
Abstract
Objective:
Individuals with a depressive and/or anxiety disorder are known to have an elevated risk of suicide. However, these diagnoses alone are insufficient at differentiating patients with suicide ideation that attempt suicide from those that do not. Few studies examined such differences in an ideation-to-action framework. Using this framework, extensive multivariate testing was performed to examine differences between suicidal patients with and without a suicide attempt.
Method:
Data were from 1576 respondents with a depressive and/or anxiety disorder, participating in the Netherlands Study of Depression and Anxiety. Logistic regression analyses were used to analyze associations between sociodemographic, clinical, personality, and psychosocial risk factors and suicide ideation and attempt.
Results:
Patients with suicide ideation could be uniquely distinguished from non-suicidal patients by more years of education, presence of a depressive disorder (vs anxiety disorder) and higher introversion. Patients with suicide ideation and a past suicide attempt could be uniquely distinguished from non-suicidal patients by a younger age of onset, a lifetime alcohol use disorder, more external locus of control and lower levels of social support. Within the group of patients with suicide ideation, patients with a suicide attempt were more likely to have childhood trauma and lower education, and be of non-Western descent than patients with suicide ideation and no past attempt.
Conclusion:
This study found that although various clinical, personality and psychosocial characteristics distinguish patients with suicide ideation from non-suicidal patients, many of these often-cited factors do not distinguish patients with a suicide attempt from those who only think about suicide. However, childhood trauma, lower education and non-Western descent could aid in detecting suicide attempt risk among patients with suicide ideation.
Introduction
Suicide is a worldwide concern that accounts for 1.4% of all deaths (World Health Organization [WHO], 2014) and is frequently paired with mental health problems. Studies indicate that about 60% of those who died by suicide had a depressive disorder (Cavanagh et al., 2003) and that the presence of an anxiety disorder also significantly increases suicide risk (Bentley et al., 2016). Patients with a comorbid depressive and anxiety disorder are found to be at even greater suicide risk than patients with either disorder alone (Eikelenboom et al., 2012). Despite the elevated suicide risk among these patients, identifying who will act on suicidal thoughts remains a major challenge. A large proportion may think about suicide, but the majority will not perform suicidal behavior. For example, a study by Baldessarini et al. (2019) indicated that 17.3% of individuals with a major depressive disorder had a lifetime risk of suicidal ideation, but lifetime risk of a suicide attempt was 4.8%. Therefore, ways of distinguishing patients who will attempt suicide from those who will not require further development and identification of risk factors over and above psychiatric disorders mentioned.
A multitude of studies have found risk factors for suicide ideation or suicide attempt among patients with a depressive and/or anxiety disorder (e.g. Bolton et al., 2010; Eikelenboom et al., 2012). However, many of these studies focus on suicide ideation, suicidal behavior or their combination (May and Klonsky, 2016). Therefore, these designs did not allow the disentanglement of risk factors specific to ideation or attempt from those that are common to both (May and Klonsky, 2016).
A relatively small number of studies compared both suicide ideation and suicide attempt relative to non-suicidal groups in individuals with a depressive disorder specifically. Sokero et al. (2003) found that in comparison with non-suicidal patients, both ideation and attempt groups had higher levels of psychopathology and lower levels of social functioning. Spijker et al. (2010) found that patients with suicide ideation had, in comparison with non-suicidal patients, more and a longer duration of mood disorders, comorbid anxiety, previous suicidal ideation and greater use of professional care. As compared to non-suicidal patients, patients with a suicide attempt were more likely to report having had previous suicidal thoughts, a previous suicide attempt, the presence of comorbid anxiety and living without a partner. Although such results shine some light on similarities and differences between ideation and attempt groups relative to non-suicidal patients, information on which patients with suicidal thoughts are most likely to act on these thoughts is still lacking.
According to May and Klonsky’s (2016) ‘ideation-to-action framework’, the development of suicide ideation and the progression from ideation to attempt are two distinct processes with their own explanations and predictors. Also focusing on a direct comparison between ideation with and without a history of attempt could therefore potentially increase sensitivity and specificity when it comes to predicting suicide risk.
The number of suicide risk factor studies that fit within the ideation-to-action framework is limited (May and Klonsky, 2016). May and Klonsky (2016) included such studies in a meta-analysis. Remarkably, their results suggested that few putative correlates of suicidality (e.g. depression, alcohol use disorder and hopelessness) could properly differentiate the attempt group from the ideation group. The only factors that distinguished attempt from ideation with a modest effect were the presence of an anxiety disorder, post-traumatic stress disorder (PTSD), drug problems or a history of sexual abuse. However, as a result of a narrow selection of predictor variables in studies included in the meta-analysis, variables were mainly limited to a small number of proximal sociodemographic and clinical variables. Therefore, a number of putative suicide risk factors require further investigation.
With regard to clinical variables, studies comparing suicide ideation and attempt directly focused mainly on psychiatric diagnoses (May and Klonsky, 2016). Variables such as age of onset or duration of a psychiatric disorder and psychiatric treatment have also been found to distinguish depressed patients with suicide ideation or a past attempt from non-suicidal patients (Claassen et al., 2007; Spijker et al., 2010) and should be applied to an ideation-to-action framework. In addition, studies comparing suicide ideation and attempt seldomly correct for depression severity (May and Klonsky, 2016), a variable referred to as one of the three most important predictors of a suicidal act in patients with a mood disorder (Oquendo et al., 2004).
Personality and psychosocial variables are considered to comprise major risk domains for suicide attempts as well (Brezo et al., 2007). A systematic review by Brezo et al. (2006) highlights associations between distal risk factors such as aggression, neuroticism and extroversion and a history of suicide attempts. Psychosocial variables such as stressful life events, childhood abuse and social support have also frequently been linked with increased suicide risk (Lee and Jung, 2006). Nevertheless, few examples exist of studies that applied such variables in the ideation-to-action framework.
Overall, the literature suggests that the ideation-to-action framework is rarely applied, small subsamples are often used and more clarity is required about the role of previously identified proximal and distal suicide risk factors in the progression from suicidal thoughts to a suicide attempt. This needs to be done by concurrently testing such variables in comprehensive multivariate analyses to identify the extent to which these variables have an independent effect on ideation-to-action processes. In addition, studies comparing suicide ideation and attempt directly in samples with mental disorders are lacking (Pérez et al., 2016) and could offer insight into risk factors that transcend psychiatric diagnoses. Thus, the present study aims to apply the ideation-to-action framework to investigate whether a wide range of often-cited sociodemographic, clinical, personality and psychosocial variables can distinguish patients with suicide ideation and no previous suicide attempt and patients with suicide ideation and a history of attempt from (1) non-suicidal patients and (2) each other in a large sample consisting of individuals with a depressive and/or anxiety disorder. By performing extensive multivariate analyses, we intend to gain information that could improve the detection of patients at risk of suicide.
Method
Sample
Baseline assessment data were used from the Netherlands Study of Depression and Anxiety (NESDA), a longitudinal cohort study investigating the long-term course of depression and anxiety and impact of various factors on their development. The initial sample contained 2981 respondents (age 18–65 years) who did or did not have symptoms of anxiety and/or depression. Respondents were recruited between September 2004 and March 2007 from the community (18.9%), primary care (54.0%) and mental health care centers (27.1%) across the Netherlands. Respondents with a primary diagnosis of other clinically overt psychiatric disorders (e.g. obsessive-compulsive, bipolar, severe addiction or psychotic disorder) or not sufficiently mastering the Dutch language were excluded. The Research Ethics Committee of the VU University Medical Center (2003/183) approved the study. All respondents signed informed consent after being informed about the study verbally and in writing. For a detailed description of the NESDA study, see Penninx et al. (2008).
For the present study, 1576 respondents were selected who had a depressive and/or anxiety disorder in the 12 months prior to baseline assessment and provided information regarding current suicide ideation and lifetime attempt. Of the 1576 respondents, 376 (23.9%) had a pure depressive disorder, 471 (29.9%) had a pure anxiety disorder and 729 (46.3%) had a comorbid depressive and anxiety disorder. Furthermore, 1250 (79.3%) respondents had no current suicidal ideation and no lifetime attempt, 231 (14.7%) had current suicidal ideation without a lifetime attempt and 95 (6.0%) had current suicidal ideation with a lifetime attempt. Respondents with a lifetime attempt and without current suicide ideation (n = 198) were excluded, because comparing such patients to currently suicidal patients would essentially entail comparing a current crisis with a crisis in the past (May and Klonsky, 2016).
Measurement of suicidality
Suicide ideation was measured using the five-item semi-structured interview version of the Scale for Suicide Ideation (SSI; Beck et al., 1979), which scores the extent to which thoughts of suicide were present in the past week. Beck et al. (1979) found a high internal consistency (α = 0.89) for the SSI and it was also high in the present study (α = 0.79). Current suicidal ideation was defined as scoring positively on one SSI item. Presence of a lifetime suicide attempt was measured using the question: ‘Have you ever made a serious attempt to end your life, for instance by harming or poisoning yourself or by getting into an accident?’ The question was taken from the WHO/Euro multicenter study on parasuicide (Platt et al., 1992).
Psychopathology and clinical characteristics
All respondents were clinically assessed using the Composite Interview Diagnostic Instrument (CIDI) version 2.1, for diagnoses as defined by the Diagnostic and Statistical Manual of Mental Disorders (4th ed., DSM-IV) classification system (American Psychiatric Association, 2001). The Diagnostic and Statistical Manual of Mental Disorders (5th ed., DSM-5) was only published after gathering the data for the present study. The CIDI has been found to have a sound reliability and validity (Wittchen, 1994). The instrument was administered by clinically trained research assistants. In the current study, respondents with a depressive (major depression and dysthymia) and/or anxiety disorder (social phobia, panic disorder, agoraphobia and generalized anxiety disorder) in the past 12 months were included.
Lifetime alcohol use disorder and the age of onset of an anxiety and depressive disorder were also assessed using the CIDI. If a comorbid depressive and anxiety disorder was present, the disorder that appeared first was used to determine age of onset. The Life Chart Interview was used to measure the duration of symptoms (Lyketsos et al., 1994). In the present study, the percentage of time with anxiety or depressive symptoms was measured over a period of 4 years prior to baseline (ranging from 0% to 100% of the time with symptoms).
Use of psychiatric treatment was measured by the presence or absence of psychotherapy and/or counseling in the past 6 months and/or frequent current antidepressant use. The former was measured using the Treatment Inventory of Costs in Patients with psychiatric disorders (TiC-P; Hakkaart-Van Roijen, 2002). The latter was measured by classifying medication used in the past month (according to the Anatomical Therapeutic Chemical [ATC]) and asking about medication adherence in the past month.
Severity of depression was measured using the 30-item self-report version of the Inventory of Depressive Symptomatology (IDS-SR; Rush et al., 1996). According to Rush et al. (1996), the instrument has good psychometric properties. The internal consistency of the IDS-SR was high in the present study (α = 0.88). Item 18, which assesses suicide ideation, was removed in all statistical analyses to prevent circularity.
Sociodemographics
Included were gender, age, years of education, net household income expressed in euros per month and employment status ((self)-employed, unemployed, sick or incapacitated, and other). Being of Western descent was based on nationality and country of birth of the participant (if these were both from the Netherlands, other European countries [excluding Turkey], the USA or Canada, this determined a Western descent).
Personality traits
A shortened five-item version of the Pearlin Mastery Scale (PMS; Ormel et al., 1992; Pearlin and Schooler, 1978) measured locus of control. A previous study (Penninx et al., 1997) found a reasonable internal consistency for this measure (α = 0.67), while the present study finds this measure to have an excellent reliability (α = 0.97). The Big Five personality traits neuroticism, extraversion, openness, agreeableness and conscientiousness were measured using the 60-item NEO-Five Factor Inventory (NEO-FFI). This measure has good psychometric properties (Murray et al., 2003) and the internal consistency of the subscales ranges from reasonable to high (α = 0.69–0.82) in our sample. Cognitions experienced in a sad state related to hopelessness, acceptance/coping, aggression, control/perfectionism, risk aversion and rumination were measured using the Leiden Index of Depression Sensitivity–Revised (LEIDS-R; Van der Does, 2002). For the same reason as removing IDS-SR item 18, suicide items in the Hopelessness subscale of the LEIDS-R were removed. The LEIDS-R has good psychometric properties (Solis et al., 2017) and the internal consistency of subscales in our sample was found to range from reasonable to high (α = 0.60–0.80).
Psychosocial
Partner status was labeled as having a partner or not. The Close Persons Questionnaire measures the level of social support given by a partner and two confidants at most and was found to have a good reliability and validity (Stansfeld and Marmot, 1992). The internal consistency in our sample for this measure is high (α = 0.76). The absence of partner or confidant resulted in a zero score for the partner or confidant in question. Sum scores were created for the partner and each confident and the resulting sum scores together formed a total social support score. The 11-item self-report Loneliness Scale (De Jong-Gierveld and van Tilburg, 1999) was used to measure loneliness. The internal consistency of this scale was found to be high to excellent in previous research (König-Zahn et al., 1994) as well as our sample (α = 0.99).
Early traumatic life events were measured using the Childhood Trauma Interview (CTI; De Graaf et al., 2002). Specifically, the occurrence and frequency of emotional neglect, psychological abuse, physical abuse and sexual abuse experienced in the first 16 years of the participant’s life were measured. As was done in an earlier study (Eikelenboom et al., 2019), a total score was created by creating a cumulative index (range 0–8) of the frequency of each childhood trauma (0 = never, 1 = once, sometimes and 2 = regularly, often, very often) per participant. The scores on the cumulative childhood trauma index were subsequently categorized into five categories ranging from 0 to 4 (0 = 0, 1 = 1–2, 2 = 3–4, 3 = 5–6 and 4 = 7–8). Recent negative life events were measured using the Recent Life Events Questionnaire, which measures the number of life events in the past 12 months and was found to have good psychometric properties (Brugha and Cragg, 1990).
Statistical analysis
There were several continuous variables with missing data (see Table 1). The number of missings ranged from 0.0% to 15.5%. Only the LEIDS-R, PMS and Loneliness Scale had more than 3.0% missing. Missings were replaced using the multiple imputation method Fully Conditional Specification based on Liu and De’s (2015) guidelines. A total of 100 imputations were performed and results in the present study are based on pooled estimates. The multiple imputation method assumes that the data are missing at random (MAR). Missing data were evaluated to get an indication of what mechanism might be causing the missing data using guidelines by Heymans and Eekhout (2019). Given the evidence, missing data were considered MAR. Group differences were evaluated using chi-square tests for categorical variables and analyses of variance for continuous variables.
Sample characteristics of patients with a depressive and/or anxiety disorder in the past 12 months according to suicidal status (n = 1576).
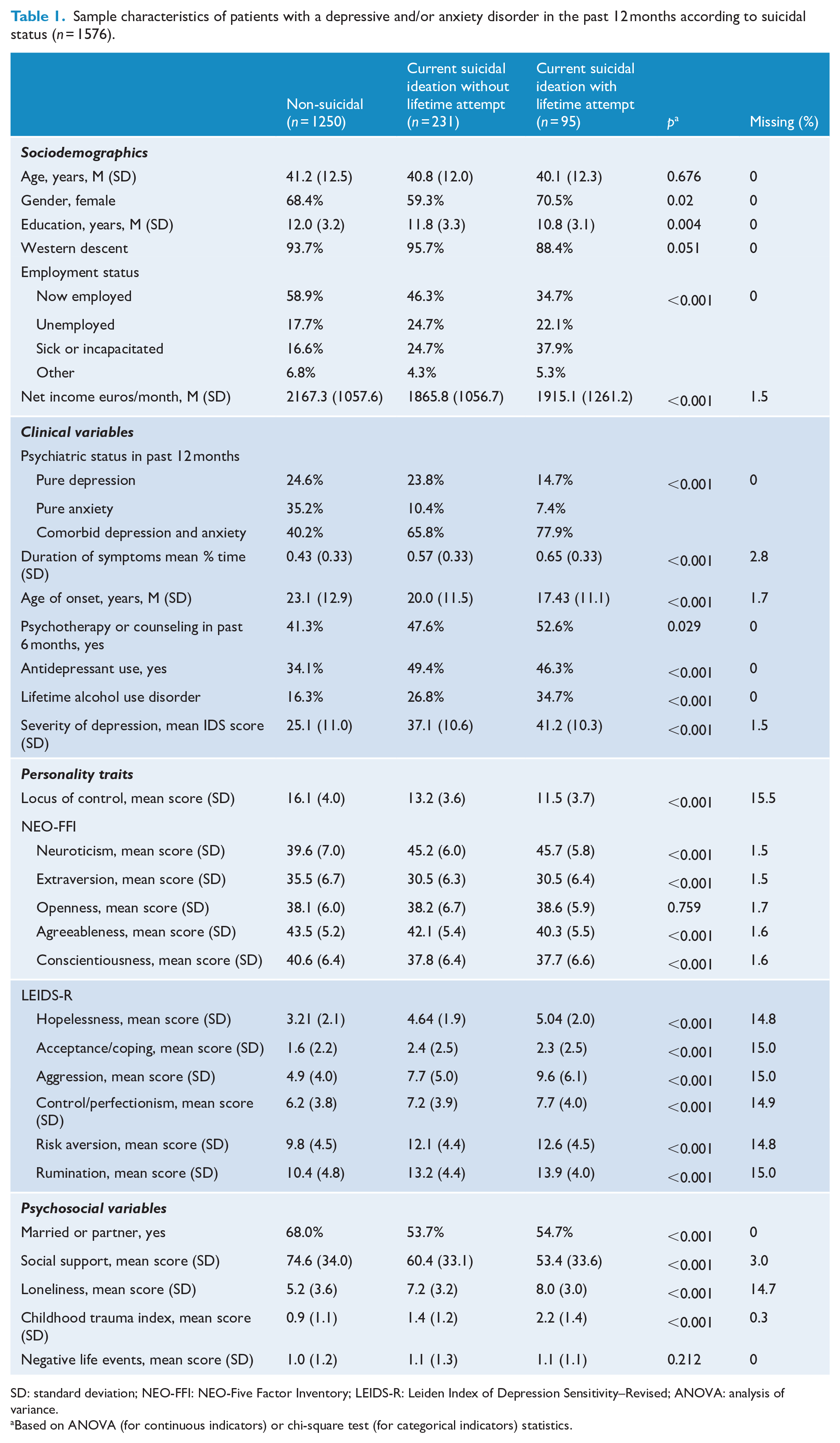
SD: standard deviation; NEO-FFI: NEO-Five Factor Inventory; LEIDS-R: Leiden Index of Depression Sensitivity–Revised; ANOVA: analysis of variance.
Based on ANOVA (for continuous indicators) or chi-square test (for categorical indicators) statistics.
To investigate associations between the predictor variables and the outcomes, logistic regression analyses were applied. A series of steps were taken to reach the final models using the forced entry method in each step. First, univariate multinomial logistic regression analyses were conducted that compared patients with suicide ideation with and without a suicide attempt to non-suicidal patients. Next, variable clusters (sociodemographic, clinical, personality, psychosocial) were analyzed using multivariate multinomial logistic regression analyses, using only variables that were significant at a p < 0.10 level in univariate analyses. Finally, all predictors significantly (p < 0.10) associated with an outcome variable in per cluster analyses were then simultaneously entered into a multivariate analysis to reach the final model. The method used was meant to retain only the strongest predictors per cluster in the final multivariate analysis and to minimize over-fitting. Also, it could give an indication of the predictive contribution of each domain. In order to directly compare suicidal patients with and without a suicide attempt (without the non-suicidal group), a similar stepwise method was repeated in logistic regression analyses. Associations in the final models were considered statistically significant if p value <0.05. Variance inflation factor (VIF) and tolerance values did not indicate a multicollinearity problem. IBM SPSS version 25.0 for Mac was used to conduct statistical analyses.
Results
Clinical characteristics
The analytic sample (N = 1576) had a mean age of 41.1 years (SD = 12.4) and 67.2% of the respondents were female. Sample characteristics for the respondents were split up according to the outcomes in Table 1. In the suicide attempt group, respondents had an average of 2.05 (SD = 1.61) previous attempts and the average number of years since last attempt was 8.80 (SD = 10.30) years. In total, 27.4% of the suicide attempt group reported an attempt in the past year and 52.8% in the past 5 years.
Univariate and multivariate analyses
For studying predictors of suicide ideation and suicide attempts using non-suicidal patients as the reference group, only the final model is presented (see Table 2). In the univariate and per-domain analyses (see Supplemental Table S1 and S2, respectively), predictors for the suicide ideation and suicide attempt group hardly differed. In both analyses, suicide ideation and suicide attempt were significantly predicted by various clinical variables (younger age of onset, presence of comorbid depressive and anxiety disorder vs pure anxiety disorder, presence of alcohol use disorder and higher severity of depression), personality variables (high external locus of control, introversion and aggression), psychosocial variables (low social support, more loneliness and more childhood trauma) and being non-employed due to sickness or incapacitation. In the final multivariate analysis, many associations lost statistical significance, yet the suicide ideation and suicide attempt group continued to share a number of predictors. The suicide ideation and suicide attempt outcomes were both significantly predicted by a comorbid depressive and anxiety disorder, higher severity of depression, higher levels of aggression and increased childhood trauma. However, only the suicide ideation group was significantly predicted by more years of education, the presence of pure depressive disorder (vs the presence of pure anxiety disorder) and introversion. Only the suicide attempt group was significantly predicted by a lower age of onset of a depressive or anxiety disorder, comorbid lifetime alcohol use disorder, higher external locus of control and lower social support.
Determinants of suicide ideation with and without a history of suicide attempt in patients with a depressive and/or anxiety disorder in the past 12 months (multivariate multinomial logistic regression analysis).
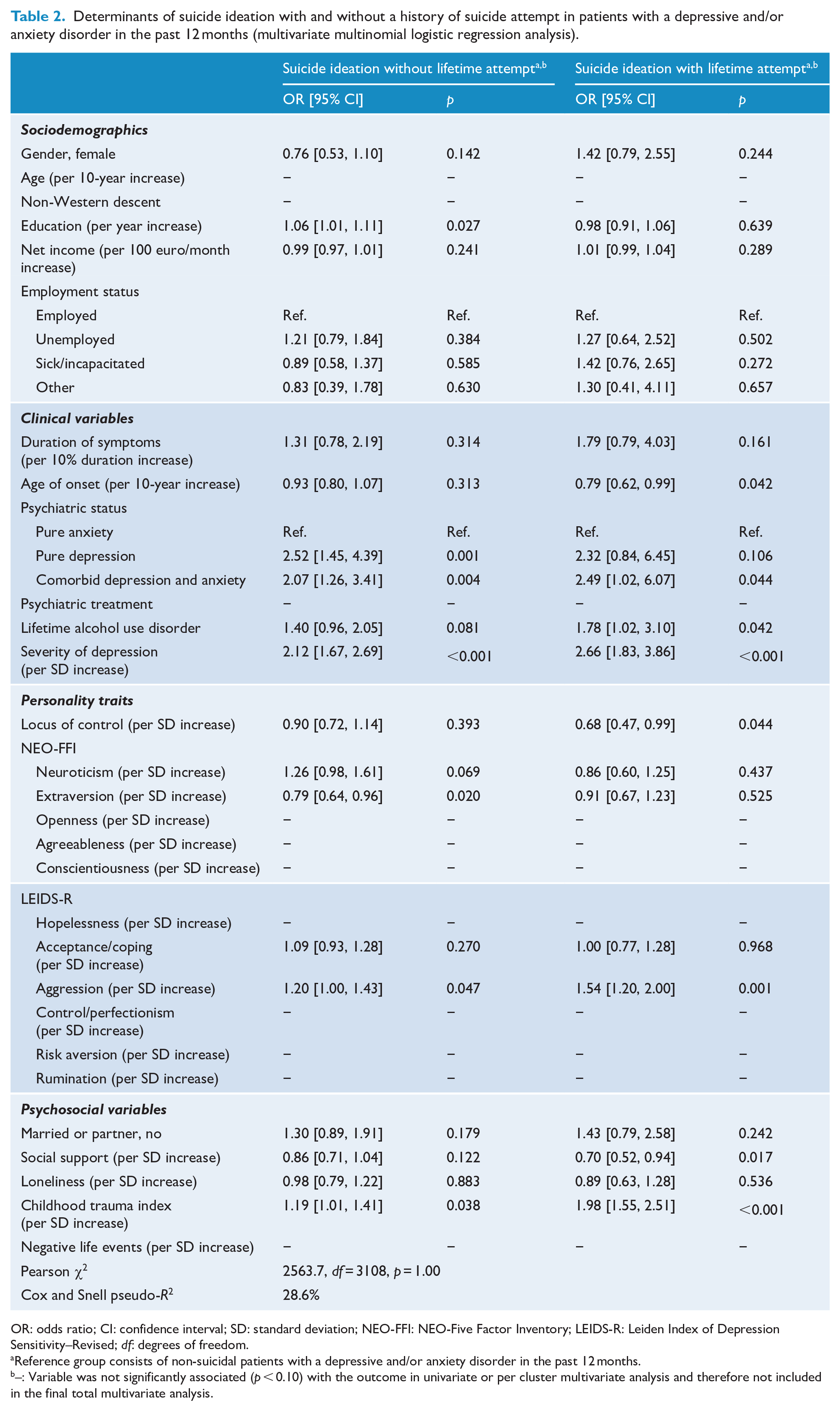
OR: odds ratio; CI: confidence interval; SD: standard deviation; NEO-FFI: NEO-Five Factor Inventory; LEIDS-R: Leiden Index of Depression Sensitivity–Revised; df: degrees of freedom.
Reference group consists of non-suicidal patients with a depressive and/or anxiety disorder in the past 12 months.
–: Variable was not significantly associated (p < 0.10) with the outcome in univariate or per cluster multivariate analysis and therefore not included in the final total multivariate analysis.
Table 3 reports associations within the suicide ideation group, comparing patients with and without a past attempt. The suicide attempt group was significantly more likely to be of non-Western descent, non-employed due to being sick or incapacitated, and to have less years of education, higher severity of depression, higher external locus of control and more childhood trauma in the univariate and per-domain analyses. The only variables significantly associated with suicide attempt within a group of patients with suicide ideation in the final multivariate analysis were being of non-Western descent, lower education and more childhood trauma.
Determinants of a history of suicide attempt in patients with suicide ideation and depressive and/or anxiety disorder in the past 12 months (univariate and multivariate logistic regression analyses).
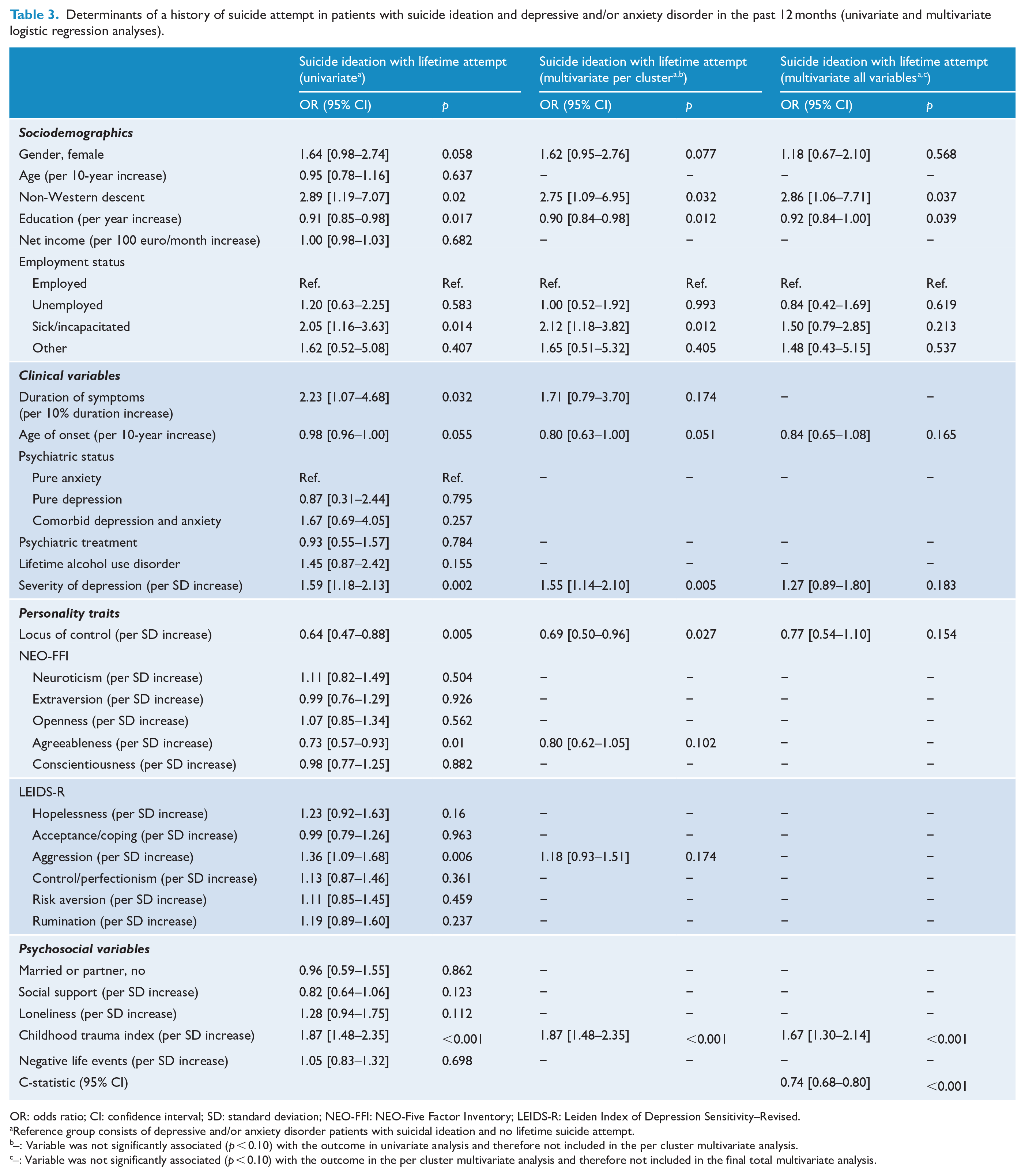
OR: odds ratio; CI: confidence interval; SD: standard deviation; NEO-FFI: NEO-Five Factor Inventory; LEIDS-R: Leiden Index of Depression Sensitivity–Revised.
Reference group consists of depressive and/or anxiety disorder patients with suicidal ideation and no lifetime suicide attempt.
–: Variable was not significantly associated (p < 0.10) with the outcome in univariate analysis and therefore not included in the per cluster multivariate analysis.
–: Variable was not significantly associated (p < 0.10) with the outcome in the per cluster multivariate analysis and therefore not included in the final total multivariate analysis.
Discussion
Few studies have investigated differences between suicide ideation and suicide attempt that fit within the ideation-to-action framework, especially using a wide range of variables, a large sample and comprehensive multivariate analyses. Therefore, the present study investigated whether often-cited sociodemographic, clinical, personality and psychosocial suicide risk factors could distinguish a suicide ideation and suicide attempt group from a non-suicidal group and suicide attempt from suicide ideation in depression and/or anxiety patients.
Suicide ideation and suicide attempt versus non-suicidal
A wide variety of variables, especially in the clinical, personality and psychosocial domains, could distinguish both suicide ideation and suicide attempt from a non-suicidal patient group. Sokero et al. (2003) similarly found that ideation and attempt could be distinguished from a non-suicidal group among patients with a depressive disorder by several clinical and psychosocial variables and had multiple overlapping risk factors. However, they found that severity of depression was associated with attempts and social support was associated with ideation, which is not entirely consistent with our findings. In the present study, severity of depression significantly increased the odds of both suicide ideation and attempt and lower levels of social support increased the odds for suicide attempt only. Sokero et al. (2003) did similarly show alcohol dependence to be uniquely associated with suicide attempt. We additionally found a comorbid depressive and anxiety disorder (vs an anxiety disorder alone) to increase the odds of suicide ideation and attempt and a younger age of onset to increase the likelihood of attempt only, results supported by previous studies (Claassen et al., 2007; Eikelenboom et al., 2012).
Furthermore, several personality and psychosocial factors could distinguish the suicide ideation and attempt group from non-suicidal patients. Unlike Spijker et al. (2010), we found a lower locus of control to be associated with a suicide attempt. However, our studies similarly identified neuroticism not to be associated with suicide ideation or attempt. Results also indicate that higher aggression increases the odds of both suicide ideation and attempts and that introversion is associated with suicide ideation, associations commonly found in other studies (Brezo et al., 2006). Finally, the finding that childhood trauma increases the odds of suicide ideation and attempt in the present study is in agreement with a literature review by Lee and Jung (2006), in which childhood trauma is referred to as a key suicide risk factor.
Altogether, findings suggest that clinical factors distinguish suicide ideation and suicide attempt most reliably from a non-suicidal group, meaning they could be interpreted as important risk factors for the development of suicidal thoughts and behavior in individuals with a depressive and/or anxiety disorder. Present findings point toward comorbid depression and anxiety and the severity of depression to be especially significant. However, these variables increase the odds of both suicide ideation and suicide attempt when compared with non-suicidal patients, making it difficult to identify specific high-risk patients. This again emphasizes the need for direct comparisons between suicide ideation and attempt.
Suicide ideation versus suicide attempt
Direct comparisons of suicidal patients with and without an attempt show none of the included clinical or personality indicators to be associated with suicide attempt, suggesting that these variables are mainly associated with suicide ideation. Nock et al. (2009) similarly found that the clinical variables depressive disorders and comorbidity were mainly predictive of suicidal ideation. May and Klonsky (2016) also showed that a depressive and alcohol use disorder and depression severity strongly distinguished the suicide ideation from the non-suicidal group, but could hardly distinguish attempt from ideation. Furthermore, Aaltonen et al. (2016) did not find the Big Five personality traits to distinguish attempt from ideation either. Unlike the present study, Fairweather et al. (2006) indicated that a lower locus of control could distinguish attempt from ideation, but only in males and Brezo et al. (2007) found elevated disruptive aggression to increase the odds of a suicide attempt in female ideators only.
We did find several sociodemographic and psychosocial indicators to be independently associated with suicide attempt within patients with suicide ideation. These were the presence of childhood trauma, non-Western descent and lower education. Our finding that suicide attempt is associated with lower education when compared to the suicide ideation group is in line with previous studies (May and Klonsky, 2016; Nock et al., 2008). Nock et al. (2008) found that low education was cross-nationally significantly associated with suicide attempt among those with suicide ideation. May and Klonsky’s (2016) meta-analysis found the attempt group to have a slightly lower education level than the ideation group. Although the association between education and suicide risk is not yet well understood (Phillips and Hempstead, 2017), a study by Bazrafshan et al. (2014) indicates that less educated may have a greater risk of performing a suicide attempt due to lacking effective coping skills.
Rarely has ethnicity been used as a variable to distinguish patients with suicide ideation and an attempt from those without an attempt due to small sample sizes (May and Klonsky, 2016). As a result, May and Klonsky’s (2016) meta-analysis could only compare Caucasians and African Americans. This division could not differentiate attempt from ideation. Our study, however, shows ethnicity to be important in distinguishing suicide attempt from suicide ideation, since being of non-Western descent significantly increased the likelihood of an attempt among patients with suicide ideation. This ties in with earlier findings indicating that risk of attempt is increased for various groups of Dutch women of non-Western descent (Burger et al., 2009; Van Bergen et al., 2010, 2018). As of yet, there is no clear-cut explanation for this. Many risk factors found in studies by Van Bergen et al. (2010, 2018), such as low socioeconomic status, low education levels, higher aggression, a history of sexual and physical abuse and low psychological well-being, were not unique to individuals of non-Western descent and varied per ethnic group. A literature review by Forte et al. (2018) shined light on other factors associated with elevated suicide ideation and attempt in groups of immigrants and ethnic minorities, such as problems with acculturation and religious well-being, lower levels of help-seeking behavior and a thwarted sense of belongingness. More culturally specific factors need to be investigated.
Childhood trauma had a stronger association with suicide attempt than with suicide ideation in the present study. Brezo et al. (2007) also found that childhood sexual abuse significantly differentiated suicide attempt from suicide ideation, but only in women. In May and Klonsky’s (2016) meta-analysis, childhood trauma was moderately elevated in the attempt group compared to the ideation group. They suggest that the step from ideation to attempt requires suicide capability, as is explained by ideation-to-action models such as the interpersonal-psychological theory (IPT) of suicidal behavior (Joiner et al., 2009). The theory states that the capability to harm oneself in a lethal manner can be acquired in various ways, one of which is through the experience of ‘painful and provocative life events’ (PPLs) such as childhood trauma (May and Klonsky, 2016). PPLs may cause a psychological shift by means of habituation to fearful and painful events that decreases fear and avoidance of pain, leading to the consideration that death could be a solution (May and Klonsky, 2016). Smith et al. (2010) also found evidence for this theory; PPLs were significantly more present in the suicide attempt group than in the suicide ideation or the control group.
Other psychosocial variables such as negative life events and social support did not distinguish suicide attempt from suicide ideation in the present study. Previous studies support these findings (Aaltonen et al., 2016; Fairweather et al., 2006).
Limitations
Despite strengths such as a large sample size and extensive multivariate analyses using a multitude of often-cited suicide risk factors, several limitations must be addressed. Retrospective questions about matters such as childhood trauma, age of onset and duration of symptoms may be liable to recall bias. Putative risk factors such as PTSD, borderline personality disorder and bipolar disorder were not accounted for, although these factors have previously been found to distinguish attempt from ideation (Aaltonen et al., 2016; May and Klonsky, 2016; Nock et al., 2009). We could not add suicide as an outcome. Further investigation is required to determine whether associations found in the present study could account for the transition from ideation to suicide. We did not differentiate between single and multiple attempters or low- and high-lethality attempters, which may be different types of individuals with different associated risk factors (Aaltonen et al., 2016; Oquendo et al., 2009). The cross-sectional design of this study does not allow for the identification of causal associations between predictors and the outcome variables. Finally, although five events per predictor variable should be permissible (Vittinghoff and McColloch, 2007), there remains a possibility of type II error in our study despite the fact that our sample size was quite adequate.
Future research
The present study offers preliminary evidence of what often-cited suicide risk factors may play a role in the progression from ideation to attempt. This contributes to the development of suicide theories involving the ideation-to-action framework. Longitudinal studies are required to determine whether factors found indeed predict a suicide attempt among patients with suicidal thoughts. Based on the association found in the current study between childhood trauma and suicide attempt, the suicide capability and its place in the ideation-to-action framework also requires more extensive investigation (May and Klonsky, 2016). Furthermore, specifying the types of ideation and attempt (e.g. active vs passive suicide ideation or actual vs interrupted vs aborted attempt), could provide an even more precise view of mechanisms involved in the suicide process.
Conclusion
Overall, our results indicate that many often-cited suicide risk factors lose their significance when trying to distinguish suicide attempt from suicide ideation. However, the present findings point out that clinicians should be particularly alert to childhood trauma, lower education and being of non-Western descent when faced with a depression and/or anxiety patient with suicide ideation. Doing so may help recognize high-risk patients who turn their thoughts into action.
Supplemental Material
Supplementary_Material_ANZJP – Supplemental material for Suicide ideation versus suicide attempt: Examining overlapping and differential determinants in a large cohort of patients with depression and/or anxiety
Supplemental material, Supplementary_Material_ANZJP for Suicide ideation versus suicide attempt: Examining overlapping and differential determinants in a large cohort of patients with depression and/or anxiety by Jasper XM Wiebenga, Merijn Eikelenboom, Henriette D Heering, Patricia van Oppen and Brenda WJH Penninx in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The infrastructure for the NESDA study (![]() ) is funded through the Geestkracht program of the Netherlands Organisation for Health Research and Development (ZonMw, grant number 10-000-1002) and financial contributions by participating universities and mental health care organizations (VU University Medical Center, GGZ inGeest, Leiden University Medical Center, Leiden University, GGZ Rivierduinen, University Medical Center Groningen, University of Groningen, Lentis, GGZ Friesland, GGZ Drenthe, Rob Giel Onderzoekscentrum).
) is funded through the Geestkracht program of the Netherlands Organisation for Health Research and Development (ZonMw, grant number 10-000-1002) and financial contributions by participating universities and mental health care organizations (VU University Medical Center, GGZ inGeest, Leiden University Medical Center, Leiden University, GGZ Rivierduinen, University Medical Center Groningen, University of Groningen, Lentis, GGZ Friesland, GGZ Drenthe, Rob Giel Onderzoekscentrum).
Declaration of Conflicting Interests
B.W.J.H.P. received (non-related) research funding from Boehringer Ingelheim and Jansen Research. The other authors declare that they have no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.