
Abstract
Australia was one of the first countries to put in place a national suicide prevention strategy [1], beginning its coordinated efforts in 1995 with the National Youth Suicide Prevention Strategy, broadening its emphasis to include the full age spectrum in 2000 with the Living Is For Everyone (LIFE) Framework, and renewing its approach in 2007 with a re-development of the LIFE Framework. These overarching policy frameworks have guided a population health approach to suicide prevention that acknowledges biological, psychological and social risk factors for suicide.
Originally, the prevention activities delivered through these policy frameworks focused on completed suicide only. More recently, however, there has been an acknowledgement that suicidality occurs on a gradient and suicidal ideation, suicide plans and attempted suicide are significant public health problems in their own right. Attempted suicide, for example, is acknowledged as one of the most salient predictors of subsequent completed suicide [2] and is associated with high health-care costs [3, 4].
It is more difficult to gauge the extent of suicidal ideation, suicide plans and suicide attempts in the Australian population than it is to glean a picture of completed suicide. Although there are some issues with the way completed suicide is ascertained and recorded [De Leo D et al.: unpublished data, 2008], routinely collected annual rate data are available at a national level. From these data it is known that suicide rates, particularly those for young men, have declined during the past 15 years [5], and some have cautiously attributed this decline to Australia's coordinated national approach to suicide prevention [6] (although there may be a number of alternative explanations [7, 8]). There is no equivalent knowledge about other manifestations of suicidality in Australia. Information on suicidal ideation and suicide plans clearly cannot be collected in any routine fashion. Data on hospitalizations and emergency department presentations for suicide attempts exist, but in Australia they are event based, not person based, and cannot readily be converted to population-based rates because there is no national, comprehensive unique identifier system that allows hospitalizations or emergency department presentations to be reliably linked to individuals [9].
The 2007 National Survey of Mental Health and Wellbeing (NSMHWB 2007) provides a unique opportunity to examine current person-based rates of suicidal ideation, suicide plans and attempted suicide among Australian adults. This paper takes advantage of that opportunity, and presents an overview of the lifetime and 12 month prevalence of suicidal ideation, suicide plans and suicide attempts for Australian adults as a whole and for particular sociodemographic and clinical subgroups in the population. It also explores health service use among individuals with suicidal thoughts and behaviours.
Method
Sampling and procedure
The NSMHWB was conducted between August and December 2007 by trained interviewers from the Australian Bureau of Statistics (ABS). The ABS identified a stratified multistage probability sample of households, and interviewers identified those aged 16–85 years in each through a set of household composition questions. Once the household composition was known, the interviewer selected the specific person to be interviewed, using a pre-determined algorithm developed by the ABS. If that person declined, no further attempt was made to recruit from that household. The algorithm oversampled younger people (16–24 years) and older people (65–85 years), in order to improve the reliability of estimates for these groups. This sampling process yielded 8841 fully responding households, or a response rate of 60%. This sample represented a projected Australian adult resident population aged 16–85 years of 16 015 300.
Interviews took place in respondents’ homes and took an average of 90 min. Due to the sensitive nature of the interview none was conducted with an interpreter or by proxy. Further detail about the sampling and procedure can be found in Slade et al. (in this issue) [10] and the ABS document [11].
Survey instrument
The survey instrument was based on the World Mental Health Survey Initiative version of the Composite International Diagnostic Interview (WMH-CIDI), and relied on the respondent being sufficiently proficient in English to complete it. It sought information on the respondents’ mental health status, permitting a judgement to be made about whether or not they had experienced an affective disorder, an anxiety disorder and/or a substance use disorder during their lifetime, during the past 12 months or during the past 30 days. The survey also sought information on respondents’ health service use, perceived needs for care, levels of functioning and disability, levels of psychological distress, quality of life, physical health status, social networks and provision of care to family for physical and mental health problems. Again, for further detail about the survey instrument see Slade et al. (in this issue) [10] and the ABS document [11].
Assessment of suicidality
The survey instrument included a section on suicidality that was designed to elicit information on respondents’ experiences of suicidal ideation, suicide plans and suicide attempts ‘ever’ or ‘within the past 12 months’. To counter potential biases associated with the underreporting of sensitive topics such as this, the interviewer asked each respondent to consider particular experiences described in a respondent booklet. Experience A was ‘seriously thought about committing suicide’ (suicidal ideation), experience B was ‘made a plan for committing suicide’ (suicide plan), and experience C was ‘attempted suicide’ (suicide attempt). The interviewer asked respondents whether experience A, B or C had happened to them in the timeframe of interest, rather than explicitly mentioning the experience aloud. A parallel set of questions with the experiences integrated into the question text was provided for respondents who were unable to read.
Respondents were sequenced out of the suicidality section and not asked questions about plans and attempts if they did not report having ever ‘seriously thought about committing suicide’. Those who responded affirmatively to any of the three experiences were asked how old they were the first time it had happened, whether it had happened to them within the past 12 months and, if not, how old they were the last time it happened. In the case of suicide attempts, respondents were also asked about the number of attempts, the intent of the first attempt, and about the intent, consequences and method of the last attempt.
Data from the questions on whether respondents had ‘ever’ or ‘within the past 12 months’ experienced suicidal ideation, suicide plans and attempted suicide were used to calculate lifetime and 12 month prevalence estimates, respectively. Survey responses from the questions relating to the onset and duration of suicidal behaviours, and questions relating to the intent, consequences and methods of suicide attempts were not analysed here but are the subject of forthcoming papers [Johnstone A et al.: unpublished data].
Data analysis
Unit record data were not available at the time of writing. Therefore all results were based on tables of aggregate data provided by the ABS. The tables contained population estimates and standard errors from, which 95% confidence intervals (95%CIs) were estimated. Estimates were weighted to account for differential probability of selection and to adjust for oversampling or undersampling of population subgroups. All data are presented as simple frequencies and percentages with 95%CIs. Differences with non-overlapping 95% confidence intervals were treated as statistically significant. This approach is conservative: when two 95%CIs do not overlap, the difference between the two estimates is statistically significant, but when they do overlap this may still reach the nominal 0.05 level of statistical significance.
Results
Suicidality in the general population
Lifetime and 12 month prevalence of suicidality vs sex
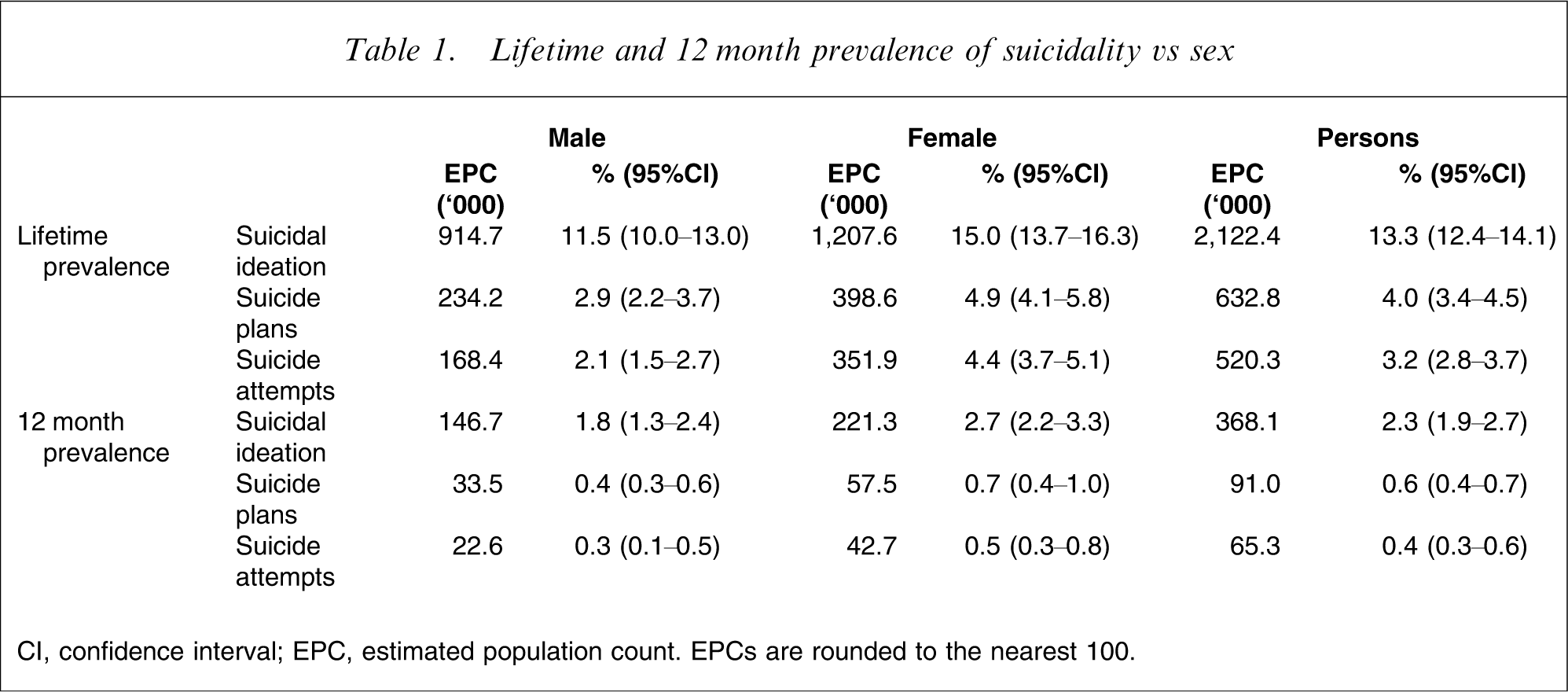
CI, confidence interval; EPC, estimated population count. EPCs are rounded to the nearest 100.
Table 1 also extrapolates these figures to the 2007 Australian population aged 16–85 years. The population-based figures underscore the magnitude of the problem, showing that during their lifetime, >2.1 million Australian adults seriously consider suicide, >600 000 make a plan and >500 000 make an attempt. During a 12 month period >350 000 consider suicide, nearly 100 000 make a plan and >65 000 make an attempt.
The remainder of this paper considers 12 month prevalence of suicidality only.
Suicidality across age/sex groupings
12 month prevalence of suicidality vs age and sex
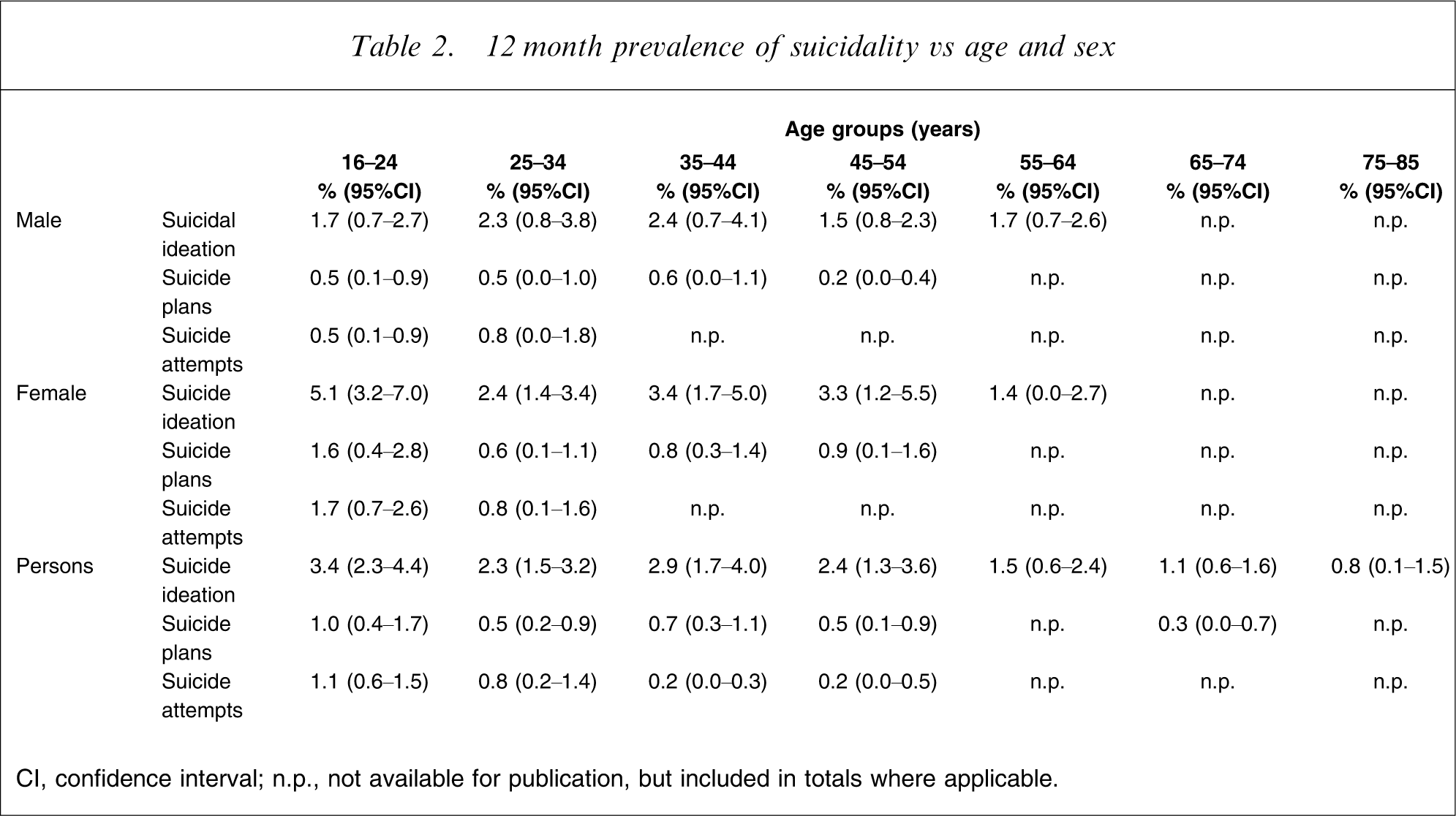
CI, confidence interval; n.p., not available for publication, but included in totals where applicable.
Suicidality among different sociodemographic groups
12 month prevalence of suicidality vs marital status, labour force status, education and country of birth
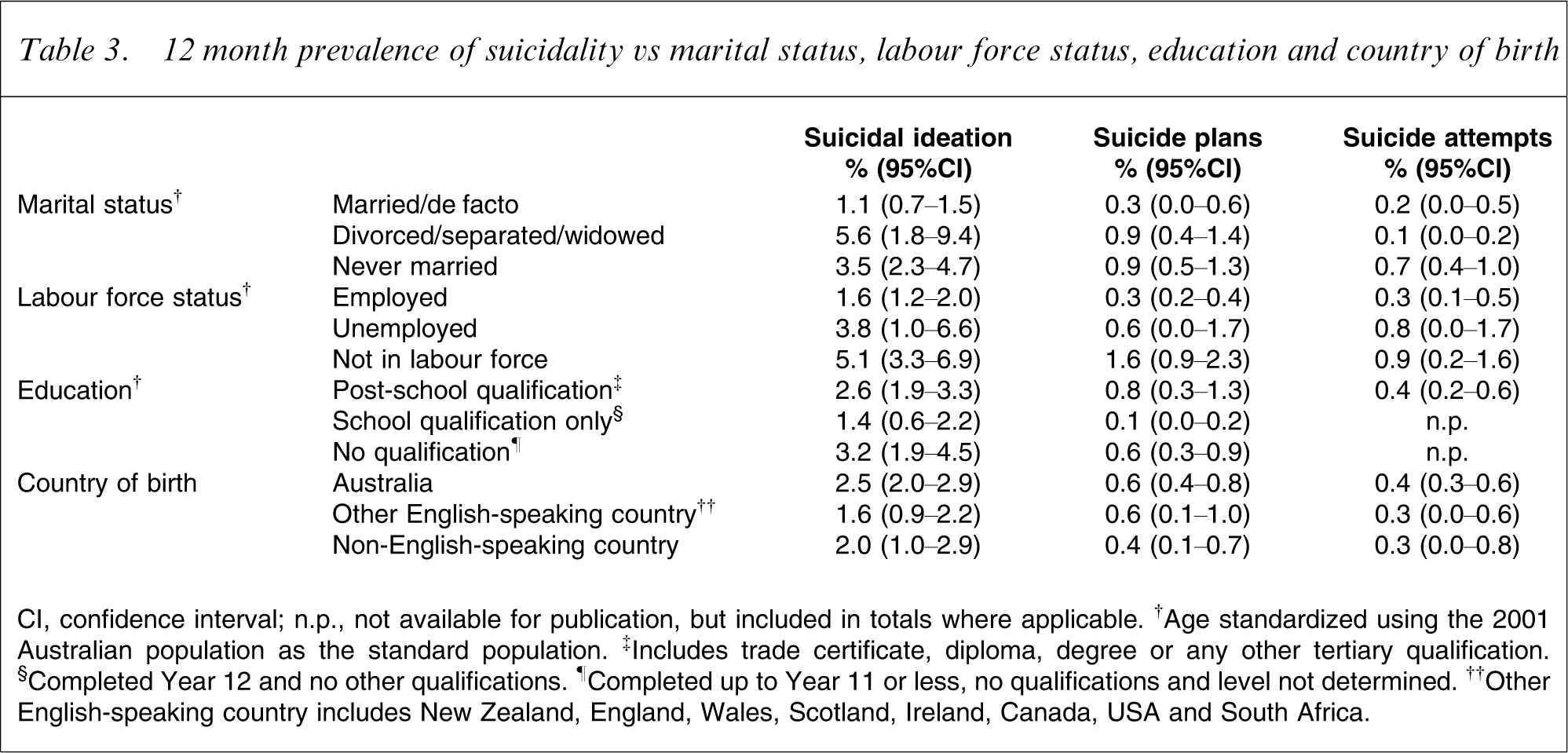
CI, confidence interval; n.p., not available for publication, but included in totals where applicable. †Age standardized using the 2001 Australian population as the standard population. ‡Includes trade certificate, diploma, degree or any other tertiary qualification. §Completed Year 12 and no other qualifications. ¶Completed up to Year 11 or less, no qualifications and level not determined. ††Other English-speaking country includes New Zealand, England, Wales, Scotland, Ireland, Canada, USA and South Africa.
The rate of suicidal ideation was 5.6% (95%CI = 1.8–9.4%) in people who were divorced, separated or widowed and 3.5% (95%CI = 2.3–4.7%) in people who had never married, compared with 1.1% (95%CI = 0.7–1.5%) in those who were married or in a de facto relationship. A similar pattern of lower prevalence among those who were married or in de facto relationships was observed for suicide plans and suicide attempts, but did not reach statistical significance.
Those who were not in the labour force were significantly more likely to experience suicidal ideation and make suicide plans than those who were employed. Rates of suicidal ideation and suicide plans among those who were not in the labour force were 5.1% (95%CI = 3.3–6.9%) and 1.6% (95%CI = 0.9–2.3%), respectively. The equivalent figures for those who were employed were 1.6% (95%CI = 1.2–2.0) and 0.3% (95%CI = 0.2–0.4%). Rates of both suicidal ideation and suicide plans for those who were unemployed were not statistically different to rates among those not in the labour force or those who were employed. The prevalence, however, tended to be higher than for the employed and lower than for those not in the labour force. Labour force status was not significantly associated with rates of suicide attempts.
People with post-school qualifications and people with no qualifications were more likely to have made a suicide plan (0.8%, 95%CI = 0.3–1.3% and 0.6%, 95%CI = 0.3–0.9%, respectively) than those with school qualifications (0.1%, 95%CI = 0.0–0.2%). A similar pattern was observed with respect to suicidal ideation, but these differences were not statistically significant. Data were not available to examine the relationship between education and suicide attempts.
There was a tendency for suicidal ideation to be more common among Australian-born people than among people born in other English-speaking countries or in non-English-speaking countries, but these differences were not statistically significant. The same was true for suicide plans and suicide attempts.
Suicidality among people with mental disorders
12 month prevalence of suicidality vs 12 month mental disorders and number of disorder classes
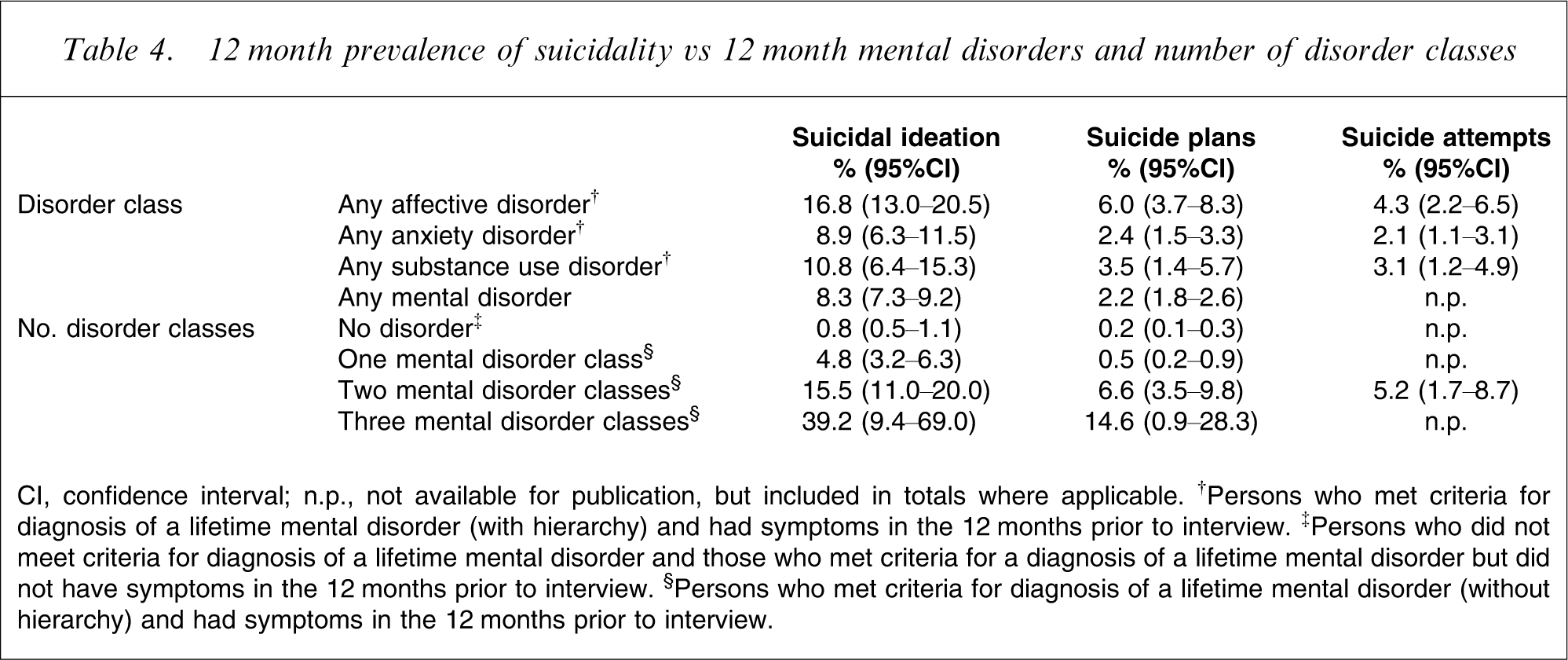
CI, confidence interval; n.p., not available for publication, but included in totals where applicable. †Persons who met criteria for diagnosis of a lifetime mental disorder (with hierarchy) and had symptoms in the 12 months prior to interview. ‡Persons who did not meet criteria for diagnosis of a lifetime mental disorder and those who met criteria for a diagnosis of a lifetime mental disorder but did not have symptoms in the 12 months prior to interview. §Persons who met criteria for diagnosis of a lifetime mental disorder (without hierarchy) and had symptoms in the 12 months prior to interview.
Table 4 also shows the 12 month prevalence of suicidality for people experiencing no disorder, a disorder or disorders from only one class (e.g. affective disorders only), from two classes (e.g. affective disorders plus anxiety disorders) and from three classes (e.g. affective disorders plus anxiety disorders plus substance use disorders). There was a clear dose–response relationship between comorbidity of mental disorders and suicidal ideation, with each additional disorder class substantially increasing the rates, at least up to two disorder classes (the relatively smaller numbers of those with disorders from three classes introduced greater uncertainty around this estimate). The impact of having disorders from two classes was also significant for suicide plans. Equivalent data were unavailable for suicide attempts.
Service use among people with suicidal thoughts and behaviours
12 month use of mental health services by those with 12 month experiences of suicidality
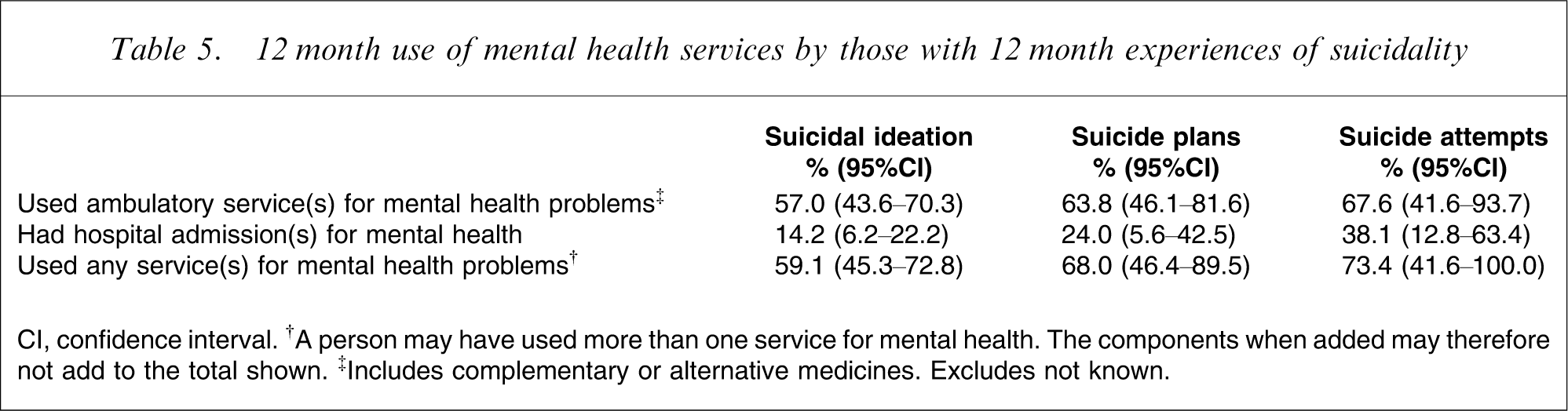
CI, confidence interval. †A person may have used more than one service for mental health. The components when added may therefore not add to the total shown. ‡Includes complementary or alternative medicines. Excludes not known.
Discussion
Summary of findings
To summarize, 13.3% of respondents had serious thoughts about suicide at some stage in their lives, 4.0% had made a suicide plan and 3.2% had made a suicide attempt. The equivalent 12 month prevalence rates were 2.3%, 0.6% and 0.4%, for ideation, plans and attempts, respectively. In general, suicidal thoughts and behaviours during the previous 12 months tended to be relatively more common in women, younger people, those outside the labour force, and those with mental disorders; they tended to be less common in those who were married or in de facto relationships, and those with moderate levels of education. A number of the differences in prevalence rates between sociodemographic and clinical subgroups may not have reached statistical significance due to data availability constraints and the conservative tests of significance that were used by necessity. These patterns warrant further exploration. Service use for mental health problems was higher among people with suicidal thoughts and behaviours than it was among the general population, but significant numbers of those experiencing suicidal thoughts and behaviours did not receive treatment.
Comparisons with recent international surveys
As noted, the survey instrument used in the 2007 NSMHWB was based on the WMH-CIDI, which has been used in recent years in a number of countries. Use of a common instrument facilitates international comparisons regarding the prevalence of suicidal ideation, suicide plans and suicide attempts, and instils greater confidence that any cross-country differences are genuine rather than artefactual (although the impact of subtle design differences and differences in response rates remain important considerations). With this in mind, some relevant comparisons are made in this section. Data are also available from other countries on the extent to which people with suicidality make use of health services for mental health problems, but interpreting comparisons of this kind relies on understanding the service system context in each country, so no such comparisons are made here.
Nock et al. pooled data from surveys conducted in 17 developed and developing countries using the WMH-CIDI (Nigeria, South Africa, Colombia, Mexico, USA; Japan, New Zealand, China; Belgium, France, Germany, Italy, The Netherlands, Spain, Ukraine, Israel and Lebanon) [12]. This yielded lifetime prevalence estimates that were lower than Australia's for suicidal ideation (9.2%), suicide plans (3.1%) and suicide attempts (2.7%). Australia's lifetime and 12 month prevalence rates were, however, generally lower than those reported for its two most similar counterparts, namely New Zealand (lifetime suicidal ideation = 15.7%, lifetime suicide plans = 5.5%, lifetime suicide attempts = 4.5%, 12 month suicidal ideation = 3.2%, 12 month suicide plans = 1.0%, 12 month suicide attempts = 0.4%) [16] and the USA (lifetime suicidal ideation = 15.5%, lifetime suicide plans = 5.4%, lifetime suicide attempts = 5.0%, 12 month suicidal ideation = 3.3%, 12 month suicide plans = 1.0%, 12 month suicide attempts = 0.6%) [13, 14].
The sociodemographic and clinical variables that were found to be associated with suicidal ideation, suicide attempts and suicide plans in the past 12 months were relatively consistent with those identified in other surveys. The New Zealand and US surveys found that being young was predictive of all three forms of suicidality, and although there was a tendency for there to be greater evidence of suicidality in women than in men, this difference was typically not significant [13, 14]. These surveys also identified factors such as marital status, employment status and level of education as being important to varying degrees [13, 14]. Most importantly, the factor identified in these surveys as being most strongly associated with 12 month suicidal ideation, suicide plans and suicide attempts was presence of a mental disorder, particularly an affective disorder [13, 14].
Comparison with the 1997 Australian NSMHWB
The earlier NSMHWB, conducted in Australia in 1997, also made an assessment of suicidality. Some caution must be exercised in comparing the findings from the current survey with those from the 1997 survey because of differences in the two instruments, which have been documented elsewhere in this issue [10]. With this caveat in mind, it is possible to consider the relative rates of suicidality for the total population and particular subgroups in 1997 and 2007, and to compare the rates of health service use by people with suicidal thoughts and behaviours in the two time periods. A thorough examination of these issues is not possible here but is the subject of a forthcoming paper [Johnston A et al.: unpublished data].
Pirkis et al. considered the lifetime and 12 month rates of and risk factors for suicidal ideation and suicide attempts (but not suicide plans) [15]. They reported that the lifetime rates of suicidal ideation and suicide attempts were 14.3% and 3.1%, respectively, and the 12 month rates were 2.9% and 0.3%. It would appear that the prevalence of suicidal thoughts and suicide attempts in the Australian adult population have changed little.
Pirkis et al. also identified a similar constellation of factors as being associated with suicidality in 1997 [15]. Twelve month ideation and attempts were both associated with mental disorders (particularly affective disorders). Ideation was also associated with age, marital status, and disability; attempts were associated with marital status and employment status.
In a separate analysis, Pirkis et al. considered the extent to which individuals who had experienced suicidal thoughts or behaviours within the past 12 months had made use of services for mental health problems during the same period [16]. The analysis showed that although thinking about suicide and attempting it were predictive of service use, significant proportions of ideators and attempters either did not seek or did not receive services.
Study limitations
The 2007 NSMHWB had a number of limitations that should be taken into account in interpreting the findings presented.
The response rate of 60% was lower than expected, and certain selection biases may have occurred if people with suicidal thoughts and behaviours were more or less likely to participate. The survey relied on self-report and individuals may have either selectively remembered particular experiences or been unlikely to report them because of the associated stigma. The logical skips in the survey design meant that only those who had ‘seriously thought about committing suicide’ were asked whether they had made plans and attempts. This may have led to the misclassification of some respondents, such as those who made particularly impulsive suicide attempts. The data available for the current analyses came in the form of extract tables, rather than unit record data. This limited the questions that could be asked of the data, and had implications for the reliability of the findings. Cells with low numbers were suppressed. This had particular implications for an examination of the prevalence of suicidal thoughts and behaviours, which, despite being significant public health issues, are relatively rare events. This was further compounded by a reliance on non-overlapping CIs to identify significant differences between groups. As noted earlier, this method is conservative and may have yielded false negatives. Together, these limitations mean that some significant differences in the rates of suicidal thoughts and behaviours between particular subgroups may have been missed. Where significant differences in the prevalence of suicidality were observed between particular sociodemographic and clinical subgroups, some caution must be exercised in interpreting the results. Although these findings provide hints about factors that may be associated with suicidal thoughts and behaviours, they do not permit any definitive statements to be made about causality.
Potential implications for policy and practice
Notwithstanding the aforementioned limitations, the findings from the current analyses have some potential implications for policy and practice. Perhaps the most salient policy-relevant finding reported here is the fact that the percentage of the population who attempted suicide was found to be similar in 2007 and 1997. It is interesting to consider how this finding fits with an observed reduction in completed suicides over the same period, which has been tentatively attributed to Australia's coordinated national approach to suicide prevention. It may be that even though the proportion of the population who attempt suicide has not reduced, those who do are making fewer or less severe attempts, and/or using less lethal means. Nonetheless, the finding suggests that the renewed LIFE Framework should ensure that adequate consideration is given to suicide attempts.
The framework should target both those at particularly elevated risk (notably those with mental disorders) and those in the general community, and should draw on the full spectrum of interventions. Some of these interventions need to be clinically oriented, and should involve ensuring that clinicians are supported to appropriately detect, diagnose, assess, and manage mental disorders in general and suicide risk in particular, through relevant training and the development of evidence-based guidelines. Other interventions need to be population based and should draw on sectors outside health to reduce known risk factors, for example, reduce unemployment. Still others will need to straddle the interface between clinical and population based approaches, in order to encourage those in the community who might not otherwise seek treatment to do so.
Conclusions
Suicidal thoughts and behaviours are not uncommon among the Australian adult population. These thoughts and behaviours are not only predictive of subsequent fatal suicidal acts, but are also significant public health problems in their own right. They are associated with high levels of burden at an individual and societal level. Further analysis is required to assess the impact of the national policy frameworks on the spectrum of suicidal thoughts and behaviours.
Footnotes
Acknowledgements
The 2007 NSMHWB was funded by the Australian Government Department of Health and Ageing, and conducted by the Australian Bureau of Statistics. The authors would like to thank the NSMHWB Reference Group for their input into the survey's design. The authors would also like to thank those who participated in the survey.