problematic with low response and retention rates in reported programs.
Effectiveness
Family-focused interventions targeting the children of substance abusers appear effective in the short term. Long-term follow ups measuring risk behaviours in adolescence are necessary. Suicidal behaviour was not examined as an outcome in any of the available studies.
Cost-effectiveness and dissemination
Data are not available. The Strengthening Families Program has been trialed in the USA with several racial and ethnic groups in a variety of settings.
Universal interventions
Several large school-based interventions designed to prevent alcohol initiation or reduce consumption have been trialed in North America. Projects ranged from interventions emphasising social resistance training [80–84] or the development of general life skills [85,86], through to comprehensive community interventions involving schools, parents, media and community leaders [87,88].
Social resistance training aims to promote ‘refusal skills’ in situations where drugs are available. Interventions take place in classroom settings during early secondary school with later booster sessions. They use different combinations of health educators, teachers and peer leaders and focus on promoting attitudes and skills associated with non-use. Effects are often measured in terms of lower initiation rates. The effects on substance abuse are less clear.
In contrast, life skills training focuses more broadly on interpersonal skills which are relevant to substance abuse and other health risk behaviours arising from a social context. These have taken place in both school [80,85] and community settings [89]. A notable study is the Life Skills Training Program, which drew on social resistance training, but was set within a broader framework of learning to deal with anxiety and emotional difficulties, promoting self-esteem and effective communication [80]. The original program consisted of 15 classes, with 10 booster sessions in year 8 and five in year 9.
Project Northland is an example of a combined health education and broader community intervention designed to promote social norms inconsistent with alcohol use [90]. The person-focused intervention dealt with social resistance training with peer- and teacher-led curricula. Other components included structured homework with parents, parent meetings, peer leadership experience outside of the classroom, promotion of alcohol-free activities and involvement of local retailers to restrict alcohol sales to minors.
Implementation
Several large universal RCTs have been undertaken in North America with varying degrees of success. Prevention programs have generally been delivered by health program staff who require intensive training. Implementation can be problematic depending on circumstances such as high staff turnover or school closure [84].
Effectiveness
There is a growing consensus across studies that it is possible to bring about short-term reductions in alcohol and substance use in younger adolescents. The evidence examining long-term effects is most promising for more broadly focused life-skills education and those programs where health education and community interventions have been combined. In the Life Skills Training Program [80] reductions were found in smoking prevalence (22% vs 33%) and drinking to the point of drunkenness (34% vs 40%). Rates of weekly polydrug use were halved (3% vs 6%). Difficulties in interpretation arose from a high level of follow-up attrition.
Cost-effectiveness/dissemination
Person-focused interventions derive largely from North American settings where the predominant message is one of abstinence rather than harm-minimisation. There has been little work evaluating the effectiveness of similar programs in countries with different policy and legislative frameworks.
Antisocial behaviour
Antisocial behaviour generally emerges before puberty. Interventions, therefore, target younger children in family and/or school settings. Numerous studies of varying size and quality have been published. The review by Howell et al. [91] covers some notable examples. Studies target multiple health and risk outcomes and therefore interventions for antisocial behaviour commonly have an impact on family and/or school functioning as well as other individual risk factors (e.g. substance abuse and psychopathology).
Clinical and/or indicated interventions
Several studies have targeted children with early signs of antisocial behaviour and/or academic failure in school, family and community settings [92–99]. School-based strategies may include small group sessions and rewards for positive behaviours [100]. Multi-Systemic Therapy (MST) incorporates elements of family therapy and parent management training and has recently attracted considerable attention as an intervention for juvenile offenders [101–103].
Implementation
Evidence has suggested successful implementation in a range of settings and for a range of antisocial behaviours regardless of severity. Skills-based professional staff development appears an important element for interventions incorporating mentor programs, primary or early secondary school programs and programs for young offenders where there is a substantial training need for justice staff [91].
Efficacy
There is good evidence of effectiveness on antisocial behaviour as well as other important intermediary outcomes such as family functioning. Eighteen-month and 5-year follow ups indicate that participants were 66% less likely to have a juvenile record [100]. Self-reports suggest they were less likely to abuse drugs and be engaged in criminal activity. Mentor programs for youth manifesting antisocial behaviour [91] show little impact on academic achievement, but may be effective in reducing antisocial behaviour. This effect is only apparent when mentors are adequately trained in behavioural management [104,105]. Multi-Systemic Therapy appears particularly promising with effects on family cohesion and conflict persisting after 12 months. Most importantly, there were substantially lower rates of re-arrest and days incarcerated, an effect that was maintained for 4 years [101–103].
Suicidal behaviour has not been studied as an outcome.
Cost-effectiveness
Results from a brief family intervention for young juvenile offenders suggest that cost–benefits depend on the level of participant risk for re-offending, agency effectiveness (ranging from 20% to 40%) and the extent to which costs were included (e.g. personal injury, property damage, court and police expenses) [106]. For high-risk youth in agencies with the most effective interventions, cost–benefit ratios were close to 9. For youth at lowest risk with less effective intervention program, the costs outweighed the program's financial benefits. Evidence of cost-effectiveness for specific outcomes were not available.
Selective interventions
Family- and school-based programs have targeted youth at higher risk of offending. Klein et al. [107], for example, provided an 8-h intervention of behavioural family therapy over a 4-week period where a sibling had been an offender. The Positive Action Through Holistic Education (PATHE) program focused on economic disadvantage in a 3-year, multi-component, school-based intervention [108]. This program included teacher professional development examining classroom management and a family-based element aimed at the promotion of communication around academic and disciplinary problems.
Implementation and/or efficacy
At follow up, the rates of offending for subjects receiving family therapy or family counselling and for controls were 20%, 40% and 63%, respectively. Recidivism rates for offenders were substantially lower for the family therapy group (26% vs 47% and 73%, respectively) [107]. In the PATHE program academic outcomes were favourable, but antisocial behaviours did not differ from control group participants [108]. In a follow-up project, significant benefits were reported for antisocial behaviour and academic outcomes for at risk youth selected by teachers [109,110].
Universal interventions
Schools are commonly the setting with a particular emphasis in health education on promoting skills in dealing with conflict. Significant changes in skills have been reported in programs focusing on primary school children [111–113].
The Good Behaviour Game (GBG) is an example of a simple classroom-based intervention trialed in early primary school [114–116]. The intervention involved dividing a class into small groups, instituting clear class-rules, which if broken meant a team gaining points on a running tally. The intervention had a clear effect on aggressive behaviour in males at the end of the year, the biggest effect being on those boys with the highest levels of previous aggression.
An impressive demonstration is a nationwide campaign implemented in Norway and Sweden which was designed to modify the school social environment. The intervention targeted 11–14-year-olds and tackled the problems of victimisation and bullying in schools [117]. Elements of the program included creation of school and home environments characterised by warmth, positive interest and involvement with adults; introduction of firm limits on unacceptable behaviour; use of non-hostile, non-physical sanctions when rules are broken; adults acting as authorities; and the use of surveillance to monitor progress. Targeted outcomes included reductions in aggressive behaviour, poor family management and favourable attitudes to bullying. Elements of the interventions included an instruction booklet given to schools, a folder given to all families in Norway, a video on bullying and the results of questionnaire data.
The Seattle Social Development Project is another impressive demonstration of the scope for intervention for antisocial behaviour [77,118]. This multi-component intervention aimed to develop bonds to family, school and pro-social peers by promoting opportunities for involvement, interpersonal skills and reinforcement for participation. The program included teacher training, classroom management, child-skills training with a focus on communication, decision making, negotiation and conflict resolution and a seven-session parent skills training program.
Implementation
A range of universal and selective strategies can be implemented at a school level.
Effectiveness
Different strategies (school-, family- and community-based) are effective in substantially modifying antisocial behaviour, as well as other related risk and/or protective factors (e.g. academic attainment, school retention). The effect of these interventions on suicidal behaviour and depressive symptomatology has not been studied.
Cost-effectiveness and/or dissemination
Evidence is not available examining cost-effectiveness or dissemination strategies. The Communities that Care program has been disseminated in the USA and UK [119].
Interventions targeting social risk factors
Table 2 shows the effects of interventions targeting social risk factors for youth suicide.
Evidence on interventions for family, community, educational and peer risk factors for youth suicide
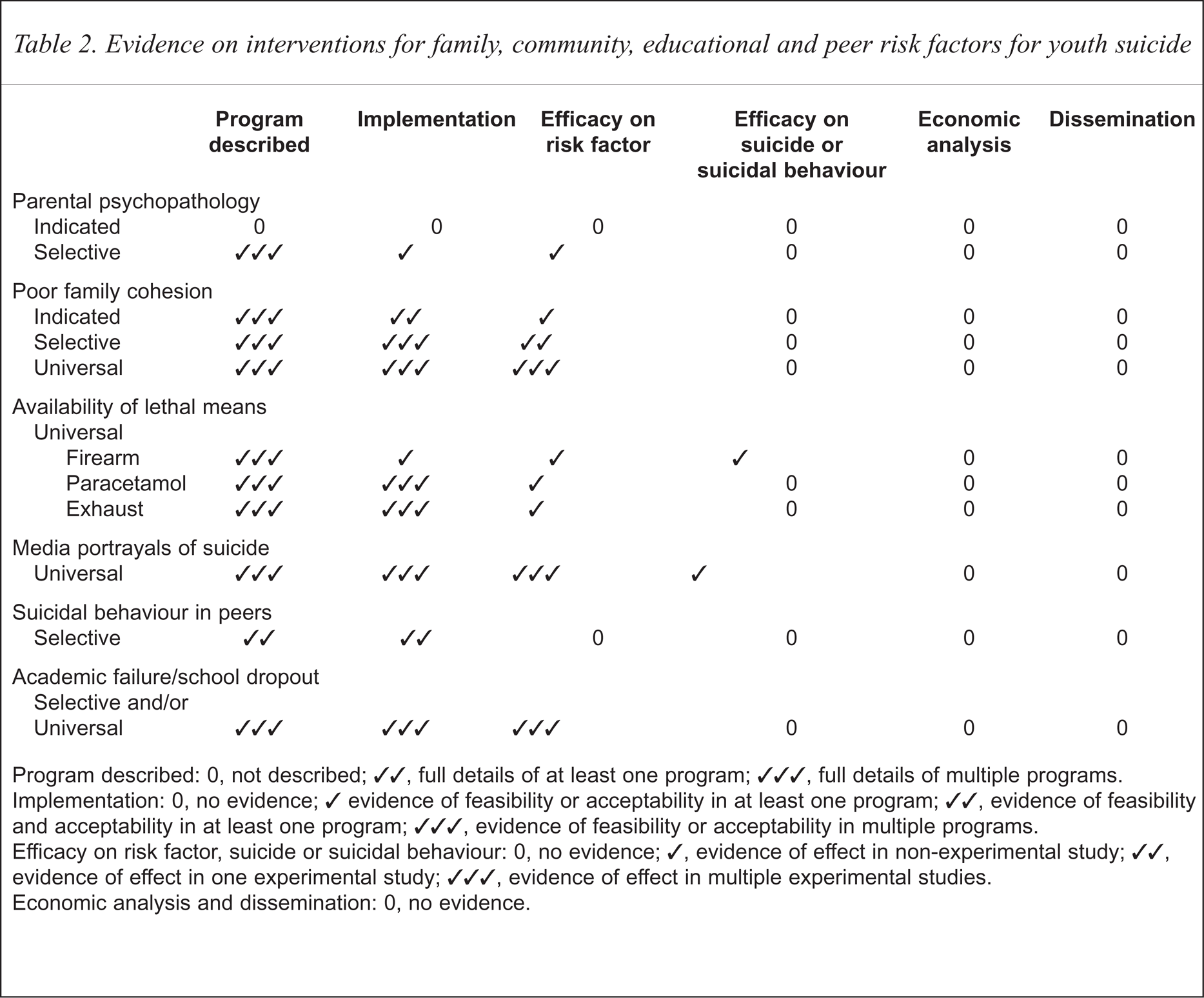
Program described: 0, not described; ✓✓, full details of at least one program; ✓✓✓, full details of multiple programs.
Implementation: 0, no evidence; ✓ evidence of feasibility or acceptability in at least one program; ✓✓, evidence of feasibility and acceptability in at least one program; ✓✓✓, evidence of feasibility or acceptability in multiple programs.
Efficacy on risk factor, suicide or suicidal behaviour: 0, no evidence; ✓, evidence of effect in non-experimental study; ✓✓, evidence of effect in one experimental study; ✓✓✓, evidence of effect in multiple experimental studies.
Economic analysis and dissemination: 0, no evidence.
Family
Interventions targeting families use a variety of overlapping strategies and measure multiple outcomes including family conflict and cohesion, parenting styles, antisocial behaviour and academic failure.
Family history of suicidal behaviour
Familial suicidal behaviour is often cited as a risk factor for attempted or completed suicide in young people. This association is commonly attributed to a genetic predisposition to affective disorder. Even after adjustment for mood disorder, Gould et al. [120] reports a fivefold elevation of suicidal behaviour in the relatives of suicide victims by comparison with controls. This study suggests that modelling or transmission of attitudes may be important and potentially modifiable.
Indicated and/or selective interventions
Studies examining indicated or selective interventions targetting family history of suicidal behaviour are not available.
Parental psychopathology
Indicated interventions
Studies examining indicated interventions targetting parental psychopathology are not available.
Selective interventions
Two studies were reviewed, a program promoting self-understanding in adolescents of depressed mothers [121] and the Family Bereavement Program [122]. The Bereavement Program is a 12-session intervention consisting of a family grief workshop and adviser program designed to target the remaining parent and family after a parental death. It focuses on four putative risk mediators: dealing with difficult family events, parental warmth and demoralisation and the promotion of stable positive events such as bedtime talk and regular family meals.
Implementation
More evidence is required to assess the feasibility of these strategies. Problems might include identifying program participants and availability of resources to support the intervention.
Efficacy
Evidence suggests positive outcomes for some relevant indices such as parental warmth and the reduction of depressive symptomatology [121,122]. The significance for youth suicide prevention is unclear.
Family cohesion, conflict and parenting
Several authors have reviewed interventions targeting family management and cohesion [2,5,123]. Family and marital therapies have commonly been used to address family conflict with moderate effect sizes [124].
Indicated interventions
Strayhorn and Weidman [93], targeted low-income families experiencing behavioural problems in their 4–5-year-old children. The intervention, designed to increase positive parent–child interaction, consisted of four or five 2-h group training and play sessions. Instructions included giving approval and reinforcing positive behaviour, giving effective reprimands, using ‘time-out’, modelling pro-social behaviour and non-directive verbalisation of the child's behaviour during play. Teacher ratings at 12-month follow up indicate that children randomised to the intervention improved on attention-deficit-hyperactivity scales with a non-significant trend to higher achievement.
Selective interventions
The Houston Parent–Child Development Project [125] is an example of a selective intervention focusing on economically disadvantaged ethnic families. In the first year of the two-stage program home visits occurred fortnightly with the ‘educator’ promoting mother–child interactions, noting developmental status and use of the home as a learning environment. The second phase included a nursery school element and centre-based parent training dealing with home management and child development. Program attrition was high due to the mobility of Mexican-American families.
Selective interventions have also targeted children of divorced parents with programs typically promoting continued parental involvement with children. Interventions vary in design, but often employ psychoeducation with additional elements of peer support and facilitated expressions of feelings [126–128]. Many use both home and school elements including social support, promotion of social skills and parental involvement through discussions on divorce [129].
Universal interventions
Universal interventions have commonly focused on parenting skills. Some consist of brief interventions addressing communication skills for young couples [130,131]. A brief Australian general practitioner intervention promoting maternal self-esteem and fostering positive child–parent interactions has produced remarkable results [132].
Implementation
It is possible to engage parents in programs in the preschool or primary school years with simple interventions [5,123,124].
Effectiveness
Teacher reports of 8–11-year-old children indicate that control children in the Houston Parent–Child Development Project were more hostile, overactive and likely to be involved in fights [125]. Substantial behavioural differences were seen in children scoring highly on the Stanford–Binet test at 24 months. Universal interventions to diminish conflict and enhance cohesion have long-term benefits for the behaviour and mental health of offspring [130,131]. In the Australian study 90% of the original subjects, between the ages of 27 and 29 years, were reassessed (124 experimental, 122 control) [132]. They reported lower rates of neurotic symptoms, sleep disturbance, tobacco use and higher rates of academic achievement. Females reported lower rates of depressive symptoms [132]. The findings are surprising given the level of intervention.
Cost-effectiveness
Cost–benefits for preschool interventions appear substantial although cost-effectiveness data are not available.
Community interventions
Community interventions have generally targeted ‘suicide-specific’ risk factors.
Availability of lethal methods
Evidence derives largely from interrupted-time-series analyses. Success of a strategy directed at one suicide method depends on the availability of that particular means. Notable Australian examples include the phasing out of coal gas and legislation restricting availability of barbiturates, which had been lethal in overdose. In both instances the longer-term effects are questionable as observations indicate only short-term falls in overall suicide rates [133]. Both restrictions occurred before the current rise in youth suicide.
For a broader discussion readers are referred to the paper by Cantor et al. ‘Access to means of suicide by young Australians’ [134].
Firearms
Evidence is limited regarding compliance with legislative changes by gun owners, the level of enforcement required to implement gun legislation and which elements of legislation are most likely to be effective in restricting access to young people: restriction of ownership, delays in purchase or storage requirements.
Firearm restrictions and the role they play in reducing overall suicide rates remains controversial because of the possible substitution of other methods [135–139]. The introduction of ‘long-arm’ legislation in Queensland was followed by substantial falls in firearm suicides in provincial and metropolitan, but not rural, areas [140]. Falls were particularly marked in 15–29-year-old males. This and other studies suggest a role in the prevention of young male suicides where gun restrictions have not previously been in place [135,141]. The potential for enforcement to make a difference where legislation is already in place or where levels of gun ownership are already low is probably limited [142].
Other means
The rise in non-fatal and fatal self-poisoning with the availability of sedative and anti-inflammatory drugs has been noted in a number of countries [143–145]. There have been recent calls for restrictions on the availability of paracetamol, with data from France suggesting that the use of smaller paracetamol packs is associated with lower overdose rates [146]. Other strategies such as the introduction of methionine and warning messages on paracetamol packs have not been evaluated.
Carbon-monoxide poisoning accounts for approximately one in eight suicides in young males and one in 12 in young females [134]. Possible prevention strategies include fitting catalytic converters or sensors to detect carbon monoxide and exhaust pipe modification. Evidence is not available examining such measures. The introduction of catalytic converters to Australian cars manufactured since 1986 has not been accompanied by a fall in deaths from motor vehicle exhausts despite these cars making up 43% of all registered vehicles [147]. Some overseas data, however, suggest an effect [148].
Hanging accounts for just over one-third of suicide deaths in young Australians [134]. Universal strategies to prevent death by hanging have not been evaluated. Limited prevention control occurs in correctional or inpatient psychiatric settings where restriction appears viable. Trials have not been reported from these settings.
Key questions for strategies focusing on access to lethal means concern the level of penetration needed to affect risk and the extent of substitution by other less easily controlled methods (e.g. hanging).
Media suicide portrayal
The potential role in suicide prevention of restricting media coverage was first raised by a report showing a regional fall in suicide rates coinciding with a newspaper strike in Detroit [149]. In Vienna, railway suicides had been the subject of extensive media attention. Guidelines were introduced in mid-1987 to ensure suicide was reported in a responsible manner. An interrupted-time-series analysis was used to examine the guidelines introduction [150].
Implementation
Evidence suggests that media guidelines can be devised and implemented though probably require constant monitoring. There are little data on the use and penetration of the mass media to provide mental health educational messages to young people. Similarly, the potential benefits and harms that derive from new mediums such as the Internet has, as yet, received little scrutiny.
Effectiveness
The reduction in suicides from railway injury in Vienna was sudden and dramatic at a time when suicide rates were relatively stable. Similarly, there was a dramatic fall in subway suicide attempts. There was some evidence of method substitution, but overall rates of suicide reduced 20% over a 4-year period [150].
Cost-effectiveness
Cost-effectiveness data are not available. Introducing and monitoring media guidelines would be relatively inexpensive. In contrast, mental health education using the mass media is likely to involve considerable expense in program production and purchase of air-time.
School and peer settings
Table 2 highlights the intervention effects at the school and peer level.
Exposure to suicidal behaviour in school peers
For adolescents exposed to suicide or suicide attempts in peers, rates of new onset psychiatric disorder are high [151,152] and some reports indicate that suicidal behaviour is elevated [153,154]. These findings underpin the use of postvention in schools, however, empirical data are scant.
A non-randomised, controlled study examined postvention delivered to secondary students in the Lower Hunter region of New South Wales [155]. This consisted of counselling provided to groups of 20–30 friends of the victim within 7 days of the suicide. A psychiatrist conducted sessions with assistance from school staff.
Implementation
Limited data are available on overall uptake rates and the feasibility of specific intervention elements. Hazell and Lewin [155] highlight difficulties in identifying subjects for intervention.
Efficacy
Evidence is not available on the efficacy of these studies. Postvention could have adverse consequences if it contributes to a romantic or idealised view of the victim [156,157].
School-based interventions to promote resilience
Evidence shows that schools environments' policies and programs have a substantial effect on educational attainment, school retention rates, antisocial behaviour and indices of social competence [158,159]. However, debate surrounds the impact this may have in relation to suicide prevention [160,161].
Selective interventions
Transition from primary to secondary school has been a focus for students at higher risk of academic failure and school disengagement. Elements include re-structuring homerooms to allow continuity with peers and expanding the teachers' role to include giving advice and counselling. Other selective interventions have focused on academic failure in children with low socioeconomic backgrounds. The Comer program, for example, targeted African-American students and included a social calendar, a parent program, visits from a multidisciplinary mental health team and the development of a more democratic and participatory system of school governance [162].
Universal interventions
Classroom-level interventions (i.e. GBG [116]) and whole school strategies (i.e. Project PATHE [108] and the Seattle Social Development Project [77,118]) have been used to reduce school dropout, promote school attachment and academic achievement.
Implementation
Interventions to modify classroom climate are feasible with focused teacher training. It is also possible to modify discrete aspects of the whole-school social climate (e.g. bullying). Evidence on the implementation of multicomponent, whole-school interventions suggest that only 50% of studies will manage to complete all or most elements [108].
Efficacy
There is good evidence that change in classroom and school climate has an impact on proximal risk factors for suicidal behaviour. The GBG, for example, reduced aggression through to year 6, with the biggest improvement in the most aggressive males [116]. As yet, neither suicidal behaviour nor other distal risk factors (depression) have been examined.
Implications for research
An inventory of Australian suicide prevention activities provides little indication of the feasibility of many of the interventions outlined in this report [163]. In most instances study designs, target populations and evaluation strategies are unclear or unavailable. Currently, youth suicide prevention efforts in Australia have focused on clinical interventions for self-harmers, restricting access to means, providing services to higher risk groups (e.g. rural youth and marginalised youth) and enhancing general practitioner responses. Less attention has been given to the development of novel approaches targeting risk factors that sit outside traditional approaches to suicide prevention.
The lack of investment in research designs that can demonstrate effectiveness of piloted interventions is arguably the greatest gap in the current Australian initiative. The inventory of Australian suicide prevention initiatives highlights that only one project outside a clinical setting was listed as using a RCT design [163]. Similarly, of those projects funded under the National Youth Suicide Strategy Prevention, only one, a psychological intervention in youth with a mental illness (The Lifespan Project) was listed as utilising a RCT design. Without the use of appropriate research designs to address the efficacy of interventions, Australia will not make any significant contributions to international efforts to develop effective strategies for suicide prevention.
There is now evidence from North America that there are effective indicated, selective and universal interventions for many important risk factors for suicide. However, there are important exceptions.
Depression
Affective psychopathology stands out as the most important risk factor for suicide and suicidal behaviour in community settings. The limited number of effective interventions for depression is striking. The few available evaluation studies have serious methodological limitations for judging their potential in suicide prevention. Given the linear risk relationship between depressive symptoms and suicidal behaviour, universal or population-based approaches may be of benefit.
Suicidal behaviour
There are no adequately trialed interventions targeting the treatment or prevention of suicidal behaviour in adolescence or young adulthood. Available studies have been marred by poor design. Clinical interventions have been hampered by problems of non-compliance with treatment and poor follow up. There is a need to examine what interventions appear most feasible and effective in clinical settings. Successful interventions may then be modified for use in other settings.
A further consideration is the continued use of interventions for which there is little evidence of efficacy.
Crisis intervention and telephone counselling
Crisis intervention and telephone counselling attracts wide support. These services attract a high-risk female clientele, but neither evidence of effect on suicide rates nor use by young males, the group at most risk, is evident. Given continued investment in this area, evaluation is warranted.
Suicide education programs
Suicide education programs based on the provision of knowledge about suicide risk and the identification of at-risk youth, have been used extensively over 20 years with little or no evidence for their efficacy. In part, this stems from poor evaluation design. Even so, judging from the evidence on the level of intervention required to bring about behavioural change in areas such as adolescent substance use and abuse, it seems unlikely that educational interventions of the kind previously used are likely to be effective. There is scope for considering their incorporation into more comprehensive programs addressing emotional health and social wellbeing. In such a context they may prove useful.
Beyond research into process and efficacy: economic evaluation and dissemination
Economic evaluation of both clinical services and preventive interventions remains a complex and largely unexplored area. An important consideration is that the costs and consequences of intervention (or failure to intervene) are borne not simply by mental health services, but by other government (e.g. education and social services) and non-government sectors. Accurate cost–benefit evaluations require long-term follow up, and, in relation to youth suicide specifically, continued tracing through the period of high risk in young adulthood. Available information suggests that the economic benefits of early childhood interventions and early intervention with juvenile offenders are likely to be substantial [106,164].
Progress has been made with the establishment of the National Death Index to provide a nationwide means of monitoring rates and methods of suicide. However, limited data are available to guide prevention. Such data might address the prevalence of individual outcomes (rates of depression, non-fatal suicidal behaviour) and patterns of service utilisation (general practitioner attendance, use of telephone crisis lines) or prevention activity. Similarly, data on the level of established risk factors in the family (abuse or conflict), community (access to firearms), peer and school domains (school attachment) could provide a framework for intervention delivery.
Currently there is little Australian capacity to provide information and training for community practitioners in the adaptation and implementation of promising interventions. The Centre for Disease Control in the USA has developed a resource guide that might serve as a useful model. It is restricted to a narrow range of programs, but does provide an indication of what should in another setting allow implementation. Elements of the guide include a detailed description of intervention components and steps, availability of training, costs of implementation, tools for monitoring implementation, evidence (if available) of effectiveness and the scope for linkage with other programs. If youth suicide prevention is to move beyond its traditional focus, the development of this capacity to engage and train those working with youth, children and their families will be essential.