
Abstract
Objectives:
We compare the prevalence of suicidal thoughts and attempts between Indigenous and non-Indigenous males in urban and regional Australia, and examine the extent to which any disparity between Indigenous and non-Indigenous males varies across age groups.
Methods:
We used data from the baseline wave of The Australian Longitudinal Study on Male Health (Ten to Men), a large-scale cohort study of Australian males aged 10–55 years residing in urban and regional areas. Indigenous identification was determined through participants self-reporting as Aboriginal, Torres Strait Islander or both. The survey collected data on suicidal thoughts in the preceding 2 weeks and lifetime suicide attempts.
Results:
A total of 432 participants (2.7%) identified as Indigenous and 15,425 as non-Indigenous (97.3%). Indigenous males were twice as likely as non-Indigenous males to report recent suicidal thoughts (17.6% vs 9.4%; odds ratio = 2.1, p < 0.001) and more than three times as likely to report a suicide attempt in their lifetime (17.0% vs 5.1%; odds ratio = 3.6; p < 0.001). The prevalence of recent suicidal thoughts did not differ between Indigenous and non-Indigenous males in younger age groups, but a significant gap emerged among men aged 30–39 years and was largest among men aged 40–55 years. Similarly, the prevalence of lifetime suicide attempts did not differ between Indigenous and non-Indigenous males in the 14- to 17-years age group, but a disparity emerged in the 18- to 24-years age group and was even larger among males aged 25 years and older.
Conclusion:
Our paper presents unique data on suicidal thoughts and attempts among a broad age range of Indigenous and non-Indigenous males. The disparity in the prevalence of suicidal thoughts increased across age groups, which is in contrast to the large disparity between the Indigenous and non-Indigenous suicide rates in younger age groups.
Background
High rates of Indigenous suicide is a distressing phenomenon that plagues several postcolonial countries, including Australia, Canada, the United States and New Zealand (Leenaars et al., 2007; McLoughlin et al., 2015). Suicide among Indigenous peoples is a complex socio-cultural, political, biological and psychological phenomenon that needs to be understood in the context of colonisation, loss of land and culture, trans-generational trauma, grief and loss and racism and discrimination (Coupe, 2000; Elias et al., 2012; Hunter and Harvey, 2002). The higher levels of marginalisation and social disadvantage experienced by Indigenous peoples increases their exposure to mental disorders, substance abuse and a suite of chronically stressful life events, e.g., unemployment, homelessness, incarceration and family breakdown, all of which are well-documented suicide risk factors (Barlow et al., 2012; Cwik et al., 2015; Elliott-Farrelly, 2004; Gracey and King, 2009; Hawton and Van Heeringen, 2009; King et al., 2009).
In Australia, suicide is a leading cause of mortality for Indigenous people, and this is particularly the case for Indigenous males among whom suicide is the second leading cause of death (Australian Bureau of Statistics, 2016a). Indigenous suicide prevention has become a major theme of the Close the Gap Campaign, given that premature mortality from suicide is a major contributor to the life expectancy gap between Indigenous and non-Indigenous Australians (Holland, 2015). The suicide rate for Indigenous males was estimated to be 34.1 per 100,000 in 2014, twice the rate (17.7 per 100,000) for non-Indigenous males (Australian Bureau of Statistics, 2016a). Figure 1 provides a useful visual overview of the disparity between the Indigenous and non-Indigenous suicide rates across age groups, and was the primary motivator behind the concept of this paper. The Indigenous suicide rate is highest among younger males aged 25–29 years at 90.8 per 100,000, compared to 22.1 per 100,000 among their non-Indigenous peers (Australian Bureau of Statistics, 2016c) – a fourfold difference. These figures underscore a striking disparity in suicide rates between Indigenous and non-Indigenous males in younger cohorts; among males aged 15–34 years, the Indigenous suicide rate is approximately four times the non-Indigenous rate, and it remains two-and-a-half to three-and-a-half times the non-Indigenous rate among those aged 35–44 years. Meanwhile, among males aged 45 years and older, there appears to be no or minimal disparity in suicide rates by Indigenous identification.
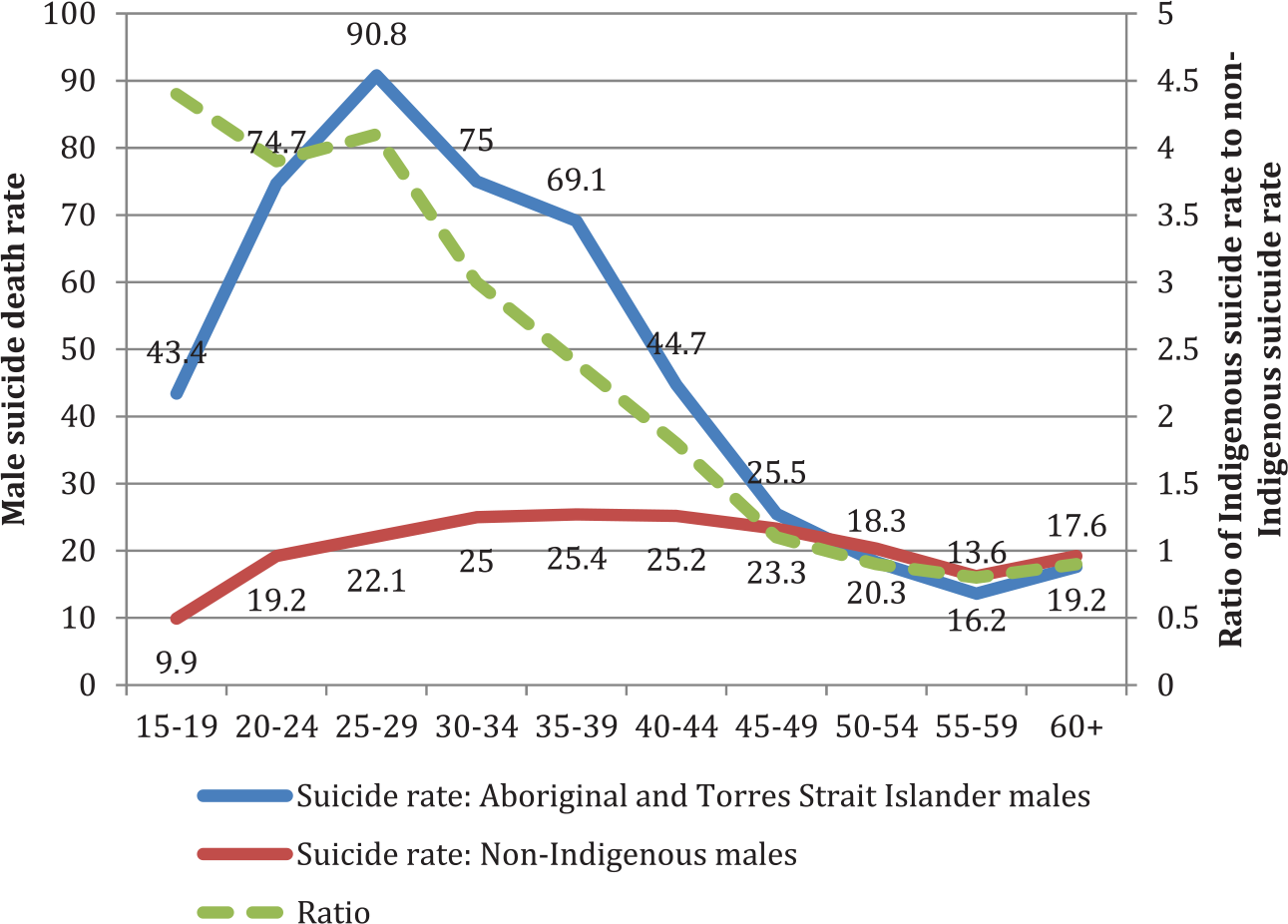
Comparison of age-specific suicide rates of males from five Australian states, by Indigenous identification.
While there is evidence about the disparity in suicide rates between Indigenous and non-Indigenous males, there is a dearth of data related to suicidal thoughts and attempts among Indigenous men across a broader range of age groups. Regional cross-sectional studies have predominantly been undertaken among youth and have observed a high prevalence of suicidal thoughts and attempts. These studies have used a wide variety of measures and have targeted different population groups making comparisons difficult. For example, a study of male and female Indigenous youth aged 12–26 years who were affiliated with the Victorian Aboriginal Health Service reported a prevalence of 23.3% for suicidal thoughts in the preceding 2 weeks, and 24.4% had attempted suicide in their lifetime, with no statistically significant difference across genders (Luke et al., 2013). The Western Australian Aboriginal Child Health Survey of 12- to 17-year-olds from Perth and rural Western Australia reported a prevalence of 15.6% (males 11.9%, females 19.5%) for suicidal thoughts and 6.5% (males 4.1%, females 9.0%) for suicide attempts in the 12 months prior to the survey (Zubrick et al., 2005). Additionally, there have been surveys of suicidal thoughts and/or attempts among predominantly male Indigenous offenders in a variety of locations (Butler et al., 2007; Larney et al., 2012; Sawyer et al., 2010; Stathis et al., 2012), although it is difficult to generalise the findings from these studies beyond custody/detention settings.
Notwithstanding these studies, much remains unknown about the prevalence of suicidal thoughts and attempts across a broader age range of Indigenous men in general community settings throughout Australia. This paper contributes to addressing this gap by analysing data collected for the Ten to Men study of the health of boys and men aged 10–55 years from urban and regional Australia, with analyses of differences in suicidal thoughts and attempts between sub-samples of Indigenous and non-Indigenous males. The objectives of our analyses were (1) to compare the prevalence of suicidal thoughts and attempts between Indigenous and non-Indigenous males in the Ten to Men sample and (2) to examine the extent to which any disparity between Indigenous and non-Indigenous males varies across age groups.
Methodology
Data source
We used data from The Australian Longitudinal Study on Male Health (Ten to Men), a large-scale cohort study of Australian males aged 10–55 years. Ten to Men is a longitudinal study and our paper presents analyses of cross-sectional data collected in 2013–2014 for the baseline wave. Full details of the study design and methods are available elsewhere (Currier et al., 2016; Pirkis et al., 2016). In brief, multi-stage stratified cluster sampling was used to recruit Australian boys and men from households in Australian Statistical Geographical Standard (ASGS) major city, inner regional and outer regional areas of Australia. Due to resource limitations and operational considerations, remote and very remote areas were excluded. Because it was not possible to include males from remote areas, it was decided to over-sample males from regional areas. A total of 104,484 households were approached in 2013 and 2014, from which 15,988 Australian males were recruited, resulting in a response fraction of 35% among confirmed in-scope males.
Eligible participants were males aged 10–55 years at the time of recruitment, who were Australian citizens or permanent residents and had a sufficient understanding of English to provide informed consent and to complete the questionnaire. The questionnaire for young men aged 15–17 years and the questionnaire for adults aged 18–55 years were self-administered, while the questionnaire for boys aged 10–14 years was completed using a computer-assisted personal interview. The questionnaires captured information about suicidal thoughts and attempts, as well as other information about physical and mental health, health-related behaviours, social and environmental determinants of health, health literacy and health service use. Copies of the questionnaires are available at the study website www.tentomen.org.au.
The baseline wave of Ten to Men received ethical clearance from the University of Melbourne Human Sciences Human Ethics Sub-Committee (HREC 1237897 and 1237376). Participants aged 18–55 years provided written consent; participants aged 10–17 years provided written assent and a parent/guardian provided written, parental consent.
Measures
The prevalence of recent suicidal thoughts was assessed using Item 9 of the Patient Health Questionnaire-9 (PHQ-9) Brief Depression Severity Measure for adults and the PHQ-9 Modified for Teens (Kroenke et al., 2001; Richardson et al., 2010). Item 9 asks participants how often they had been bothered by ‘thoughts you would be better off dead or of hurting yourself in some way’ in the preceding 2 weeks. Participants who responded ‘several days’, ‘more than half the days’ and ‘nearly every day’ were collapsed into one category in a dichotomous variable and compared against those who responded ‘not at all’. This variable has been observed to be associated with a 75%–185% increase in the risk of suicide in a study of veterans in the United States (Louzon et al., 2016). The lifetime prevalence of suicide attempt(s) was assessed by asking participants aged 14 or older whether they had ever tried to kill themselves; participants aged 10–13 years were not asked this question. Both measures of suicidality have previously been used in a survey of Indigenous youth in Australia (Luke et al., 2013).
Indigenous identification was determined through participants self-reporting as Aboriginal, Torres Strait Islander or both. Participants were excluded from our analyses if they refused or did not answer the question (n = 117), if they answered that they ‘don’t know’ (n = 13) or if they gave an invalid multiple response (n = 1).
Statistical analyses
All analyses were conducted in Stata version 13.0 using survey commands to account for the complex sampling design (Spittal et al., 2016). Sampling weights were also used to account for unequal probability of selection, and these were calculated based on the inverse of the probability of selection at the level of the individual participant (Spittal et al., 2016). Both unweighted and weighted percentages were generated to describe the Indigenous and non-Indigenous sub-samples across age, state and remoteness categories, with chi-square tests used to examine differences between the two sub-samples. Adjusted estimates of the prevalence of suicidal thoughts and attempts within the Indigenous and non-Indigenous sub-samples were generated with 95% confidence intervals, both across all age groups and within age groups. Logistic regression analyses were used to generate the odds of Indigenous males experiencing suicidal thoughts and attempts compared to non-Indigenous males. These analyses were conducted both across all age groups and within age groups; analyses across all age groups adjusted for age and remoteness, while analyses within age groups adjusted for remoteness.
Results
Sample characteristics
The sample size for our analyses was 15,857 men, among whom 432 (2.7%) identified as Aboriginal (n = 379), Torres Strait Islander (n = 27) or both (n = 26); and 15,425 (97.3%) identified as non-Indigenous. The characteristics of the Indigenous and non-Indigenous sub-samples differed significantly across age, state and remoteness categories (see Table 1). Compared to non-Indigenous participants, the Indigenous sub-sample had a higher proportion of younger males, with approximately one-quarter (24.0%) between the ages of 10 and 17 years (cf. 12.9% among non-Indigenous males). There was a lower proportion of Indigenous males than non-Indigenous males from major cities (35.0% vs 58.4%) and a higher proportion from outer regional areas (35.2% vs 19.2%). There was also some variation by state, with higher proportions of Indigenous males than non-Indigenous males from New South Wales (38.2% vs 27.7%) and Queensland (34.5% vs 20.8%), and a considerably lower proportion from Victoria (9.0% vs 31.2%). The majority of participants in both the Indigenous (88.2%) and non-Indigenous (82.4%) sub-samples resided in eastern Australia (Queensland, New South Wales, Victoria, Australian Capital Territory or Tasmania).
Sample characteristics, by Indigenous identification.
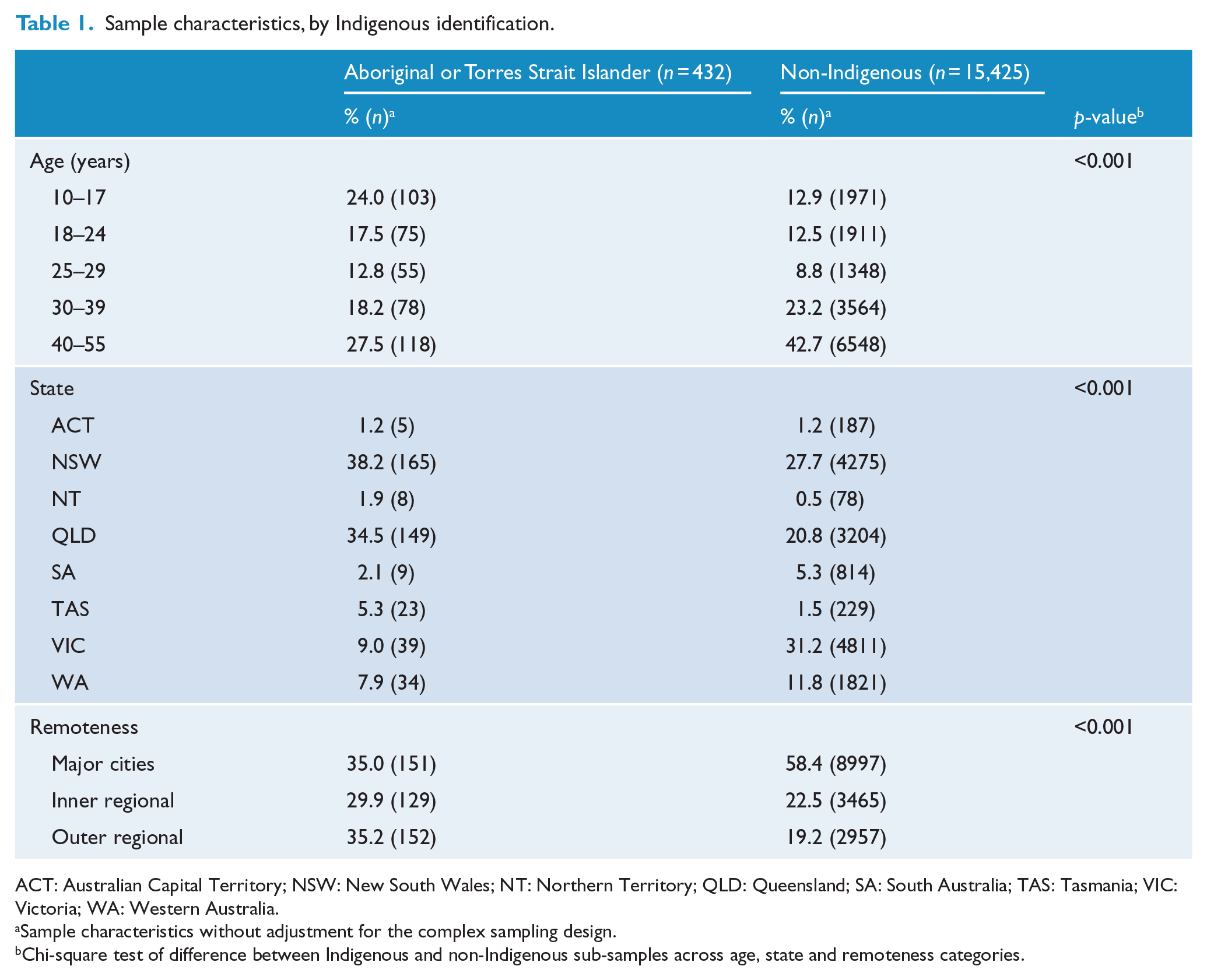
ACT: Australian Capital Territory; NSW: New South Wales; NT: Northern Territory; QLD: Queensland; SA: South Australia; TAS: Tasmania; VIC: Victoria; WA: Western Australia.
Sample characteristics without adjustment for the complex sampling design.
Chi-square test of difference between Indigenous and non-Indigenous sub-samples across age, state and remoteness categories.
Disparity in the prevalence of recent suicidal thoughts and lifetime attempts
Table 2 shows the disparity in the prevalence of suicidal thoughts and attempts between Indigenous and non-Indigenous males. Indigenous males were twice as likely to report recent suicidal thoughts (17.6% vs 9.4%; odds ratio [OR] = 2.1, p < 0.001) and more than three times as likely to report a suicide attempt in their lifetime (17.0% vs 5.1%; OR = 3.6; p < 0.001), adjusting for age and remoteness.
Two-week prevalence of suicidal thoughts and lifetime prevalence of suicide attempt(s) by Indigenous identification, both across age groups and within age groups.
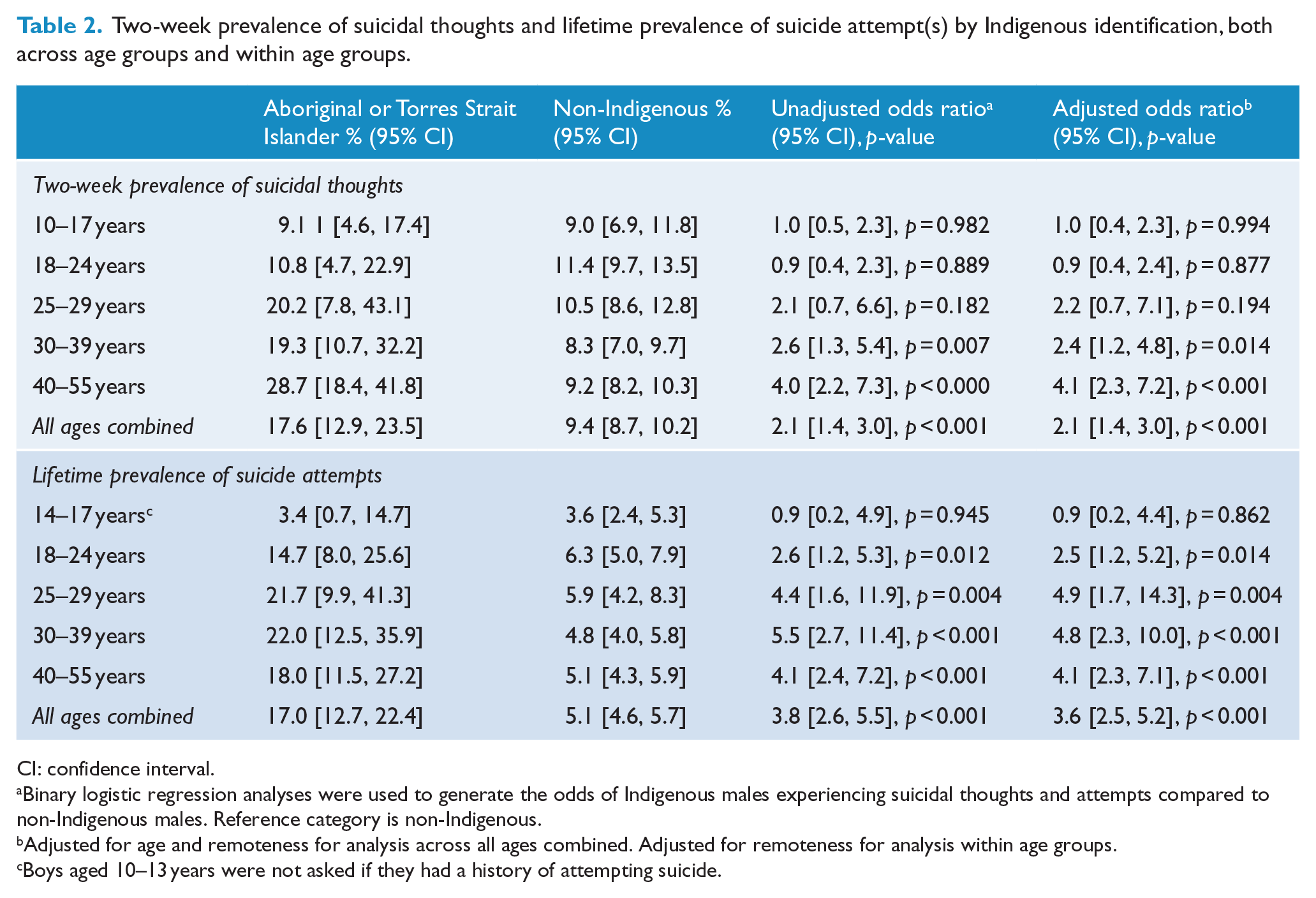
CI: confidence interval.
Binary logistic regression analyses were used to generate the odds of Indigenous males experiencing suicidal thoughts and attempts compared to non-Indigenous males. Reference category is non-Indigenous.
Adjusted for age and remoteness for analysis across all ages combined. Adjusted for remoteness for analysis within age groups.
Boys aged 10–13 years were not asked if they had a history of attempting suicide.
The pattern of disparity across age groups
Table 2 also shows the pattern of disparity across age groups. The disparity between Indigenous and non-Indigenous males in recent suicidal thoughts trended upwards across age groups. The prevalence of recent suicidal thoughts did not differ between Indigenous and non-Indigenous males in the 10–17 years or 18–24 -years age groups. Although the difference wasn’t significant, the beginning of a disparity between Indigenous and non-Indigenous males emerged in the 25- to 29-years age group (20.2 vs 10.5%; OR = 2.1, p = 0.182); this age group had the smallest number of Indigenous males (n = 55), which may have reduced the power to detect differences between these sub-samples. There was strong evidence of a difference among those aged 30–39 years (19.3% vs 8.3%; OR = 2.6, p = 0.007), and among those aged 40–55 years (28.7% vs 9.2%; OR = 4.0, p < 0.001).
The lifetime prevalence of suicide attempts did not differ between Indigenous and non-Indigenous males in the 14–17 years age group (3.4% vs 3.6%; OR = 0.9, p = 0.862). However, there was evidence of a disparity in the 18–24 years age group (14.7% vs 6.3%; OR = 2.5, p = 0.014). In the age groups 25–29 years, 30–39 years and 45–50 years, approximately one in five Indigenous males had ever attempted suicide, and they had odds that were 4.4, 5.5 and 4.1 times higher for ever attempted suicide respectively compared to their non-Indigenous counterparts within the same age groups.
Discussion
We found that, in urban and regional Australia, the prevalence of recent suicidal thoughts and having ever attempted suicide was substantially higher among Indigenous males compared to non-Indigenous males. This is extremely concerning, yet the findings from our analyses of the Ten to Men sample are consistent with what is already known about the gap in suicide rates between Indigenous and non-Indigenous males, with suicide rates being twice as high among Indigenous males (Australian Bureau of Statistics, 2016a; De Leo et al., 2011; Snowdon, 2016).
While there was no disparity in the lifetime prevalence of a suicide attempt between Indigenous and non-Indigenous males aged 14–17 years (3.4% vs 3.6%), there was a disconcertingly higher proportion of young Indigenous males aged 18–24 years who had attempted suicide (14.6%) compared to non-Indigenous males (6.3%). This disparity was even larger among males aged 25–29 years. This indicates an immediate rise in the risk of suicide for young Indigenous males as they enter adulthood, which is consistent with the peak in Indigenous suicide rates among males in this age group (see Figure 1). Of further concern, those Indigenous males who have attempted suicide at this young age will be carrying a lifelong suicide risk factor into their adult years, given that a history of attempting suicide has consistently been identified as a predictor of future suicide attempts and deaths (Cavanagh et al., 2003; Hawton and Van Heeringen, 2009; Ribeiro et al., 2016).
There was a noteworthy age pattern in the disparity between Indigenous and non-Indigenous males with respect to the prevalence of recent suicidal thoughts. There was no disparity in younger age groups of males aged 10–24 years, and a non-significant gap among males aged 25–29 years. However, among those aged 30–39 years, there was a marked and statistically significant disparity that was even larger in the 40–55 years age group. A key feature of this disparity was that the prevalence of recent suicidal thoughts increased across age groups among Indigenous males, while it remained relatively flat across age groups among non-Indigenous males. Interestingly, this is consistent with a review of findings from community mental health surveys (Jorm et al., 2012). Across seven studies, Indigenous adults were consistently found to have a higher prevalence of self-reported psychological distress than non-Indigenous adults, while two surveys of adolescents found no similar disparity.
This trend is curiously different from the age pattern for the ratio of the Indigenous suicide rate compared to the non-Indigenous suicide rate, where there is a high level of disparity observed in the younger age groups which then trends towards parity among middle-aged males (see Figure 1). One might have expected to find that the disparity in suicidal thoughts across age groups in our sample would follow this pattern, but it trends in the opposite direction and moves from parity at younger ages to disparity at older ages.
There are a number of aetiological and methodological reasons why these two suicide indicators may not match neatly. First, suicide deaths and suicidal thoughts are related yet still quite different phenomena. While suicidal thoughts may be a necessary antecedent to a suicide death, not all people who have suicidal thoughts will attempt or die by suicide (Ribeiro et al., 2016). Second, the data presented in Figure 1 refer to suicide deaths between 2001 and 2010, which is a considerably different time period to the 2013–2014 sample being studied in this paper. Third, our sample was collected in urban and regional areas, whereas the suicide death data also represent deaths in remote areas. This is relevant given that approximately one in five Indigenous people reside in remote areas and the Indigenous suicide death rate in some remote areas is very high and has a prominent youth profile; e.g., 68% of suicide deaths in the high-suicide Kimberley region between 2005–2014 were under the age of 30 (McHugh et al., 2016). Further to this point, the data in Figure 1 refer to suicide deaths in only five states and territories where Indigenous identification in mortality data was considered to be acceptable: New South Wales, Queensland, South Australia, Northern Territory and Western Australia. However, our sample is under-represented in terms of Indigenous males from the Northern Territory, Western Australia and South Australia (Australian Bureau of Statistics, 2016b), and these states have the highest Indigenous suicide rates (Australian Bureau of Statistics, 2016c). Thus, the data we have presented are primarily representative of Indigenous males from regional and urban areas in eastern Australia and we ought not to generalise beyond this.
Another part of the explanation may lie in the high number of suicide deceased persons whose Indigenous identification is classified as ‘unknown’, which could impede accurate estimates of the Indigenous suicide rate across age groups. An examination of data from the National Coronial Information System (NCIS) revealed that, in older age groups compared to younger age groups, there is a marked increase in the proportion of deaths with an unknown Indigenous status relative to those classified as Indigenous (see Supplementary File 1) (NCIS, 2016). If a percentage of those with unknown Indigenous identification is actually Indigenous people, then we are potentially more severely underestimating the Indigenous suicide rate in older age groups than in younger age groups. However, even if this were the case, it is unlikely that the suicide rate for older Indigenous males would rise to the same heights as the rate for younger Indigenous males.
Notwithstanding these aetiological and methodological considerations, the divergent trends across age groups for suicide deaths and suicidal thoughts raise some pertinent questions. In some ways, the features of the divergent trends we have observed are somewhat similar to ‘the gender paradox of suicidal behaviour’ (Canetto and Sakinofsky, 1998); in many countries, females have higher rates of suicidal ideation and behaviour than males, while mortality from suicide is typically lower for females than males. Our observation raises the possibility that a similar paradox exists among Indigenous males in Australia, in that older Indigenous males could have higher rates of suicidal ideation than younger Indigenous males, while mortality from suicide remains higher for younger Indigenous males. Aside from the use of more lethal suicide methods by males, several other hypotheses have been posited to explain the gender paradox, two of which may be relevant to the discussion of our observation (Canetto and Sakinofsky, 1998; Schrijvers et al., 2012).
First, it is posited that the duration of ‘the suicidal process’ (i.e. the transition from suicidal thoughts to a suicide plan through to a suicide death), which can vary from many years to a few hours or even minutes, is shorter for men (Schrijvers et al., 2012). This means that, on average, men may have a quicker progression from suicidal thoughts to a suicide death than women, and thus have a shorter period of time for their suicidal thoughts to be detected by a suicide survey/assessment. Following this idea, our observation certainly raises the possibility that the suicidal process is shorter for younger Indigenous males than it is for older Indigenous males. Indigenous males in late adolescence and early adulthood are also going through a life stage where they are susceptible to a range of compounding risk factors for suicidality, e.g., early exposure to alcohol and other substance misuse and higher levels of aggression/violence, risk-taking and impulsivity (Bridge et al., 2006; McLoughlin et al., 2015), all of which may coalesce with suicidal thoughts to contribute to a substantial shortening of the suicidal process. It is also a life stage at which culture-based identity forming structures and social systems (e.g. cultural ceremonies, guidance from Elders) are important, yet these are less available to guide and help moderate Indigenous youth through this period than they once were (Procter, 2005). Importantly, we don’t have data on how intense or determined the suicidal thoughts were for the participants. It may be that younger Indigenous males who do have suicidal thoughts tend to experience them in a more intense and resolute way that allows them to progress to a suicide attempt at a more rapid pace.
Second, ‘cultural script theory’ posits that women and men will tend to adopt the self-destructive behaviours that are congruent with the gender scripts of their cultures, with attempting suicide ascribed a more feminine quality and killing oneself ascribed a more masculine quality in some cultural settings (Canetto and Sakinofsky, 1998). Without discussing the merits of this as it applies to the gender paradox, it is useful to contemplate that cultural narratives can influence the dynamics and frequency of individual suicides, in that individuals draw upon these cultural meanings in choosing their course of action. In this vein, it is possible that a particular cultural script may be present among some young Indigenous males who attempt or die by suicide, and that this script does not affect older Indigenous males. In the 1980s, Rubinstein undertook research on the newly emerging male youth suicide epidemic in Micronesia (Rubinstein, 1983). His findings suggested that, in one setting, a single suicide case had become a model for successive youth suicides. These youth suicides were typically characterised as spontaneous, unplanned and connected to seemingly minor situational triggers, predominantly relationship conflict with parents or girlfriends. He suggested that some male youth in this setting had developed a greater familiarity with, and acceptance of, the idea of suicide, and in some cases had expressed a sense of inevitability in relation to suicide. It was also noted that the youth suicide epidemic was occurring within the context of rapidly changing socio-cultural and intergenerational dynamics. Rubinstein’s work signposted that cultural scripts around suicide may heighten the suicide contagion process and that they can affect, even temporarily, particular age groups. We should definitely be cautious in reasoning about suicide phenomena across unique culture groups; however, several aspects of his description of the youth suicide epidemic in Micronesia echo some features of the literature on Indigenous youth suicide in Australia. In particular, the concepts of suicide contagion and suicide clusters are similarly prominent in the Australian Indigenous suicide literature (Hanssens, 2008; Hunter and Harvey, 2002), and there are some reports raising concerns about the normalisation of suicide and suicidal behaviour in youth in some Indigenous communities (Select Committee on Youth Suicide in the Northern Territory, 2012). Our observation resonates with a previous suggestion that future research should explore the potential ‘age cohort’ feature of suicide contagion in Indigenous communities (Hanssens, 2011).
Finally, the data also highlight some potentially positive findings. The prevalence of suicidal thoughts among younger Indigenous males was equivalent to the prevalence of suicidal thoughts among younger non-Indigenous males. That is, there was no gap at younger ages, and this is good news. Notwithstanding the nuances discussed above, it is thus possible that there could be a cohort effect, whereby the younger generation of Indigenous males in urban and regional areas is experiencing less suicidal thoughts than older generations of young Indigenous males. However, given that very high rates of Indigenous youth suicide in some locations continue to be reported, this may be wishful thinking (Campbell et al., 2016). There is another aspect of the findings that could be worth further consideration. If it holds true that older Indigenous males are less likely than younger Indigenous males to act on their suicidal thoughts, there may be value in examining the resilience and protective strategies deployed by older Indigenous males that support them in preventing their suicidal thoughts from translating into suicide attempts, and how these can best be shared with younger Indigenous males.
In any case, these are all queries that our data can only tentatively provoke, but cannot answer. As stated earlier, this paper is based on analyses of cross-sectional data collected for the baseline wave of the Ten to Men cohort study. The longitudinal nature of the Ten to Men study will mean that we may be able to explore this further with future waves of data.
Strengths and weaknesses
Our study has a number of strengths, most notably the large sample size and use of data collected from males in urban and regional settings across Australia. To the best of our knowledge, our analyses are the first to present data on suicidal thoughts and attempts among a nationwide sample of urban and regional Indigenous males in the general community encompassing a broad range of age groups.
Nonetheless, the data used for our analyses were collected for the baseline wave of the Ten to Men cohort study and, as such, were not designed to make these prevalence estimates. While the Ten to Men cohort study attempted to recruit as representative a sample as possible, there were various constraints. Thus, there are some limitations to the generalisability of the findings that should be taken into consideration. First, the Ten to Men study didn’t have the resources to go to remote areas and, related to this, there is an under-representation of Indigenous males from the Northern Territory, Western Australia and South Australia. However, the Ten to Men study intentionally over-sampled men from regional areas, which appears to have helped in recruiting a larger sample of Indigenous males; 65.1% of the Indigenous sub-sample were from regional areas compared to 41.7% of the non-Indigenous sub-sample. Additionally, the total proportion of Indigenous males in the sample (2.7%) is roughly equivalent to the proportion of Indigenous males in the general population (3.0%) (Australian Bureau of Statistics, 2016b). Second, the survey was self-administered for males aged 15–55 years (with a computer-assisted personal interview for boys aged 10–14 years) and this could have prevented Indigenous males with poor literacy from taking part in the study. This could be an important source of sampling bias considering that the substantial gap in literacy measures between Indigenous and non-Indigenous people remains a major issue (Ford, 2012), and the prevalence of suicidal thoughts and attempts among less literate Indigenous males could be markedly different.
Third, Indigenous researchers and advocates are calling for a greater focus on the cultural context of suicide and strengths-based research that focuses on cultural resilience and culture-based protective factors (Department of Health and Ageing, 2013), as well as the development and evaluation of self-harm interventions that are led by Aboriginal and Torres Strait Islander communities (Carter et al., 2016). This also includes the evaluation of culturally appropriate interventions that are framed around the holistic concept of social and emotional wellbeing and the promotion of multiple protective factors (e.g. physical activity, employment opportunities, strengthening families and engaging young people in culture), not just screening and clinical treatment (Aboriginal and Torres Strait Islander Suicide Prevention Evaluation Project, 2016; Luke et al., 2013). Our epidemiological analyses of trends in the prevalence of suicidality across age groups are unable to illuminate on the cultural strengths that will be of benefit to upstream Indigenous suicide prevention, although we do present new prevalence data that can inform policy, programming and future research. Finally, the primary variable in our analyses (i.e. Indigenous status) is a dichotomous variable based on an Indigenous identification question. We recognise that while this categorisation has been useful for the objectives of our analyses, neither the Indigenous persons nor the non-Indigenous persons (comprising Caucasian, Asian and other ethnicities) categories represent a homogenous group of people. Moreover, research from Queensland highlights that the concentration of Indigenous suicide deaths varies considerably across different Indigenous communities at different time points, suggesting a degree of ‘community risk’ that varies by time and location (Hunter and Harvey, 2002). Further studies in this area are required that disaggregate Indigenous suicide data across a range of socio-demographic, geographical and cultural resilience variables.
Conclusion
Our study of men from urban and regional Australia found a substantial disparity between Indigenous and non-Indigenous males with respect to the prevalence of recent suicidal thoughts and a history of having attempted suicide. There is a clear imperative to devote resources and further research to the area of Indigenous suicide prevention, with a view to increasing the availability of culturally appropriate and holistic suicide prevention supports that target Indigenous males of all ages.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The survey data on which this paper is based were collected by The University of Melbourne as part of the Australian Longitudinal Study on Male Health, funded by the Australian Government Department of Health. We are grateful to the boys and men who provided this survey data. The development and publication of this manuscript was supported by funds from a National Health and Medical Research Council targeted grant on Indigenous youth suicide prevention.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.