
Abstract
Objective:
Suicidal ideation and suicidal behaviour are both regarded as important risk factors for suicide, but it is usually believed that suicidal ideation is less strongly linked to suicide than suicidal behaviours. In this study, we assessed and compared the strengths of the associations that suicidal ideation and suicidal behaviour have with later suicide using meta-analysis of primary studies reporting both these independent variables and the dependent variable of suicide.
Methods:
A total of 51 English language publications describing cohort or controlled studies that reported on both the association between suicidal ideation and suicide and the association between suicidal behaviours and suicide were located using searches for titles in PubMed containing variants of the word suicide (suicid*). Suicides were considered to include reported suicides and open verdicts from mortality registers. The strengths of the two associations were examined in separate random effects meta-analyses and were then compared using mixed effects meta-regression. Subgroups were examined according to study characteristics including the definitions of suicidal ideation or behaviour used, setting (psychiatric or non-psychiatric), diagnostic mix of the study population, study design (cohort or control) and study quality.
Results:
Suicidal ideation (odds ratio = 3.11, 95% confidence interval = 2.51, 3.86) and suicidal behaviours (odds ratio = 4.09, 95% confidence interval = 3.05, 5.49) were both significantly associated with suicide but there was no significant difference in the strengths of association (p = 0.14). Nor were there significant differences in the strengths of the two associations in multiple subgroup analyses.
Conclusion:
Suicidal ideation and suicidal behaviour are both moderately associated with suicide. Existing data cannot conclusively demonstrate that suicidal behaviours are more strongly associated with suicide than suicidal ideation. Clinicians should not strongly prioritise suicidal behaviour over suicidal ideation when considering suicide risk.
Introduction
Previous suicidal behaviour is often regarded as a key risk factor and warning sign for later suicide (Berman, 2018; Bostwick et al., 2016; Gunnell and Lewis, 2005; Smith et al., 2013). A World Health Organization (WHO, 2018) fact-sheet states that ‘a prior suicide attempt is the single most important risk factor’ for suicide. The salience of the association between suicidal behaviour and suicide is also emphasised by leading psychological theories of suicide, such as Joiner’s interpersonal theory of suicide, which suggests that in order for completed suicide to occur, an individual must have both suicidal ideation and an acquired capability to engage in suicidal behaviour. An acquired capability to engage in suicidal behaviour may override the individual’s innate fear of death and tendency towards perseveration of life and can develop as a result of exposure to trauma and violence, non-suicidal self-harming behaviours, substance use and access to means, all of which may increase an individual’s capability to carry out an act that would result in death (Van Orden et al., 2010). Importantly, Joiner’s theory suggests that suicidal ideation and behaviour are separate dimensions, rather than the same construct with differing degrees of severity. Although some studies have reported very strong associations between suicidal behaviour and suicide (Beck et al., 1999; Didham et al., 2006; Hyman et al., 2012), the strength of the association between suicidal behaviours and suicide was called into questioned by a recent meta-analysis by Ribeiro et al. (2016). Ribeiro et al. (2016) found a pooled odds ratio (OR) of suicide associated with suicide attempt of 2.03 (95% confidence interval [CI] = 1.61, 2.57) among a sample of 21 studies, consistent with a weak statistical association that they described as providing ‘marginal improvement in diagnostic accuracy above chance’. Ribeiro et al. (2016) also examined a separate sample of six studies finding that suicidal ideation was associated with suicide with an OR of 1.95 (95% CI = 1.31, 2.90) suggesting that suicidal ideation and behaviour are associated with suicide with a very similar effect size. Ribeiro et al.’s (2016) meta-analysis had the important strength of examining longitudinal studies that were free from possible hindsight and outcome bias in the assessment of suicidal ideation and behaviour. However, the inclusion of un-matched data sets and the exclusion of a large number of controlled studies left open some possibility that suicidal behaviour and suicidal ideation had a similar pooled OR by chance in their study, and that a larger study of matched data for the two independent variables would demonstrate that suicidal behaviour was more strongly associated with suicide than suicidal ideation.
Knowledge of the relative strengths of the associations between suicidal ideation and suicide and suicidal behaviours and suicide is of interest for both theoretical and practical reasons. First, if an acquired capability for suicidal behaviour is a necessary precursor for suicide, then it would be expected that suicidal behaviour would be more strongly associated with suicide than suicidal ideation because suicidal ideation may occur without an acquired capability. Second, people presenting with suicidal behaviour in clinical practice sometimes deny suicidal ideation, and people with suicidal ideation may have a history of suicide attempts (Berman, 2018; Smith et al., 2013). In both situations, the relative weight given to suicidal ideation and suicidal behaviour by clinicians might be important.
The aim of this study was to assess the strengths of the associations between the two independent variables (suicidal ideation and suicidal behaviour) and the dependent variable of suicide in a sample of primary studies reporting both associations. The null hypothesis was that the effect size of the associations between suicidal ideation and suicide and suicidal behaviours and suicide would not be statistically different with an alpha of 0.05 in the main or in any subgroup analyses.
Methods
We extended a previous meta-analysis of the association between suicidal ideation and suicide (McHugh et al., 2019) to include studies also reporting on suicidal behaviour. The extended meta-analysis was registered with PROSPERO (133007) and conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009).
Searches
Preliminary searches of Medline, Embase and PsychINFO from inception to January 2017 looking for papers that examined the association between suicidal ideation and suicide using the word ‘suicide’ as a key word or in the title resulted in an excessive number of results (McHugh et al., 2019), while placing limits using relevant terms such as ‘thoughts’, ‘ideation’ or ‘mortality’ missed relevant papers that were known to the authors from earlier meta-analyses (Chapman et al., 2015; Large et al., 2011b, 2018). In contrast, searches of PubMed using variants of the word suicide in the title reliably located papers known to the authors and those found in searches of multiple databases in earlier studies (Chapman et al., 2015; Hubers et al., 2018). Therefore, and in order to obtain a large and representative sample of relevant studies, one author (M.M.L.) examined the titles of English language publications with an accompanying abstract that contained variants of the single term ‘suicide’ (suicid*) in their title and were published in PubMed from inception to 18 July 2018. The reference list of relevant review articles (Chapman et al., 2015; Franklin et al., 2017; Hubers et al., 2018; Large et al., 2011a, 2011b; McHugh et al., 2019; Ribeiro et al., 2016) was hand searched. Two authors (M.M.L. and C.M.) winnowed the resulting abstracts and full-text publications (see Figure 1, Supplementary Material).
Inclusion and exclusion criteria
Full-text papers were initially examined for cohort or controlled studies that reported the effect size data (ORs, counts or other measures of effect size discrimination) quantifying the association between suicidal ideation and suicide. The resulting papers were then examined for similar effect size data about the association between suicidal behaviours and suicide. Papers that only reported on the association between suicidal ideation and suicide were excluded in order to examine the two independent variables in matched primary study populations and to avoid any possibility of systematic bias associated with an association between the study population and the choice of either suicidal ideation or suicidal behaviours. Hence, we included papers that reported on (1) the expression or non-expression of suicidal ideation, (2) the presence or absence of non-lethal suicidal behaviour and (3) relevant effect size data or counts (true positives, false positives, false negatives and true negatives) related to suicide. We included studies of patients who had received psychiatric care and people recruited from non-psychiatric settings as defined in an earlier meta-analysis of the association between suicidal ideation and suicide (Hubers et al., 2018; McHugh et al., 2019).
We excluded studies in which suicidal ideation and behaviour were assessed by psychological autopsy method, studies in which the non-suicidal controls were deceased and studies of patients with severe medical illnesses such as malignancies or human immunodeficiency virus.
Data extraction and definitions of suicide and suicidal ideation
Two authors (M.M.L. and C.M.) independently extracted the effect size data and the moderator variables. The OR was the preferred data format, followed by raw counts and other effect size data. A third author (A.C.) re-examined the data points. The discrepant points were re-examined by two authors until there was consensus. We accepted the definitions of suicidal behaviour (such as self-harm, suicide attempt, suicidal behaviour) and suicidal ideation (suicidal ideas/ideation/thoughts/threats) as used in the primary research. Data points regarding ‘suicide plans’ were excluded because suicide planning may be considered both ideation and behaviour, in particular if steps have been taken to enact a plan. When studies reported suicidal ideation and suicidal behaviour on a spectrum that assumed that all those with suicidal behaviour had suicidal ideation, estimates for the association between suicidal ideation and suicide were made using those without suicidal ideation or behaviours as the reference category. In these studies, estimates of the association between suicidal behaviour and suicide used those with no suicidal behaviour (including those with suicidal ideation) as the reference category. Where suicidal ideation and suicidal behaviours were recorded as separate categories, we analysed both variables separately using those without suicidal ideation and suicidal behaviours, respectively, as the reference group. In regarding suicidal ideation and suicidal behaviours as separate categories, we were aware that many patients with suicidal behaviour in the primary studies would have had suicidal ideation and some patients with suicidal ideation would have had suicidal behaviour. When papers reported more than one data set for suicidal behaviour or suicidal ideation (e.g. a past history of suicide attempts and recent presentation with suicidal behaviour), we chose most contemporaneous assessment of the two independent variables.
Moderator variables
We collected five moderator variables: (1) study population (whether the study consisted of patients from non-psychiatric settings such as primary care or military settings adopting the nomenclature of earlier research) (Hubers et al., 2018) and samples of psychiatric patients defined by having a schizophrenia spectrum psychosis, a mood disorder or mixed or other psychiatric diagnoses; (2) duration of follow-up between the assessment of the independent variables and possible suicide; (3) whether the study used a cohort of control design; (4) whether the studies reported suicidal ideation and behaviour dimensionally (thus excluding those with suicidal behaviour from the suicidal ideation group) or reported suicidal ideation and suicidal behaviours as independent categories; (5) according to a strength of reporting scale.
Assessment of strength of reporting
Two researchers (M.M.L. and C.M.) independently assessed the reporting strength (and hence the risk of bias of each individual study) of the methods used in the primary research using a scale (scored 0–4) derived from the Strengthening the Reporting of Observational Studies in Epidemiology statement checklist (Von Elm et al., 2007) and used in a related study (McHugh et al., 2019). The term strength of reporting was used instead of study quality to acknowledge that the primary studies were not generally conducted to assess the association between suicidal ideation and suicidal behaviour and suicide and could be regarded as being of adequate quality for their research purpose. One point was allocated according to each of the following criteria: (1) use of a structured method to assess suicidal ideation, (2) collection of data about suicidal ideation and behaviour in a method that was blinded to the patient’s suicide (either by a blinding method or by electronic recording at the point of assessment), (3) ascertainment of suicide using a mortality database and (4) inclusion of open verdicts as suicide. These items were added to produce a 5-point scale (0–4), with a score of 2 or more being considered high quality.
Data synthesis
Random effects meta-analysis was chosen a priori for all estimates because of the diversity of study populations and differences in the methods used in the primary research. As a first analytic step, the two independent variables of suicidal ideation and suicidal behaviour and the dependent variable of suicide were examined in two separate meta-analyses. The effect size data in the primary research data and pooled effect size were expressed in OR. Between-study heterogeneity in effect sizes was examined using I2, Q value statistics. The possibility of publication bias was assessed using a funnel plot and Egger’s regression (Egger et al., 1997). Subgroups were examined in both the estimates of suicidal ideation and suicidal behaviours using a mixed model that assumed a random effect within subgroups and a fixed effect between subgroups. The study null hypothesis was examined in the second analytic step in which the statistical difference between the strength of the associations between suicidal ideation and suicidal behaviour and the null hypothesis was compared using a mixed effects meta-regression of all the studies and within subgroups. For the purpose of the meta-regression, data reporting the association between suicidal ideation and suicide were coded as ‘0’ and used as the reference variable and data reporting with suicidal behaviour were coded as ‘1’ such that a positive coefficient indicated a stronger association between suicidal ideation than suicidal behaviours. Comprehensive Meta-Analysis (CMA; Version 3; Biostat, Englewood, NJ, USA) was used in all analysis.
Results
Systematic searching located 51 publications where both the associations between suicidal behaviour and suicide and the associations between suicidal ideation and suicide were reported (see Table 1). The studies reported on 7,415,193 individuals (mean per study = 146,396, standard deviation [SD] = 859,898), among whom there were 3921 suicides (mean per study = 77, SD = 150). The mean length of follow-up was 5.5 years. These included 8 studies from non-psychiatric populations and 43 from psychiatric populations including 9 studies of people with schizophrenia, 9 studies of people with affective disorder and 25 studies of people with mixed or other psychiatric diagnoses. There were 30 case–control studies and 21 cohort studies. In all, 20 were classified as of lower quality and 31 of higher quality according to our quality scale (see Table 1, Supplementary Material).
Studies reporting on both the association between suicide ideation and suicide and suicide behaviour and suicide.
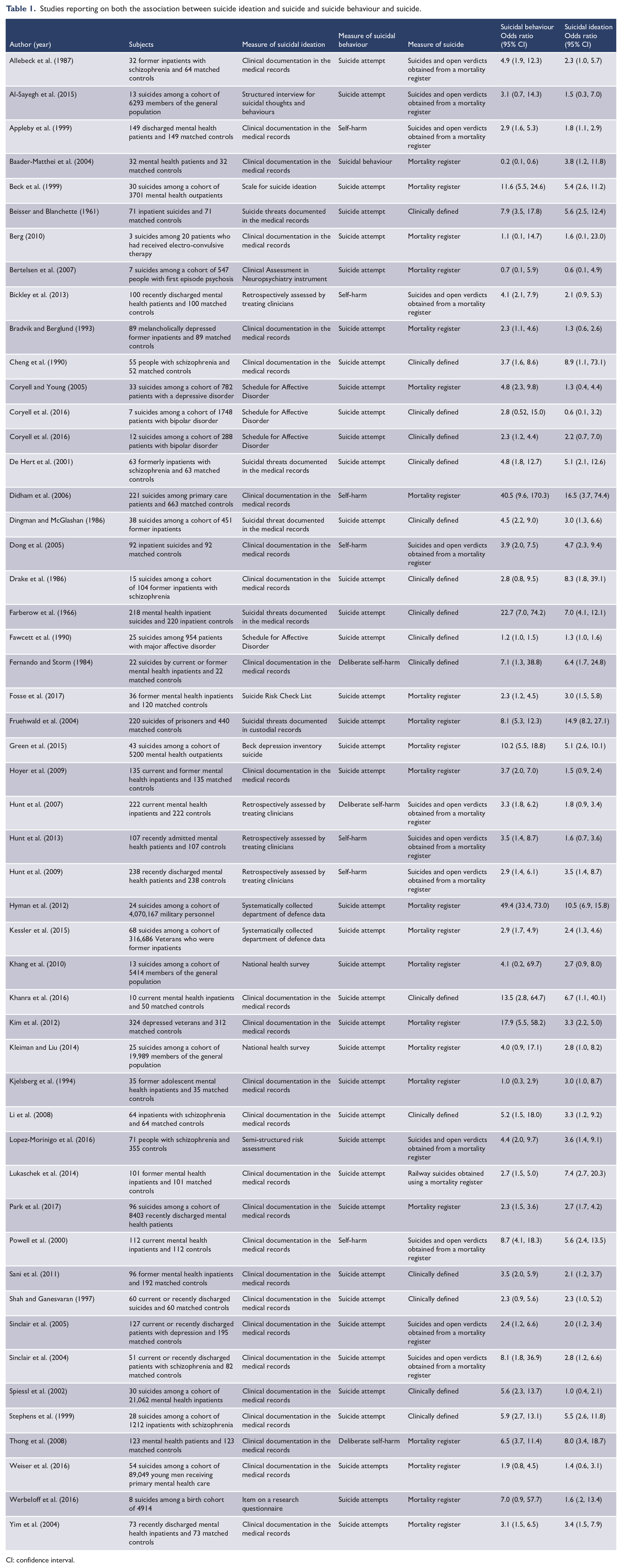
CI: confidence interval.
Suicidal ideation
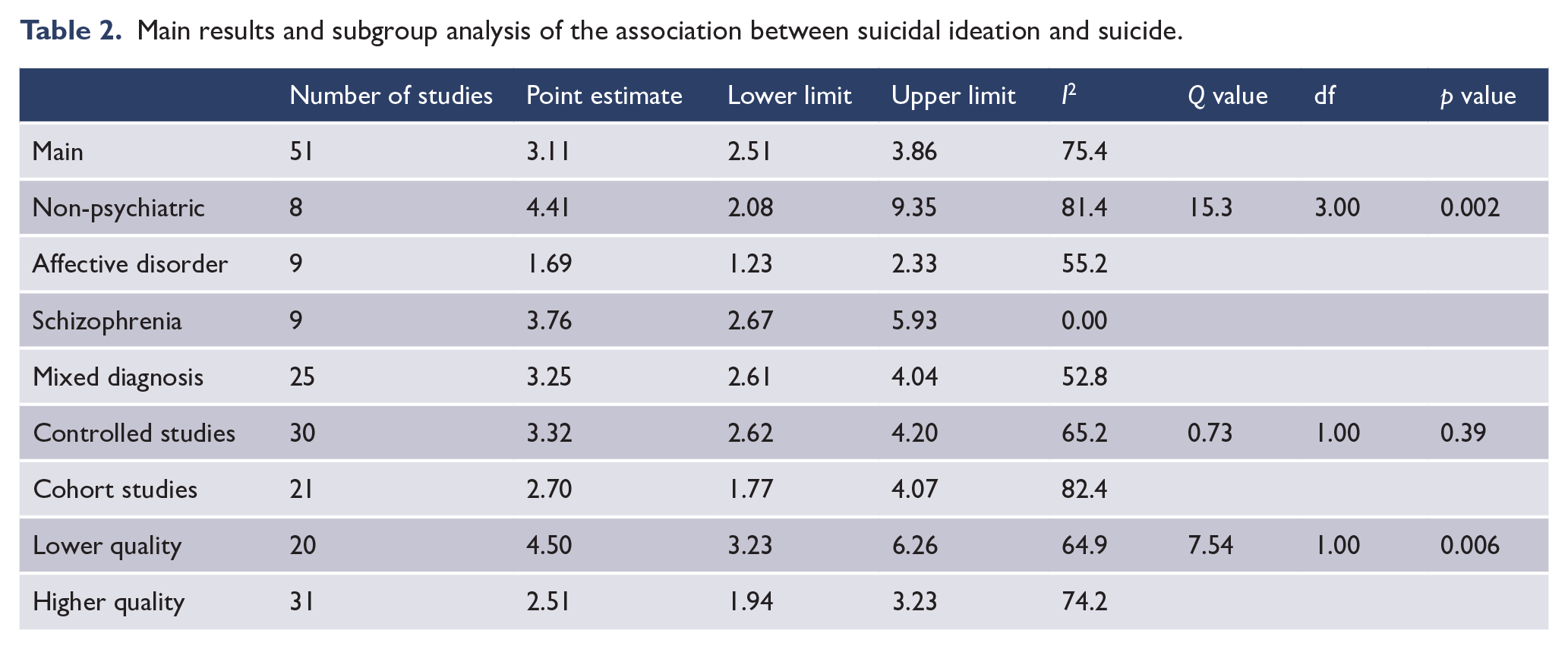
Suicidal ideation was associated with suicide with a median OR of 2.90 and a study range of 0.55 to 16.5 with a pooled OR of 3.11 (see Figure 1). Studies conducted in non-psychiatric settings had the strongest pooled association between suicidal ideation and suicide, while studies of patients with affective disorder had a weaker association (see Table 2). The strength of the association between suicidal ideation and suicide was stronger in a small subgroup of studies that reported on people who were described as making a suicidal ‘threat’ (four studies; OR = 7.82, 95% CI = 4.80, 12.47), than 47 studies that reported on patients with suicidal ideation (OR = 2.83, 95% CI = 2.30, 3.49; Q = 14.1, df = 1, p = 0.001). The association between suicidal ideation and suicide was not associated with the mean duration of follow-up (coefficient = −0.02, 95% CI = −0.06, 0.01, Z = −1.34, p = 0.18). There was no evidence of publication bias on examination of the funnel plot (see Figure 2, Supplementary Material) or by Egger’s regression (intercept = 1.03, df = 49, p = 0.09).
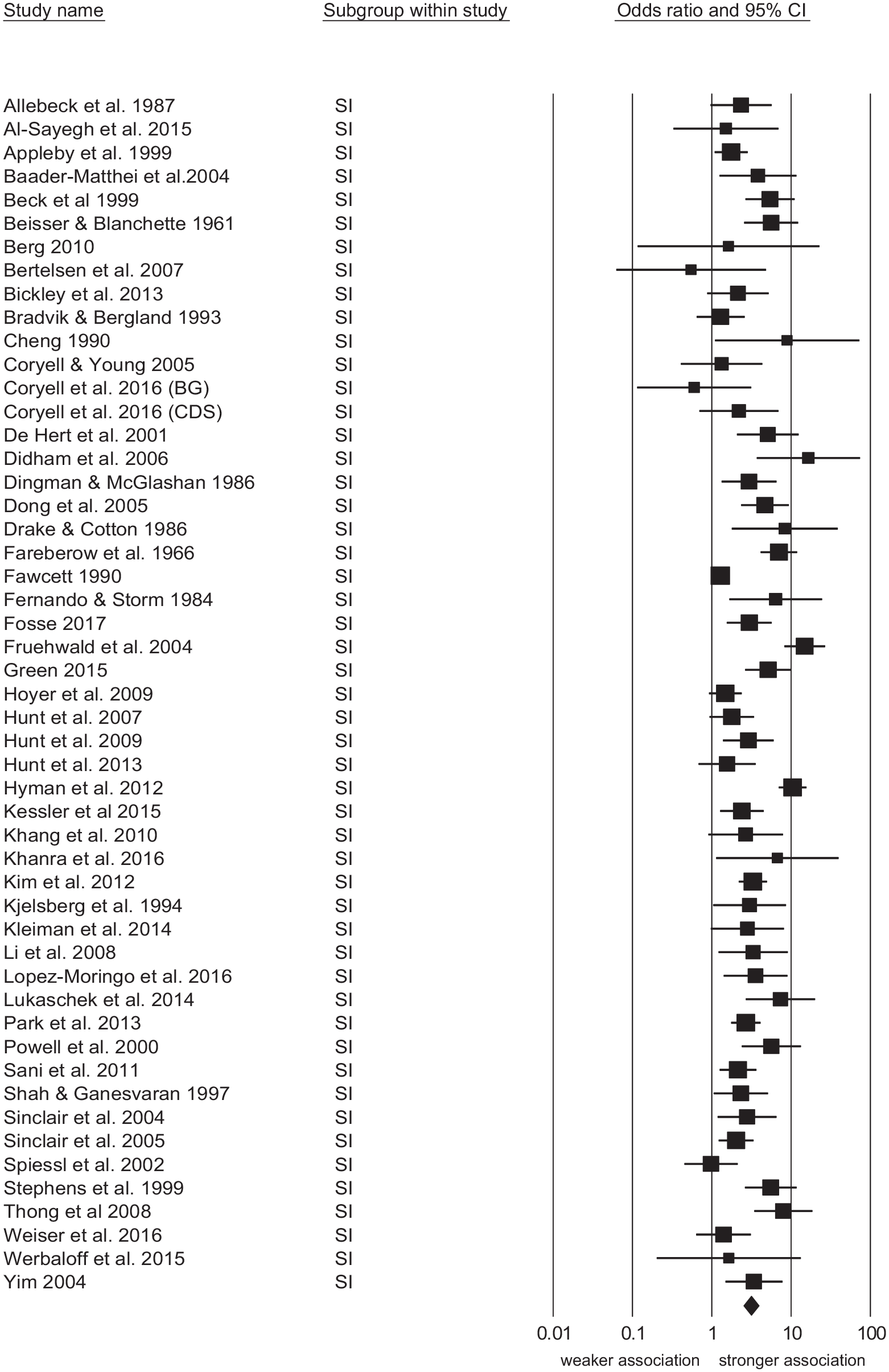
Forest plot of studies reporting the association between suicidal ideation, behaviour and suicide.
Main results and subgroup analysis of the association between suicidal ideation and suicide.
Suicidal behaviour
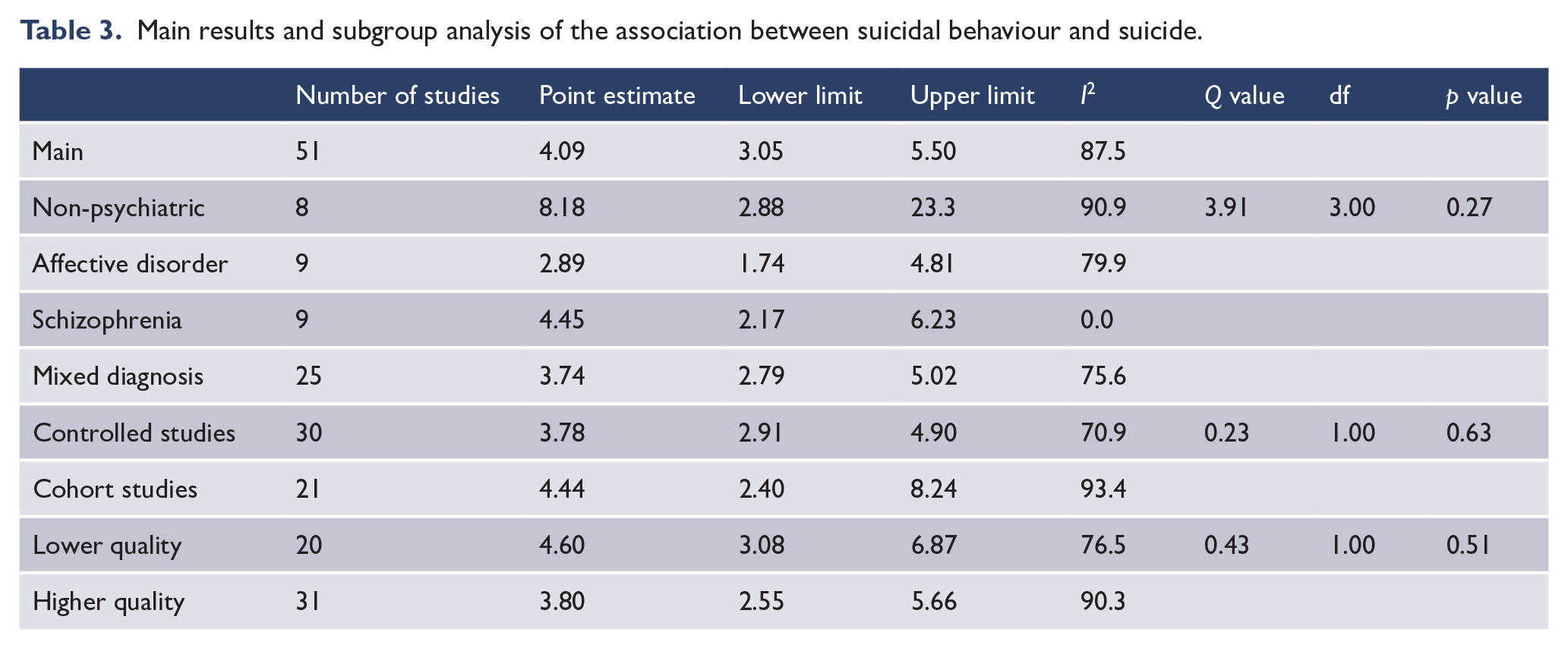
Suicidal behaviour was associated with suicide with median OR of 3.87 and study range of 0.18 to 49.4 with a pooled OR of 4.09 (see Figure 2). Studies conducted in non-psychiatric settings had the strongest pooled association between suicidal behaviour and suicide, while studies of patients with affective disorder had a weaker association (see Table 3). The was no difference in the strength of the association between suicidal behaviour and suicide between the 39 studies that reported on patients with suicide attempts (OR = 4.39, 95% CI = 3.08, 6.24) and 12 studies that reported on patients with self-harm (OR = 3.25, 95% CI = 1.95, 5.40; Q = 0.91, df = 1, p = 0.34). The association between suicidal behaviour and suicide was not influenced by the mean duration of follow-up (coefficient = −0.01, 95% CI = −0.06, 0.04, Z = −0.47, p = 0.64). There was no evidence of publication bias on examination of the funnel plot (see Figure 3, Supplementary Material) or by Egger’s regression (intercept = 0.99, df = 49, p = 0.26).
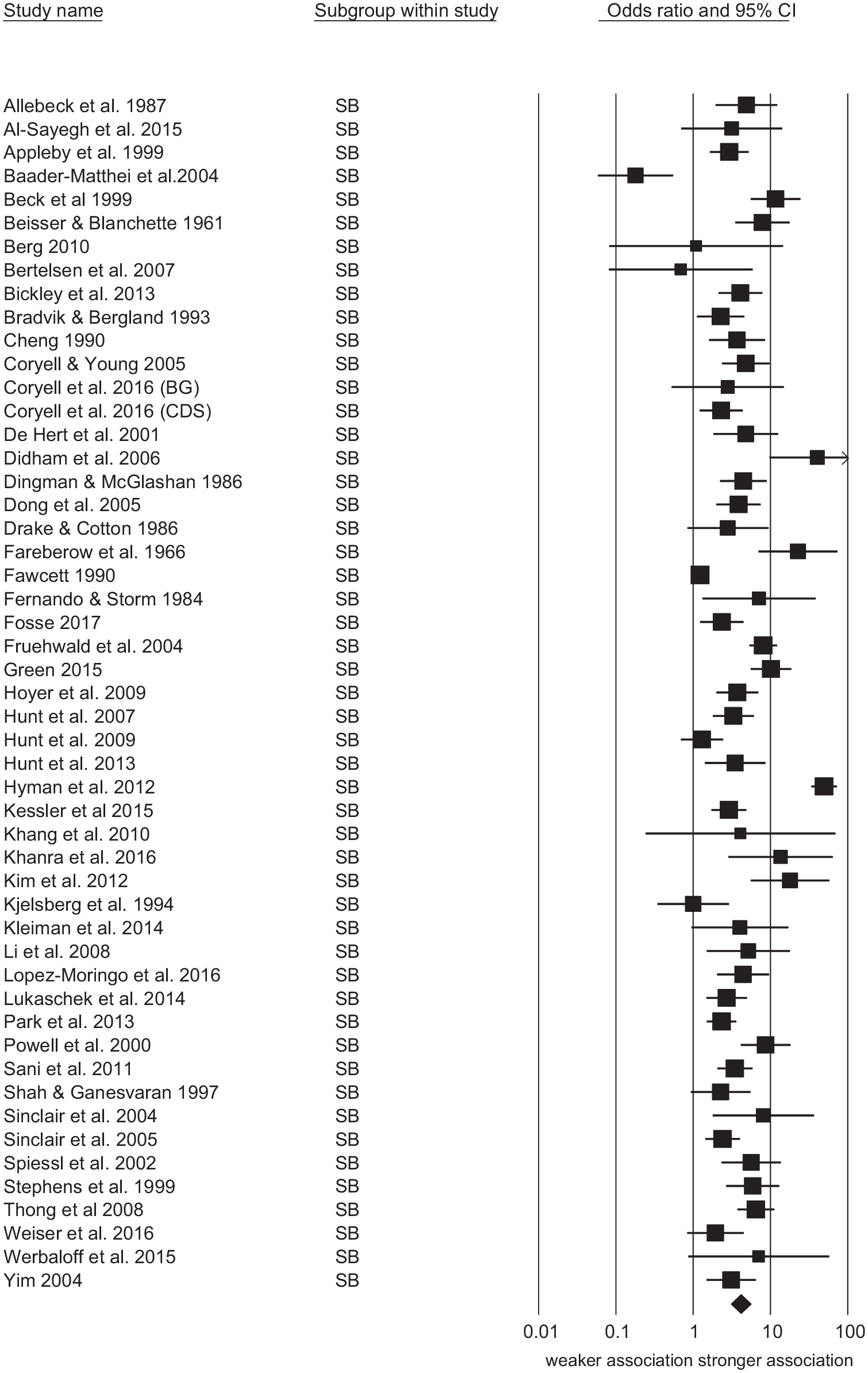
Forest plot of studies reporting association between suicidal behaviour and suicide.
Main results and subgroup analysis of the association between suicidal behaviour and suicide.
Comparison of the strength of the association between suicidal ideation and suicidal behaviours and later suicide
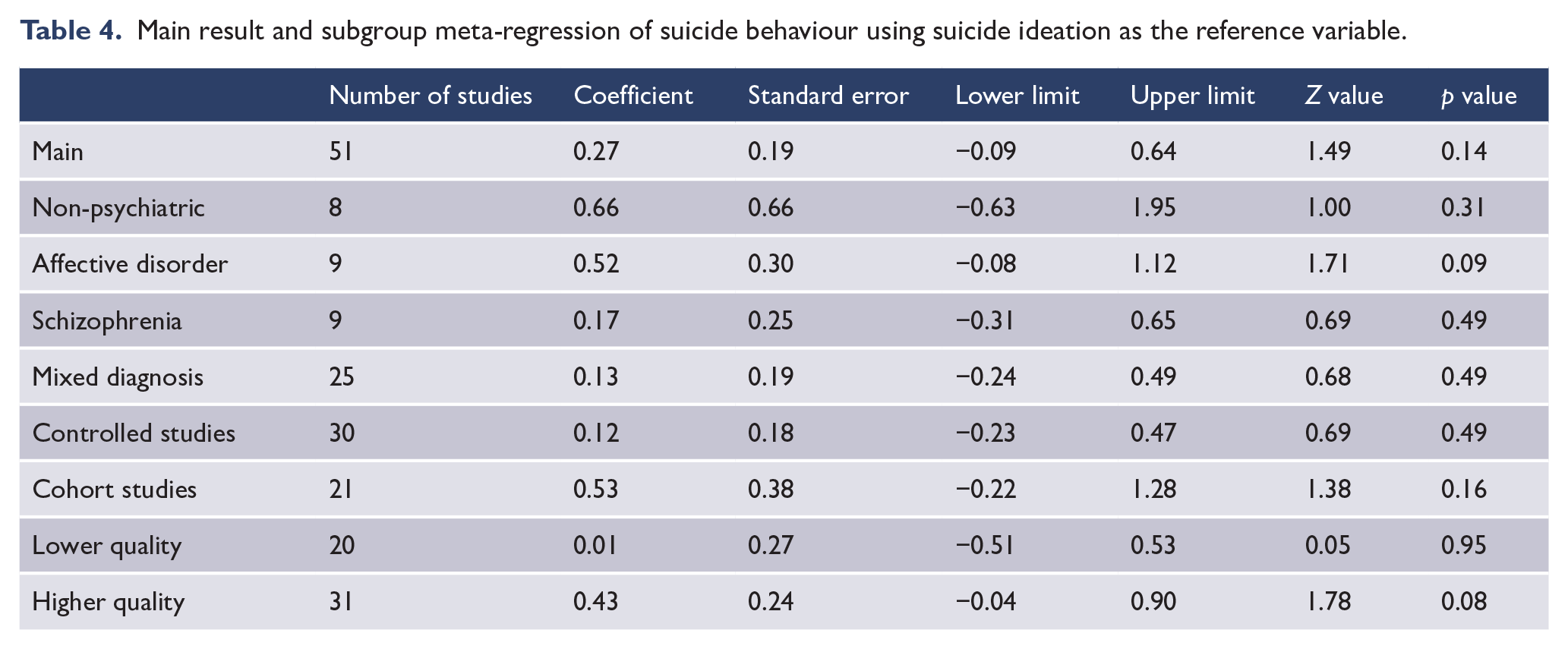
Suicidal behaviours were more strongly associated with suicide than suicidal ideation (OR = 4.06 vs 3.02) but this did not reach significance as assessed with meta-regression (see Table 4). Among six studies that allowed us to exclude people with prior suicidal behaviour from the suicidal ideation group, there was a trend towards a weaker association between suicidal ideation and suicide (six studies; OR = 2.57, 95% CI = 1.63, 4.03) than the association between suicidal behaviour and suicide (six studies; OR = 5.28, 95% CI = 2.72, 10.2; Q = 3.11, df = 1, p = 0.08). There was no difference between the strength of the associations between suicidal ideation and suicide and suicidal behaviour and suicide in subgroups of studies as defined by study setting (non-psychiatric or psychiatric), diagnostic mix of study population, study design (cohort or control) or study quality.
Main result and subgroup meta-regression of suicide behaviour using suicide ideation as the reference variable.
Discussion
Both the independent variables of suicidal ideation and suicidal behaviour are associated with suicide with an effect size that can be qualitatively assessed to be moderate (Rosenthal, 1995) and is similar in the strength of association as that found between male gender and suicide in most countries (Large, 2018). In the main analysis and in each of the subgroup analyses, suicidal behaviour was more strongly associated with suicide than suicidal ideation but this difference did not reach statistical significance and we were not able to reject the null hypothesis. There was a trend towards statistical significance in the subset of six studies in which those with suicidal behaviour were excluded from the suicidal ideation group. Our results should not be interpreted to suggest that future studies will not find a significant difference in the strength of the association between suicide and either suicidal ideation or suicidal behaviour. The consistency of non-significantly stronger association between suicidal behaviour in all subgroups does suggest that suicidal behaviour might be eventually shown to be more strongly associated with suicide than suicidal ideation as more data become available. However, our data suggest that any difference in statistical strength is likely to be small and of dubious clinical significance.
This study also provided an opportunity to assess whether measurement of dimensions of suicidal thoughts and behaviour impacts the strength of associations that are found between these distinct, but overlapping constructs, and later suicide. As mentioned, our previous meta-analysis (McHugh et al., 2019) assessed the strength of association between suicidal ideation and later suicide. Of the 71 studies in that meta-analysis, 51 measured suicidal ideation and behaviour separately and were thus included in this meta-analysis. The remaining 22 studies were not included as they did not include a measure of suicidal behaviour. While in the previous meta-analysis we found a pooled OR for suicidal ideation of 3.41, the current meta-analysis found an OR of 3.11. This indicates that studies that only report on suicidal ideation and not suicidal behaviour may tend to report a slightly higher OR. This may also be true for studies that report on suicidal behaviour only; however, we were not able to compare that data as the prior review focused on ideation only.
The main weakness of this study flowed from the conceptualisation of suicidal ideation and suicidal behaviours as categorically independent entities in all but six studies. In reality, it is likely that most patients classified as having suicidal behaviours had suicidal ideation and that many patients with suicidal ideation had a history of suicidal behaviour. This overlap between the two variables would lessen the extent of any difference in the strength of the two associations in 45 of the 51 included studies and in our meta-analytic result. Specifically, the inclusion of patients with suicidal behaviour in the suicidal ideation group might increase the observed association between suicidal ideation and suicide, lessening the possibility of finding a difference in the extent of the associations between these two variables and suicide. Despite the above caveat, we believe that the result of our study is somewhat surprising to the extent that we found that the objective sign of suicidal behaviour was not very much more strongly associated with suicide than the subjective symptom of suicidal ideation and that this difference did not reach statistical significance despite a highly powered meta-analysis. Prior to conducting this study, we held the opinion that suicidal behaviours were likely to be more strongly associated with suicide than suicidal ideation and formulated our hypothesis accordingly. We believed a priori that suicidal ideation would be less strongly associated with suicidal behaviours because they can be regarded as a communication of a persons’ inner world and level of distress rather than behaviour per se. Further suicidal ideation is much more common than suicidal behaviours (Johnston et al., 2009) and can be conceptualised as being dynamic and fluctuating over time, lessening the likely strength of any association. In contrast, suicidal behaviour is more static and objective and therefore a potentially reliable marker of suicide in line with a large body of research that suggests that actuarial prediction usually outperforms clinical prediction (Dawes et al., 1989). Moreover, one might expect suicidal behaviour to be more strongly associated with suicide because it is more similar to suicide, with both involving self-destructive behaviour and an acquired capability for self-harm (Van Orden et al., 2010). After this study, we modified our opinions about the relative strengths of the association between suicidal ideation and suicidal behaviours and considered that our results might be because people may be more reliable in their reporting of suicidal ideation than might generally be believed (Berman, 2018) and/or that the recording of suicidal behaviour is either less reliable (Eikelenboom et al., 2014) or less accurate (Hart et al., 2013) than one might imagine.
Conclusion
The results of this study are clinically relevant in that it is not rare for patients to present with suicidal behaviour yet deny current suicidal ideation while other patients will present with suicidal ideation in the absence of suicidal behaviour. This study suggests that, to the extent to which suicidal ideation and behaviours are conceptualised as risk factors, patients with either of these phenomena are more or less equal but only modestly increased risk of suicide. Patients with suicidal ideation only should not be dismissed as not having suicidal behaviour and there is no strong reason why people with suicidal behaviours should receive more restrictive mental health care than those with suicidal ideation only. The study also has some implications for future primary studies. Studies that report suicidal ideation and suicidal behaviours as both dimensional and categorical risk factors could more fully discriminate between the two risk factors. Highly powered primary studies and future meta-analyses might further clarify the relative strengths of these two common and important clinical aspects of suicidality.
While we urge clinicians to make very careful assessments of both past suicidal behaviour and of suicidal ideation, our results suggest that presently there are no strong grounds to put particular emphasis on suicidal behaviour over suicidal ideation.
Supplemental Material
Suppl._Material – Supplemental material for Is suicidal behaviour a stronger predictor of later suicide than suicidal ideation? A systematic review and meta-analysis
Supplemental material, Suppl._Material for Is suicidal behaviour a stronger predictor of later suicide than suicidal ideation? A systematic review and meta-analysis by Matthew Large, Amy Corderoy and Catherine McHugh in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: M.M.L. received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. C.M. received a New Investigator Grant from the Royal Australia and New Zealand College of Psychiatry.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.